Embed Size (px)
Citation preview
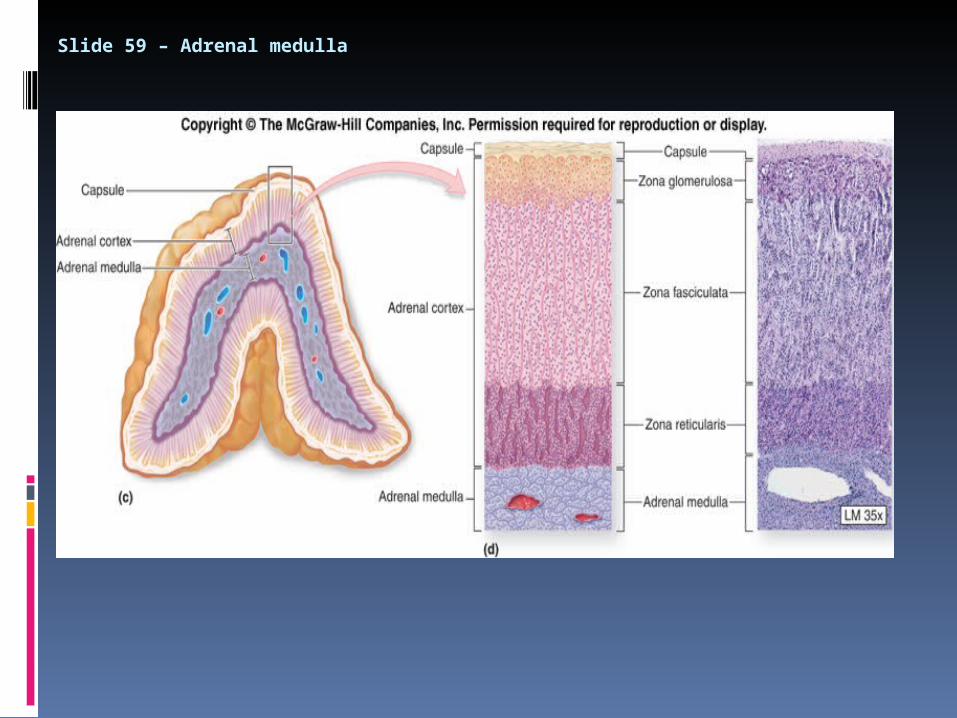
Slide 59 – Adrenal medulla
Adrenal Medulla
The inner medulla, is a source of the catecholamines epinephrine and norepinephrine.
• The chromaffin cell is the principle cell type.
• The medulla is richly innervated by preganglionic sympathetic fibers and is, in essence, an extension of the sympathetic nervous system.
Chromaffin cells in the adrenal medulla synthesize and secrete norepinephrine and epinephrine.
The ratio of these two catecholamines differs considerably among species: in humans, roughly 80% of the catecholamine output is epinephrine.
Storage and secretion-Norepinephine and epinephrine are stored in electron-dense granules, which also contain ATP and several neuropeptides. Secretion of these hormones is stimulated by acetylcholine release from preganglionic sympathetic fibres innervating the medulla. Many types of "stresses" stimulate such secretion, including exercise, hypoglycaemia and trauma. Following secretion into blood, the catecholamines bind loosely to and are carried in the circulation by albumin and perhaps other serum proteins.
Catecholamines
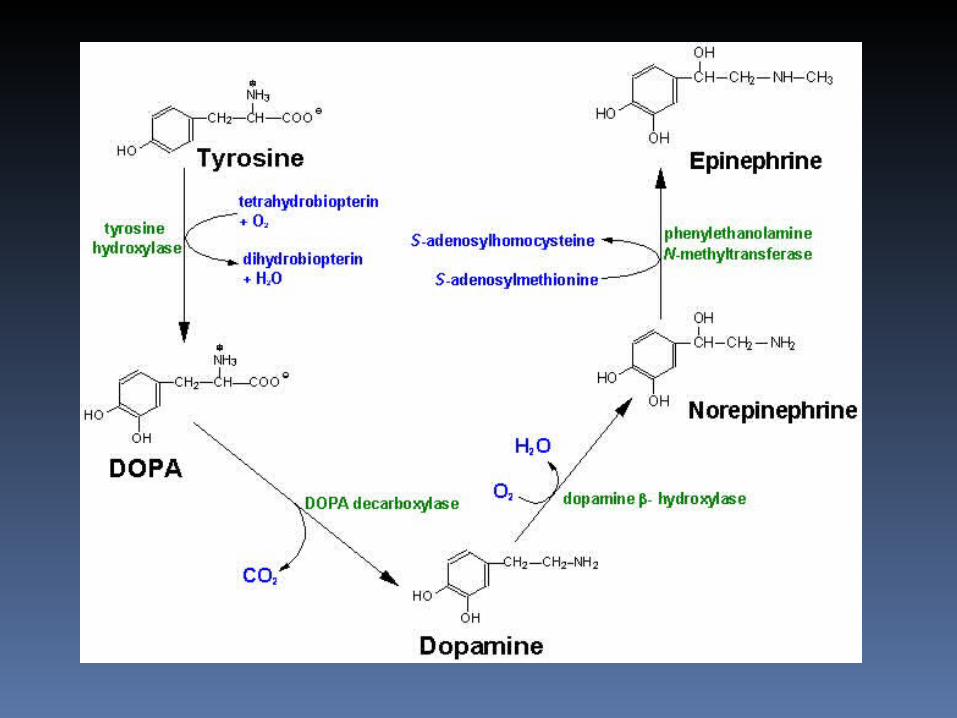
Synthesized from L-tyrosine Dopamine, noradrenaline, adrenaline L-tyr in plasma (1-1.5 mg/dL) Active transport into cells Conversion L-tyr by 4 enz’s Adrenal medulla catecholamine output
approx 80% adrenaline BUT plasma ratio 9:1 noradrenaline:
adrenaline
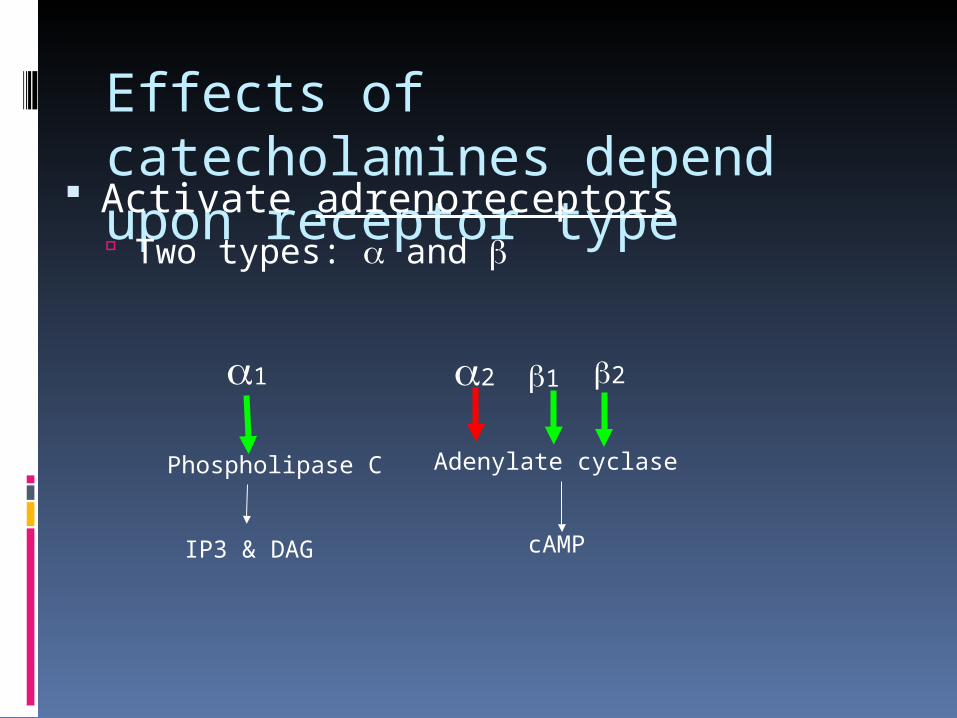
Effects of catecholamines depend upon receptor type
Activate adrenoreceptors Two types: and
1 2 1 2
Phospholipase C
IP3 & DAG
Adenylate cyclase
cAMP
Physiological actions of the catecholamines •Norepinephrinefunctions primarily act as
a neurotransmitter. •Both norepinephrine and epinephrine
influence the vascular system, whereas epinephrine affects metabolic processes such as carbohydrate metabolism.
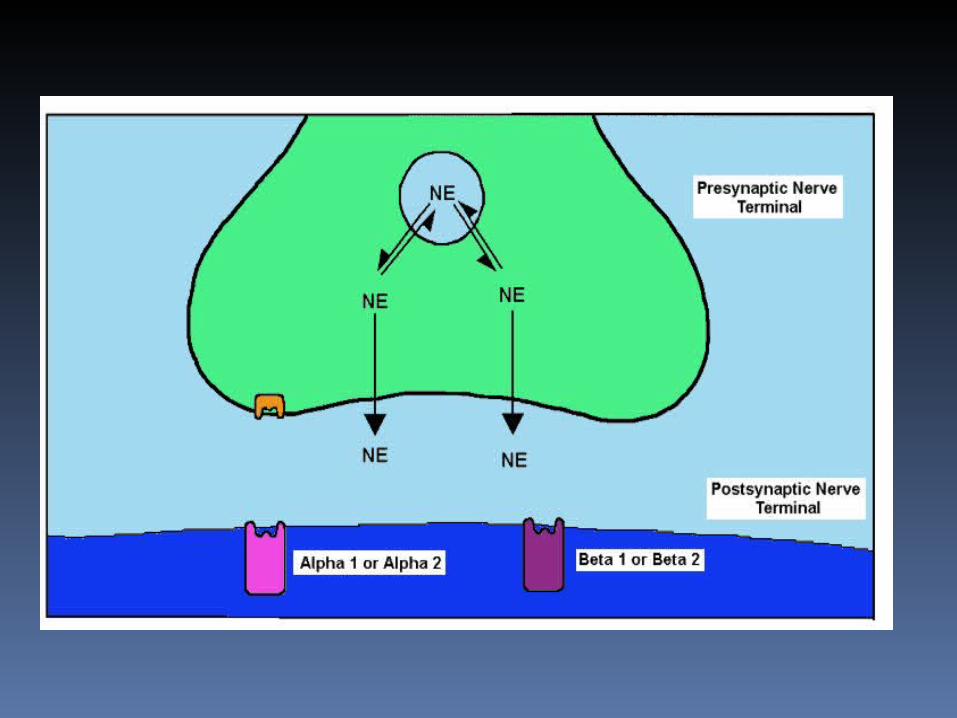
•The actions of the catecholamines are initiated through their interaction with two different types of specific cell membrane receptors, the alpha-adrenergic and beta- adrenergic receptors. •
These receptors have different affinities for norepinephrine and epinephrine and cause opposing physiological effects. •Norepinephrine primarily interacts with alpha-adrenergic receptors, whereas epinephrine interacts with both alpha- and beta-receptors.
Stimulation of alpha-adrenergic receptors results in: vasoconstriction, decrease in insulin and increase in glucagon secretion, sweating, piloerection(hair standing on end), and stimulation of glycogenolysis in the liver and skeletal muscle leading to an increase in blood glucose concentration.
Stimulation of beta-receptors leads to: vasodilatation; stimulation of insulin release; increased cardiac contraction rate; relaxation of smooth muscle in the intestinal tract; bronchodilatation by relaxation of smooth muscles in bronchi; stimulation of renin release, which enhances sodium reabsorption from the kidney; and enhanced lipolysis.
Factors Regulating release
•The synthesis of epinephrine and norepinephrineis regulated by the intracellular concentrations of these hormones by negative-feedback inhibition. •The catecholaminesare released from the adrenal medulla in response to hypotension, hypoxia, expsoureto cold, muscular exertion, pain, and emotional disturbances.
Source of circulating catecholaminesCirculating catecholamines, epinephrine and norepinephrine, originate from two sources. •Epinephrine is released by the adrenal medulla upon activation of preganglionic sympathetic nerves innervating this tissue. This activation occurs during times of stress (e.g., exercise, heart failure, hemorrhage, emotional stress or excitement, pain).
•Norepinephrineis also released by the adrenal medulla (about 20% of its total catecholamine release is norepinephrine). The primary source of circulating norepinephrine spill over from sympathetic nerves innervating blood vessels. Normally, most of the norepinephrine released by sympathetic nerves is taken back up by the nerves (some is also taken up by extra-neuronal tissues) where it is metabolized. A small amount of norepinephrine, however, diffuses into the blood and circulates throughout the body. At times of high sympathetic nerve activation, the amount of norepinephrine entering the blood increases dramatically.
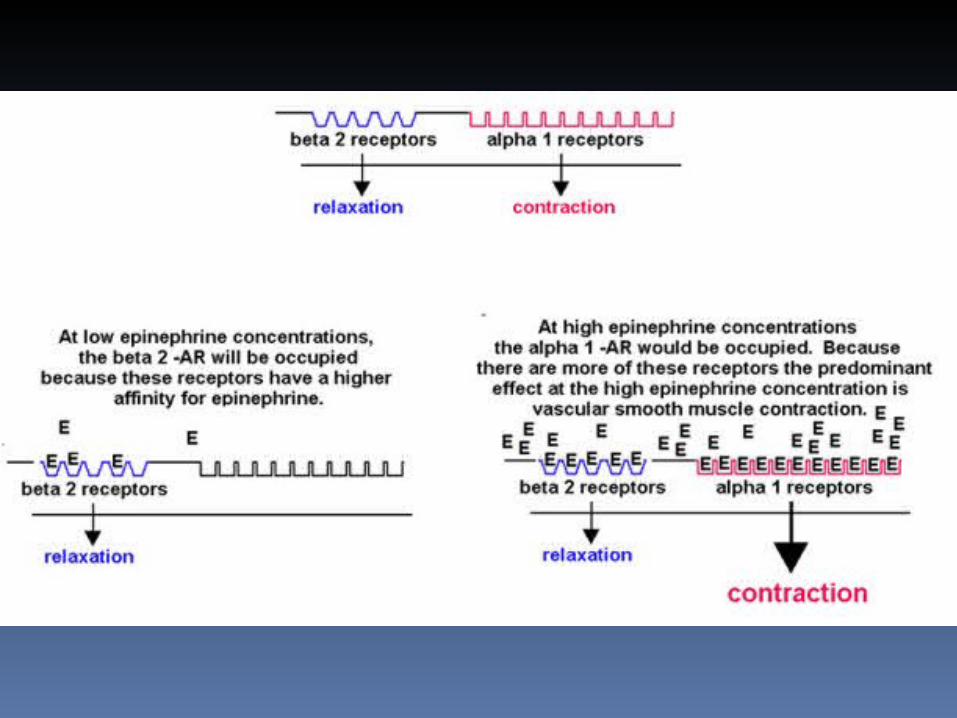
Circulating epinephrine causes: •Increased heart rate and inotropy(ß1- adrenoceptor mediated) •Vasoconstriction in most systemic arteries and veins (postjunctional a1 and a2 adrenoceptors) •Vasodilation in muscle and liver vasculatures at low concentrations (b2-adrenoceptor); vasoconstriction at high concentrations (a1- adrenoceptor mediated) •The overall cardiovascular responseto low- to-moderate circulating concentrations of epinephrine results in increased cardiac output and a redistribution of the cardiac output to muscular and hepatic circulations with only a small change in mean arterial pressure.
Although cardiac output is increased, arterial pressure does not change much because the systemic vascular resistance falls due to b2- adrenoceptor activation. •At high plasma concentrations, epinephrine increases arterial pressure because of binding to a-adrenoceptors on blood vessels, which offsets the b2-adrenoceptor mediated vasodilation.
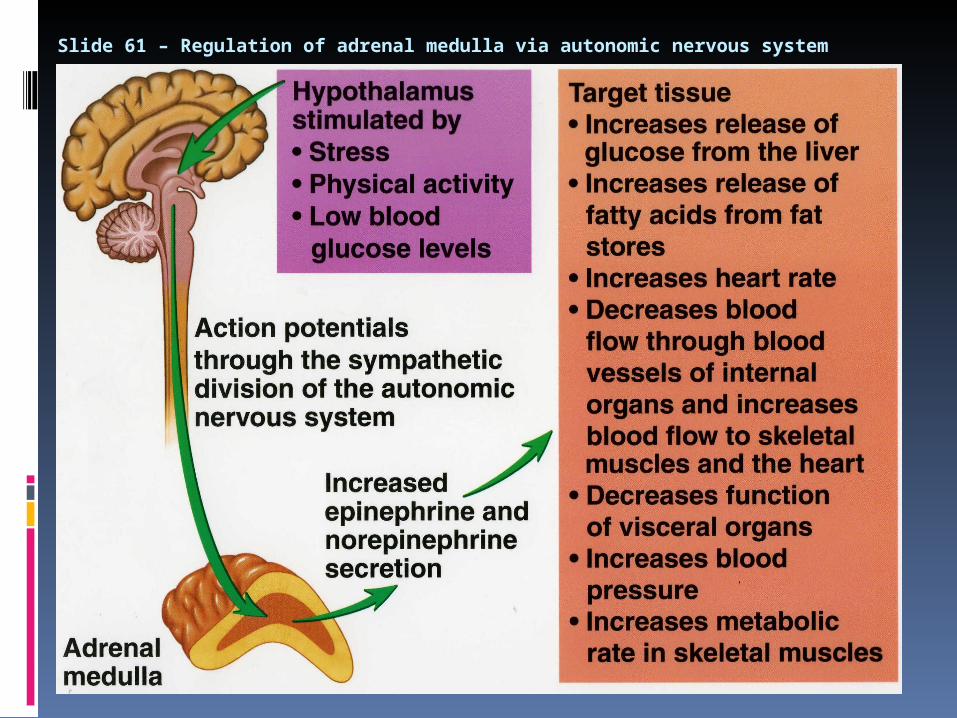
Slide 61 – Regulation of adrenal medulla via autonomic nervous system
Actions of Catecholamines Catecholamines act on their target tissues through G-protein-linked membrane
receptors.
Cardiovascular Increase in heart rate Increased venous return Increased peripheral resistance
Visceral Smooth muscle relaxation and contraction Modulation of fluid and electrolyte transport in the gut, kidney, gall bladder
Metabolic Glycogenolysis, lipolysis
Water and electrolyte metabolism Decreased sodium excretion and glomerular filtration Effects on renin secretion leads to increased aldosterone production
Hormone secretion Modulates the responses of a number of endocrine systems, including: The renin-
angiotensin-aldosterone system Increased secretion of glucagon and insulin