Embed Size (px)
Citation preview

mohammad reza rajabi
Page 1 432012
Introduction
When temporary mechanical ventilation is required either in the treatment of respiratory failure or during surgery with muscular
relaxation endotracheal intubation is usually the preferred method of airway management
Why is this the preferred means of airway management The primary reason is that it provides a protected airway
Protected from what you ask
Well protected from introduction of foreign matter particularly gastric contents
The accurate placement of an endotracheal tube requires skill Usually the patient is rendered unconscious and immobile (including
paralysis of the muscles of respiration) for the placement Obviously inability to rapidly obtain control of the patients airway in this
setting would be bad if not lethal
The airway examination is an effort to identify those patients in whom conventional endotracheal intubation will be difficult It is vitally important to recognize such patients BEFORE administering medications that induce apnea( Lack of breathing)
Endotracheal Intubation
mohammad reza rajabi
Page 2 432012
Endotracheal Tube
Acknowledgements
This educational site was developed by
Tammy Euliano MD Associate Professor of Anesthesiology
with the assistance of
future doctor Amy Lee programmers Karthik Paladugu and Rick Lockwood graphic artist future doctor Christopher Hurt
Major contributions were provided by
Ilona Schmalfuss MD Assistant Professor of Radiology Jeremy Melker MD Otolaryngology Resident
Funding was provided by the
University of Florida College of Medicine Education Committee
mohammad reza rajabi
Page 3 432012
Aspiration of Gastric Contents
The risk of passive reflux of gastric contents into the pharynx is increased when the stomach is full If the gag reflex has been
blunted (by alcohol ingestion decreased mental status or medications) the acidic volume can make its way into the trachea
causing potentially extensive damage
Aspiration Prevention
In this case which of the following could reduce the risk of
aspiration and its consequences
Wait 6 hours before proceeding keeping the patient NPO
Yes No
(yes) Incorrect - Nil per os
While this will help for elective surgery patients trauma patients and
those with acute GI problems will not empty their stomachs well In
addition this operation should not be postponed for any length of time due to the risk of appendix rupture andor sepsis
(no)Correct
While a 6-hour NPO period is ideal this surgery should not be
postponed
Administration of a non-particulate antacid
Yes No
(yes)Correct - Non-particulate antacid
Many would advocate having the patient drink 15-30cc sodium citrate or bicitra within 30 minutes of induction of anesthesia
Though this increases the stomach volume it is actually protective
mohammad reza rajabi
Page 4 432012
as it raises the pH of the stomach contents reducing injury to the
lung in the event of an aspiration
(no)Incorrect - Non-particulate antacid
Many would advocate having the patient drink 15-30cc sodium citrate or bicitra within 30 minutes of induction of anesthesia
Though this increases the stomach volume it is actually protective as it raises the pH of the stomach contents reducing injury to the
lung in the event of an aspiration
Administration of H2 blockers
Yes No
(yes)Correct - H2 Blockers
The onset time of these medications is 30+ minutes and even then they do not affect the pH of the volume already in the stomach
However new fluid will be secreted into the stomach at a higher pH perhaps increasing the overall pH by the time of emergence from
anesthesia (the other time at which patients are at risk for aspiration)
(no)Incorrect - H2 Blockers
The onset time of these medications is 30+ minutes and even then they do not affect the pH of the volume already in the stomach
However new fluid will be secreted into the stomach at a higher pH perhaps increasing the overall pH by the time of emergence from
anesthesia (the other time at which patients are at risk for aspiration)
Administration of metoclopramide
Yes No
mohammad reza rajabi
Page 5 432012
(yes)Correct - Metoclopramide
Metoclopramide speeds gastric emptying and increases the lower
esophageal sphincter (LES) pressure While the latter is helpful at reducing the risk of aspiration within minutes stomach volume
reduction takes more time This emptying should occur however
and can reduce the risk of aspiration during emergence and extubation at the end of the operation There are some risks to
metoclopramide so as with everything a riskbenefit evaluation must be performed
(no)Incorrect - Metoclopramide
Metoclopramide speeds gastric emptying and increases the lower esophageal sphincter (LES) pressure While the latter is helpful at
reducing the risk of aspiration within minutes stomach volume reduction takes more time This emptying should occur however
and can reduce the risk of aspiration during emergence and extubation at the end of the operation There are some risks to
metoclopramide so as with everything a riskbenefit evaluation must be performed
Rapid Sequence Induction
Yes No
(yes)Correct - Rapid Sequence Induction
Following pre-oxygenation the patient is put to sleep with a rapid acting IV induction agent such as sodium thiopental immediately
followed by succinylcholine (or other rapid-acting agent) application of cricoid pressure and intubation of the trachea
Positive pressure mask ventilation is not performed to avoid increasing gastric volume The purpose of this technique is to
minimize the duration of impaired gag reflex prior to intubation
Cricoid Pressure during intubation
Yes No
mohammad reza rajabi
Page 6 432012
(no) Incorrect - Cricoid Pressure during Intubation
An assistant identifies the cricoid ring and applies pressure compressing the esophagus against the underlying vertebral
body This prevents passive reflux of gastric contents into the lung How much pressure to apply is a continuing question
current recommendations suggest approximately 10 Newtons (1 kg) of force (mild discomfort for the patient) as the induction
medications are being administered Once the patient loses consciousness the cricoid pressure should be increased to
approximately 30 Newtons (3 kg) It is possible for this pressure to make intubation more difficult and some reduction in force
may be necessary
(yes)Correct - Cricoid Pressure during Intubation
An assistant identifies the cricoid ring and applies pressure compressing the esophagus against the underlying vertebral
body This prevents passive reflux of gastric contents into the lung How much pressure to apply is a continuing question
current recommendations suggest approximately 10 Newtons (1 kg) of force (mild discomfort for the patient) as the induction
medications are being administered Once the patient loses consciousness the cricoid pressure should be increased to
approximately 30 Newtons (3 kg) It is possible for this pressure to make intubation more difficult and some reduction in force
Endotracheal Intubation
Intubation is typically performed under direct visualization That is
by looking through the mouth directly at the vocal cords (direct laryngoscopy) and watching the endotracheal tube pass through the
cords and into the trachea However there is no direct line-of-sight from the mouth to the vocal cords
Check in a mirror or examine a friend (preferably one who has not
eaten onions recently) even with the mouth maximally opened and
tongue extended you cannot see the vocal cords in fact only rarely can you see the epiglottis
mohammad reza rajabi
Page 7 432012
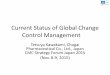
Mallampati Classification
Actually the amount of the posterior pharynx you can visualize is
important and correlates with the difficulty of intubation
Visualization of the pharynx is obscured by a large tongue (relative to the size of the mouth) which also interferes with visualization of
the larynx on laryngoscopy The Mallampati Classification is based on the structures visualized with maximal mouth opening and tongue
protrusion in the sitting position (originally described without phonation but others have suggested minimum Mallampati
Classification with or without phonation best correlates with intubation difficulty)
mohammad reza rajabi
Page 8 432012
Class I soft palate fauces uvula pillars Class II soft palate fauces portion of uvula
Class III soft palate base of uvula Class IV hard palate only
Other Predictors of Difficult Intubation
Obesity ndash body weight gt 110kg
Mouth opening ndash inter-incisor distance lt 4cm in an adult
Ability to prognath ndash a large overbite or the inability to shift
the lower incisors in front of the upper incisors
Thyromental distance ndash The distance from the thyroid cartilage to the mentum (tip of the chin) should be gt 65-7 cm
Mentum-Hyoid distance ndash Similar to thyromental distance and should be at least 3-4 finger-breadths
Many other factors have been investigated with variable results
Other factors that may indicate a difficult intubation
Sternomental distance ndash Similar to above measured from the sternum to the tip of the mandible with the head extended This measure is influenced by neck extension Should be gt125cm
Mandibulohyoid distance ndash the vertical distance between the mandible and the hyoid bone determined radiographically This may be increased with a short mandibular ramus or a caudally located hyoid bone Such an increase in this distance may be associated with difficult intubation Chou 1993
Thyrosternal distance ndash lt8cm may suggest difficulty probably related to the caudally located hyoid as above
mohammad reza rajabi
Page 9 432012
Various radiographic measurements of the cervical spine its alignment with airway structures and the atlanto-occipital joint
Positioning
To obtain a direct line of sight the patient is positioned in the sniffing position The neck is flexed at the lower cervical spine and
extended at the atlanto-occipital joint This flexion and extension is amplified during laryngoscopy
The patientrsquos neck mobility should be assessed preoperatively by
having them flex and extend their head maximally The range of
motion should be more than 90deg Motion less than 80deg may triple the risk of a poor view at laryngoscopy
mohammad reza rajabi
Page 10 432012
Direct Laryngoscopy
Then a laryngoscope is used to pull the lower jaw and tongue up and out of the way
The metal blade is passed into the mouth to the level of the epiglottis then with an anterior and caudad motion (ie toward the
edge of the ceiling across the room) the lower jaw is elevated allowing visualization of the glottic structures( The glottis is the
structures of phonation including the vocal cords and surrounding structures) In most patients this results in a clear view of the larynx
and the endotracheal tube is passed through the vocal cords under
direct visualization
mohammad reza rajabi
Page 11 432012
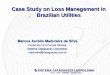
Laryngoscopy Grades
In most patients Direct Laryngoscopy results in a clear view of the larynx The laryngeal view has been classified by Cormack and
Lehane as follows
Grade 1 Full view of the glottis Grade 2 Only the posterior commissure is visible
Grade 3 Only the epiglottis is seen Grade 4 No epiglottis or glottis structure visible
Airway Review
What might make Direct Laryngoscopy and Intubation more difficult
Inability to open the mouth
Yes No
(yes)Correct
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
(no)Incorrect
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
mohammad reza rajabi
Page 12 432012
Inability to extend the neck
Yes No
(yes)Correct
The sniffing position requires significant neck extension
(no)Incorrect
The sniffing position requires significant neck extension
Inability to breathe through the nose
Yes No
(no)Correct
Unless a nasal intubation is planned
(yes)Incorrect
Unless a nasal intubation is planned
Large tongue
Yes No
(yes)Correct
Also if it is immobile as from radiation therapy
(no)Incorrect
Also if it is immobile as from radiation therapy
Redundant pharyngeal tissue
Yes No
(yes)Correct
This occurs with obesity and is often suggested by a history of
snoring andor obstructive sleep apnea
mohammad reza rajabi
Page 13 432012
(no)Incorrect
This occurs with obesity and is often suggested by a history of snoring andor obstructive sleep apnea
Case 2 Abnormal Exam
A healthy 25-year-old man is scheduled to have a shoulder repair requiring general anesthesia
Lets review his airway examination
What would you like the patient to do
Open his mouth as wide as possible
Extend his neck as far as possible without pain
View from the side
mohammad reza rajabi
Page 14 432012
Open Mouth
This patients mouth opening is 2 finger-breadths the soft palate is
barely visible on maximal mouth opening
Neck
mohammad reza rajabi
Page 15 432012
View from the side
2 finger-breadths fit between the tip of the chin and the neck
Airway Examination
Mouth opening
Normal
Reduced
What is mouth opening
(normal)Incorrect
it is less than 3 finger breadths
mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 2 432012
Endotracheal Tube
Acknowledgements
This educational site was developed by
Tammy Euliano MD Associate Professor of Anesthesiology
with the assistance of
future doctor Amy Lee programmers Karthik Paladugu and Rick Lockwood graphic artist future doctor Christopher Hurt
Major contributions were provided by
Ilona Schmalfuss MD Assistant Professor of Radiology Jeremy Melker MD Otolaryngology Resident
Funding was provided by the
University of Florida College of Medicine Education Committee
mohammad reza rajabi
Page 3 432012
Aspiration of Gastric Contents
The risk of passive reflux of gastric contents into the pharynx is increased when the stomach is full If the gag reflex has been
blunted (by alcohol ingestion decreased mental status or medications) the acidic volume can make its way into the trachea
causing potentially extensive damage
Aspiration Prevention
In this case which of the following could reduce the risk of
aspiration and its consequences
Wait 6 hours before proceeding keeping the patient NPO
Yes No
(yes) Incorrect - Nil per os
While this will help for elective surgery patients trauma patients and
those with acute GI problems will not empty their stomachs well In
addition this operation should not be postponed for any length of time due to the risk of appendix rupture andor sepsis
(no)Correct
While a 6-hour NPO period is ideal this surgery should not be
postponed
Administration of a non-particulate antacid
Yes No
(yes)Correct - Non-particulate antacid
Many would advocate having the patient drink 15-30cc sodium citrate or bicitra within 30 minutes of induction of anesthesia
Though this increases the stomach volume it is actually protective
mohammad reza rajabi
Page 4 432012
as it raises the pH of the stomach contents reducing injury to the
lung in the event of an aspiration
(no)Incorrect - Non-particulate antacid
Many would advocate having the patient drink 15-30cc sodium citrate or bicitra within 30 minutes of induction of anesthesia
Though this increases the stomach volume it is actually protective as it raises the pH of the stomach contents reducing injury to the
lung in the event of an aspiration
Administration of H2 blockers
Yes No
(yes)Correct - H2 Blockers
The onset time of these medications is 30+ minutes and even then they do not affect the pH of the volume already in the stomach
However new fluid will be secreted into the stomach at a higher pH perhaps increasing the overall pH by the time of emergence from
anesthesia (the other time at which patients are at risk for aspiration)
(no)Incorrect - H2 Blockers
The onset time of these medications is 30+ minutes and even then they do not affect the pH of the volume already in the stomach
However new fluid will be secreted into the stomach at a higher pH perhaps increasing the overall pH by the time of emergence from
anesthesia (the other time at which patients are at risk for aspiration)
Administration of metoclopramide
Yes No
mohammad reza rajabi
Page 5 432012
(yes)Correct - Metoclopramide
Metoclopramide speeds gastric emptying and increases the lower
esophageal sphincter (LES) pressure While the latter is helpful at reducing the risk of aspiration within minutes stomach volume
reduction takes more time This emptying should occur however
and can reduce the risk of aspiration during emergence and extubation at the end of the operation There are some risks to
metoclopramide so as with everything a riskbenefit evaluation must be performed
(no)Incorrect - Metoclopramide
Metoclopramide speeds gastric emptying and increases the lower esophageal sphincter (LES) pressure While the latter is helpful at
reducing the risk of aspiration within minutes stomach volume reduction takes more time This emptying should occur however
and can reduce the risk of aspiration during emergence and extubation at the end of the operation There are some risks to
metoclopramide so as with everything a riskbenefit evaluation must be performed
Rapid Sequence Induction
Yes No
(yes)Correct - Rapid Sequence Induction
Following pre-oxygenation the patient is put to sleep with a rapid acting IV induction agent such as sodium thiopental immediately
followed by succinylcholine (or other rapid-acting agent) application of cricoid pressure and intubation of the trachea
Positive pressure mask ventilation is not performed to avoid increasing gastric volume The purpose of this technique is to
minimize the duration of impaired gag reflex prior to intubation
Cricoid Pressure during intubation
Yes No
mohammad reza rajabi
Page 6 432012
(no) Incorrect - Cricoid Pressure during Intubation
An assistant identifies the cricoid ring and applies pressure compressing the esophagus against the underlying vertebral
body This prevents passive reflux of gastric contents into the lung How much pressure to apply is a continuing question
current recommendations suggest approximately 10 Newtons (1 kg) of force (mild discomfort for the patient) as the induction
medications are being administered Once the patient loses consciousness the cricoid pressure should be increased to
approximately 30 Newtons (3 kg) It is possible for this pressure to make intubation more difficult and some reduction in force
may be necessary
(yes)Correct - Cricoid Pressure during Intubation
An assistant identifies the cricoid ring and applies pressure compressing the esophagus against the underlying vertebral
body This prevents passive reflux of gastric contents into the lung How much pressure to apply is a continuing question
current recommendations suggest approximately 10 Newtons (1 kg) of force (mild discomfort for the patient) as the induction
medications are being administered Once the patient loses consciousness the cricoid pressure should be increased to
approximately 30 Newtons (3 kg) It is possible for this pressure to make intubation more difficult and some reduction in force
Endotracheal Intubation
Intubation is typically performed under direct visualization That is
by looking through the mouth directly at the vocal cords (direct laryngoscopy) and watching the endotracheal tube pass through the
cords and into the trachea However there is no direct line-of-sight from the mouth to the vocal cords
Check in a mirror or examine a friend (preferably one who has not
eaten onions recently) even with the mouth maximally opened and
tongue extended you cannot see the vocal cords in fact only rarely can you see the epiglottis
mohammad reza rajabi
Page 7 432012
Mallampati Classification
Actually the amount of the posterior pharynx you can visualize is
important and correlates with the difficulty of intubation
Visualization of the pharynx is obscured by a large tongue (relative to the size of the mouth) which also interferes with visualization of
the larynx on laryngoscopy The Mallampati Classification is based on the structures visualized with maximal mouth opening and tongue
protrusion in the sitting position (originally described without phonation but others have suggested minimum Mallampati
Classification with or without phonation best correlates with intubation difficulty)
mohammad reza rajabi
Page 8 432012
Class I soft palate fauces uvula pillars Class II soft palate fauces portion of uvula
Class III soft palate base of uvula Class IV hard palate only
Other Predictors of Difficult Intubation
Obesity ndash body weight gt 110kg
Mouth opening ndash inter-incisor distance lt 4cm in an adult
Ability to prognath ndash a large overbite or the inability to shift
the lower incisors in front of the upper incisors
Thyromental distance ndash The distance from the thyroid cartilage to the mentum (tip of the chin) should be gt 65-7 cm
Mentum-Hyoid distance ndash Similar to thyromental distance and should be at least 3-4 finger-breadths
Many other factors have been investigated with variable results
Other factors that may indicate a difficult intubation
Sternomental distance ndash Similar to above measured from the sternum to the tip of the mandible with the head extended This measure is influenced by neck extension Should be gt125cm
Mandibulohyoid distance ndash the vertical distance between the mandible and the hyoid bone determined radiographically This may be increased with a short mandibular ramus or a caudally located hyoid bone Such an increase in this distance may be associated with difficult intubation Chou 1993
Thyrosternal distance ndash lt8cm may suggest difficulty probably related to the caudally located hyoid as above
mohammad reza rajabi
Page 9 432012
Various radiographic measurements of the cervical spine its alignment with airway structures and the atlanto-occipital joint
Positioning
To obtain a direct line of sight the patient is positioned in the sniffing position The neck is flexed at the lower cervical spine and
extended at the atlanto-occipital joint This flexion and extension is amplified during laryngoscopy
The patientrsquos neck mobility should be assessed preoperatively by
having them flex and extend their head maximally The range of
motion should be more than 90deg Motion less than 80deg may triple the risk of a poor view at laryngoscopy
mohammad reza rajabi
Page 10 432012
Direct Laryngoscopy
Then a laryngoscope is used to pull the lower jaw and tongue up and out of the way
The metal blade is passed into the mouth to the level of the epiglottis then with an anterior and caudad motion (ie toward the
edge of the ceiling across the room) the lower jaw is elevated allowing visualization of the glottic structures( The glottis is the
structures of phonation including the vocal cords and surrounding structures) In most patients this results in a clear view of the larynx
and the endotracheal tube is passed through the vocal cords under
direct visualization
mohammad reza rajabi
Page 11 432012
Laryngoscopy Grades
In most patients Direct Laryngoscopy results in a clear view of the larynx The laryngeal view has been classified by Cormack and
Lehane as follows
Grade 1 Full view of the glottis Grade 2 Only the posterior commissure is visible
Grade 3 Only the epiglottis is seen Grade 4 No epiglottis or glottis structure visible
Airway Review
What might make Direct Laryngoscopy and Intubation more difficult
Inability to open the mouth
Yes No
(yes)Correct
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
(no)Incorrect
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
mohammad reza rajabi
Page 12 432012
Inability to extend the neck
Yes No
(yes)Correct
The sniffing position requires significant neck extension
(no)Incorrect
The sniffing position requires significant neck extension
Inability to breathe through the nose
Yes No
(no)Correct
Unless a nasal intubation is planned
(yes)Incorrect
Unless a nasal intubation is planned
Large tongue
Yes No
(yes)Correct
Also if it is immobile as from radiation therapy
(no)Incorrect
Also if it is immobile as from radiation therapy
Redundant pharyngeal tissue
Yes No
(yes)Correct
This occurs with obesity and is often suggested by a history of
snoring andor obstructive sleep apnea
mohammad reza rajabi
Page 13 432012
(no)Incorrect
This occurs with obesity and is often suggested by a history of snoring andor obstructive sleep apnea
Case 2 Abnormal Exam
A healthy 25-year-old man is scheduled to have a shoulder repair requiring general anesthesia
Lets review his airway examination
What would you like the patient to do
Open his mouth as wide as possible
Extend his neck as far as possible without pain
View from the side
mohammad reza rajabi
Page 14 432012
Open Mouth
This patients mouth opening is 2 finger-breadths the soft palate is
barely visible on maximal mouth opening
Neck
mohammad reza rajabi
Page 15 432012
View from the side
2 finger-breadths fit between the tip of the chin and the neck
Airway Examination
Mouth opening
Normal
Reduced
What is mouth opening
(normal)Incorrect
it is less than 3 finger breadths
mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 3 432012
Aspiration of Gastric Contents
The risk of passive reflux of gastric contents into the pharynx is increased when the stomach is full If the gag reflex has been
blunted (by alcohol ingestion decreased mental status or medications) the acidic volume can make its way into the trachea
causing potentially extensive damage
Aspiration Prevention
In this case which of the following could reduce the risk of
aspiration and its consequences
Wait 6 hours before proceeding keeping the patient NPO
Yes No
(yes) Incorrect - Nil per os
While this will help for elective surgery patients trauma patients and
those with acute GI problems will not empty their stomachs well In
addition this operation should not be postponed for any length of time due to the risk of appendix rupture andor sepsis
(no)Correct
While a 6-hour NPO period is ideal this surgery should not be
postponed
Administration of a non-particulate antacid
Yes No
(yes)Correct - Non-particulate antacid
Many would advocate having the patient drink 15-30cc sodium citrate or bicitra within 30 minutes of induction of anesthesia
Though this increases the stomach volume it is actually protective
mohammad reza rajabi
Page 4 432012
as it raises the pH of the stomach contents reducing injury to the
lung in the event of an aspiration
(no)Incorrect - Non-particulate antacid
Many would advocate having the patient drink 15-30cc sodium citrate or bicitra within 30 minutes of induction of anesthesia
Though this increases the stomach volume it is actually protective as it raises the pH of the stomach contents reducing injury to the
lung in the event of an aspiration
Administration of H2 blockers
Yes No
(yes)Correct - H2 Blockers
The onset time of these medications is 30+ minutes and even then they do not affect the pH of the volume already in the stomach
However new fluid will be secreted into the stomach at a higher pH perhaps increasing the overall pH by the time of emergence from
anesthesia (the other time at which patients are at risk for aspiration)
(no)Incorrect - H2 Blockers
The onset time of these medications is 30+ minutes and even then they do not affect the pH of the volume already in the stomach
However new fluid will be secreted into the stomach at a higher pH perhaps increasing the overall pH by the time of emergence from
anesthesia (the other time at which patients are at risk for aspiration)
Administration of metoclopramide
Yes No
mohammad reza rajabi
Page 5 432012
(yes)Correct - Metoclopramide
Metoclopramide speeds gastric emptying and increases the lower
esophageal sphincter (LES) pressure While the latter is helpful at reducing the risk of aspiration within minutes stomach volume
reduction takes more time This emptying should occur however
and can reduce the risk of aspiration during emergence and extubation at the end of the operation There are some risks to
metoclopramide so as with everything a riskbenefit evaluation must be performed
(no)Incorrect - Metoclopramide
Metoclopramide speeds gastric emptying and increases the lower esophageal sphincter (LES) pressure While the latter is helpful at
reducing the risk of aspiration within minutes stomach volume reduction takes more time This emptying should occur however
and can reduce the risk of aspiration during emergence and extubation at the end of the operation There are some risks to
metoclopramide so as with everything a riskbenefit evaluation must be performed
Rapid Sequence Induction
Yes No
(yes)Correct - Rapid Sequence Induction
Following pre-oxygenation the patient is put to sleep with a rapid acting IV induction agent such as sodium thiopental immediately
followed by succinylcholine (or other rapid-acting agent) application of cricoid pressure and intubation of the trachea
Positive pressure mask ventilation is not performed to avoid increasing gastric volume The purpose of this technique is to
minimize the duration of impaired gag reflex prior to intubation
Cricoid Pressure during intubation
Yes No
mohammad reza rajabi
Page 6 432012
(no) Incorrect - Cricoid Pressure during Intubation
An assistant identifies the cricoid ring and applies pressure compressing the esophagus against the underlying vertebral
body This prevents passive reflux of gastric contents into the lung How much pressure to apply is a continuing question
current recommendations suggest approximately 10 Newtons (1 kg) of force (mild discomfort for the patient) as the induction
medications are being administered Once the patient loses consciousness the cricoid pressure should be increased to
approximately 30 Newtons (3 kg) It is possible for this pressure to make intubation more difficult and some reduction in force
may be necessary
(yes)Correct - Cricoid Pressure during Intubation
An assistant identifies the cricoid ring and applies pressure compressing the esophagus against the underlying vertebral
body This prevents passive reflux of gastric contents into the lung How much pressure to apply is a continuing question
current recommendations suggest approximately 10 Newtons (1 kg) of force (mild discomfort for the patient) as the induction
medications are being administered Once the patient loses consciousness the cricoid pressure should be increased to
approximately 30 Newtons (3 kg) It is possible for this pressure to make intubation more difficult and some reduction in force
Endotracheal Intubation
Intubation is typically performed under direct visualization That is
by looking through the mouth directly at the vocal cords (direct laryngoscopy) and watching the endotracheal tube pass through the
cords and into the trachea However there is no direct line-of-sight from the mouth to the vocal cords
Check in a mirror or examine a friend (preferably one who has not
eaten onions recently) even with the mouth maximally opened and
tongue extended you cannot see the vocal cords in fact only rarely can you see the epiglottis
mohammad reza rajabi
Page 7 432012
Mallampati Classification
Actually the amount of the posterior pharynx you can visualize is
important and correlates with the difficulty of intubation
Visualization of the pharynx is obscured by a large tongue (relative to the size of the mouth) which also interferes with visualization of
the larynx on laryngoscopy The Mallampati Classification is based on the structures visualized with maximal mouth opening and tongue
protrusion in the sitting position (originally described without phonation but others have suggested minimum Mallampati
Classification with or without phonation best correlates with intubation difficulty)
mohammad reza rajabi
Page 8 432012
Class I soft palate fauces uvula pillars Class II soft palate fauces portion of uvula
Class III soft palate base of uvula Class IV hard palate only
Other Predictors of Difficult Intubation
Obesity ndash body weight gt 110kg
Mouth opening ndash inter-incisor distance lt 4cm in an adult
Ability to prognath ndash a large overbite or the inability to shift
the lower incisors in front of the upper incisors
Thyromental distance ndash The distance from the thyroid cartilage to the mentum (tip of the chin) should be gt 65-7 cm
Mentum-Hyoid distance ndash Similar to thyromental distance and should be at least 3-4 finger-breadths
Many other factors have been investigated with variable results
Other factors that may indicate a difficult intubation
Sternomental distance ndash Similar to above measured from the sternum to the tip of the mandible with the head extended This measure is influenced by neck extension Should be gt125cm
Mandibulohyoid distance ndash the vertical distance between the mandible and the hyoid bone determined radiographically This may be increased with a short mandibular ramus or a caudally located hyoid bone Such an increase in this distance may be associated with difficult intubation Chou 1993
Thyrosternal distance ndash lt8cm may suggest difficulty probably related to the caudally located hyoid as above
mohammad reza rajabi
Page 9 432012
Various radiographic measurements of the cervical spine its alignment with airway structures and the atlanto-occipital joint
Positioning
To obtain a direct line of sight the patient is positioned in the sniffing position The neck is flexed at the lower cervical spine and
extended at the atlanto-occipital joint This flexion and extension is amplified during laryngoscopy
The patientrsquos neck mobility should be assessed preoperatively by
having them flex and extend their head maximally The range of
motion should be more than 90deg Motion less than 80deg may triple the risk of a poor view at laryngoscopy
mohammad reza rajabi
Page 10 432012
Direct Laryngoscopy
Then a laryngoscope is used to pull the lower jaw and tongue up and out of the way
The metal blade is passed into the mouth to the level of the epiglottis then with an anterior and caudad motion (ie toward the
edge of the ceiling across the room) the lower jaw is elevated allowing visualization of the glottic structures( The glottis is the
structures of phonation including the vocal cords and surrounding structures) In most patients this results in a clear view of the larynx
and the endotracheal tube is passed through the vocal cords under
direct visualization
mohammad reza rajabi
Page 11 432012
Laryngoscopy Grades
In most patients Direct Laryngoscopy results in a clear view of the larynx The laryngeal view has been classified by Cormack and
Lehane as follows
Grade 1 Full view of the glottis Grade 2 Only the posterior commissure is visible
Grade 3 Only the epiglottis is seen Grade 4 No epiglottis or glottis structure visible
Airway Review
What might make Direct Laryngoscopy and Intubation more difficult
Inability to open the mouth
Yes No
(yes)Correct
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
(no)Incorrect
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
mohammad reza rajabi
Page 12 432012
Inability to extend the neck
Yes No
(yes)Correct
The sniffing position requires significant neck extension
(no)Incorrect
The sniffing position requires significant neck extension
Inability to breathe through the nose
Yes No
(no)Correct
Unless a nasal intubation is planned
(yes)Incorrect
Unless a nasal intubation is planned
Large tongue
Yes No
(yes)Correct
Also if it is immobile as from radiation therapy
(no)Incorrect
Also if it is immobile as from radiation therapy
Redundant pharyngeal tissue
Yes No
(yes)Correct
This occurs with obesity and is often suggested by a history of
snoring andor obstructive sleep apnea
mohammad reza rajabi
Page 13 432012
(no)Incorrect
This occurs with obesity and is often suggested by a history of snoring andor obstructive sleep apnea
Case 2 Abnormal Exam
A healthy 25-year-old man is scheduled to have a shoulder repair requiring general anesthesia
Lets review his airway examination
What would you like the patient to do
Open his mouth as wide as possible
Extend his neck as far as possible without pain
View from the side
mohammad reza rajabi
Page 14 432012
Open Mouth
This patients mouth opening is 2 finger-breadths the soft palate is
barely visible on maximal mouth opening
Neck
mohammad reza rajabi
Page 15 432012
View from the side
2 finger-breadths fit between the tip of the chin and the neck
Airway Examination
Mouth opening
Normal
Reduced
What is mouth opening
(normal)Incorrect
it is less than 3 finger breadths
mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 4 432012
as it raises the pH of the stomach contents reducing injury to the
lung in the event of an aspiration
(no)Incorrect - Non-particulate antacid
Many would advocate having the patient drink 15-30cc sodium citrate or bicitra within 30 minutes of induction of anesthesia
Though this increases the stomach volume it is actually protective as it raises the pH of the stomach contents reducing injury to the
lung in the event of an aspiration
Administration of H2 blockers
Yes No
(yes)Correct - H2 Blockers
The onset time of these medications is 30+ minutes and even then they do not affect the pH of the volume already in the stomach
However new fluid will be secreted into the stomach at a higher pH perhaps increasing the overall pH by the time of emergence from
anesthesia (the other time at which patients are at risk for aspiration)
(no)Incorrect - H2 Blockers
The onset time of these medications is 30+ minutes and even then they do not affect the pH of the volume already in the stomach
However new fluid will be secreted into the stomach at a higher pH perhaps increasing the overall pH by the time of emergence from
anesthesia (the other time at which patients are at risk for aspiration)
Administration of metoclopramide
Yes No
mohammad reza rajabi
Page 5 432012
(yes)Correct - Metoclopramide
Metoclopramide speeds gastric emptying and increases the lower
esophageal sphincter (LES) pressure While the latter is helpful at reducing the risk of aspiration within minutes stomach volume
reduction takes more time This emptying should occur however
and can reduce the risk of aspiration during emergence and extubation at the end of the operation There are some risks to
metoclopramide so as with everything a riskbenefit evaluation must be performed
(no)Incorrect - Metoclopramide
Metoclopramide speeds gastric emptying and increases the lower esophageal sphincter (LES) pressure While the latter is helpful at
reducing the risk of aspiration within minutes stomach volume reduction takes more time This emptying should occur however
and can reduce the risk of aspiration during emergence and extubation at the end of the operation There are some risks to
metoclopramide so as with everything a riskbenefit evaluation must be performed
Rapid Sequence Induction
Yes No
(yes)Correct - Rapid Sequence Induction
Following pre-oxygenation the patient is put to sleep with a rapid acting IV induction agent such as sodium thiopental immediately
followed by succinylcholine (or other rapid-acting agent) application of cricoid pressure and intubation of the trachea
Positive pressure mask ventilation is not performed to avoid increasing gastric volume The purpose of this technique is to
minimize the duration of impaired gag reflex prior to intubation
Cricoid Pressure during intubation
Yes No
mohammad reza rajabi
Page 6 432012
(no) Incorrect - Cricoid Pressure during Intubation
An assistant identifies the cricoid ring and applies pressure compressing the esophagus against the underlying vertebral
body This prevents passive reflux of gastric contents into the lung How much pressure to apply is a continuing question
current recommendations suggest approximately 10 Newtons (1 kg) of force (mild discomfort for the patient) as the induction
medications are being administered Once the patient loses consciousness the cricoid pressure should be increased to
approximately 30 Newtons (3 kg) It is possible for this pressure to make intubation more difficult and some reduction in force
may be necessary
(yes)Correct - Cricoid Pressure during Intubation
An assistant identifies the cricoid ring and applies pressure compressing the esophagus against the underlying vertebral
body This prevents passive reflux of gastric contents into the lung How much pressure to apply is a continuing question
current recommendations suggest approximately 10 Newtons (1 kg) of force (mild discomfort for the patient) as the induction
medications are being administered Once the patient loses consciousness the cricoid pressure should be increased to
approximately 30 Newtons (3 kg) It is possible for this pressure to make intubation more difficult and some reduction in force
Endotracheal Intubation
Intubation is typically performed under direct visualization That is
by looking through the mouth directly at the vocal cords (direct laryngoscopy) and watching the endotracheal tube pass through the
cords and into the trachea However there is no direct line-of-sight from the mouth to the vocal cords
Check in a mirror or examine a friend (preferably one who has not
eaten onions recently) even with the mouth maximally opened and
tongue extended you cannot see the vocal cords in fact only rarely can you see the epiglottis
mohammad reza rajabi
Page 7 432012
Mallampati Classification
Actually the amount of the posterior pharynx you can visualize is
important and correlates with the difficulty of intubation
Visualization of the pharynx is obscured by a large tongue (relative to the size of the mouth) which also interferes with visualization of
the larynx on laryngoscopy The Mallampati Classification is based on the structures visualized with maximal mouth opening and tongue
protrusion in the sitting position (originally described without phonation but others have suggested minimum Mallampati
Classification with or without phonation best correlates with intubation difficulty)
mohammad reza rajabi
Page 8 432012
Class I soft palate fauces uvula pillars Class II soft palate fauces portion of uvula
Class III soft palate base of uvula Class IV hard palate only
Other Predictors of Difficult Intubation
Obesity ndash body weight gt 110kg
Mouth opening ndash inter-incisor distance lt 4cm in an adult
Ability to prognath ndash a large overbite or the inability to shift
the lower incisors in front of the upper incisors
Thyromental distance ndash The distance from the thyroid cartilage to the mentum (tip of the chin) should be gt 65-7 cm
Mentum-Hyoid distance ndash Similar to thyromental distance and should be at least 3-4 finger-breadths
Many other factors have been investigated with variable results
Other factors that may indicate a difficult intubation
Sternomental distance ndash Similar to above measured from the sternum to the tip of the mandible with the head extended This measure is influenced by neck extension Should be gt125cm
Mandibulohyoid distance ndash the vertical distance between the mandible and the hyoid bone determined radiographically This may be increased with a short mandibular ramus or a caudally located hyoid bone Such an increase in this distance may be associated with difficult intubation Chou 1993
Thyrosternal distance ndash lt8cm may suggest difficulty probably related to the caudally located hyoid as above
mohammad reza rajabi
Page 9 432012
Various radiographic measurements of the cervical spine its alignment with airway structures and the atlanto-occipital joint
Positioning
To obtain a direct line of sight the patient is positioned in the sniffing position The neck is flexed at the lower cervical spine and
extended at the atlanto-occipital joint This flexion and extension is amplified during laryngoscopy
The patientrsquos neck mobility should be assessed preoperatively by
having them flex and extend their head maximally The range of
motion should be more than 90deg Motion less than 80deg may triple the risk of a poor view at laryngoscopy
mohammad reza rajabi
Page 10 432012
Direct Laryngoscopy
Then a laryngoscope is used to pull the lower jaw and tongue up and out of the way
The metal blade is passed into the mouth to the level of the epiglottis then with an anterior and caudad motion (ie toward the
edge of the ceiling across the room) the lower jaw is elevated allowing visualization of the glottic structures( The glottis is the
structures of phonation including the vocal cords and surrounding structures) In most patients this results in a clear view of the larynx
and the endotracheal tube is passed through the vocal cords under
direct visualization
mohammad reza rajabi
Page 11 432012
Laryngoscopy Grades
In most patients Direct Laryngoscopy results in a clear view of the larynx The laryngeal view has been classified by Cormack and
Lehane as follows
Grade 1 Full view of the glottis Grade 2 Only the posterior commissure is visible
Grade 3 Only the epiglottis is seen Grade 4 No epiglottis or glottis structure visible
Airway Review
What might make Direct Laryngoscopy and Intubation more difficult
Inability to open the mouth
Yes No
(yes)Correct
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
(no)Incorrect
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
mohammad reza rajabi
Page 12 432012
Inability to extend the neck
Yes No
(yes)Correct
The sniffing position requires significant neck extension
(no)Incorrect
The sniffing position requires significant neck extension
Inability to breathe through the nose
Yes No
(no)Correct
Unless a nasal intubation is planned
(yes)Incorrect
Unless a nasal intubation is planned
Large tongue
Yes No
(yes)Correct
Also if it is immobile as from radiation therapy
(no)Incorrect
Also if it is immobile as from radiation therapy
Redundant pharyngeal tissue
Yes No
(yes)Correct
This occurs with obesity and is often suggested by a history of
snoring andor obstructive sleep apnea
mohammad reza rajabi
Page 13 432012
(no)Incorrect
This occurs with obesity and is often suggested by a history of snoring andor obstructive sleep apnea
Case 2 Abnormal Exam
A healthy 25-year-old man is scheduled to have a shoulder repair requiring general anesthesia
Lets review his airway examination
What would you like the patient to do
Open his mouth as wide as possible
Extend his neck as far as possible without pain
View from the side
mohammad reza rajabi
Page 14 432012
Open Mouth
This patients mouth opening is 2 finger-breadths the soft palate is
barely visible on maximal mouth opening
Neck
mohammad reza rajabi
Page 15 432012
View from the side
2 finger-breadths fit between the tip of the chin and the neck
Airway Examination
Mouth opening
Normal
Reduced
What is mouth opening
(normal)Incorrect
it is less than 3 finger breadths
mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 5 432012
(yes)Correct - Metoclopramide
Metoclopramide speeds gastric emptying and increases the lower
esophageal sphincter (LES) pressure While the latter is helpful at reducing the risk of aspiration within minutes stomach volume
reduction takes more time This emptying should occur however
and can reduce the risk of aspiration during emergence and extubation at the end of the operation There are some risks to
metoclopramide so as with everything a riskbenefit evaluation must be performed
(no)Incorrect - Metoclopramide
Metoclopramide speeds gastric emptying and increases the lower esophageal sphincter (LES) pressure While the latter is helpful at
reducing the risk of aspiration within minutes stomach volume reduction takes more time This emptying should occur however
and can reduce the risk of aspiration during emergence and extubation at the end of the operation There are some risks to
metoclopramide so as with everything a riskbenefit evaluation must be performed
Rapid Sequence Induction
Yes No
(yes)Correct - Rapid Sequence Induction
Following pre-oxygenation the patient is put to sleep with a rapid acting IV induction agent such as sodium thiopental immediately
followed by succinylcholine (or other rapid-acting agent) application of cricoid pressure and intubation of the trachea
Positive pressure mask ventilation is not performed to avoid increasing gastric volume The purpose of this technique is to
minimize the duration of impaired gag reflex prior to intubation
Cricoid Pressure during intubation
Yes No
mohammad reza rajabi
Page 6 432012
(no) Incorrect - Cricoid Pressure during Intubation
An assistant identifies the cricoid ring and applies pressure compressing the esophagus against the underlying vertebral
body This prevents passive reflux of gastric contents into the lung How much pressure to apply is a continuing question
current recommendations suggest approximately 10 Newtons (1 kg) of force (mild discomfort for the patient) as the induction
medications are being administered Once the patient loses consciousness the cricoid pressure should be increased to
approximately 30 Newtons (3 kg) It is possible for this pressure to make intubation more difficult and some reduction in force
may be necessary
(yes)Correct - Cricoid Pressure during Intubation
An assistant identifies the cricoid ring and applies pressure compressing the esophagus against the underlying vertebral
body This prevents passive reflux of gastric contents into the lung How much pressure to apply is a continuing question
current recommendations suggest approximately 10 Newtons (1 kg) of force (mild discomfort for the patient) as the induction
medications are being administered Once the patient loses consciousness the cricoid pressure should be increased to
approximately 30 Newtons (3 kg) It is possible for this pressure to make intubation more difficult and some reduction in force
Endotracheal Intubation
Intubation is typically performed under direct visualization That is
by looking through the mouth directly at the vocal cords (direct laryngoscopy) and watching the endotracheal tube pass through the
cords and into the trachea However there is no direct line-of-sight from the mouth to the vocal cords
Check in a mirror or examine a friend (preferably one who has not
eaten onions recently) even with the mouth maximally opened and
tongue extended you cannot see the vocal cords in fact only rarely can you see the epiglottis
mohammad reza rajabi
Page 7 432012
Mallampati Classification
Actually the amount of the posterior pharynx you can visualize is
important and correlates with the difficulty of intubation
Visualization of the pharynx is obscured by a large tongue (relative to the size of the mouth) which also interferes with visualization of
the larynx on laryngoscopy The Mallampati Classification is based on the structures visualized with maximal mouth opening and tongue
protrusion in the sitting position (originally described without phonation but others have suggested minimum Mallampati
Classification with or without phonation best correlates with intubation difficulty)
mohammad reza rajabi
Page 8 432012
Class I soft palate fauces uvula pillars Class II soft palate fauces portion of uvula
Class III soft palate base of uvula Class IV hard palate only
Other Predictors of Difficult Intubation
Obesity ndash body weight gt 110kg
Mouth opening ndash inter-incisor distance lt 4cm in an adult
Ability to prognath ndash a large overbite or the inability to shift
the lower incisors in front of the upper incisors
Thyromental distance ndash The distance from the thyroid cartilage to the mentum (tip of the chin) should be gt 65-7 cm
Mentum-Hyoid distance ndash Similar to thyromental distance and should be at least 3-4 finger-breadths
Many other factors have been investigated with variable results
Other factors that may indicate a difficult intubation
Sternomental distance ndash Similar to above measured from the sternum to the tip of the mandible with the head extended This measure is influenced by neck extension Should be gt125cm
Mandibulohyoid distance ndash the vertical distance between the mandible and the hyoid bone determined radiographically This may be increased with a short mandibular ramus or a caudally located hyoid bone Such an increase in this distance may be associated with difficult intubation Chou 1993
Thyrosternal distance ndash lt8cm may suggest difficulty probably related to the caudally located hyoid as above
mohammad reza rajabi
Page 9 432012
Various radiographic measurements of the cervical spine its alignment with airway structures and the atlanto-occipital joint
Positioning
To obtain a direct line of sight the patient is positioned in the sniffing position The neck is flexed at the lower cervical spine and
extended at the atlanto-occipital joint This flexion and extension is amplified during laryngoscopy
The patientrsquos neck mobility should be assessed preoperatively by
having them flex and extend their head maximally The range of
motion should be more than 90deg Motion less than 80deg may triple the risk of a poor view at laryngoscopy
mohammad reza rajabi
Page 10 432012
Direct Laryngoscopy
Then a laryngoscope is used to pull the lower jaw and tongue up and out of the way
The metal blade is passed into the mouth to the level of the epiglottis then with an anterior and caudad motion (ie toward the
edge of the ceiling across the room) the lower jaw is elevated allowing visualization of the glottic structures( The glottis is the
structures of phonation including the vocal cords and surrounding structures) In most patients this results in a clear view of the larynx
and the endotracheal tube is passed through the vocal cords under
direct visualization
mohammad reza rajabi
Page 11 432012
Laryngoscopy Grades
In most patients Direct Laryngoscopy results in a clear view of the larynx The laryngeal view has been classified by Cormack and
Lehane as follows
Grade 1 Full view of the glottis Grade 2 Only the posterior commissure is visible
Grade 3 Only the epiglottis is seen Grade 4 No epiglottis or glottis structure visible
Airway Review
What might make Direct Laryngoscopy and Intubation more difficult
Inability to open the mouth
Yes No
(yes)Correct
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
(no)Incorrect
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
mohammad reza rajabi
Page 12 432012
Inability to extend the neck
Yes No
(yes)Correct
The sniffing position requires significant neck extension
(no)Incorrect
The sniffing position requires significant neck extension
Inability to breathe through the nose
Yes No
(no)Correct
Unless a nasal intubation is planned
(yes)Incorrect
Unless a nasal intubation is planned
Large tongue
Yes No
(yes)Correct
Also if it is immobile as from radiation therapy
(no)Incorrect
Also if it is immobile as from radiation therapy
Redundant pharyngeal tissue
Yes No
(yes)Correct
This occurs with obesity and is often suggested by a history of
snoring andor obstructive sleep apnea
mohammad reza rajabi
Page 13 432012
(no)Incorrect
This occurs with obesity and is often suggested by a history of snoring andor obstructive sleep apnea
Case 2 Abnormal Exam
A healthy 25-year-old man is scheduled to have a shoulder repair requiring general anesthesia
Lets review his airway examination
What would you like the patient to do
Open his mouth as wide as possible
Extend his neck as far as possible without pain
View from the side
mohammad reza rajabi
Page 14 432012
Open Mouth
This patients mouth opening is 2 finger-breadths the soft palate is
barely visible on maximal mouth opening
Neck
mohammad reza rajabi
Page 15 432012
View from the side
2 finger-breadths fit between the tip of the chin and the neck
Airway Examination
Mouth opening
Normal
Reduced
What is mouth opening
(normal)Incorrect
it is less than 3 finger breadths
mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 6 432012
(no) Incorrect - Cricoid Pressure during Intubation
An assistant identifies the cricoid ring and applies pressure compressing the esophagus against the underlying vertebral
body This prevents passive reflux of gastric contents into the lung How much pressure to apply is a continuing question
current recommendations suggest approximately 10 Newtons (1 kg) of force (mild discomfort for the patient) as the induction
medications are being administered Once the patient loses consciousness the cricoid pressure should be increased to
approximately 30 Newtons (3 kg) It is possible for this pressure to make intubation more difficult and some reduction in force
may be necessary
(yes)Correct - Cricoid Pressure during Intubation
An assistant identifies the cricoid ring and applies pressure compressing the esophagus against the underlying vertebral
body This prevents passive reflux of gastric contents into the lung How much pressure to apply is a continuing question
current recommendations suggest approximately 10 Newtons (1 kg) of force (mild discomfort for the patient) as the induction
medications are being administered Once the patient loses consciousness the cricoid pressure should be increased to
approximately 30 Newtons (3 kg) It is possible for this pressure to make intubation more difficult and some reduction in force
Endotracheal Intubation
Intubation is typically performed under direct visualization That is
by looking through the mouth directly at the vocal cords (direct laryngoscopy) and watching the endotracheal tube pass through the
cords and into the trachea However there is no direct line-of-sight from the mouth to the vocal cords
Check in a mirror or examine a friend (preferably one who has not
eaten onions recently) even with the mouth maximally opened and
tongue extended you cannot see the vocal cords in fact only rarely can you see the epiglottis
mohammad reza rajabi
Page 7 432012
Mallampati Classification
Actually the amount of the posterior pharynx you can visualize is
important and correlates with the difficulty of intubation
Visualization of the pharynx is obscured by a large tongue (relative to the size of the mouth) which also interferes with visualization of
the larynx on laryngoscopy The Mallampati Classification is based on the structures visualized with maximal mouth opening and tongue
protrusion in the sitting position (originally described without phonation but others have suggested minimum Mallampati
Classification with or without phonation best correlates with intubation difficulty)
mohammad reza rajabi
Page 8 432012
Class I soft palate fauces uvula pillars Class II soft palate fauces portion of uvula
Class III soft palate base of uvula Class IV hard palate only
Other Predictors of Difficult Intubation
Obesity ndash body weight gt 110kg
Mouth opening ndash inter-incisor distance lt 4cm in an adult
Ability to prognath ndash a large overbite or the inability to shift
the lower incisors in front of the upper incisors
Thyromental distance ndash The distance from the thyroid cartilage to the mentum (tip of the chin) should be gt 65-7 cm
Mentum-Hyoid distance ndash Similar to thyromental distance and should be at least 3-4 finger-breadths
Many other factors have been investigated with variable results
Other factors that may indicate a difficult intubation
Sternomental distance ndash Similar to above measured from the sternum to the tip of the mandible with the head extended This measure is influenced by neck extension Should be gt125cm
Mandibulohyoid distance ndash the vertical distance between the mandible and the hyoid bone determined radiographically This may be increased with a short mandibular ramus or a caudally located hyoid bone Such an increase in this distance may be associated with difficult intubation Chou 1993
Thyrosternal distance ndash lt8cm may suggest difficulty probably related to the caudally located hyoid as above
mohammad reza rajabi
Page 9 432012
Various radiographic measurements of the cervical spine its alignment with airway structures and the atlanto-occipital joint
Positioning
To obtain a direct line of sight the patient is positioned in the sniffing position The neck is flexed at the lower cervical spine and
extended at the atlanto-occipital joint This flexion and extension is amplified during laryngoscopy
The patientrsquos neck mobility should be assessed preoperatively by
having them flex and extend their head maximally The range of
motion should be more than 90deg Motion less than 80deg may triple the risk of a poor view at laryngoscopy
mohammad reza rajabi
Page 10 432012
Direct Laryngoscopy
Then a laryngoscope is used to pull the lower jaw and tongue up and out of the way
The metal blade is passed into the mouth to the level of the epiglottis then with an anterior and caudad motion (ie toward the
edge of the ceiling across the room) the lower jaw is elevated allowing visualization of the glottic structures( The glottis is the
structures of phonation including the vocal cords and surrounding structures) In most patients this results in a clear view of the larynx
and the endotracheal tube is passed through the vocal cords under
direct visualization
mohammad reza rajabi
Page 11 432012
Laryngoscopy Grades
In most patients Direct Laryngoscopy results in a clear view of the larynx The laryngeal view has been classified by Cormack and
Lehane as follows
Grade 1 Full view of the glottis Grade 2 Only the posterior commissure is visible
Grade 3 Only the epiglottis is seen Grade 4 No epiglottis or glottis structure visible
Airway Review
What might make Direct Laryngoscopy and Intubation more difficult
Inability to open the mouth
Yes No
(yes)Correct
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
(no)Incorrect
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
mohammad reza rajabi
Page 12 432012
Inability to extend the neck
Yes No
(yes)Correct
The sniffing position requires significant neck extension
(no)Incorrect
The sniffing position requires significant neck extension
Inability to breathe through the nose
Yes No
(no)Correct
Unless a nasal intubation is planned
(yes)Incorrect
Unless a nasal intubation is planned
Large tongue
Yes No
(yes)Correct
Also if it is immobile as from radiation therapy
(no)Incorrect
Also if it is immobile as from radiation therapy
Redundant pharyngeal tissue
Yes No
(yes)Correct
This occurs with obesity and is often suggested by a history of
snoring andor obstructive sleep apnea
mohammad reza rajabi
Page 13 432012
(no)Incorrect
This occurs with obesity and is often suggested by a history of snoring andor obstructive sleep apnea
Case 2 Abnormal Exam
A healthy 25-year-old man is scheduled to have a shoulder repair requiring general anesthesia
Lets review his airway examination
What would you like the patient to do
Open his mouth as wide as possible
Extend his neck as far as possible without pain
View from the side
mohammad reza rajabi
Page 14 432012
Open Mouth
This patients mouth opening is 2 finger-breadths the soft palate is
barely visible on maximal mouth opening
Neck
mohammad reza rajabi
Page 15 432012
View from the side
2 finger-breadths fit between the tip of the chin and the neck
Airway Examination
Mouth opening
Normal
Reduced
What is mouth opening
(normal)Incorrect
it is less than 3 finger breadths
mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 7 432012
Mallampati Classification
Actually the amount of the posterior pharynx you can visualize is
important and correlates with the difficulty of intubation
Visualization of the pharynx is obscured by a large tongue (relative to the size of the mouth) which also interferes with visualization of
the larynx on laryngoscopy The Mallampati Classification is based on the structures visualized with maximal mouth opening and tongue
protrusion in the sitting position (originally described without phonation but others have suggested minimum Mallampati
Classification with or without phonation best correlates with intubation difficulty)
mohammad reza rajabi
Page 8 432012
Class I soft palate fauces uvula pillars Class II soft palate fauces portion of uvula
Class III soft palate base of uvula Class IV hard palate only
Other Predictors of Difficult Intubation
Obesity ndash body weight gt 110kg
Mouth opening ndash inter-incisor distance lt 4cm in an adult
Ability to prognath ndash a large overbite or the inability to shift
the lower incisors in front of the upper incisors
Thyromental distance ndash The distance from the thyroid cartilage to the mentum (tip of the chin) should be gt 65-7 cm
Mentum-Hyoid distance ndash Similar to thyromental distance and should be at least 3-4 finger-breadths
Many other factors have been investigated with variable results
Other factors that may indicate a difficult intubation
Sternomental distance ndash Similar to above measured from the sternum to the tip of the mandible with the head extended This measure is influenced by neck extension Should be gt125cm
Mandibulohyoid distance ndash the vertical distance between the mandible and the hyoid bone determined radiographically This may be increased with a short mandibular ramus or a caudally located hyoid bone Such an increase in this distance may be associated with difficult intubation Chou 1993
Thyrosternal distance ndash lt8cm may suggest difficulty probably related to the caudally located hyoid as above
mohammad reza rajabi
Page 9 432012
Various radiographic measurements of the cervical spine its alignment with airway structures and the atlanto-occipital joint
Positioning
To obtain a direct line of sight the patient is positioned in the sniffing position The neck is flexed at the lower cervical spine and
extended at the atlanto-occipital joint This flexion and extension is amplified during laryngoscopy
The patientrsquos neck mobility should be assessed preoperatively by
having them flex and extend their head maximally The range of
motion should be more than 90deg Motion less than 80deg may triple the risk of a poor view at laryngoscopy
mohammad reza rajabi
Page 10 432012
Direct Laryngoscopy
Then a laryngoscope is used to pull the lower jaw and tongue up and out of the way
The metal blade is passed into the mouth to the level of the epiglottis then with an anterior and caudad motion (ie toward the
edge of the ceiling across the room) the lower jaw is elevated allowing visualization of the glottic structures( The glottis is the
structures of phonation including the vocal cords and surrounding structures) In most patients this results in a clear view of the larynx
and the endotracheal tube is passed through the vocal cords under
direct visualization
mohammad reza rajabi
Page 11 432012
Laryngoscopy Grades
In most patients Direct Laryngoscopy results in a clear view of the larynx The laryngeal view has been classified by Cormack and
Lehane as follows
Grade 1 Full view of the glottis Grade 2 Only the posterior commissure is visible
Grade 3 Only the epiglottis is seen Grade 4 No epiglottis or glottis structure visible
Airway Review
What might make Direct Laryngoscopy and Intubation more difficult
Inability to open the mouth
Yes No
(yes)Correct
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
(no)Incorrect
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
mohammad reza rajabi
Page 12 432012
Inability to extend the neck
Yes No
(yes)Correct
The sniffing position requires significant neck extension
(no)Incorrect
The sniffing position requires significant neck extension
Inability to breathe through the nose
Yes No
(no)Correct
Unless a nasal intubation is planned
(yes)Incorrect
Unless a nasal intubation is planned
Large tongue
Yes No
(yes)Correct
Also if it is immobile as from radiation therapy
(no)Incorrect
Also if it is immobile as from radiation therapy
Redundant pharyngeal tissue
Yes No
(yes)Correct
This occurs with obesity and is often suggested by a history of
snoring andor obstructive sleep apnea
mohammad reza rajabi
Page 13 432012
(no)Incorrect
This occurs with obesity and is often suggested by a history of snoring andor obstructive sleep apnea
Case 2 Abnormal Exam
A healthy 25-year-old man is scheduled to have a shoulder repair requiring general anesthesia
Lets review his airway examination
What would you like the patient to do
Open his mouth as wide as possible
Extend his neck as far as possible without pain
View from the side
mohammad reza rajabi
Page 14 432012
Open Mouth
This patients mouth opening is 2 finger-breadths the soft palate is
barely visible on maximal mouth opening
Neck
mohammad reza rajabi
Page 15 432012
View from the side
2 finger-breadths fit between the tip of the chin and the neck
Airway Examination
Mouth opening
Normal
Reduced
What is mouth opening
(normal)Incorrect
it is less than 3 finger breadths
mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 8 432012
Class I soft palate fauces uvula pillars Class II soft palate fauces portion of uvula
Class III soft palate base of uvula Class IV hard palate only
Other Predictors of Difficult Intubation
Obesity ndash body weight gt 110kg
Mouth opening ndash inter-incisor distance lt 4cm in an adult
Ability to prognath ndash a large overbite or the inability to shift
the lower incisors in front of the upper incisors
Thyromental distance ndash The distance from the thyroid cartilage to the mentum (tip of the chin) should be gt 65-7 cm
Mentum-Hyoid distance ndash Similar to thyromental distance and should be at least 3-4 finger-breadths
Many other factors have been investigated with variable results
Other factors that may indicate a difficult intubation
Sternomental distance ndash Similar to above measured from the sternum to the tip of the mandible with the head extended This measure is influenced by neck extension Should be gt125cm
Mandibulohyoid distance ndash the vertical distance between the mandible and the hyoid bone determined radiographically This may be increased with a short mandibular ramus or a caudally located hyoid bone Such an increase in this distance may be associated with difficult intubation Chou 1993
Thyrosternal distance ndash lt8cm may suggest difficulty probably related to the caudally located hyoid as above
mohammad reza rajabi
Page 9 432012
Various radiographic measurements of the cervical spine its alignment with airway structures and the atlanto-occipital joint
Positioning
To obtain a direct line of sight the patient is positioned in the sniffing position The neck is flexed at the lower cervical spine and
extended at the atlanto-occipital joint This flexion and extension is amplified during laryngoscopy
The patientrsquos neck mobility should be assessed preoperatively by
having them flex and extend their head maximally The range of
motion should be more than 90deg Motion less than 80deg may triple the risk of a poor view at laryngoscopy
mohammad reza rajabi
Page 10 432012
Direct Laryngoscopy
Then a laryngoscope is used to pull the lower jaw and tongue up and out of the way
The metal blade is passed into the mouth to the level of the epiglottis then with an anterior and caudad motion (ie toward the
edge of the ceiling across the room) the lower jaw is elevated allowing visualization of the glottic structures( The glottis is the
structures of phonation including the vocal cords and surrounding structures) In most patients this results in a clear view of the larynx
and the endotracheal tube is passed through the vocal cords under
direct visualization
mohammad reza rajabi
Page 11 432012
Laryngoscopy Grades
In most patients Direct Laryngoscopy results in a clear view of the larynx The laryngeal view has been classified by Cormack and
Lehane as follows
Grade 1 Full view of the glottis Grade 2 Only the posterior commissure is visible
Grade 3 Only the epiglottis is seen Grade 4 No epiglottis or glottis structure visible
Airway Review
What might make Direct Laryngoscopy and Intubation more difficult
Inability to open the mouth
Yes No
(yes)Correct
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
(no)Incorrect
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
mohammad reza rajabi
Page 12 432012
Inability to extend the neck
Yes No
(yes)Correct
The sniffing position requires significant neck extension
(no)Incorrect
The sniffing position requires significant neck extension
Inability to breathe through the nose
Yes No
(no)Correct
Unless a nasal intubation is planned
(yes)Incorrect
Unless a nasal intubation is planned
Large tongue
Yes No
(yes)Correct
Also if it is immobile as from radiation therapy
(no)Incorrect
Also if it is immobile as from radiation therapy
Redundant pharyngeal tissue
Yes No
(yes)Correct
This occurs with obesity and is often suggested by a history of
snoring andor obstructive sleep apnea
mohammad reza rajabi
Page 13 432012
(no)Incorrect
This occurs with obesity and is often suggested by a history of snoring andor obstructive sleep apnea
Case 2 Abnormal Exam
A healthy 25-year-old man is scheduled to have a shoulder repair requiring general anesthesia
Lets review his airway examination
What would you like the patient to do
Open his mouth as wide as possible
Extend his neck as far as possible without pain
View from the side
mohammad reza rajabi
Page 14 432012
Open Mouth
This patients mouth opening is 2 finger-breadths the soft palate is
barely visible on maximal mouth opening
Neck
mohammad reza rajabi
Page 15 432012
View from the side
2 finger-breadths fit between the tip of the chin and the neck
Airway Examination
Mouth opening
Normal
Reduced
What is mouth opening
(normal)Incorrect
it is less than 3 finger breadths
mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 9 432012
Various radiographic measurements of the cervical spine its alignment with airway structures and the atlanto-occipital joint
Positioning
To obtain a direct line of sight the patient is positioned in the sniffing position The neck is flexed at the lower cervical spine and
extended at the atlanto-occipital joint This flexion and extension is amplified during laryngoscopy
The patientrsquos neck mobility should be assessed preoperatively by
having them flex and extend their head maximally The range of
motion should be more than 90deg Motion less than 80deg may triple the risk of a poor view at laryngoscopy
mohammad reza rajabi
Page 10 432012
Direct Laryngoscopy
Then a laryngoscope is used to pull the lower jaw and tongue up and out of the way
The metal blade is passed into the mouth to the level of the epiglottis then with an anterior and caudad motion (ie toward the
edge of the ceiling across the room) the lower jaw is elevated allowing visualization of the glottic structures( The glottis is the
structures of phonation including the vocal cords and surrounding structures) In most patients this results in a clear view of the larynx
and the endotracheal tube is passed through the vocal cords under
direct visualization
mohammad reza rajabi
Page 11 432012
Laryngoscopy Grades
In most patients Direct Laryngoscopy results in a clear view of the larynx The laryngeal view has been classified by Cormack and
Lehane as follows
Grade 1 Full view of the glottis Grade 2 Only the posterior commissure is visible
Grade 3 Only the epiglottis is seen Grade 4 No epiglottis or glottis structure visible
Airway Review
What might make Direct Laryngoscopy and Intubation more difficult
Inability to open the mouth
Yes No
(yes)Correct
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
(no)Incorrect
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
mohammad reza rajabi
Page 12 432012
Inability to extend the neck
Yes No
(yes)Correct
The sniffing position requires significant neck extension
(no)Incorrect
The sniffing position requires significant neck extension
Inability to breathe through the nose
Yes No
(no)Correct
Unless a nasal intubation is planned
(yes)Incorrect
Unless a nasal intubation is planned
Large tongue
Yes No
(yes)Correct
Also if it is immobile as from radiation therapy
(no)Incorrect
Also if it is immobile as from radiation therapy
Redundant pharyngeal tissue
Yes No
(yes)Correct
This occurs with obesity and is often suggested by a history of
snoring andor obstructive sleep apnea
mohammad reza rajabi
Page 13 432012
(no)Incorrect
This occurs with obesity and is often suggested by a history of snoring andor obstructive sleep apnea
Case 2 Abnormal Exam
A healthy 25-year-old man is scheduled to have a shoulder repair requiring general anesthesia
Lets review his airway examination
What would you like the patient to do
Open his mouth as wide as possible
Extend his neck as far as possible without pain
View from the side
mohammad reza rajabi
Page 14 432012
Open Mouth
This patients mouth opening is 2 finger-breadths the soft palate is
barely visible on maximal mouth opening
Neck
mohammad reza rajabi
Page 15 432012
View from the side
2 finger-breadths fit between the tip of the chin and the neck
Airway Examination
Mouth opening
Normal
Reduced
What is mouth opening
(normal)Incorrect
it is less than 3 finger breadths
mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 10 432012
Direct Laryngoscopy
Then a laryngoscope is used to pull the lower jaw and tongue up and out of the way
The metal blade is passed into the mouth to the level of the epiglottis then with an anterior and caudad motion (ie toward the
edge of the ceiling across the room) the lower jaw is elevated allowing visualization of the glottic structures( The glottis is the
structures of phonation including the vocal cords and surrounding structures) In most patients this results in a clear view of the larynx
and the endotracheal tube is passed through the vocal cords under
direct visualization
mohammad reza rajabi
Page 11 432012
Laryngoscopy Grades
In most patients Direct Laryngoscopy results in a clear view of the larynx The laryngeal view has been classified by Cormack and
Lehane as follows
Grade 1 Full view of the glottis Grade 2 Only the posterior commissure is visible
Grade 3 Only the epiglottis is seen Grade 4 No epiglottis or glottis structure visible
Airway Review
What might make Direct Laryngoscopy and Intubation more difficult
Inability to open the mouth
Yes No
(yes)Correct
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
(no)Incorrect
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
mohammad reza rajabi
Page 12 432012
Inability to extend the neck
Yes No
(yes)Correct
The sniffing position requires significant neck extension
(no)Incorrect
The sniffing position requires significant neck extension
Inability to breathe through the nose
Yes No
(no)Correct
Unless a nasal intubation is planned
(yes)Incorrect
Unless a nasal intubation is planned
Large tongue
Yes No
(yes)Correct
Also if it is immobile as from radiation therapy
(no)Incorrect
Also if it is immobile as from radiation therapy
Redundant pharyngeal tissue
Yes No
(yes)Correct
This occurs with obesity and is often suggested by a history of
snoring andor obstructive sleep apnea
mohammad reza rajabi
Page 13 432012
(no)Incorrect
This occurs with obesity and is often suggested by a history of snoring andor obstructive sleep apnea
Case 2 Abnormal Exam
A healthy 25-year-old man is scheduled to have a shoulder repair requiring general anesthesia
Lets review his airway examination
What would you like the patient to do
Open his mouth as wide as possible
Extend his neck as far as possible without pain
View from the side
mohammad reza rajabi
Page 14 432012
Open Mouth
This patients mouth opening is 2 finger-breadths the soft palate is
barely visible on maximal mouth opening
Neck
mohammad reza rajabi
Page 15 432012
View from the side
2 finger-breadths fit between the tip of the chin and the neck
Airway Examination
Mouth opening
Normal
Reduced
What is mouth opening
(normal)Incorrect
it is less than 3 finger breadths
mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 11 432012
Laryngoscopy Grades
In most patients Direct Laryngoscopy results in a clear view of the larynx The laryngeal view has been classified by Cormack and
Lehane as follows
Grade 1 Full view of the glottis Grade 2 Only the posterior commissure is visible
Grade 3 Only the epiglottis is seen Grade 4 No epiglottis or glottis structure visible
Airway Review
What might make Direct Laryngoscopy and Intubation more difficult
Inability to open the mouth
Yes No
(yes)Correct
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
(no)Incorrect
There must be room to place the laryngoscope in the mouthhellipusually
at least 3 finger breadths in the adult
mohammad reza rajabi
Page 12 432012
Inability to extend the neck
Yes No
(yes)Correct
The sniffing position requires significant neck extension
(no)Incorrect
The sniffing position requires significant neck extension
Inability to breathe through the nose
Yes No
(no)Correct
Unless a nasal intubation is planned
(yes)Incorrect
Unless a nasal intubation is planned
Large tongue
Yes No
(yes)Correct
Also if it is immobile as from radiation therapy
(no)Incorrect
Also if it is immobile as from radiation therapy
Redundant pharyngeal tissue
Yes No
(yes)Correct
This occurs with obesity and is often suggested by a history of
snoring andor obstructive sleep apnea
mohammad reza rajabi
Page 13 432012
(no)Incorrect
This occurs with obesity and is often suggested by a history of snoring andor obstructive sleep apnea
Case 2 Abnormal Exam
A healthy 25-year-old man is scheduled to have a shoulder repair requiring general anesthesia
Lets review his airway examination
What would you like the patient to do
Open his mouth as wide as possible
Extend his neck as far as possible without pain
View from the side
mohammad reza rajabi
Page 14 432012
Open Mouth
This patients mouth opening is 2 finger-breadths the soft palate is
barely visible on maximal mouth opening
Neck
mohammad reza rajabi
Page 15 432012
View from the side
2 finger-breadths fit between the tip of the chin and the neck
Airway Examination
Mouth opening
Normal
Reduced
What is mouth opening
(normal)Incorrect
it is less than 3 finger breadths
mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 12 432012
Inability to extend the neck
Yes No
(yes)Correct
The sniffing position requires significant neck extension
(no)Incorrect
The sniffing position requires significant neck extension
Inability to breathe through the nose
Yes No
(no)Correct
Unless a nasal intubation is planned
(yes)Incorrect
Unless a nasal intubation is planned
Large tongue
Yes No
(yes)Correct
Also if it is immobile as from radiation therapy
(no)Incorrect
Also if it is immobile as from radiation therapy
Redundant pharyngeal tissue
Yes No
(yes)Correct
This occurs with obesity and is often suggested by a history of
snoring andor obstructive sleep apnea
mohammad reza rajabi
Page 13 432012
(no)Incorrect
This occurs with obesity and is often suggested by a history of snoring andor obstructive sleep apnea
Case 2 Abnormal Exam
A healthy 25-year-old man is scheduled to have a shoulder repair requiring general anesthesia
Lets review his airway examination
What would you like the patient to do
Open his mouth as wide as possible
Extend his neck as far as possible without pain
View from the side
mohammad reza rajabi
Page 14 432012
Open Mouth
This patients mouth opening is 2 finger-breadths the soft palate is
barely visible on maximal mouth opening
Neck
mohammad reza rajabi
Page 15 432012
View from the side
2 finger-breadths fit between the tip of the chin and the neck
Airway Examination
Mouth opening
Normal
Reduced
What is mouth opening
(normal)Incorrect
it is less than 3 finger breadths
mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 13 432012
(no)Incorrect
This occurs with obesity and is often suggested by a history of snoring andor obstructive sleep apnea
Case 2 Abnormal Exam
A healthy 25-year-old man is scheduled to have a shoulder repair requiring general anesthesia
Lets review his airway examination
What would you like the patient to do
Open his mouth as wide as possible
Extend his neck as far as possible without pain
View from the side
mohammad reza rajabi
Page 14 432012
Open Mouth
This patients mouth opening is 2 finger-breadths the soft palate is
barely visible on maximal mouth opening
Neck
mohammad reza rajabi
Page 15 432012
View from the side
2 finger-breadths fit between the tip of the chin and the neck
Airway Examination
Mouth opening
Normal
Reduced
What is mouth opening
(normal)Incorrect
it is less than 3 finger breadths
mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 14 432012
Open Mouth
This patients mouth opening is 2 finger-breadths the soft palate is
barely visible on maximal mouth opening
Neck
mohammad reza rajabi
Page 15 432012
View from the side
2 finger-breadths fit between the tip of the chin and the neck
Airway Examination
Mouth opening
Normal
Reduced
What is mouth opening
(normal)Incorrect
it is less than 3 finger breadths
mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 15 432012
View from the side
2 finger-breadths fit between the tip of the chin and the neck
Airway Examination
Mouth opening
Normal
Reduced
What is mouth opening
(normal)Incorrect
it is less than 3 finger breadths
mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 16 432012
(reduced)Correct
The mouth opening is less than 3 finger-breadths
Open Mouth
The inter-incisor distance on maximal mouth opening Should be gt4 cm in an adult or 3-4 of the patients finger-breadths
This patients mouth opening is 2 finger breadths the soft palate is barely visible on maximal mouth opening
Mallampati Score
I
II
III
IV
What is Mallampati Score
mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 17 432012
(I)Incorrect
The uvula cannot be seen
(II)Incorrect
Not even the top of the uvula is visible
(III)Yes
All structures visible up to the soft palate is a Mallampati Class III
(IV)Incorrect
The soft palate is visible
Mentum-Hyoid distance
Normal
Reduced
What distance
(normal)Incorrect
3 finger-breadths is normal this patient has only 2
(reduced)Yes
this is less than the normal 3 finger-breadths
View from the side
2 finger-breadths fit between the tip of the chin and the neck
mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 18 432012
Neck Extension
Normal
Reduced
What is neck extension
(normal)Correct
The neck extends
(reduced)Incorrect
The neck motion is gt 90 degrees
Neck
The range of motion should be more than 90deg Motion less than 80deg may triple the risk
of a poor view at laryngoscopy
Airway Evaluation Summary
Because of the reduced mentum-hyoid distance it may be difficult to visualize the larynx with traditional direct laryngoscopy There are
other options including other blades and techniques that do not require a direct line-of-sight which are beyond the scope of this site
Perhaps the most conservative method of securing the airway of a
patient who is anticipated to have a difficult airway is with awake
fiberoptic intubation This technique requires substantial skill but allows intubation in an awake spontaneously breathing patient The
trachea is identified with a flexible fiberscope and then the endotracheal tube is advanced over the fiberscope like a stylet Such
mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 19 432012
a procedure requires blockade of the sensory innervation to the
airway and blunting of the gag reflex
Innervation of the Upper Airway
Awake fiberoptic intubation requires topical anesthesia for patient
comfort as well as to blunt the gag reflex that would prevent successful intubation of the trachea
Several nerves are involved in the sensation of the upper airway
Anterior 23 of the tongue - Trigeminal nerve (V)
Posterior 13 of tongue to epiglottis - Glossopharyngeal nerve (IX afferent limb of gag reflex)
Epiglottis to vocal cords - Internal branch of Superior Laryngeal Nerve (Vagus X)
mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 20 432012
Trachea below vocal cords - Recurrent Laryngeal Nerve
(Vagus X)
MOTOR INNERVATION
Motor innervation to the larynx is provided by the Vagus Nerve but recall there are two branches involved The Recurrent Laryngeal
Nerve innervates all the muscles of the larynx EXCEPT the
cricothyroid muscle which is innervated by the External Branch of the Superior Laryngeal Nerve Because the function of the
cricothyroid muscle is to stretch and tense the vocal cords unopposed action of the cricothyroid as may occur with bilateral
destruction of the recurrent laryngeal nerves would lead to stridor respiratory distress and possibly airway obstruction
GAG REFLEX
So the sensory afferent limb of the gag reflex is the glossopharyngeal nerve (IX) while the motor efferent limb is the
Vagus (X)
Its not much of a mnemonic but I remember this as a variant of TGIF Thank God its Recurrent I know its lame perhaps just
lame enough to be memorable
Airway Blocks
Topical application of local anesthetics is usually sufficient for the tongue and oronasopharynx though glossopharyngeal blocks are
performed occasionally Blunting of the gag reflex requires Transtracheal (really translaryngeal) with or without bilateral
Superior Laryngeal Nerve blocks as shown below
mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 21 432012
The superior laryngeal nerves are blocked by deposition of 1 lidocaine near where the nerves penetrate the thyrohyoid
membrane The transtracheal block is accomplished with 4 lidocaine injected directly into the tracheal lumen Often this block
alone coupled with nebulized or atomized lidocaine is sufficient for awake intubation
mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 22 432012
Airway Structures
The right panel displays images seen during fiberoptic bronchoscopy The corresponding level on CT is displayed on the middle panel
Place the cursor over structures to learn their identity
mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 23 432012
mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 24 432012
Review of Airway Innervation
Lets review the innervation of the upper airway
mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 25 432012
Purple
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(V)Yes
The maxillary branch (V2) supplies the nasal cavity and palate while the mandibular branch (V3) supplies the anterior 23 of the tongue
(IX)Incorrect
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(X)No
The vagus innervates the airway further distal
Green
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)Yes
The glossopharyngeal nerve supplies sensation to the posterior 13
of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(X)No
The vagus innervates the airway further distal
mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 26 432012
Blue
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Yes
The Internal Branch of the Superior Laryngeal Nerve provides
sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Incorrect
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 27 432012
Red
Facial (VII) Trigeminal (V)
Glossopharyngeal (IX) Vagus (X)
(VII)No
The Facial Nerve supplies only taste to the tongue
(IX)No
The glossopharyngeal nerve supplies sensation to the posterior 13 of the tongue and its overlying structures including the soft palate
(V)No
The maxillary branch (V2) supplies the nasal cavity and palate while
the mandibular branch (V3) supplies the anterior 23 of the tongue
(x)Yes but which branch
Internal branch of superior laryngeal
External branch of superior laryngeal
Recurrent laryngeal
(Incorrect
The Internal Branch of the Superior Laryngeal Nerve provides sensory innervation to the mucous membrane from the epiglottis to
and including the vocal cords
Incorrect
The External Branch of the Superior Laryngeal nerve provides motor innervation to the cricothyroid muscle only
Yes
The Recurrent Laryngeal Nerve supplies sensory innervation to the
trachea below the vocal cords as well as motor innervation to all the
intrinsic muscles of the larynx except the cricothyroid muscle)
mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 28 432012
Case 3 Spine Evaluation
A previously healthy 40-year-old male presents with an open femur fracture from a Motor Vehicle Accident (MVA) that needs to be
repaired under general anesthesia He is currently on a backboard
with a cervical collar in place and is hemodynamically stable
Examination of this patients airway is complicated by the presence of the cervical collar which both inhibits mouth opening and by
definition prevents neck extension As you have seen above neck extension is required for direct laryngoscopy
So what shall we do
Remove the neck collar and intubate as usual
Intubate with a technique that does not require neck movement
Avoid general anesthesia and perform a regional block for the
procedure
Perform studies to clear the cervical spine
First a basic review of the anatomy is helpful
Recall that the cervical spine consists of 7 vertebrae the first two of
which are highly specialized
(Should this patient have an unstable cervical spine the movement resulting from laryngoscopy could permanently damage the spinal
cord likely resulting in quadriplegia)
(There are numerous techniques (retrograde intubationhellip) purported
to involve less cervical spine motion each of which requires substantial skill and experience These should only be attempted by
experienced practitioners Some advocate in-line stabilization where a second person attempts to hold the cervical spine still while
the primary person attempts direct laryngoscopy This technique makes intubation more difficult and is inadequate for stabilization)
mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 29 432012
(While an attractive option many would argue that anytime a
regional anesthetic is planned immediate endotracheal intubation must be possible Complications may occur during the regional block
or it may be inadequate for the operation or wear off before the surgeons are done Therefore inability to emergently intubate a
patient is a relative contraindication to regional anesthesia and should be considered in this patient with a possible unstable neck)
(Great idea)
Cervical Spine Anatomy-Atlas
C1 The Atlas is a ring that interacts with the skull base above and
C2 shown on next page It is unique in that it lacks a vertebral body and spinous process The articulation of C1 with the occiput is very
tight providing little of the flexion of the cervical spine and only about 20 degrees of extension
mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 30 432012
Cervical Spine Anatomy-Axis
C2 The Axis has an unusual thumb-like extension of its vertebral body that passes through the arch of C1 This process is called the
dens or odontoid The odontoid process is normally held very tightly against the anterior arch of C1 by the transverse ligament
Meanwhile the spinal cord travels behind the odontoid within the
arch of C1
mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 31 432012
Atlanto Axial Joint
This atlanto-axial joint provides the majority of the rotational motion of the cervical spine Meanwhile flexion and extension are primarily
accomplished at C2 and below and particularly between C4 and C6
Neck Movement with DL
What happens to the neck during direct laryngoscopy and
intubation
As you have seen the sniffing position involves neck flexion in the lower cervical spine with extension superiorly In the process of
direct laryngoscopy this motion is accentuated As the laryngoscope
is lifted upward the occiput is extended primarily at the atlanto-occipital joint (occiput-C1) while flexion occurs at C2-3 and below
Therefore any intervention that impedes this flexion and extension
will make visualization of the glottis more difficult In someone with a cervical fusion up to the occiput it is pretty much impossible to
perform direct laryngoscopy Similarly a patient with external stabilization such as a c-collar in this case will (SHOULD) have neck
movement reduced sufficient to make visualization difficult if not impossible
mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 32 432012
Clearing the C-Spine
How does one rule out damage to the cervical spine
At present history is our greatest ally If the healthy patient has no history of neck problems and no symptoms on maximal flexion and
extension they are unlikely to have cervical spine disease
On the other hand there are many patients whose cervical spine
SHOULD be radiographically evaluated pre-operatively including certain trauma patients as well as those with disease states that
affect the cervical spine including rheumatoid arthritis and Downs Syndrome These diseases may affect the transverse ligament and
thus the stability at the atlanto-axial joint
Nexus Criteria
Which trauma patients require cervical spine films prior to surgery or
intubation There is a set of criteria identified by the National Emergency X-
Radiography Utilization Study (NEXUS) that attempt to identify patients with a low probability of injury thereby reducing the
number of negative cervical spine radiographs taken
The criteria include No midline cervical tenderness
No focal neurologic deficit
Normal alertness
No intoxication
No painful distracting injury that might make them ignore their
neck pain
For those patients whose cervical spine is not cleared the
anesthesiologist must consider the risks of cervical spine damage that can be worsened through direct laryngoscopy versus the risk of
alternative techniques that may minimize neck motion including awake fiberoptic intubation A description of these alternate
techniques is beyond the scope of this site at present
mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 33 432012
Spine Film
For the current case the following film is obtained
Patients Film
Normal for Comparison
mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 34 432012
Explanation
Note the large step-off between C6 and C7 This subluxation causes entrapment of the spinal cord and damage
Therefore this patient requires an intubation technique with minimal neck motion and awake positioningas well as some external
stabilization or operative intervention to prevent damage to the spinal cord at the neck
mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 35 432012
C-Spine Review
So which patients are at higher risk for neck injury during intubation
Trauma patients
Yes No
(yes)Correct
They may have trauma to the cervical spine as well
(no)Incorrect
They may have trauma to the cervical spine as well
Rheumatoid arthritis patients
Yes No
(yes)Correct
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
(no)Incorrect
Approximately 30 of patients with severe disease will have some
instability at C1-C2 All should have periodic flexion or extension xrays particularly prior to surgery
Downs Syndrome patients
Yes No
(yes)Correct
About 15 of these patients have laxity in the transverse ligament
that holds the odontoid against the anterior arch of C1 Xrays are also recommended in these patients prior to anticipated neck
manipulation including laryngoscopy
mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 36 432012
(no)Incorrect
About 15 of these patients have laxity in the transverse ligament that holds the odontoid against the anterior arch of C1 Xrays are
also recommended in these patients prior to anticipated neck manipulation including laryngoscopy
Osteoarthritic patients
Yes No
(yes)Incorrect
They are not at higher risk
(no)Correct
They are not at higher risk
Patient with a prior cervical spine fusion
Yes No
(yes)Incorrect
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
(no)Correct
Assuming the repair is stable and there is no further disease there is
little risk of damage Such patients may be difficult to intubate though if their mobility is significantly limited
mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 37 432012
Airway References
Cricoid Pressure
Vanner RG Asai T Safe use of cricoid pressure Anaesthesia 1999 54 1-3 A review of literature with recommendations
Sellick BA Cricoid pressure to control regurgitation of stomach contents during induction of anaesthesia Lancet 1961 2 404-6 The original description
Views and Grades
Mallampati SR Gatt SP et al A clinical sign to predict difficult tracheal intubation a prospective study Can Anaesth Soc J 198532(4)429-434 The original paper describing the classification system but only 3 grades (III and IV combined)
Samsoon GLT and Young JRB Difficult tracheal intubation a retrospective study Anaesthesia 198742487-490 Describes the addition of Mallampati class 4
Cormack RS and Lehane J Difficult tracheal intubation in obstetrics Anaesthesia 1984391105-1111 Describes the laryngoscopy grades and correlates with difficult intubation Also proposes a technique of attempting to intubate while intentionally achieving a suboptimal (Class III) view
Studies of Predictive Indices
There are many studies some which counter others One difficulty is defining a difficult airway Most use a Cormack-Lehane laryngoscopy grade of III-IV Some investigate specific radiographic measurements that are impractical in daily clinical practice Below are a few useful references
El-Ganzouri AR McCarthy RJ et al Preoperative airway assessment Predictive value of a multivariate risk index Anesth Analg 1996821197-1204 A logistic regression comparing examination tests and developing a risk index
Chou HC Wu TL et al Mandibulohyoid distance in difficult laryngoscopy Br J Anaesth 1993 71335-339 A single article sighting this distance as an important factor in an analysis of only 11 patients
Frerk CM Predicting difficult intubation Anaesthesia 1991461005-1008 A study suggesting that a Mallampati Class III or IV with thyromental distance of lt7cm is sensitive and specific for difficult intubation (laryngoscopy grade 3 or 4)
C-Spine Evaluation
mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria

mohammad reza rajabi
Page 38 432012
Hoffman JR Mower WR et al Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma N Engl J Med 200034394-99 Application of the NEXUS criteria