Embed Size (px)
Citation preview

PULMONARY HYPERTENSION
Augustine Lee, MD
Mayo Clinic Florida

Definition
Hemodynamically defined
mPAP >25 mmHg at rest (or >30 with exercise)
PCWP <15 mmHg
(PVR > 3 wood units)
Diagnosis requires hemodynamic
assessment
Echocardiography alone is not sufficient
Right heart or PA catheterization required

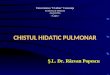
LUNGS
RA RV PA PC PV LA LV
PVR CO
PA Pressure PV Pressure
V = I R

WHO Classification
1. PAH Idiopathic
Familial (6%): BMPR2, ALK1, Endoglin (HHT), KCNK3?
Drug and toxin-induced
Fenfluramine
Associated conditions (APAH):
Connective tissue disease: Scleroderma, SLE
HIV
Portal hypertension
CHD: Eisenmenger’s, Systemic-pulmonary shunt
Schistosomiasis
Chronic hemolytic anemia: Sickle cell anemia
1’. PVOD, Pulmonary capillary hemangiomatosis

WHO Classification
2. Left heart disease (“venous”)
Systolic, diastolic, valvular
3. Lung disease and/or hypoxemia
COPD, ILD, Sleep disordered breathing, Hypoventilation syndromes, High altitude
4. Chronic thromboembolic pulmonary hypertension
(CTEPH)
5. Other
Sarcoidosis, PLCH, Neoplastic, Metabolic disorders, Myeloproliferative disorders, Fibrosing mediastinitis

Breakdown (REVEAL)
McGoon, Eur Resp Rev 2012
ALL PH APAH

Idiopathic
No risk factor
No family history or genetic mutation
Leading cause ~40%
Women > men
Mean age 52

Associated conditions
CTD ~15% Systemic sclerosis (~50%) have worst prognosis
HIV ~6% Declining
Schistosomiasis Possibly most prevalent worldwide
Sickle cell ~20% Poor prognosis
COPD, IPF/ILD ~ 40% Worsens prognosis
Venothromboembolism Even after single “normotensive” acute PE ~27%
Might be less if treated with thrombolytics ~11%

Europe: Galie, EHJ 2009

Europe: Galie, EHJ 2009

US: ACCF/AHA 2009

ACCF/AHA 2009

www.Pah-info.com
Right Heart Catheterization

REVEAL Registry
“Registry to Evaluate Early and Long Term
PAH Disease Management”
United States
2006-2009
3515 subjects
Multiple publications

Prognosis (REVEAL) Benza, Chest 2012.
McGoon, Eur Resp Rev 2012

IPF and PAH Nadrous, Chest 2005

COPD and PAH Oswald-Mammosser, Chest 1995

Quick bad prognostic findings
Age > 45
WHO functinal class III or IV
Failure to drop a functional class after therapy
Echocardiography Pericardial effusion
Large right atrial size and RAP >20
Septal shift during diastole
RV dysfunction
Increased BNP
Prolonged QRS
Hypocapnia
Comorbid conditions: COPD, IPF, diabetes, sickle cell, HIV, etc.

Causes of death (IPAH)
73%: RV failure
27% Other
Medication adverse effect
Surgery
Pneumonia
Stroke
D’Alonzo. AIM 1991. (NBHLBI)

McGoon, Eur Resp Rev 2012

Treatment: General Measures
Manage primary disorder E.g. Mitral stenosis, COPD, stop toxins
Manage aggravating conditions E.g. Sleep apnea, renal failure
Oxygen: Goal >90%
Anticoagulation Extrapolated survival data from IPAH
Management of RHF Diuretics, Digoxin
Exercise, rehabilitation
Move quicker & earlier to advanced therapy EARLY Study: Galie, Lancet 2008

Special case: Vasodilator responsive
~ 13% will “Respond”
Absolute mPAP falls <40mmHg
Decrease in mPAP by at least 10mmHg
Vasodilator
Inhaled NO, Epoprostenol, CCB, Adenosine
Therapy (Optional)
CCB (diltiazem, nifedipine, amlodipine)
Sustained response ~54%
Requires regular monitoring

ACCF/AHA 2009

Pathophysiology: “Vasculopathy”
Smooth muscle cell & endothelial cell proliferation (plexiform lesions)
Growth inhibitors, mitogens
Vasoconstriction
Imbalance of vasodilators/constrictors
Thrombosis
Imbalance in local coagulation factors

www.Pah-info.com

Humbert, NEJM 2004

Advanced Therapy
Prostanoid (“Gold standard”)
Epoprostenol (IV)
Treprostinil (IV, SQ, inhaled, [PO])
Iloprost (inhaled)
Endothelin receptor antagonists (ERA)
Bosentan, [macitentan], ambrisentan, sitaxsetan
PDE5 inhibitors
Sildenafil, tadalafil, vardenafil
Guanylate cyclase stimulant (sGC)
[Riociguat]

Adverse effects
Prostanoids
Jaw pain, flushing, headache, nausea, diarrhea,
arthralgias, central line infection, skin reaction
ERA
Edema
Liver toxicity: sitaxsentan > bosentan >
ambrisentan
Teratogenicity
(Pregnancy is contraindicated)
ERA contraindicated. Prostanoid preferred.

Combination therapy (REVEAL) McGoon, Eur Resp Rev 2012
BREATHE-2 TRIUMPH
FREEDOM-C

Benza, Chest 2012
McGoon, Eur Resp Rev 2012
So are patients doing better? (REVEAL)

Super-Advanced
Lung transplantation
Bilateral lung +/- heart
Median survival ~3 years
Pulmonary thromboendarterectomy
Can be curative
Expert centers only
Atrial septostomy
High procedural mortality (15-20%)
Worsening hypoxia from shunt
Palliative measure with goal to improve cardiac output in severe RHF

Summary
PAH is bad news, by itself or when complicating other conditions
Use the WHO classification to guide diagnostic considerations, & specific therapeutics
Diagnose it early, and treat it early.
RHC is necessary for diagnosis.
Lots of therapeutic options now available & more coming
But prostanoids remain gold standard in severe PAH
Consider referral to advanced PH/Transplant center early