Embed Size (px)
Citation preview

10
Cholestasis and end-stage liver disease
SUSAN M. PROTHEROE MRCP Specialist Registrar
DEIRDRE A. KELLY MD, FRCPI, PRCP
Consultant Paediatric Hepatologist and Reader in Paediatric Hepatology, University of Birmingham
The Liver Unit, The Birmingham Children’s Hospital NHS Trust, Steelhouse Lane, Birmingham 84 6NH, UK
Protein-energy malnutrition is an inevitable consequence of chronic liver disease, particularly in the developing infant. Severe malnutrition with loss of fat stores and muscle wasting affects between 60% and 80% of infants with liver disease (Beath, 1993a; Holt et al, 1997). Reduced energy intake secondary to anorexia, vomiting and fat malabsorption, in association with a disordered metabolism of carbohydrate and protein, increased energy requirements and vitamin and mineral deficiencies, contributes towards growth failure. Reversal of malnutrition is one of the key aims of liver transplantation and is achieved in the majority of long-term survivors. The aetiology of persistent growth failure post- transplantation is multifactorial and is related to pre-operative malnutrition, glucocorticoid administration, feeding problems and post-operative complications. Strategies to prevent pre- and post-transplant growth failure include early referral for liver transplantation and a multidisciplinary approach to nutritional support, which may increase survival and improve the quality of life and outcome of liver transplantation.
Key words: cholestasis; liver diseases; liver failure; liver transplantation; child nutrition disorders; growth; malnutrition.
PATHOPHYSIOLOGY OF MALNUTRITION IN LIVER DISEASE
Reduced energy intake Anorexia is common in children with liver disease and may result from ascites, hepatosplenomegaly or dietary manipulations such as fluid restriction or the prescription of unpalatable feeds. BailliZre ‘s Clinical Gastroenterology - Vol. 12, No. 4, December 1998 ISBN C&7020-2469-4 0950-3528/98/040823+ 19 $12.00/00
823 Copyright 0 1998, by BaillErc Tindall
All rights of reproduction in any form reserved

824 S.M.PROTHEROE AND D.A. KELLY
Fat malabsorption
At least 50% of long-chain triglycerides (LCTs), fat-soluble vitamins and the essential polyunsaturated fatty acids (PUFAs) may not be absorbed because of reduced bilary secretion and intraluminal bile concentration (Glasgow et al, 1973; Kaufman et al, 1992; Beath et al, 1993b). Water- soluble lipid such as medium-chain triglyceride (MCT) does not depend on the presence of bile to optimize solubility, and 95% or more may be absorbed even in profoundly cholestatic infants (Beath et al, 1993~).
Portal hypertension, leading to a congested gastric and intestinal mucosa, combined with small bowel overgrowth (in the presence of a roux-en-Y ‘blind’ loop created in a Kasai portoenterostomy) may furthur exacerbate malabsorption, as may cholestyramine (which is used to reduce pruritus), by binding bile salts. Pancreatic function is usually intact (Beath et al, 1993b) except in children with Alagilles syndrome, in whom pancreatic lipase may be low (Chong et al, 1989).
Long-chain polyunsaturated fatty acids
Long-chain polyunsaturated fatty acids (LCPUFAs), such as arachidonic acid (AA) and docosahexanoic acid (DHA) are emerging as essential nutrients in infancy. LCPUFAs have been reported to affect the develop- ment of visual acuity and mental development in the first year of life, and DHA plays an important role in the development of the nervous system, particularly the retina and visual pathway (Makrides et al, 1995). Neonatal DHA is supplied transplacentally, but after birth, the major source is dietary. AA, which is formed from linoleic acid, may be important for normal growth, at least in pre-term infants (Carlson et al, 1992).
Infants with cholestatic liver disease are at risk of DHA deficiency secondary to malabsorption of LCT, prescription of diets rich in MCT and inadequate liver desaturase enzyme activity (Kaufman et al, 1992). Low red cell phospholipid and DHA have been documented in cholestatic infants and may be associated with impaired visual development. Deficiency arises between 3 and 12 months of age when maternally derived DHA is exhausted (Spray et al, 1995). This suggests that infants with cholestatic liver disease may benefit from DHA supplements.
Hepatic metabolism
Reduced hepatic and muscle glycogen stores lead to the early recruitment of fat and an increased reliance on amino acids as an alternative fuel (McCullough et al, 1989). These metabolic changes result in muscle wast- ing, hyperammonaemia, hypoproteinaemia, hypoglycaemia, hyperlipaemia and reduced circulating triglyceride levels (due to increased fat oxidation) in infants. Low branched-chain amino acids (BCAAs) and raised aromatic amino acids (AAAs) and methionine reflect abnormal protein utilization (Weisdorf et al, 1987; Protheroe et al, 1996a). A recent study of protein metabolism in infants with liver disease has demonstrated that muscle

CHOLESTASIS AND END-STAGE LIVER DISEASE 825
protein degradation and protein oxidation are increased, probably as a result of the loss of control of carbohydrate metabolism and the utilization of protein as an energy supply (Protheroe et al, 1996a). Unlike the situation in normal children, muscle protein degradation continues despite feeding, suggesting that this may be a factor in the muscle wasting common in chronic liver disease.
Growth hormone/IGF-1 axis
Growth failure may be compounded by the impaired growth hormone (GH)/IGF-1 axis (Quirk et al, 1994; Holt et al, 1996) since insulin-like growth factor-l (IGF-1) and its major circulating binding protein, IGF- BP-3, are derived from the liver. Many studies have indicated that plasma IGF-1 levels are low in children with chronic liver disease despite elevated serum GH, which may be related to end organ insensitivity to IGF-1 (Bucuvalas et al, 1996; Holt et al, 1997).
Increased energy expenditure
Energy requirements are increased up to 140% (Pierro et al, 1989; McKieman et al, 1994; Protheroe et al, 1996b) by different mechanisms, including portosystemic shunting and ascites, abnormal intermediary metabolism and the energy demands of complications such as sepsis and variceal haemorrhage.
CONSEQUENCES OF CHOLESTASIS
Children with progressive cholestasis or an unsuccessful Kasai porto- enterostomy for biliary atresia will develop significant fat malabsorption with associated fat-soluble vitamin deficiency and protein malnutrition, which leads to growth failure and immunosuppression (Table 1). Fat malabsorption leads to steatorrhoea and loss of fat stores (which may be measured by triceps or subscapular skinfolds). The abnormalities in the absorption of LCTs lead to essential fatty acid deficiency, which presents as a skin rash. Attempts to correlate essential fatty acid deficiency and visual function indicate that there may be abnormalities in all the electroretino- grams in severely deficient patients (Spray et al, 1995). Fat-soluble vitamin deficiency is common and may occur within 6- 12 weeks of birth (Table 1). Vitamin A and E deficiency may be detected biochemically before any clinical symptoms. Rickets and pathological fractures as a result of vitamin D deficiency are more common in children with renal tubular disorders associated with inherited metabolic liver disease, and may be resistant to treatment. Vitamin K deficiency is inevitable and may present as haemor- rhagic disease of the newborn, particularly in breast-fed babies who were given insufficient vitamin K at birth (Hope et al, 1982).
Protein malnutrition develops later in the course of the disease. There is reduction in muscle bulk and significant motor developmental delay, which

826 S. M. PROTHEROE AND D. A. KELLY
Table 1. Clinical manifestations of mahmtrition in liver disease. Aetiology Clinical manifestations Protein-energy malnutrition Growth failure Protein catabolism Muscle wasting, motor development delay Fat malabsorption Steatorrhoea Essential fatty acid deficiency Peeling skin rash Vitamin A deficiency Conjunctival and corned drying, abnormal retinal
function, night blindness Vitamin E deficiency Peripheral neuropathy, ophthalmoplegia, ataxia,
haemolysis Vitamin D deficiency Osteopenia, rickets, fractures Vitamin K deficiency fbuising, epistaxis, coagulopathy Zinc deficiency Acrodermatitis, anorexia, poor growth Hypercholesterolaemia Xanthomata Impaired gastrointestinal function, Malabsorption
hypochlorhydria, reduced mucosal function Immunosuppression secondary to reduced cell- Systemic infections
mediated immunity
may resolve post-transplant (Beath et al, 1993~). The long-term effect of malnutrition and essential fatty acid deficiency on neurodevelopmental outcome has not yet been established.
SELECTING PATIENTS FOR NUTRITIONAL SUPPORT
Anthropometry
Growth failure may precede the overt signs of liver disease and should be anticipated by frequent anthropometric assessment. The need for nutritional support in infants with liver disease may be underestimated because of abnormal body composition due to ascites and/or organomegaly, and weight alone may be an unreliable parameter by which to assess nutritional state. Although linear growth is more sensitive, it is a late sign of growth failure in infancy, as stunting (or negative height velocity) may not be apparent until 1 year of age (Beath et al, 1993d). Triceps skinfold thickness and mid-arm circumference are useful indicators of body fat and protein, and serial recordings may demonstrate an early loss of fat stores before weight and height changes become obvious (Sokal and Stall, 1990; Shepherd et al, 1991). Data are expressed as standard deviation (or ‘Z’) scores related to the median value for the child’s age and sex, in which a Z score of 0 equals the 50th percentile.
Patients at particular risk of development of malnutrition
The patients especially likely to develop malnutrition are those: 1. under 2 years of age; 2. with severe cholestasis (a serum bilirubin level over 70 mmol/l with
more than 50% conjugated);

CHOLESTASIS AND END-STAGE LIVER DISEASE 827
3. with progressive liver disease such as biliary atresia on severe neonatal hepatitis, or patients awaiting liver transplant;
4. suffering recurrent hepatic complications such as ascites and bleeding varices.
STRATEGIES FOR NUTRITIONAL SUPPORT
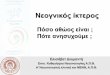
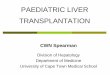
Strategies for the nutritional support of the child with end-stage liver disease are outlined in Figure 1.
Patient at risk of malnutritionlcholestasis
i (1) Increase calorie density of feed to 140-200% EAR Supplemented by increasing: l carbohydrate 15-20 g/kg/day (glucose polymer) l fat up to 8 g/kg/day (MCT:LCT in ratio 50:50) l protein to 3-4 g/kg/day (whole protein)
(2) Fat-soluble vitamin supplementation
1 inadequate weight gain/anorexia
Nasogastric tube feeding 0 top-up tube feeds 0 nocturnal enteral feeds over 12 hours
Asciteslfluid retention
4 Fluid and sodium restriction (75% of maintenance) Concentration of feed increased to 1.6-2.0 kcal/ml) I
Feeding difficulties/regurgitation/volume intolerance
J , Continuous nasogastric tube feeding
Feed intolerance/bleeding varices Severe encephalopathy
Parenteral nutrition Reduce protein to 1 g/kg/day or add BCAA
Figure 1. Algorithm for feeding the child with end-stage liver disease. MCT= medium-chain triglyceride; LCT = long-chain triglyceride; BCAA = branched-chain amino acids.

828 S. M. PROTHEROE AND D.A. KELLY
Increased energy intake
As the resting energy requirements of infants with liver disease are increased (Protheroe et al, 1996b), it is necessary to increase the energy intake to 140-200% of the estimated average requirements (EAR). In infants, this is achieved by supplementing milk feeds with extra carbo- hydrate and fat to produce a feed with an energy density of 4.18 kJ/ml (1 kcal/ml) or mote. Such a feed may have an osmolality of 500- 800 mosml/l and is introduced gradually to establish intestinal tolerance. Calorie supplementation added to drinks may be effective for older children. If there is no response to an increase in energy intake alone, nocturnal enteral feeding by nasogastric tube may be required.
Lipids The energy value of dietary lipids, the major energy source for infants, is 8-9 kcal/g. Increasing total fat intake (with LCTs and MCTs) may increase the overall amount of fat absorbed and improve growth despite increasing steatorrhoea (Beath et al, 1993b).
Medium-chain triglycerides
MCTs are well absorbed in cholestatic infants (Burke and Danks, 1966; Cohen and Gartner, 1971); hence the addition of 30-50% MCT is a useful substrate, reducing steatotrhoea, with subsequent nutritional improvement (Beath, et al 1993b).
Essential fatty acids
Although the exact requirements for essential fatty acids in infants is unknown, clinical deficiency symptoms may occur at polyunsaturated fatty acid intakes below 1% of energy (Crawford et al, 1978; Makrides et al, 1995). The minimal intake of linoleic acid recommended for young infants is 2.7-4.5% of energy intake, and a ratio of linoleic to linolenic acid of 5: 1 is proposed (Koletzko et al, 1992; Spray et al, 1995). It is not yet clear how best to supplement DHA as it is not stable in many proprietary feeds. Preliminary data indicate that the provision of 1% DHA (in total fat content) may prevent deficiency in cholestatic infants (C.H. Spray, personal communication, 1998.)
Structured lipids
Triglycerides that contain both long- and medium-chain fatty acids bound to the same glycerol molecule are absorbed like MCT and hence increase the absorption of the long-chain component. Clinical studies of these modified lipids are currently in the preliminary stages (Carnielli et al, 1996).

CHOLESTASIS AND END-STAGE LIVER DISEASE 829
Carbohydrates
Complex carbohydrates such as maltodextrin or glucose polymer restrict the osmolality of the feed while maintaing a high energy density (> 1 kcaYml), allowing fluid restriction and providing up to 20 g/kg per day carbohydrate. In infants, this may be added to milk feeds, while in older children it may be provided as supplemental drinks.
Protein
Infants with advanced liver disease may tolerate up to 4 g/kg per day protein without encephalopathy or an increase in plasma amino acid abnormalities (Charlton et al, 1992).
Modified amino acid formulations designed to improve the balance of aromatic/branched-chain amino acids in plasma may be of nutritional benefit and are under evaluation. The BCAA leucine may promote muscle protein synthesis and inhibit muscle protein breakdown through the formation of its ketoanalogue, alpha-ketoisocaproate (Garlick and Grant, 1988). The effect of a modified amino acid feed containing 50% BCAA was compared with an isonitrogenous formula containing 22% BCAA in infants with liver disease by measuring whole body protein turnover (Protheroe et al, 1996a). The BCAA-supplemented feed improved protein retention compared with the standard formula by suppressing endogenous protein catabolism, and normalized the plasma amino acid profile.
The effect of this supplement on growth is still under evaluation, but a feed containing 32% BCAA improved lean body mass in one trial conducted in children awaiting liver transplantation, although this product did not improve plasma amino acids levels (Chin et al, 1992; Protheroe et al, 1995).
Mineral supplementation Zinc deficiency secondary to chronic malabsorption may contribute to anorexia and poor linear growth. Plasma zinc concentration may not reflect total body zinc status, but supplementation may be helpful if deficiency is suspected because of persistent poor growth.
MODE OF DELIVERY
Enteral feeds If children have no nutritional response to an increase in energy intake, or become anorexic, the delivery of feeds via a nasogastric tube is indicated. Intensive enteral nasogastric feeding is highly effective in reversing malnutrition in infants and children with liver disease and may transform a child’s mood and increase voluntary intake (Moreno et al, 1991; Charlton et al, 1992; Beath et al, 1994).
Enteral feeding offers several advantages over intravenous feeding. The enteral route is cheaper as well as physiological. It maintains gastrointestinal

830 S.M.PROTHEROEAND D.A.KELLY
tract immunity, reduces bacterial overgrowth, probably via the stimulation of IgA production, and maintains the integrity of the gut barrier to micro- organisms (Stringer and Puntis, 1995). Trophic factors, for example glutamine, an important amino acid for enterocyte function (McAnena et al, 199 l), may be added to the feed if required.
A soft silastic nasogastric tube is well accepted for either complementary ‘top-up’ feeds or nocturnal feeding and does not cause bleeding from oesophageal varices. Nocturnal feeding is the method of choice as it allows adequate calorie supplementation while maintaining oral feeding during the day. In addition, nocturnal feeding may be beneficial if glucose homeostasis is disrupted as it will prevent fasting hypoglycaemia and reduce protein catabolism in end-stage liver disease. Oral feeding should be maintained as long as possible to avoid long-term behavioural problems, but many children with end-stage liver disease will eventually require continuous enteral feeding either for preventing hypoglycaemia or for feed intolerance.
Nasogastric tube feeding at home may present practical problems to an already overburdened family so it is essential to provide excellent training and support from a dedicated nutritional care team including the dietitian, liaison nurse and clinician (see Chapter 12).
Parenteral nutrition
There may be a reluctance to use parenteral nutrition in children with chronic liver disease because of the association of parenteral nutrition with hepatobiliary dysfunction (Puntis et al, 1987; Sax and Bower, 1988). However, short-term parenteral nutrition does not increase cholestasis and may be essential if the patient cannot be enterally fed because of feed intolerance, or secondary to recurrent variceal bleeding or abdominal sepsis. Improvement of nutritional status may improve liver function, particularly if oral nutrition can be maintained.
Standard amino acid and lipid solutions are well tolerated in stable patients, but the elimination of fat and plasma amino acids should be monitored. The amino acid content of the intravenous feed should be reduced to 1 g/kg per day, and lipid should be administered with caution in severe liver dysfunction and hepatic encephalopathy. Patients need careful biochemical monitoring and attention to fluid and electrolyte balance, including concurrent intravenous infusion therapy. It has been suggested that 50% of the lipid source should be provided as MCT in parenteral solutions for adults because MCT can be utilized peripherally even in advanced liver failure, and encephalopathy may improve (Glynn et al, 1988). However, intravenous MCT should be used with caution in children as incomplete oxidation may occur, producing metabolic acidosis.
BEHAVIOURAL PROBLEMS
Behavioural feeding problems are common and are secondary to long-term tube feeding, unpalatable feeds or medications. The pre-transplant

CHOLESTASIS AND END-STAGE LIVER DISEASE 831
emphasis on intensive nutritional support often creates parental anxiety about feeding. Problems may become manifest pre- and post-transplanta- tion, and contribute towards persistent growth failure.
Strategies to prevent this include day-time feeding to provide oral stimulation, particularly if nocturnal nasogastric feeding is being under- taken. A multidisciplinary approach, involving the participation of the clinician, nurse specialist, clinical psychologist and play therapist, is required.
Table 2. Fat-soluble vitamin supplementation
Vitamin Dose Drug Monitoring A 5000-20 000 units/day Aravit A or Aquasol A Serum level 0.7-2.1 mmol/l
D SO- I SO rig/kg/day Alpha calcidol Alkaline phosphatase > 1000 IU Wrist X-ray for rickets
E IS-25 IU/kg/day Tocopherol Serum level 1 I S-24.4 pmol/l Polyethylene glycol Serum E:lipid ratio > I .8 pmol/mmol 1000 succinate
K 2.5 10 me/dav Menadiol Prothrombin time > 17 seconds
LIVER TRANSPLANTATION
Effect of pre-operative nutritional status on outcome after liver transplantation
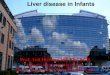
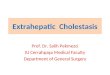
Many studies have demonstrated the relationship between pre-operative malnutrition and outcome following liver transplantation (e.g. Moukarzel et al, 1990; Chin et al, 1991). Despite intensive nutritional support, 50% of children will be malnourished at the time of liver transplantation (Figure 2), which has a significant effect on both morbidity and mortality following the procedure.
Chin et al (1991) prospectively studied 26 children post-transplantation. There was a significant difference in the 2-year actuarial survival for children with standard deviation scores (SDS) for weight of greater than -1 (57%) compared with those less than -1 (95%) at the time of transplan- tation. Moukarzel et al (1990) generated similar data using height SDSs, in which children who were less stunted (height SDS score less than -1) had less morbidity and mortality (91% 1 -year survival) compared with those who were more stunted (height SDS score greater than -l), who had a l-year survival of 75%.
Shepherd et al (1991) evaluated the nutritional profiles of 37 children (aged 0.5-14 years) with chronic liver disease at the time of liver trans- plantation. They indicated that the actuarial survival of those who were transplanted with SDS scores for weight of less than -1 were 88% at one year compared with those who were undernourished (SDS greater than -I>, which was 38%. They also found that declining nutritional status during the waiting period adversely affected outcome. The presence of pre-operative

832 S. M. PROTHEROE AND D. A. KELLY
.-
30 s .- C 5 $j 20 I 8
10
0 TSF MAMA
< - 2 SD below mean
HT
Figure 2. Pattern of malnutrition in 50 children with biliary atresia at transplantation, Birmingham Liver Transplant Programme.. TSF = triceps skinfold; MAMA = mid-arm muscle area; Ht = height. Reproduced from Kelly DA (1997) Jourt~11 ofLiver Transplantation and Surgery 3: S32-S39) with permission.
malnutrition also has a significant effect on the duration of post-operative hospitalization, in which children with height SDS scores of over -2 experienced more complications and had a prolonged hospital stay of up to 100 days compared with those who were less stunted at the time of transplantation (Shepherd et al, 1991; Beath et al, 1994).
Effect of liver transplantation on growth
Although studies that evaluated growth patterns in children after liver transplantation historically indicated that approximately two-thirds of these children failed to demonstrate catch-up growth, more recent studies have indicated that 80% of survivors achieve normal growth patterns and nutritional status within 1 year of transplantation (Andrews et al, 1989; Beath et al, 1993~; Codoner-Franch et al, 1994; Holt et al, 1997) (Figure 3). In evaluating growth patterns post-transplantation, height or weight gain are expressed as the change in 2 scores at 6-month or annual intervals, and catch-up growth has been defined as linear growth velocity that exceeds the mean (i.e. the 2 score for linear growth velocity is greater than zero).
Surviving children who have a successful liver transplantation experience a rapid return to normal of mid-arm muscle area and mid-arm fat, usually within 3-6 months (Beath et al, 1993~; Holt et al, 1997). Weight gain may initially be excessive because of the effects of steroids on appetite and salt and water retention, but most children return to a normal weight within 9-12 months (Beath et al, 1993~; Holt et al, 1997). Linear growth is often delayed between 6 and 24 months depending on the rate of hepatic complications or the immunosuppressive regimen (McKieman et al, 1992; Codoner-Franch et al, 1994; Rodeck et al, 1994).

CHOLESTASIS AND END-STAGE LIVER DISEASE
I
-a. -1, -
,’ ,’ .*
a33

834 S.M.PROTHEROE AND D.A. KELLY
A large study that followed 119 children for more than 1 year following transplantation (Codoner-Franch et al, 1994) demonstrated that there are no differences in growth between the genders. Both boys and girls develop a normal pubertal growth spurt and achieve endocrine rehabilitation with the development of secondary sexual characteristics.
Pre-operative malnutrition also has a significant effect on post- transplantation growth. Two recent studies (McKieman et al, 1992; Sama et al, 1994), which evaluated 43 and 3 1 children respectively, demonstrated that children with lower height SDS scores at the time of transplantation had a greater catch-up growth post-transplant, confirming that children with severe growth retardation have the capacity for catch-up growth once normal liver function has returned. It is interesting to note that the degree of normalization of growth was related to the extent of pre-operative stunting. For example, infants who were less stunted (height SDS less than -1) initially grew slowly but finally achieved normal growth, whereas older children who were more stunted (height SDS greater than -2) grew more quickly post-transplantation but did not achieve normal height. In both studies, more than two-thirds of children achieved normal or signifi- cant catch-up growth for height in addition to regaining normal weight. These findings were not confirmed by a large study, which followed 45 consecutive paediatric transplant recipients over 2 years. This group found that both height and skeletal age were maintained but did not demonstrate catch-up growth. It is difficult to evaluate these data as neither pre- operative malnutrition, inadequate liver function or corticosteroid dosage had any effect on skeletal growth, as has been shown in other studies (McKieman et al, 1992; Codoner-Franch et al, 1994; Rodeck et al, 1994).
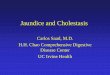
In the large study of 119 children followed for more than 1 year by Codoner-Franch et al (1994), catch-up growth occurred between 6 and 24 months post-transplantation, and there was no difference between male and female patients. In this study, Codoner-Franch et al suggested that the age of transplantation may be a limiting factor for linear growth because, in their experience, children who receive transplants when aged less than 2 years developed negative Z scores for linear growth velocity after the first 2 years post-transplantation. This has not been confirmed by our own experience in Birmingham, in which 26 infants who were transplanted before the age of 1 have been followed for more than 4 years post- transplant (Figure 4) all of whom regained normal growth within 4 years of transplantation.
Indications for transplantation
Many studies have demonstrated that there is no connection between the disease indications for liver transplantation and post-transplant growth. Codoner-Franch et al (1994) found that children who were transplanted for metabolic liver disease have the greatest catch-up growth in the first 2 years after liver transplantation, which was not confirmed by Sama et al (1994) or Peeters et al (1996). It is possible that this difference is because children who are more malnourished, for example those with cholestatic liver disease

0
-0.5
8 07
E
-1
,F
I
-1.5
-2
1 -6
01
1 6
16
30
42
54
66
(r&6)
(n
=16)
(k
12)
Tim
e fro
m t
rans
plan
tatio
n (m
onth
s)
Figur
e 4.
Comp
ariso
n of
heigh
t sta
ndar
d de
viatio
n sc
ore
(SDS
) in
child
ren
with
bil
iary
atres
ia tra
nspla
nted
at les
s tha
n (N
= 13
) an
d mo
re
than
(iV=
13)
12 m
onths
of
age.

836 S. M. PROTHEROE AND D. A. KELLY
secondary to biliary atresia, have a greater potential for catch-up growth. Children transplanted for acute liver failure who have normal growth pre-transplantation would be expected to continue to grow normally post- transplantation. Interestingly, Codoner-Franch et al (1994) found that this particular group of children developed a reduction in height Z scores 3 and 4 years post-transplantation, although the reasons for this were not specified.
Alagille’s syndrome, which is an autosomal dominant disorder in which growth retardation is part of the syndrome, is particularly resistant to nutritional supplementation pre-transplant. Cardona et al (1995) have evaluated the post-transplantation outcome in 12 children with Alagille’s syndrome, 11 of whom had severe growth retardation before transplanta- tion. Eight out of 10 survivors with growth retardation pre-transplantation have shown a significant increase in height and weight post-transplantation. Only one child had no change in nutritional parameters, but four children had height SDS scores greater than 1.5 indicating that, despite improved linear growth, height SDS scores were not completely normal in this group of patients within 3 years of transplantation. This has been subsequently confirmed by Holt et al (1997), who reported three children with Alagille’s syndrome who were not only more malnourished pre-transplantation than children with other liver diseases, but also did not show any evidence of catch-up growth post-transplantation.
Glucocorticoid administration
The effects of corticosteroids on growth are well known. They delay skeletal maturation, particularly in pre-pubertal children, and inhibit DNA synthesis in liver, heart, skeletal muscle and kidneys. There is also evidence that glucocorticoids may inhibit growth hormone release by reducing growth hormone receptor expression or uncoupling receptors from the signal transduction mechanism (Robinson et al, 1995).
The effect of corticosteroids on growth in liver transplant recipients has been well documented. All prospective studies demonstrate that there is little catch-up growth in the first 6 months post-transplantation when the steroid dosage is higher (Andrews et al, 1989; McKieman et al, 1992; Codoner-Franch et al, 1994; Rodeck et al, 1994) (Figures 3 and 4 above). Multiple regression analysis of 59 patients surviving for at least 1 year post- transplantation has demonstrated that, in the first year post-transplant, the combined influence of bilirubin concentration and steroid dosage correlated with the SDS for growth velocity (r =0.63; P=O.Ol). However, in the second year post-transplantation, only the cumulative steroid dosage was significant (r = -0.47; P = 0.001). The French study (Codoner-Franch et al, 1994) came to a similar conclusion and demonstrated that continuous corticosteroid therapy was inversely correlated with Z scores for linear growth velocity. Catch-up growth was observed only when alternate-day steroids were instigated.
These data are confirmed by other studies in which the effect of with- drawal of steroids or alternate-day steroids has been evaluated. Andrews et al (I 994) found a significant increase in linear growth in 69% of 36 children

CHOLESTASIS AND END-STAGE LIVER DISEASE 837
in whom steroid withdrawal was successfully achieved. Dunn et al (1994) discontinued steroids at 1.5 years post-transplantation and found that 66% of children who had height retardation prior to the reduction had a signifi- cant increase in linear growth following the discontinuation of the steroid treatment. More recently, McKee et al (1997) have found that steroid with- drawal was possible using Tacrolimus immunosuppression, without the development of rejection and with a positive effect on growth.
Although most studies indicate that the total dosage of methyl- prednisolone is related to growth suppression, Sama et al (1997) found that exposure to methylprednisolone, rather than dose, predicts growth inhibition in children following liver and kidney transplantation.
Effect of growth hormone and IGF-1
As indicated earlier, both GH and IGF-1 are necessary for normal growth, but many studies have demonstrated that plasma IGF-1 levels are low in children with chronic liver disease, despite elevated serum growth hormone, which may be related to an end-organ insensitivity to IGF-I (Bucuvalas, 1990, 1996; Holt et al, 1997).
As glucocorticoids may interfere with GH receptor expression, they may also inhibit GH secretion. Sarna et al (1995) compared GH secretion and IGF-1 and IGF-BP3 serum concentrations, with immunosuppressive dosage and endogenous cortisol production and growth in 18 pre-pubertal children followed up for at least 1 year post-liver transplantation. Serum IGF-1 concentration was normal in all patients, GH secretion was abnormal in only two patients, but serum IGF-BP3 level was elevated in two-thirds of the patients. Endogenous cortisol production was reduced in most patients while on steroid therapy, but growth velocity correlated positively with only serum-based or stimulated cortisol concentration. The authors concluded that elevated serum IGF-BP3 concentration may have reduced the amount of biologically active IGF-1 in the circulation but that endogenous cortisol production was the best indicator of growth inhibition in this group of patients. As indicated above, they have recently suggested that it is the exposure to methylprednisolone, rather than the dose, that may affect cortisol production (Sarna et al, 1997).
Holt et al (1996) have also investigated the relationship between IGF-1 and IGF-BP3 in 26 children before and after liver transplantation and have compared the results with 30 age-matched controls. Pre- transplantation IGF-1 level was significantly lower than control values (32.7 +4.8 ygll compared with 168.3 f 16.5 pg/l; P=O.OOOl), as was IGF-BP3 (1.11 kO.1 mg/l compared with 2.57+0.17mg/l; P=O.OOOl). Although post-transplantation IGF-1 and IGF-BP3 levels rose significantly and IGF-1 levels returned to normal, marked abnormalities in IGF-BPl, BP2 and BP3 remained.
Effect of hepatic dysfunction Children who have significant post-operative morbidity with chronic

838 S. M. PROTHEROE AND D. A. KELLY
rejection are likely to be growth retarded from the combined effect of increased steroid dosage and cholestasis (Moukarzel et al, 1990). Recurrent complications such as recurrent infection, cytomegalovirus, Epstein-Barr virus and viral gastroenteritis will all affect nutritional rehabilitation.
NUTRITIONAL STRATEGY FOR PREVENTION OF GROWTH FAILURE AFTER TRANSPLANTATION
The nutritional strategy for the prevention of growth failure pre- and post- transplantation begins with intensive nutritional support pre-operatively (see above). It is essential that post-operative nutritional management should ensure that there should be no reduction in energy intake peri- transplantation. Children who are malnourished pre-transplantation should be maintained with parenteral nutrition peri-operatively, while children with normal nutrition should have an early initiation of enteral feeds and adequate calorie intake.
In those children who were malnourished pre-operatively, nutritional support post-transplantation should continue to provide an energy intake of at least 120% EAR. In infants, this may initially be provided as a modular feed via nocturnal enteral feeding. The energy intake should include 2.5-3.0 g protein per day and 6-8 g/kg glucose polymer per day, but fat should be provided entirely as long-chain fat (5-6 g/kg per day) unless complications such as chronic rejection or cholestasis develop.
Growth hormone As glucocorticoids interfere with GH excretion and there are data to suggest that the GH, IGF-1 and IGF-BPl, BP2 and BP3 axis remains abnormal post-transplantation (Holt et al, 1996), it is rational to consider treatment with GH therapy. Recombinant human GH has been evaluated in eight growth-retarded children following liver transplantation (Sarna et al, 1996). Recombinant GH was administered in a dose of 1 IU/kg per week, given by daily subcutaneous injections. The median growth rate increased from 3.2 to 7.1 cm per year (P = 0.025), and the height SDS increased from -2.9 to -3.1 (P = 0.036) during the first year of GH treatment. Both IGF-1 and IGF-BP3 levels increased significantly during treatment. There was no effect on graft function, and no child developed rejection or any other serious side effects.
SUMMARY
The majority of children undergoing liver transplantation in the 1990s may anticipate adequate nutritional rehabilitation within 2-3 years, although 20% may have persistent growth failure related to pre-operative nutritional status, excess glucocorticoid administration and recurrent hepatic compli- cations. Nutritional strategy should include a multidisciplinary approach to

CHOLESTASIS AND END-STAGE LIVER DISEASE 839
intensive pre- and post-operative nutrition, and an evaluation of new immunosuppressive drugs to reduce glucocorticoid administration.
REFERENCES
Andrews WS, Wanek B, Fyock B et al (1989) Pediatric liver transplantation: a 3 year experience. Journal of Pediatric Surgery 24: 77-82.
Andrews WS, Shimaoka S, Sommerauer J et al (1994) Steroid withdrawal after paediatric liver trans- plantation. Transportation Proceedings 26: 159- 160.
“Beath S, Pearmain G, Kelly D et al (1993a) Liver transplantation in babies and children with extm- hepatic biliary atresia: pre-operative condition, complications, survival and outcome. Journal of Pediatric Surgery 28: 1044- 1047.
Beath S, Hooley I, Willis K et al (1993b) Long chain triacyglycerol malabsorption and pancreatic function in children with protein energy malnutrition complicating severe liver disease. Proceedings of the Nutrition Society 52: 252A.
Beath SV, Brook G, Kelly DA et al (1993~) Successful liver transplantation in babies under one year. British Medical Journal 307: 825-828.
Beath SV, Kelly DA & Booth IW (1993d) Nutritional support in liver disease. Archives of Disease in Childhood 69: 545-549.
Beath S, Brook G, Kelly D et al (1994) Improving outcome of liver transplantation in babies less than I year. Transplantation Proceedings 26: 180- 182.
*Bucuvalas JC, Cutfield W, Horn JA et al (1990) Resistance to the growth promoting metabolic effect of GH in children with chronic liver disease. Journal of Pediatrics 117: 397-402.
Bucuvalas JC, Horn JA, Slusher J et al (1996) Growth hormone insensitivity in children with biliary atresia. Journal of Paediatric Gastroenterology and Nutrition 23: 135-140.
Burke V & Danks DM (1966) Medium chain triglyceride diet: its use in treatment of liver disease. British Medical Journal 2: 1050- 105 1.
Cardona J, Houssin D, Gauthier F et al (1995) Liver transplantation in children with Alagille syndrome-a study of twelve cases. Transplantation 60: 339-342.
Carlson SE, Cooke RJ, Werkman SH & Tolley EA (1992) First year growth of preterm infants fed standard compared to marine oil n-3 supplemented formula. Lipids 27: 901-907.
Camielli VP, Luijendijk IHT, Van Goudoever JB et al (1996) Structural position and amount of palmitic acid in infant formulas: effects on fat, fatty acid and mineral balance. Journal of Paediatric Gastroenterology and Nutrition 23: 553-560.
Charlton CPJ, Buchanan E, Holden C et al (1992) The use of enteral feeding in the dietary management of children with chronic liver disease. Archives of Disease in Childhood 67: 603-607.
*Chin SE, Shepherd RW, Cleghom GJ et al (1991) Survival, growth and quality of life in children after orthotopic liver transplantation: a 5 year experience. Journal of Pediatrics and Child Health 27: 380-385.
*Chin SE, Shepherd RW, Thomas BJ et al (1992) Nutritional support in children with end-stage liver disease: a randomised crossover trial of a branched-chain amino acid supplement. American Journal of Clinical Nutrition 56: 158-163.
Chong SKF, Lindridge J, Moniz C & Mowat A (1989) Exocrine pancreatic insufficiency in syndromic paucity of interlobular bile ducts. Journal of Pediatric Gustroenterology and Nutrition 9: 445-449.
“Codoner-Franch P, Bernard 0 & Alvarez F (1994) Long-term follow-up growth in height after successful liver transplantation. Journal of Pediatrics 124: 368-373.
Cohen MI & Gartner LM (1971) The use of medium-chain triglycerides in the management of biliary atresia. Journal of Pediatrics 79: 379-384.
Cnwford MA, Hassam AG & Rivers JPW (1978) Essential fatty acid requirements in infancy. American Journal of Clinical Nutrition 31: 2181-2185.
Dunn S, Falkenstein K, Lawrence JP et al (1994) Monotherapy with cyclosporine for chronic immunosuppression in paediatric liver transplant recipients. Transplantation57: 544-547.
Garlick PJ & Grant I (1988) Amino acid infusion increases the sensitivity of muscle protein synthesis in vivo to insulin. Biochemical Journal 254: 579-584.

840 S. M. PROTHEROE AND D. A. KELLY
Glasgow JFT, Hamilton JR & Sass-Kortsak A (1973) Fat absorption in congenital obstructive liver disease: Archives &Disease in Childhood 48: 601-607.
Glynn MJ, Powell-Tuck J, Reaveley DA et al (1988) High lipid parenteral nutrition improves porto- systemic encephalopathy. Journal of Parenteral and Enteral Nutrition 12: 457-461.
*Holt RI, Jones JS, Stone NM et al (1996) Sequential changes in insulin-like growth factor (IGF-1) and IGF-binding proteins in children with end-stage liver disease before and after successful orthotopic liver transplantation. Journal of Chnical Endocrinology and Metabolism 81(l): 160- 168.
Holt RI, Broide E, Buchanan CR et al (1997) Orthotopic liver transplantation reverses the adverse nutritional changes of end-stage liver disease in children. American Journal of Clinical Nutrition 65(2): 534-542.
Hope PL, Hall MA & Millward-Sadler GH (1982) a,-antitrypsin deficiency presenting as a bleeding diathesis in the newborn. Archives of Disease in Childhood 57: 69-79.
Kaufman SS, Scrivener DJ, Murray ND et al (1992) Influence of Portagen and Pregestimil on essential fatty acid status in infantile liver disease. Pediatrics 89: I51 - 154.
Kelly DA (1997) Post-transplant growth failure in children. Journal of Liver Transplantation and Surgery 3: 532-539.
Koletzko B, Thiel 1 & Springer S (1992) Lipids in human milk: a mode1 for infant formulae? European Journal of Clinical Nutrition 46: S45-S55.
McAnena OJ, Moore FA, Moore E et al (1991) Selective uptake of glutamine in the gastrointestinal tract: confirmation in a human study. British Journal of Surgery 78: 480-482.
McCullough AJ, Mullen KD, Smanik EJ et al (1989) Nutritional therapy and liver disease. Gastroenterology Clinics of North America 18: 619-643.
McKee M, Mattei P, Schwarz K et al (1997) Steroid withdrawal in tacrolimus (FK506)-treated pediatric liver transplant recipients. Journal of Pediatric Surgery 320: 973-975.
McKieman PJ, Pearmin GD, Johnson T (1992) Catch up growth in children following orthotopic liver transplantation. Hepatology 16: 567.
McKieman PJ, Magnay AR, Booth IW & Kelly DA (1994) Determinants of resting energy expenditure in childhood liver disease. Journal of Pediatric Gastroenterology and Nutrition 19: 337A.
Makrides M, Neuman M, Simmer K et al (1995) Are long-chain polyunsaturated fatty acids essential nutrients in infancy? Lancet 345: 1463-1468.
*Momno LA, Gottrand F, Hoden S et al (1991) Improvement of nutritional status in cholestatic children with supplemental nocturnal enteral nutrition. Journal of Pediatric Gastroenterology and Nutrition 12: 213-216.
*Moukarzel AA, Najm I, Vargas J et al (1990) Effective nutritional status on outcome of orthotopic liver transplantation in pediatric patients. Transplantation Proceedings 22: 1560-1563.
Peeters PMJG, Sieders E, ten Vergert EM (1996) Analysis of growth in children after orthotopic liver transplantation. Transplantation International 9: 581-588.
Pierro A, Koletzko B, Carnielli V et al (1989) Resting energy expenditure is increased in infants with extra hepatic biliary atresia and cirrhosis. Journal of Pediatric Surgery 24: 534-538.
Protheroe S, Jones R & Kelly DA (1995) Evaluation of the role of branched chain amino acids in the treatment of protein malnutrition in infants with liver disease. Gut 37: A30.
*Protheroe S, McNurlan M, Garlick Pet al (1996a) Failure to suppress protein breakdown contributes towards malnutrition in infants with liver disease. Hepatology 24(4, Pt 2): 141A.
Protheroe SM, McKieman PJ & Kelly DA (1996b) Can measurement of dietary-induced thermo- genesis (DIT) predict response to nutritional intervention in infants with liver disease? Clinical Nutrition 15 (supplement 1): 39.
Puntis JWL, Ball PA & Booth IW (1987) Complications of neonatal parenteral nutrition. International Therapy and Clinical Monitoring 8: 48-56.
Quirk P, Owens P, Moyse K et al (1994) Insulin-like growth factors I and II are reduced in plasma from growth retarded children with chronic liver disease. Growth Regulation 4: 35-38.
Robinson I, Gabrielsson B, Kalus G (1995) Glucocorticoids and growth problems. Acta Paediatrica Supplement 411: 8 l-86.
*Rodeck B, Melter M, Hoyer PF et al (1994) Growth in long-term survivors after orthotopic liver trans- plantation in childhood. Transplantation Proceedings 26: 165-166.
Sama S, Sipila I, Jalanko H et al (1994) Factors affecting growth after pediatric liver transplantation. Transplantation Proceedings 26: 161- 164.
Sama S, Sipila I, Vihervuori E et al (1995) Growth delay after liver transplantation in childhood: studies of underlying mechanisms. Pediatric Research 38: 366-372.

CHOLESTASIS AND END-STAGE LIVER DISEASE 841
*Sama S, Sipila I, Ronnholm K et aI (1996) Recombinant human growth hormone improves growth in children receiving glucocorticoid treatment after liver transplantation. Journal of Clinical Endocrinology and Metabolism 81(4): 1476- 1482.
Sarna S, Ronnholm K, Lame J et al (1997) Mechanisms and treatment of growth retardation in children with liver transplants. Transplantation Proceedings 29(1-2): 447-448.
Sax HC & Bower RH (1988) Hepatic complications of total parenteral nutrition. Journal of Purenteral and Enteral Nutrition 12: 615-718.
Shepherd RW, Chin SE, Cleghom GJ (1991) Malnutrition in children with chronic liver disease accepted for liver transplantation: clinical profile and effect on outcome. Journal of Paediatrics and Child Health 27: 295-299.
Sokal RJ & Stall C (1990) Anthropometric evaluation of children with chronic liver disease. American Journal of Clinical Nutrition 52: 203-208.
Spray CH, Beath SV, Willis KD et al (1995) Docosahexaenoic acid (DHA) and visual function in infants with fat malabsorption secondary to liver disease. Proceedings of the Nutrition Society 54: 108A.
Stringer MD & Puntis JWL (1995) Short bowel syndrome. Archives of Disease in Childhood 73: 170-173.
Weisdorf SA (1987) Nutrition in liver disease. In Lebenthal E (ed.) Texrbook of Gastroenterology and Nutrition in Infancy, 2nd edn, pp 665-676. New York: Raven Press.
Weisdorf SA, Freese DK, Fath JJ et al (1987) Amino acid abnormalities in infants with extrahepatic biliary atresia and cirrhosis. Journal of Pediatric Gastroentemlogy and Nutrition 6: 860-864.