Embed Size (px)
Citation preview

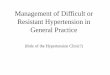
1000 hypertensive patients1000 hypertensive patients
940 essential hypertension940 essential hypertension
60 secondary hypertension60 secondary hypertension
50 renal hypertension50 renal hypertension
5 reno-vascular hypertension5 reno-vascular hypertension
5 endocrine hypertension5 endocrine hypertension
2 pheochromocytomas2 pheochromocytomas
2 primary hyperaldosteronism2 primary hyperaldosteronism
1 other endocrine cause1 other endocrine cause
avant 2000avant 2000

Pourquoi s’intéresser aux causes endocriniennes Pourquoi s’intéresser aux causes endocriniennes d’hypertension ?d’hypertension ?
Les mécanismes étiopathogéniques d’ hypertension endocrinienne Les mécanismes étiopathogéniques d’ hypertension endocrinienne
sont aussi impliqués dans l’hypertension essentiellesont aussi impliqués dans l’hypertension essentielle
activation de l’axe rénine-angiotensine-aldostéroneactivation de l’axe rénine-angiotensine-aldostérone hyperactivité du système adréno-sympathiquehyperactivité du système adréno-sympathique
L’hypertension endocrinienne est L’hypertension endocrinienne est sous-diagnostiquéesous-diagnostiquée ! !
hyperaldostéronisme primaire fréquenthyperaldostéronisme primaire fréquent bcp de phéochromocytomes restent longtemps occultesbcp de phéochromocytomes restent longtemps occultes incidentalome et syndrome de Cushing infracliniqueincidentalome et syndrome de Cushing infraclinique

Adrenal incidentalomaAdrenal incidentaloma
multicentric italian studymulticentric italian study ( ( Mantero et al, JCEM, 2000 Mantero et al, JCEM, 2000 ) :) :
- 1004 incidentalomas + hormonal work-up- 1004 incidentalomas + hormonal work-up
- malignant and symptomatic tumors excluded- malignant and symptomatic tumors excluded
non-secreting tumornon-secreting tumor 85 %85 %
subclinical Cushing’s syndrome (SCS)subclinical Cushing’s syndrome (SCS) 9,2 %9,2 %
“ “silent” pheochromocytoma silent” pheochromocytoma 4,2 %4,2 %
primary hyperaldosteronismprimary hyperaldosteronism 1,6 %1,6 %
15 %15 %
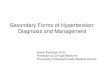
HTAHTA

1000 hypertensive patients1000 hypertensive patients
< 900 essential hypertension< 900 essential hypertension
> 100> 100 secondary hypertension secondary hypertension
50 renal hypertension50 renal hypertension
5 reno-vascular hypertension5 reno-vascular hypertension
60 60 endocrine hypertensionendocrine hypertension
33 pheochromocytomas pheochromocytomas
5050 primary hyperaldosteronism primary hyperaldosteronism
77 other endocrine causes other endocrine causes
après 2000après 2000

I. Hyperaldostéronisme primaireI. Hyperaldostéronisme primaire

L’ hyperaldostéronisme primaire “classique” de 1965 à 2000 :L’ hyperaldostéronisme primaire “classique” de 1965 à 2000 :le syndrome de Connle syndrome de Conn
HTA souvent sévère, résistante à un traitement classique HTA souvent sévère, résistante à un traitement classique
comportant au moins 2 anti-hypertenseurscomportant au moins 2 anti-hypertenseurs
hypokaliémie spontanée (ou facilement inductible par hypokaliémie spontanée (ou facilement inductible par
diurétiques ou régime riche en sel) + kaliurie > 30 mEq/24 hdiurétiques ou régime riche en sel) + kaliurie > 30 mEq/24 h
hyperaldostéronisme non suppressible par une surcharge hyperaldostéronisme non suppressible par une surcharge
sodée ou l’administration d’un minéralocorticoïdesodée ou l’administration d’un minéralocorticoïde
suppression de l’axe rénine-angiotensine (ARP ou R suppression de l’axe rénine-angiotensine (ARP ou R ))

Hyperaldostéronisme : primaire ou secondaire ?Hyperaldostéronisme : primaire ou secondaire ?
Hyperaldostéronisme Hyperaldostéronisme primaireprimaire
Hyperaldostéronisme Hyperaldostéronisme secondaire (++)secondaire (++)
• activité rénine plasmatiqueactivité rénine plasmatique (ARP) (ARP)
< 1 ng/ml/heure< 1 ng/ml/heure
• rapport aldo (ng/dl) / ARPrapport aldo (ng/dl) / ARP
> 30 (50)> 30 (50)
Nle ou Nle ou > 2 ng/ml/heure > 2 ng/ml/heure
< 20< 20
• test de surcharge salinetest de surcharge saline
aldo > 0,25 nmol/L aldo > 0,25 nmol/L ou 10 ng/dlou 10 ng/dl
(2 litres de physio / 4 heures)(2 litres de physio / 4 heures)
aldo < 0,25 nmol/l aldo < 0,25 nmol/l ou 10 ng/dlou 10 ng/dl
• test au captopriltest au captopril
pas de modification pas de modification du taux d’aldostérone du taux d’aldostérone
(50 mg per os)(50 mg per os)
aldostéronealdostérone

L’hyperaldostéronisme primaire (AP) revisité depuis l’an 2000 : L’hyperaldostéronisme primaire (AP) revisité depuis l’an 2000 : une prévalence accrue…une prévalence accrue…
plusieurs publications récentes montrent une prévalence de plusieurs publications récentes montrent une prévalence de
5 à 20%5 à 20% d’AP dans une population de patients hypertendus d’AP dans une population de patients hypertendus
(dépistage par le rapport aldostérone / rénine plasmatique)(dépistage par le rapport aldostérone / rénine plasmatique)
Lim et al, Lancet, 1999, 353: 40Lim et al, Lancet, 1999, 353: 40
Loh et al, JCEM, 2000, 85: 2854Loh et al, JCEM, 2000, 85: 2854
Fardella et al, JCEM, 2000, 85: 1863…Fardella et al, JCEM, 2000, 85: 1863…
l’hypokaliémie n’est présente que dans moins de 50% des cas !l’hypokaliémie n’est présente que dans moins de 50% des cas !
dépistage justifié si HTA (sévère) avec normokaliémiedépistage justifié si HTA (sévère) avec normokaliémie
imagerie surrénalienne souvent négative !imagerie surrénalienne souvent négative !

Diagnostic de l’hyperaldostéronisme primaire Diagnostic de l’hyperaldostéronisme primaire
dépistage :dépistage :
rapport rapport aldostérone (ng/dl)aldostérone (ng/dl) (N : 5 - 15)(N : 5 - 15)
activité rénine plasmatique (ng/ml/h)activité rénine plasmatique (ng/ml/h) (N: 0,2 – 5)(N: 0,2 – 5)
Si > 30 + aldo > 10 ng/dl (0,30 nmol/l) : forte suspicion Si > 30 + aldo > 10 ng/dl (0,30 nmol/l) : forte suspicion
Si > 50 + aldo > 15 ng/dl (0,40 nmol/l) : diagnostique Si > 50 + aldo > 15 ng/dl (0,40 nmol/l) : diagnostique
Ce rapportCe rapport varie peu varie peu avec la position, le moment du prélèvement, avec la position, le moment du prélèvement,
l’ingestion de sel, …l’ingestion de sel, …
Et les médicaments anti-hypertenseurs ??Et les médicaments anti-hypertenseurs ??

C. Seifarth et al.Clin. Endocrinol.,2002, 57 : 457
aldostéronealdostérone

C. Seifarth et al.Clin. Endocrinol.,2002, 57 : 457
réninerénine

C. Seifarth et al.,Clin. Endocrinol.,2002, 57 : 457
Rapport Rapport aldostérone/réninealdostérone/rénine

Diagnostic de l’hyperaldostéronisme primaire Diagnostic de l’hyperaldostéronisme primaire
rapport rapport aldostérone (ng/dl) aldostérone (ng/dl)
activité rénine plasmatique (ng/ml/h)activité rénine plasmatique (ng/ml/h)
Valide si : Valide si : - éventuelle hypokaliémie corrigée- éventuelle hypokaliémie corrigée
- apport en NaCl normal- apport en NaCl normal
- diurétiques, - diurétiques, -bloquants, AINS arrêtés depuis 4 semaines-bloquants, AINS arrêtés depuis 4 semaines
Faux + (rapport Faux + (rapport )) Faux – (rapport Faux – (rapport ))
-bloquants, clonidine-bloquants, clonidine diurétiques, spironolactone, IEC et diurétiques, spironolactone, IEC et
SartansSartans
AINSAINS hypokaliémiehypokaliémie
Insuffisance rénaleInsuffisance rénale HTA réno-vasculaire ou maligneHTA réno-vasculaire ou maligne
Patients âgésPatients âgés grossessegrossesse
déplétion en NaCldéplétion en NaCl

Diagnostic de l’hyperaldostéronisme primaire Diagnostic de l’hyperaldostéronisme primaire
confirmationconfirmation : :
rapport aldo / ARP très élevé > 50 + hyperaldostéronisme > 15 ng/dlrapport aldo / ARP très élevé > 50 + hyperaldostéronisme > 15 ng/dl
tests de surcharge salinetests de surcharge saline régime riche en NaCl – 3 jours (+ apports en KCl) régime riche en NaCl – 3 jours (+ apports en KCl) (Mayo clinic)(Mayo clinic)
aldostéronurie J 3 > 14 µg/24h avec Na urinaire > 200 mEq/24haldostéronurie J 3 > 14 µg/24h avec Na urinaire > 200 mEq/24h
sérum physiologique 2 litres / 4 heures ivsérum physiologique 2 litres / 4 heures iv
aldostérone plasmatique > 10 ng/dl ou 0,25 nmol/laldostérone plasmatique > 10 ng/dl ou 0,25 nmol/l
tests de suppressiontests de suppression captopril (50 mg per os)captopril (50 mg per os)
fludrocortisone (0,1 mg/6h – 4 jours) fludrocortisone (0,1 mg/6h – 4 jours)
aldo > 6 ng/dl ou 0,15 nmol/laldo > 6 ng/dl ou 0,15 nmol/l

Causes d’hyperaldostéronisme primaire Causes d’hyperaldostéronisme primaire
““APA”APA” adénome surrénalien unilatéraladénome surrénalien unilatéral 35% 35% (())
R/ chirurgicalR/ chirurgical
““BAH”BAH” hyperplasie (nodulaire) bilatérale hyperplasie (nodulaire) bilatérale 64% 64% (())
R/ médicalR/ médical
Formes familialesFormes familiales 1% 1%
type I – “GRA” – hyperaldostéronisme suppressible par les type I – “GRA” – hyperaldostéronisme suppressible par les
glucocorticoïdes – diagnostic génétique (UCL)glucocorticoïdes – diagnostic génétique (UCL)
R/ glucocorticoïdesR/ glucocorticoïdes
type II – gène non encore identifié type II – gène non encore identifié

Adénome ou hyperplasie ?Adénome ou hyperplasie ?

hyperaldostéronisme primaire : APA ou BAH ?hyperaldostéronisme primaire : APA ou BAH ?
APAAPA BAHBAH
1. Test de posture1. Test de postureSensibilité 80% Sensibilité 80%
Spécificité > 95%Spécificité > 95%Aldostérone Aldostérone ou ou Aldostérone Aldostérone de > 33% de > 33%
2. Imagerie (CT – IRM)2. Imagerie (CT – IRM)Sensibilité 70%Sensibilité 70%
Spécificité 66%Spécificité 66%
Adénome unilatéral Adénome unilatéral
(1 – 2 cm)(1 – 2 cm)
Hyperplasie bilatéraleHyperplasie bilatérale
ou surrénales normalesou surrénales normales
3. Cathétérisme des 3. Cathétérisme des veines surrénaliennesveines surrénaliennes
Sensibilité 90%Sensibilité 90%
Spécificité 95-99%Spécificité 95-99%
Gradient de Gradient de latéralisationlatéralisation
Gradient faible ou Gradient faible ou absentabsent


hyperaldostéronisme primaire : APA ou BAH ?hyperaldostéronisme primaire : APA ou BAH ?
APAAPA BAHBAH
Test de postureTest de postureSensibilité 80% Sensibilité 80%
Spécificité 95%Spécificité 95%Aldostérone Aldostérone ou ou Aldostérone Aldostérone de > 33% de > 33%
Imagerie (CT – IRM)Imagerie (CT – IRM)Sensibilité 70%Sensibilité 70%
Spécificité 66%Spécificité 66%
Adénome unilatéral Adénome unilatéral
(si (si >> 1 cm) 1 cm)
Hyperplasie bilatéraleHyperplasie bilatérale
ou surrénales normalesou surrénales normales
Cathétérisme des Cathétérisme des veines surrénaliennesveines surrénaliennes
Sensibilité 90%Sensibilité 90%
Spécificité 95-99%Spécificité 95-99%
Gradient de Gradient de latéralisationlatéralisation
Gradient faible ou Gradient faible ou absentabsent

Mr G.DM. : CT Scan abdominalMr G.DM. : CT Scan abdominal
surrénale surrénale gauchegauche
Adénome Adénome surrénalien surrénalien
droit droit 9 x 1,3 cm9 x 1,3 cm

Hyperaldostéronisme primaireHyperaldostéronisme primaire
IRM abdominale montrant une hyperplasie surrénalienne bilatéraleIRM abdominale montrant une hyperplasie surrénalienne bilatérale

hyperaldostéronisme primaire : APA ou BAH ?hyperaldostéronisme primaire : APA ou BAH ?
APAAPA BAHBAH
Test de postureTest de postureSensibilité 80% Sensibilité 80%
Spécificité 95%Spécificité 95%Aldostérone Aldostérone ou ou Aldostérone Aldostérone de > 33% de > 33%
Imagerie (CT – IRM)Imagerie (CT – IRM)Sensibilité 70%Sensibilité 70%
Spécificité 66%Spécificité 66%
Adénome unilatéral Adénome unilatéral
(1 – 2 cm)(1 – 2 cm)
Hyperplasie bilatéraleHyperplasie bilatérale
ou surrénales normalesou surrénales normales
Cathétérisme des Cathétérisme des veines surrénaliennesveines surrénaliennes
Sensibilité 90%Sensibilité 90%
Spécificité 95-99%Spécificité 95-99%
Gradient de Gradient de latéralisationlatéralisation
Gradient faible ou Gradient faible ou absentabsent

Cortisol (nM) Aldo ( nM) Aldo/Cortisol
V.C I. partie supérieure 349 1.86 0.5
V.C.I. hauteur A. rénales 403 2.21 0.5
V.C. I. partie inférieure 402 2.02 0.5
V. rénale G proximale 437 2.44 0.5
V. rénale G distale 431 2.24 0.5
V. surrénalienne G 15 095 5.5 0.03
V. surrénalienne Dr 1735 33 1.9
V. rénale polaire Dr 446 1.43 0.3
V. rénale Dr 424 2.27 0.5
Cathétérisme des veines surrénaliennes

Monsieur G. DM. : cathétérisme des veines surrénaliennes Monsieur G. DM. : cathétérisme des veines surrénaliennes (rapports cortisol /aldo)(rapports cortisol /aldo)
v. surr. gauchev. surr. gauche
v. surr. droitev. surr. droite
v. rénale polaire Dv. rénale polaire D
v. rénale Dv. rénale D v. rénale Gv. rénale G
V.C.I. infrarénaleV.C.I. infrarénale
V.C.I. suprarénaleV.C.I. suprarénale
0.50.5
0.50.5
0.50.50.50.5
0.030.030.30.3
1.91.9 0.50.5
0.50.5
Gradient ipsilatéral 1.9 / 0.5 = 3.8 (> 2)Gradient ipsilatéral 1.9 / 0.5 = 3.8 (> 2) Gradient controlatéral 0.03 / 0.5 = 0.06 (< 1)Gradient controlatéral 0.03 / 0.5 = 0.06 (< 1)
Gradient de latéralisation Gradient de latéralisation
1.9 / 0.03 = 63 ( > 4)1.9 / 0.03 = 63 ( > 4)

Hyperaldostéronisme primaireHyperaldostéronisme primaire
Test de postureTest de posture
Cathétérisme des veines Cathétérisme des veines surrénaliennessurrénaliennes
aldostérone deboutaldostérone debout+ adénome unilatéral+ adénome unilatéralchez patient < 40 anschez patient < 40 ans
Imagerie (CT / IRM)Imagerie (CT / IRM)++
APAAPA
chirurgiechirurgie
G-ipsi > 2G-ipsi > 2G-contro < 1G-contro < 1G-latér > 5G-latér > 5
Pas de gradientPas de gradient
BHABHA
R/ médicalR/ médical
Dans tous les autres casDans tous les autres cas
Si jeune âge, antéc. Si jeune âge, antéc. familiaux + :familiaux + :exclure GRAexclure GRA
??

M. Stowasser et R.D. Gordon.M. Stowasser et R.D. Gordon.
Primary aldosteronismPrimary aldosteronism
Best Practice & Research Clin Endocrinology and MetabolismBest Practice & Research Clin Endocrinology and Metabolism
2003; 591-605.2003; 591-605.

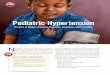
II. PhéochromocytomeII. Phéochromocytome

tachycardiatachycardia inotropic effectinotropic effect
Main effects of catecholamines on theMain effects of catecholamines on thecardio-vascular systemcardio-vascular system
DopamineDopamine
NorepinephrineNorepinephrineSympathetic nervousSympathetic nervous
systemsystempotentpotent
vasoconstrictionvasoconstriction
1- receptors1- receptors(vascular bed)(vascular bed)++
(300 pg/ml)(300 pg/ml)
AdrenalAdrenalmedullamedulla EpinephrineEpinephrine
(30 pg/ml)(30 pg/ml)
DopamineDopamine
DA-receptorsDA-receptors(vascular bed)(vascular bed)
vasodilationvasodilation
1- receptors1- receptors(heart)(heart)
22- receptors- receptors(vascular bed)(vascular bed)
vasodilationvasodilation

Pheochromocytoma Pheochromocytoma
considered as a rare cause of hypertension (0.1 - 0.2 %)considered as a rare cause of hypertension (0.1 - 0.2 %)
only 1 pheochromocytoma discovered in 100 investigations only 1 pheochromocytoma discovered in 100 investigations
for paroxystic HTAfor paroxystic HTA
a rare tumor ...a rare tumor ...

Pheochromocytoma Pheochromocytoma
4-8% of incidentally-discovered adrenal masses4-8% of incidentally-discovered adrenal masses
75% of pheos discovered at autopsy remain undiagnosed 75% of pheos discovered at autopsy remain undiagnosed
before death before death (Mayo Clinic Series)(Mayo Clinic Series)
50% of the cases are normotensive between spells50% of the cases are normotensive between spells
… … but underdiagnosed !but underdiagnosed !

Pheochromocytoma : the rule of 10%Pheochromocytoma : the rule of 10%
10%10% of pheochromocytomas ... of pheochromocytomas ...
are incidentally discoveredare incidentally discovered
are extra-adrenal (« are extra-adrenal (« paragangliomasparagangliomas ») »)
are multiple / bilateralare multiple / bilateral
are or will become malignantare or will become malignant
occur in childrenoccur in children
are familial (probably more …)are familial (probably more …)
will recurwill recur

Pheochromocytoma : clinical symptomsPheochromocytoma : clinical symptoms
paroxysmalparoxysmal (50%) or (50%) or persistentpersistent (50%) (50%) hypertensionhypertension - -
often severe and refractory to treatmentoften severe and refractory to treatment
-- headachesheadaches 70%70% - abdominal pain- abdominal pain 25%25%
-- perspirationsperspirations 65%65% - chest pain- chest pain 20%20%
-- palpitationspalpitations 65%65% - weakness- weakness 20%20%
- pallor- pallor 45%45% - dyspnea- dyspnea 20%20%
- nausea- nausea 35%35% - weight loss- weight loss 15%15%
- tremor- tremor 30%30% - visual disturbances- visual disturbances 15%15%
- anxiety- anxiety 30%30% - polyuria, polydipsia- polyuria, polydipsia 10%10%
spellsspells of any of the following symptoms : of any of the following symptoms :
« pheo’s « pheo’s triad »triad »

Pheochromocytoma : clinical symptomsPheochromocytoma : clinical symptoms
spontaneous spells or spells provoked by exercise, spontaneous spells or spells provoked by exercise, twisting, twisting,
turning, straining, micturition, coitus, surgical turning, straining, micturition, coitus, surgical procedure, delivery, procedure, delivery,
abortion, ….abortion, ….
frequency of spells : 1 every 2-3 months frequency of spells : 1 every 2-3 months 25 every day ! 25 every day !
duration of spells : usually 1 to 30 minutes duration of spells : usually 1 to 30 minutes

Pheochromocytoma :Pheochromocytoma :who should be screened for?who should be screened for?
paroxysmal or markedly fluctuating hypertensionparoxysmal or markedly fluctuating hypertension
“ “spells” of any symptoms + hypertensionspells” of any symptoms + hypertension
pheo’s triad [headaches + sweating + palpitations] pheo’s triad [headaches + sweating + palpitations]
refractoriness to conventional anti-hypertensive refractoriness to conventional anti-hypertensive treatmenttreatment
(orthostatic) hypotension alternating with hypertension(orthostatic) hypotension alternating with hypertension
paradoxical hypertensive response to beta-blockersparadoxical hypertensive response to beta-blockers
adrenal incidentalomaadrenal incidentaloma
familial history of pheochromocytoma, MEN2 syndrome, ...familial history of pheochromocytoma, MEN2 syndrome, ...
personal history of a predisposing diseasepersonal history of a predisposing disease (von-Hippel-Lindau, MEN2, neurofibromatosis, …)(von-Hippel-Lindau, MEN2, neurofibromatosis, …)

Pheochromocytoma : how to screen ?Pheochromocytoma : how to screen ?
Biochemical testBiochemical test reference valuereference value sensitivitysensitivity specificityspecificity
urinary NMN + MNurinary NMN + MN > 1.2 mg/24h> 1.2 mg/24h 90-95%90-95% 98%98%
urinary NE + Eurinary NE + E > 200 µg/24 h> 200 µg/24 h 80-85%80-85% 98%98%
urinary VMAurinary VMA > 11 mg/24h> 11 mg/24h 30-35%30-35% 99-100%99-100%
urinary NE + Eurinary NE + E > 200 µg/24h> 200 µg/24h
or urinary NMN + MNor urinary NMN + MN > 1.2 mg/24h> 1.2 mg/24h
plasma NE + Eplasma NE + E > 1000 pg/ml> 1000 pg/ml 88-90%88-90% 90%90%
> 2000 pg/ml> 2000 pg/ml lowlow 100%100%
In most cases, urinary mets + cats are diagnosticIn most cases, urinary mets + cats are diagnosticNo test has 100% sensitivity + 100% specificity !No test has 100% sensitivity + 100% specificity !
98%98% 98%98%

Pheochromocytoma : Pheochromocytoma : value of fractionated plasma metanephrinesvalue of fractionated plasma metanephrines
A. Sawka et al., JCEM, 2003A. Sawka et al., JCEM, 2003
pheopheo controlscontrols pheopheo controlscontrols
Sensitivity = 99% specificity = 85%Sensitivity = 99% specificity = 85%
May be useful if high suspicionMay be useful if high suspicion

Non-pheochromocytoma (n=15)
20000
1000080006000
2000
1000800600
400
200
100
4000
Basal Post-clonidine
Pla
sma
no
rep
inep
hri
ne
(pg
/ml)
Pheochromocytoma : the clonidine suppression test
Pheochromocytoma (n=10)

Pheochromocytoma : how to localize ?Pheochromocytoma : how to localize ?
SensitivitySensitivity SpecificitySpecificity
CT-ScanCT-Scan 97%97% 70%70%
MRIMRI 99%99% 80%80%
131131I-MIBGI-MIBG 80%80% 100%100%
111111In-octreoscanIn-octreoscan 70%70% 95%95%
PET-ScanPET-Scan ?? ??
(FDG, fluorodopamine)(FDG, fluorodopamine)

Pheochromocytoma : magnetic resonance imaging
T1-weighed image T2-weighed image

Lateral R
R Ant
Pheochromocytoma : 131-I MIBG Scanning
Posterior

Familial pheochromocytomaFamilial pheochromocytoma
• multiple endocrine neoplasia type II (MEN IIa, MEN IIb)multiple endocrine neoplasia type II (MEN IIa, MEN IIb)
• von Hippel-Lindau disease (VHL type 2)von Hippel-Lindau disease (VHL type 2)
• von Recklinghausen’s neurofibromatosis von Recklinghausen’s neurofibromatosis
• hereditary paragangliomahereditary paraganglioma
• familial isolated pheochromocytomafamilial isolated pheochromocytoma

Clinical suspicion of pheochromocytomaClinical suspicion of pheochromocytoma
2-fold increase U-cats2-fold increase U-catsU-mets > 1.2 mg/24 hU-mets > 1.2 mg/24 hpositive clonidine testpositive clonidine test
(( plasma mets) plasma mets)
lowlow
24h-urinary mets+cats24h-urinary mets+cats
Other causes Other causes of spells?of spells?
highhigh
- 24h-urinary mets+cats- 24h-urinary mets+cats- clonidine test- clonidine test- (plasma mets)- (plasma mets)
recheck after a spellrecheck after a spell do a provocative test ?do a provocative test ?
Other causes Other causes of spells?of spells?
Abdominal MRI / CTAbdominal MRI / CT131131I-MIBGI-MIBG
Pheochro-Pheochro-mocytomamocytoma
PreparationPreparation+ surgery+ surgery
negativenegative
Whole body MRIWhole body MRIoctreo-scanoctreo-scanPET-scanPET-scan
Other causes of Other causes of hypercate-hypercate-
cholaminemiacholaminemia
++++
--
++
++
++
----
--
--

Maiter D. Maiter D.
Pheochromocytoma: a paradigm for catecholamine-mediated Pheochromocytoma: a paradigm for catecholamine-mediated hypertensionhypertension
Acta Clin Belg, 2004, 59: 209-219.Acta Clin Belg, 2004, 59: 209-219.


















![VA/DoD Hypertension Clinical Practice Guideline · ] Secondary hypertension is high blood pressure that results from an underlying and identifiable cause. [3] Main causes o f secondary](https://img.pdfslide.net/doc/110x75/5dd0e688d6be591ccb633edb/vadod-hypertension-clinical-practice-guideline-secondary-hypertension-is-high.jpg)






