Embed Size (px)
Citation preview
Research Forum Abstracts
and the actual outcome for the same subject. The closer the score is to 0, the betterthe predictions.
Results: The study enrolled 497 patients between June 9, 2010 and February 28,2013. Of these patients, 377 (76%) had no 30-day adverse events, 39 (8%) had an AF-related ED return visit, 32 (6%) were hospitalized for AF-related problem, 13 (3%)patients suffered strokes, and 4 (<1%) had an AF-related death. The ORs (95% CI)for the decision aid in the original derivation cohort and in this validation cohort arereported in the Table. The c-statistic was 0.66 (95% CI, 0.6 to 0.71), which is similarto the c-statistic of 0.67 (95% CI, 0.63 to 0.71) obtained from the derivation cohort.The mean Brier scores for the decision aid’s performance at predicting the occurrenceof a 30-day adverse event was 0.06.
Conclusion: We found that our previously derived decision aid performed well in aprospective cohort of ED patients with symptomatic AF. This validation studysupports that increased patient age, inadequate 2-hour ventricular rate control,impaired respiratory status, and smoking history increase AF patient’s risk for 30-dayadverse events.
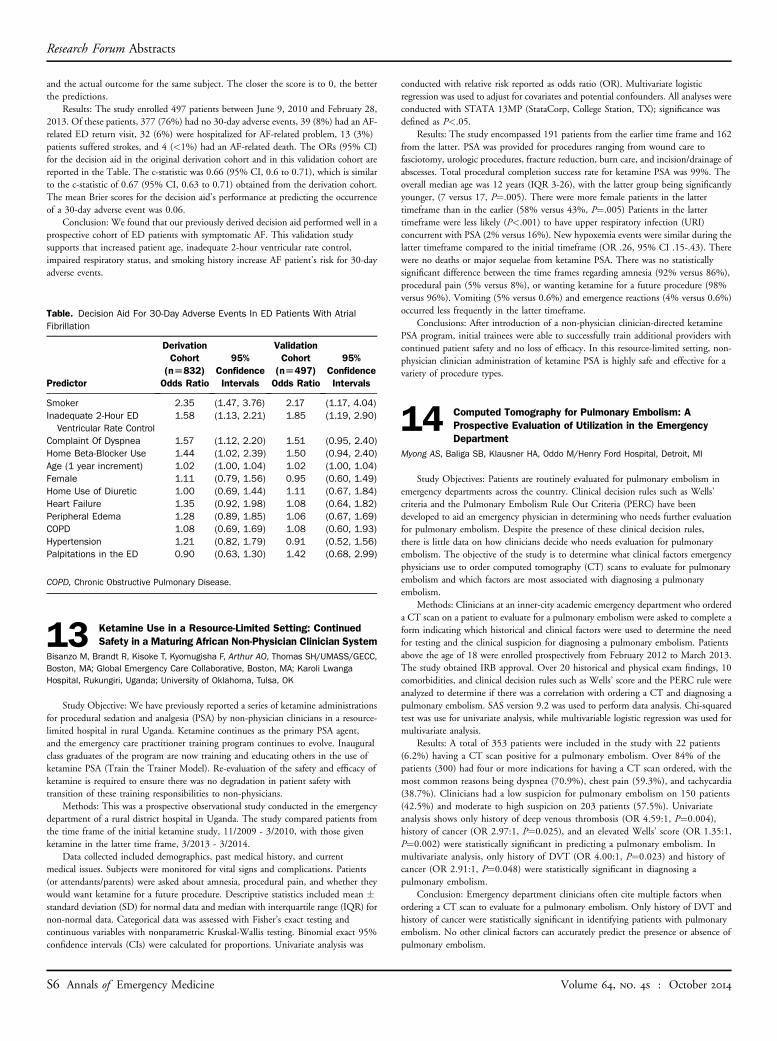
Table. Decision Aid For 30-Day Adverse Events In ED Patients With AtrialFibrillation
Derivation Validation
Predictor
S6 Annals of Emergen
Cohort(n[832)Odds Ratio
cy Medicine
95%ConfidenceIntervals
Cohort(n[497)Odds Ratio
95%ConfidenceIntervals
Smoker
2.35 (1.47, 3.76) 2.17 (1.17, 4.04) Inadequate 2-Hour EDVentricular Rate Control
1.58 (1.13, 2.21) 1.85 (1.19, 2.90)Complaint Of Dyspnea
1.57 (1.12, 2.20) 1.51 (0.95, 2.40) Home Beta-Blocker Use 1.44 (1.02, 2.39) 1.50 (0.94, 2.40) Age (1 year increment) 1.02 (1.00, 1.04) 1.02 (1.00, 1.04) Female 1.11 (0.79, 1.56) 0.95 (0.60, 1.49) Home Use of Diuretic 1.00 (0.69, 1.44) 1.11 (0.67, 1.84) Heart Failure 1.35 (0.92, 1.98) 1.08 (0.64, 1.82) Peripheral Edema 1.28 (0.89, 1.85) 1.06 (0.67, 1.69) COPD 1.08 (0.69, 1.69) 1.08 (0.60, 1.93) Hypertension 1.21 (0.82, 1.79) 0.91 (0.52, 1.56) Palpitations in the ED 0.90 (0.63, 1.30) 1.42 (0.68, 2.99)COPD, Chronic Obstructive Pulmonary Disease.
Ketamine Use in a Resource-Limited Setting: Continued
13 Safety in a Maturing African Non-Physician Clinician SystemBisanzo M, Brandt R, Kisoke T, Kyomugisha F, Arthur AO, Thomas SH/UMASS/GECC,Boston, MA; Global Emergency Care Collaborative, Boston, MA; Karoli LwangaHospital, Rukungiri, Uganda; University of Oklahoma, Tulsa, OKStudy Objective: We have previously reported a series of ketamine administrationsfor procedural sedation and analgesia (PSA) by non-physician clinicians in a resource-limited hospital in rural Uganda. Ketamine continues as the primary PSA agent,and the emergency care practitioner training program continues to evolve. Inauguralclass graduates of the program are now training and educating others in the use ofketamine PSA (Train the Trainer Model). Re-evaluation of the safety and efficacy ofketamine is required to ensure there was no degradation in patient safety withtransition of these training responsibilities to non-physicians.
Methods: This was a prospective observational study conducted in the emergencydepartment of a rural district hospital in Uganda. The study compared patients fromthe time frame of the initial ketamine study, 11/2009 - 3/2010, with those givenketamine in the latter time frame, 3/2013 - 3/2014.
Data collected included demographics, past medical history, and currentmedical issues. Subjects were monitored for vital signs and complications. Patients(or attendants/parents) were asked about amnesia, procedural pain, and whether theywould want ketamine for a future procedure. Descriptive statistics included mean �standard deviation (SD) for normal data and median with interquartile range (IQR) fornon-normal data. Categorical data was assessed with Fisher’s exact testing andcontinuous variables with nonparametric Kruskal-Wallis testing. Binomial exact 95%confidence intervals (CIs) were calculated for proportions. Univariate analysis was
conducted with relative risk reported as odds ratio (OR). Multivariate logisticregression was used to adjust for covariates and potential confounders. All analyses wereconducted with STATA 13MP (StataCorp, College Station, TX); significance wasdefined as P<.05.
Results: The study encompassed 191 patients from the earlier time frame and 162from the latter. PSA was provided for procedures ranging from wound care tofasciotomy, urologic procedures, fracture reduction, burn care, and incision/drainage ofabscesses. Total procedural completion success rate for ketamine PSA was 99%. Theoverall median age was 12 years (IQR 3-26), with the latter group being significantlyyounger, (7 versus 17, P¼.005). There were more female patients in the lattertimeframe than in the earlier (58% versus 43%, P¼.005) Patients in the lattertimeframe were less likely (P<.001) to have upper respiratory infection (URI)concurrent with PSA (2% versus 16%). New hypoxemia events were similar during thelatter timeframe compared to the initial timeframe (OR .26, 95% CI .15-.43). Therewere no deaths or major sequelae from ketamine PSA. There was no statisticallysignificant difference between the time frames regarding amnesia (92% versus 86%),procedural pain (5% versus 8%), or wanting ketamine for a future procedure (98%versus 96%). Vomiting (5% versus 0.6%) and emergence reactions (4% versus 0.6%)occurred less frequently in the latter timeframe.
Conclusions: After introduction of a non-physician clinician-directed ketaminePSA program, initial trainees were able to successfully train additional providers withcontinued patient safety and no loss of efficacy. In this resource-limited setting, non-physician clinician administration of ketamine PSA is highly safe and effective for avariety of procedure types.
Computed Tomography for Pulmonary Embolism: A
14 Prospective Evaluation of Utilization in the EmergencyDepartmentMyong AS, Baliga SB, Klausner HA, Oddo M/Henry Ford Hospital, Detroit, MI
Study Objectives: Patients are routinely evaluated for pulmonary embolism inemergency departments across the country. Clinical decision rules such as Wells’criteria and the Pulmonary Embolism Rule Out Criteria (PERC) have beendeveloped to aid an emergency physician in determining who needs further evaluationfor pulmonary embolism. Despite the presence of these clinical decision rules,there is little data on how clinicians decide who needs evaluation for pulmonaryembolism. The objective of the study is to determine what clinical factors emergencyphysicians use to order computed tomography (CT) scans to evaluate for pulmonaryembolism and which factors are most associated with diagnosing a pulmonaryembolism.
Methods: Clinicians at an inner-city academic emergency department who ordereda CT scan on a patient to evaluate for a pulmonary embolism were asked to complete aform indicating which historical and clinical factors were used to determine the needfor testing and the clinical suspicion for diagnosing a pulmonary embolism. Patientsabove the age of 18 were enrolled prospectively from February 2012 to March 2013.The study obtained IRB approval. Over 20 historical and physical exam findings, 10comorbidities, and clinical decision rules such as Wells’ score and the PERC rule wereanalyzed to determine if there was a correlation with ordering a CT and diagnosing apulmonary embolism. SAS version 9.2 was used to perform data analysis. Chi-squaredtest was use for univariate analysis, while multivariable logistic regression was used formultivariate analysis.
Results: A total of 353 patients were included in the study with 22 patients(6.2%) having a CT scan positive for a pulmonary embolism. Over 84% of thepatients (300) had four or more indications for having a CT scan ordered, with themost common reasons being dyspnea (70.9%), chest pain (59.3%), and tachycardia(38.7%). Clinicians had a low suspicion for pulmonary embolism on 150 patients(42.5%) and moderate to high suspicion on 203 patients (57.5%). Univariateanalysis shows only history of deep venous thrombosis (OR 4.59:1, P¼0.004),history of cancer (OR 2.97:1, P¼0.025), and an elevated Wells’ score (OR 1.35:1,P¼0.002) were statistically significant in predicting a pulmonary embolism. Inmultivariate analysis, only history of DVT (OR 4.00:1, P¼0.023) and history ofcancer (OR 2.91:1, P¼0.048) were statistically significant in diagnosing apulmonary embolism.
Conclusion: Emergency department clinicians often cite multiple factors whenordering a CT scan to evaluate for a pulmonary embolism. Only history of DVT andhistory of cancer were statistically significant in identifying patients with pulmonaryembolism. No other clinical factors can accurately predict the presence or absence ofpulmonary embolism.
Volume 64, no. 4s : October 2014





























