Embed Size (px)
Citation preview

2013 Lymphoma Update
2013.08.05
Outline
• Follicular lymphoma• Hodgkin’s lymphoma• Chronic lymphocytic leukemia
Follicular Lymphoma
Epidemiology of FL
• Account 22% of NHL• Chronic relapsing and remitting pattern• Most patients aged > 50• Median survival 12~14 years
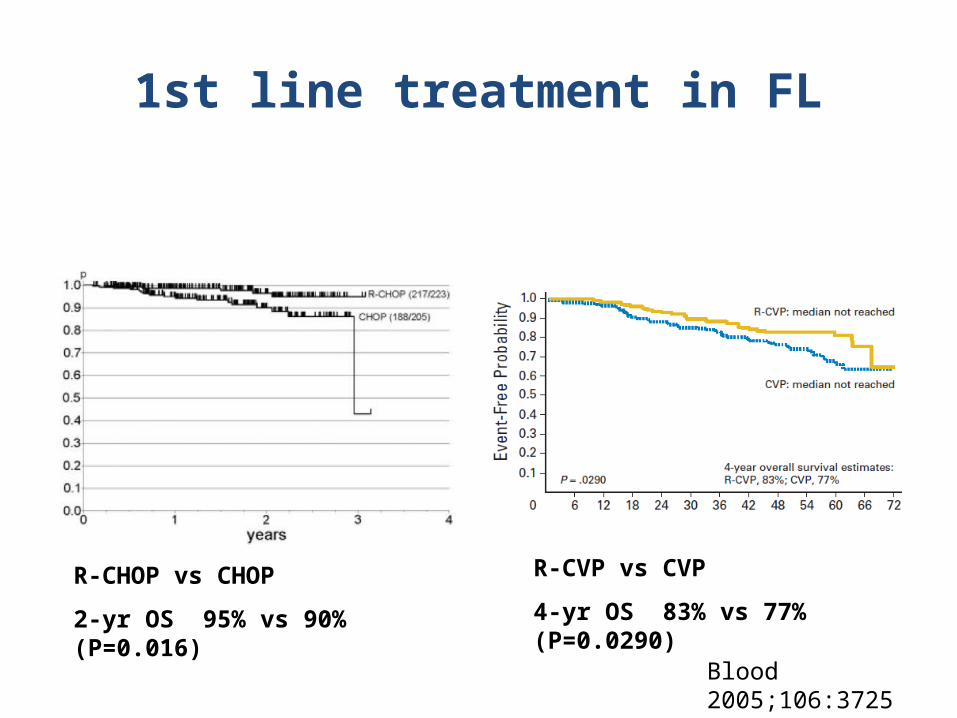
1st line treatment in FL
Blood 2005;106:3725Lancet 2013;381:1203
R-CVP vs CVP
4-yr OS 83% vs 77% (P=0.0290) R-CHOP vs CHOP
2-yr OS 95% vs 90% (P=0.016)
Standard care with indolent lymphoma
• There’s still a role for watch& wait, despite new therapy modalities
• Combined immuno-chemotherapy is standard of care
• Rituximab maintenance as consolidation
• Which chemotherapy should be best combined with Rituximab?
New perspectives
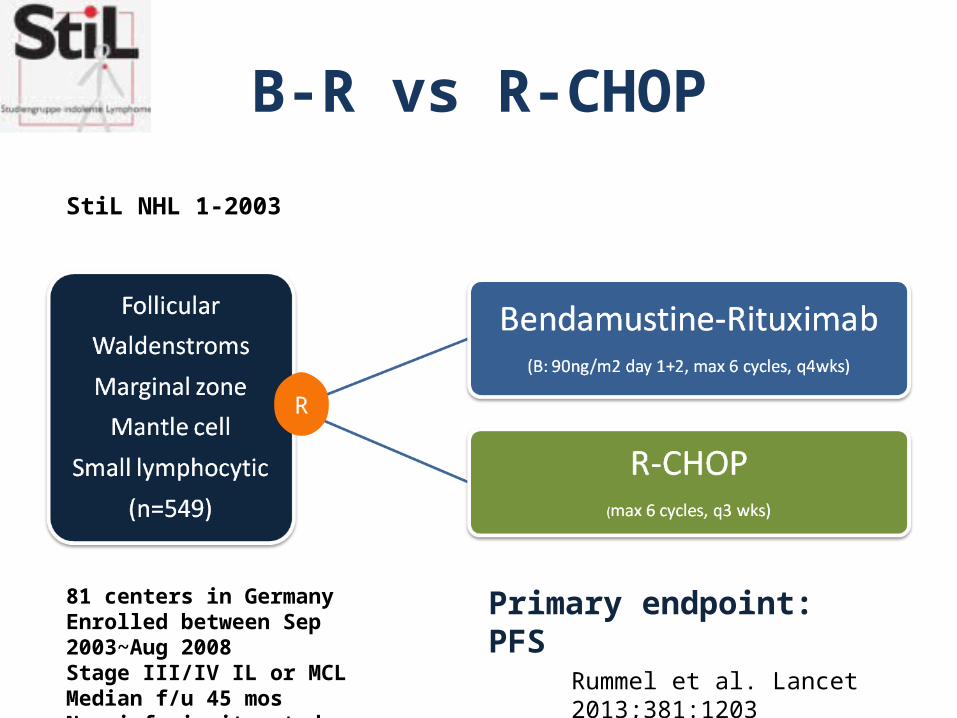
B-R vs R-CHOP
StiL NHL 1-2003
R
Rummel et al. Lancet 2013;381:1203
Primary endpoint: PFS81 centers in GermanyEnrolled between Sep 2003~Aug 2008Stage III/IV IL or MCLMedian f/u 45 mosNon-inferiority study
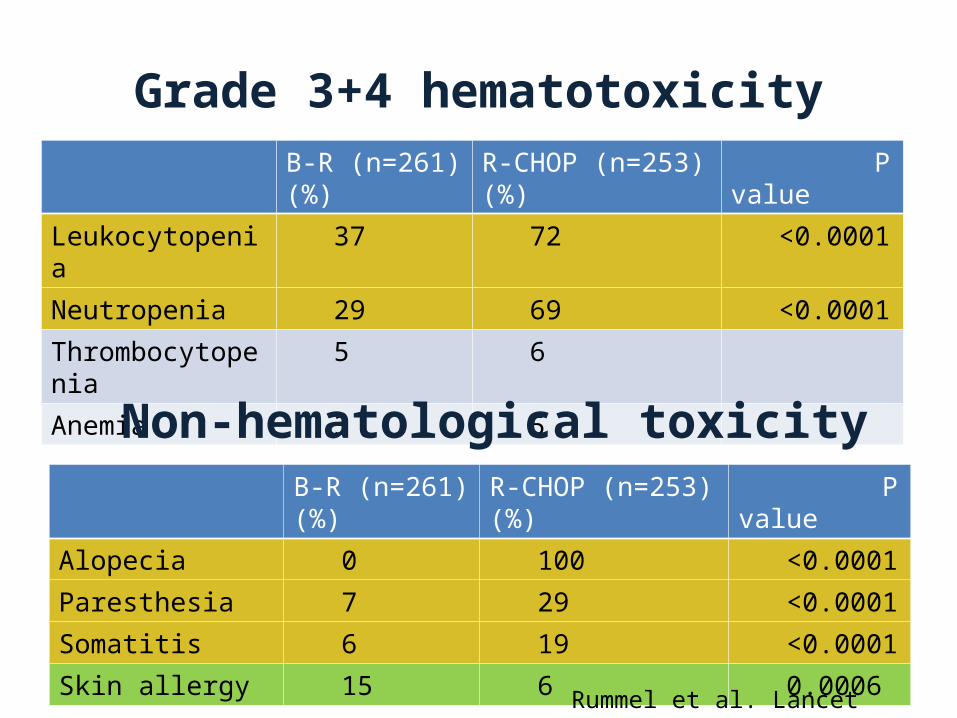
Grade 3+4 hematotoxicityB-R (n=261) (%) R-CHOP (n=253)(%) P value
Leukocytopenia 37 72 <0.0001
Neutropenia 29 69 <0.0001
Thrombocytopenia 5 6
Anemia 3 5
B-R (n=261) (%) R-CHOP (n=253)(%) P value
Alopecia 0 100 <0.0001
Paresthesia 7 29 <0.0001
Somatitis 6 19 <0.0001
Skin allergy 15 6 0.0006
Non-hematological toxicity
Rummel et al. Lancet 2013;381:1203
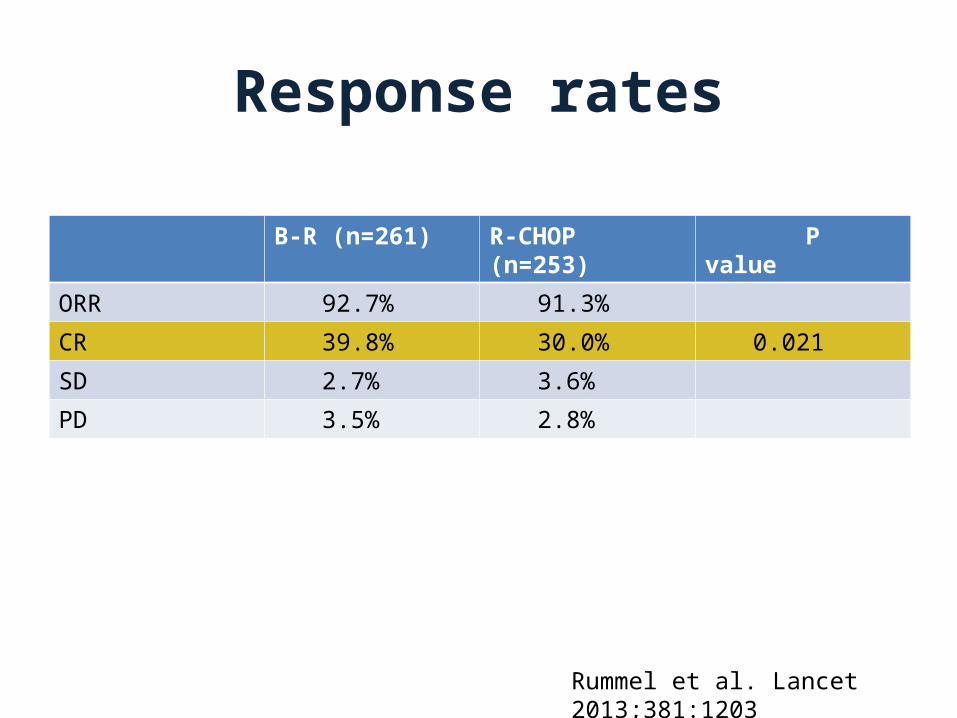
Response rates
B-R (n=261) R-CHOP (n=253) P value
ORR 92.7% 91.3%
CR 39.8% 30.0% 0.021
SD 2.7% 3.6%
PD 3.5% 2.8%
Rummel et al. Lancet 2013;381:1203
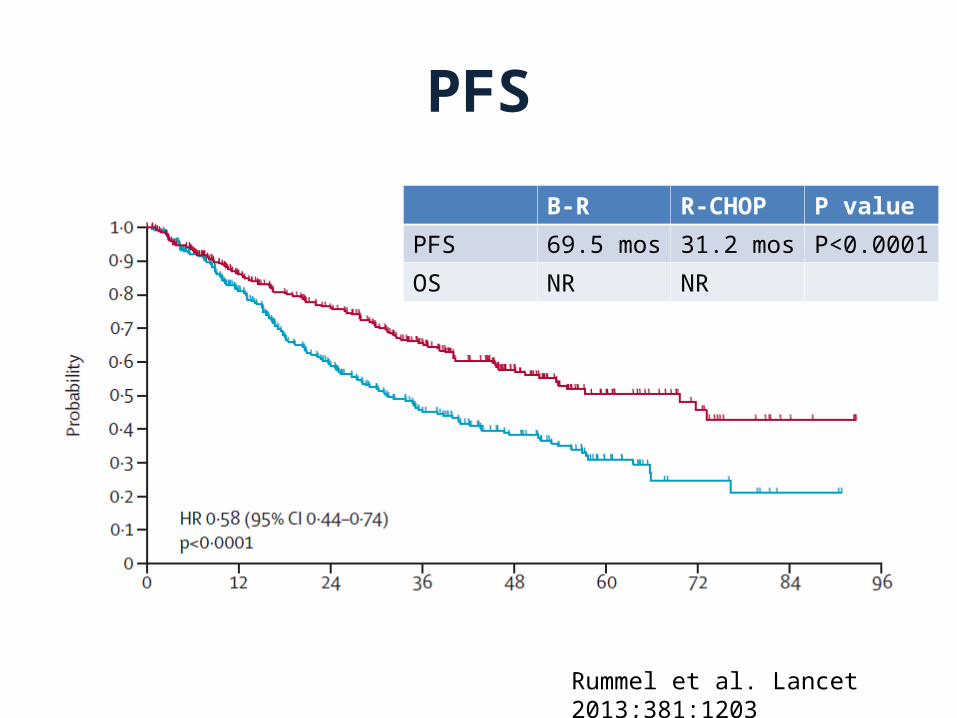
PFS
Rummel et al. Lancet 2013;381:1203
B-R R-CHOP P value
PFS 69.5 mos 31.2 mos P<0.0001
OS NR NR
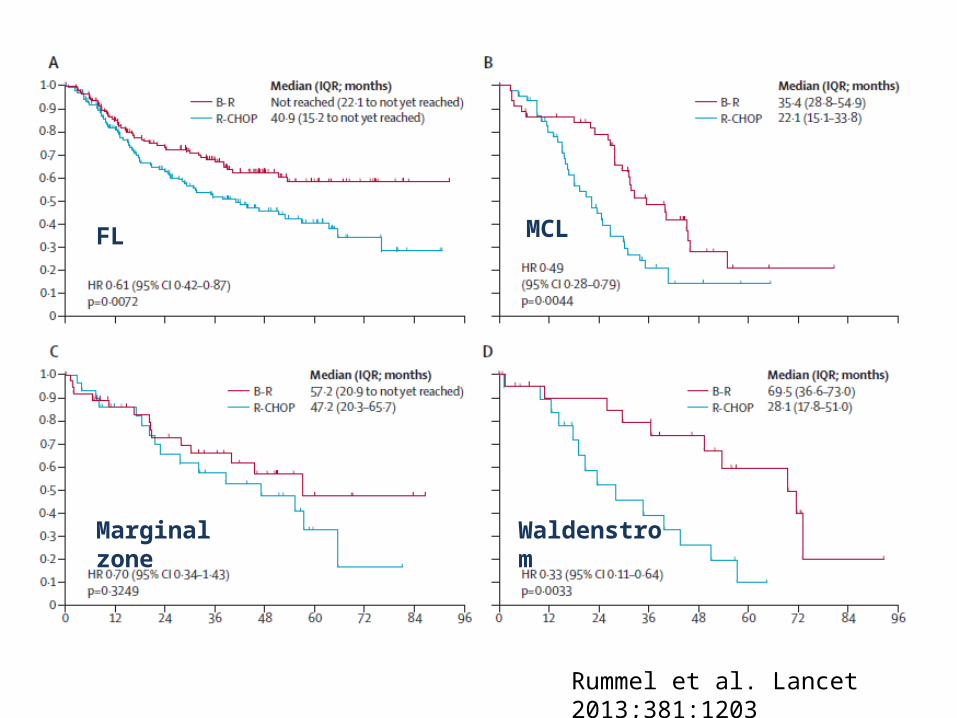
FL MCL
Marginal zone Waldenstrom
Rummel et al. Lancet 2013;381:1203
Conclusion
• B-R is not only less toxic but also more effective than R-CHOP
• B-R could be considered as a preferred 1st-line treatment for patients with FL, indolent and MCL
Rummel et al. Lancet 2013;381:1203
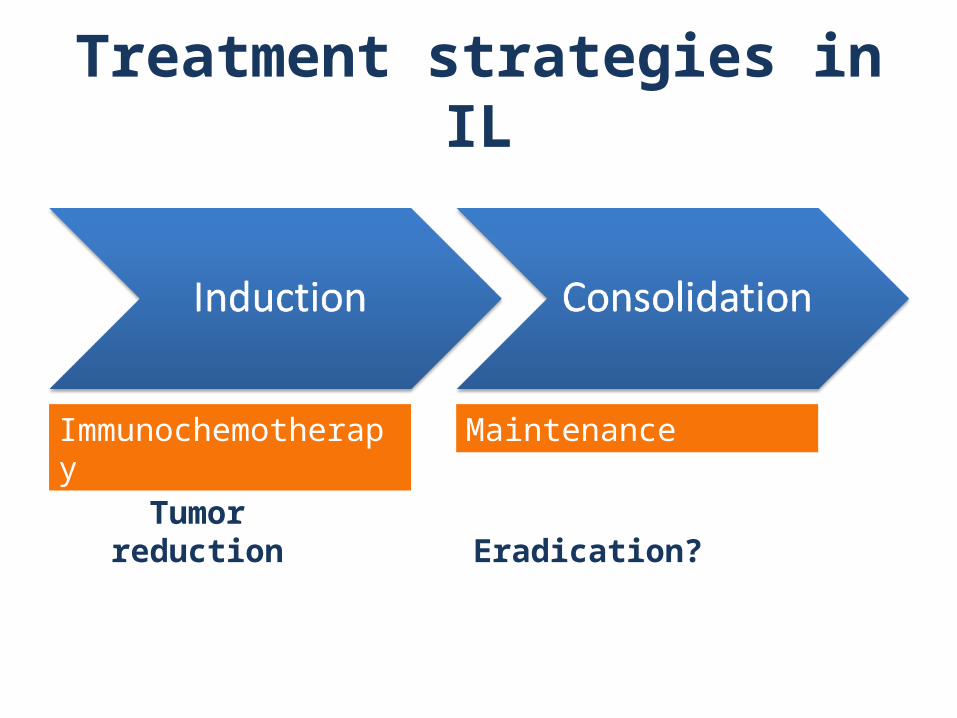
Treatment strategies in IL
Immunochemotherapy Maintenance
Tumor reduction Eradication?
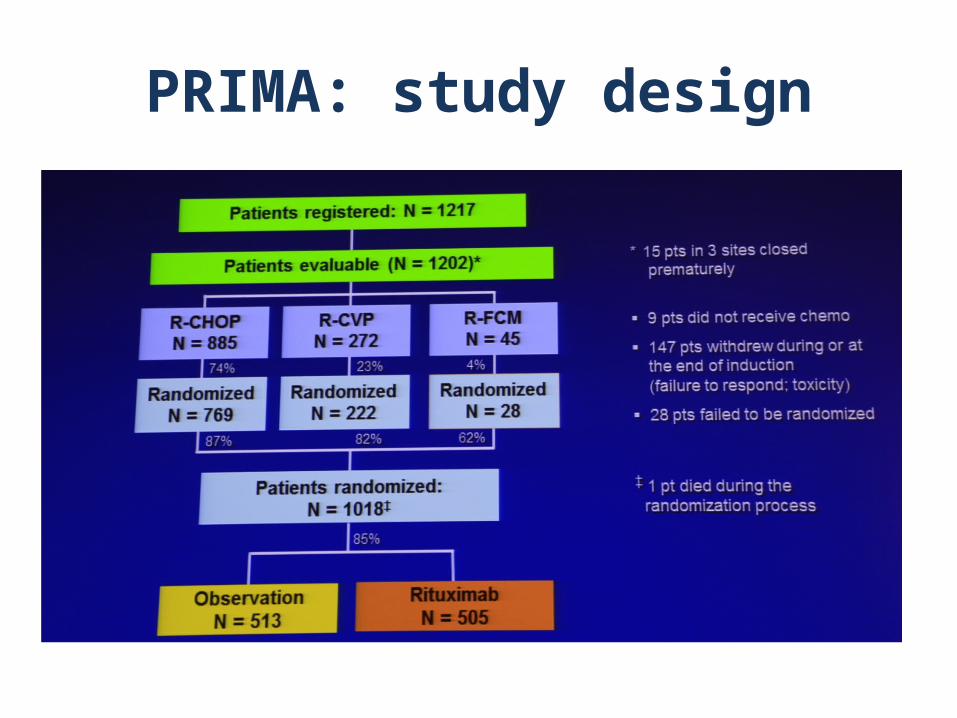
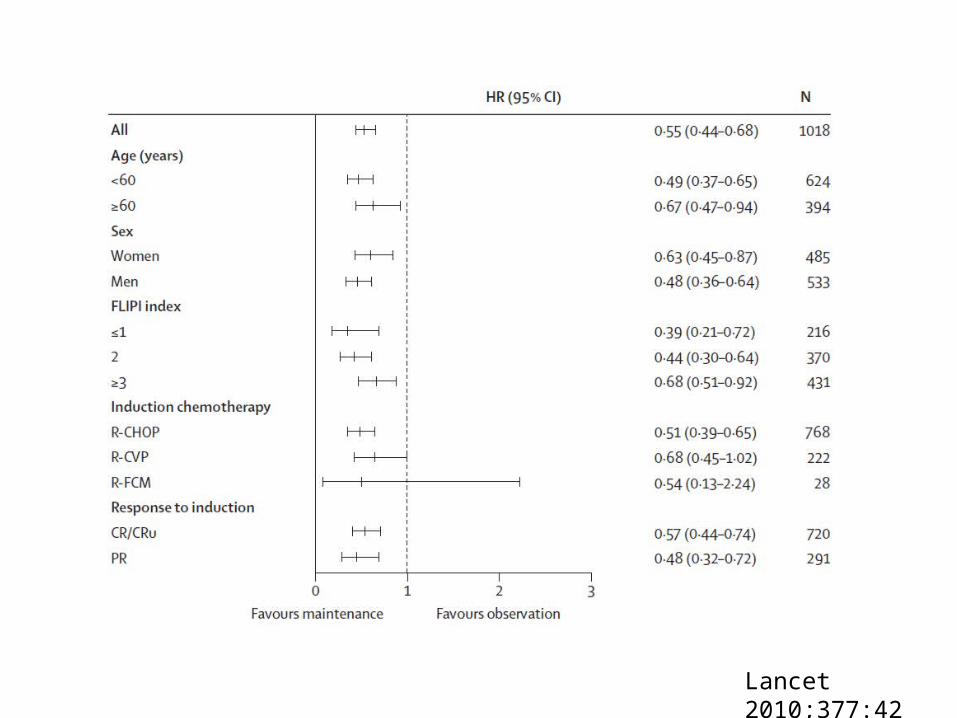
PRIMA: study design
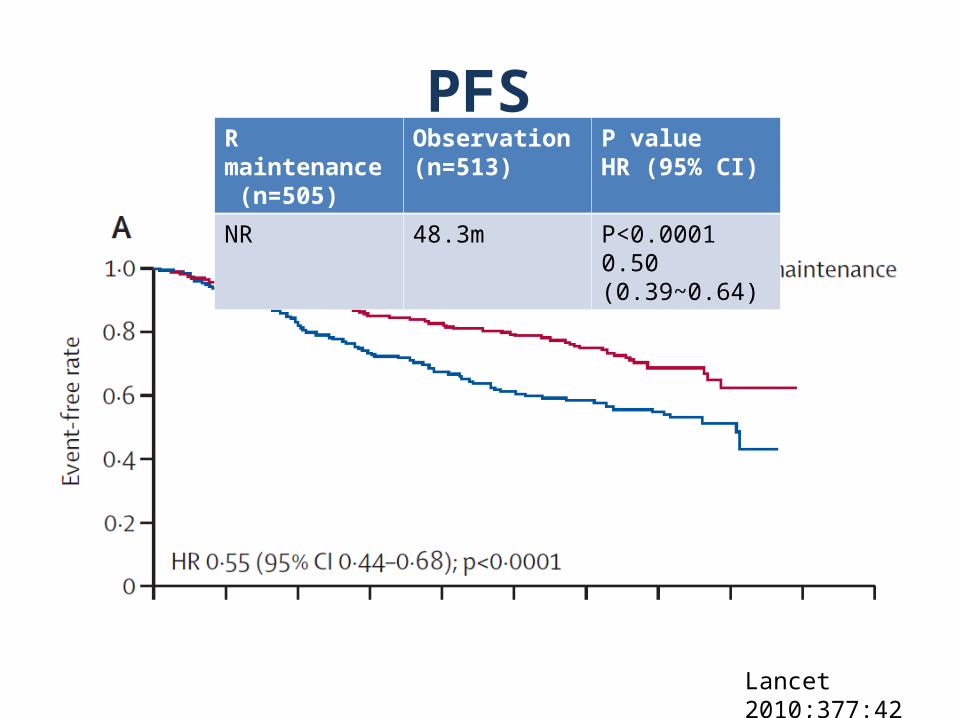
PFSR maintenance (n=505)
Observation(n=513)
P valueHR (95% CI)
NR 48.3m P<0.00010.50 (0.39~0.64)
Lancet 2010;377:42
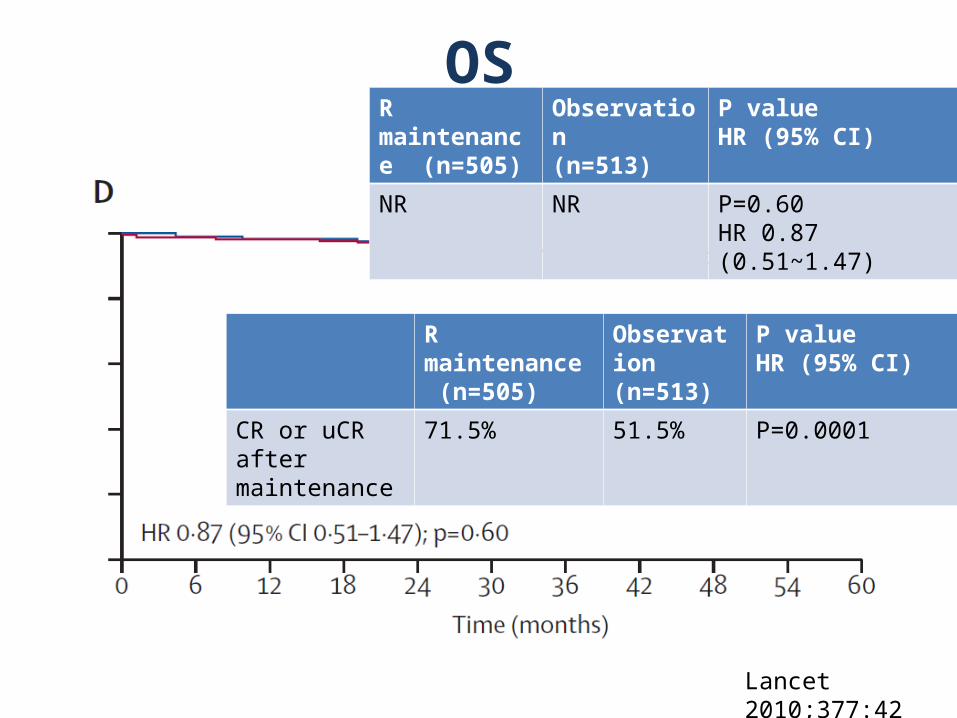
R maintenance (n=505)
Observation(n=513)
P valueHR (95% CI)
NR NR P=0.60HR 0.87 (0.51~1.47)
Lancet 2010;377:42
R maintenance (n=505)
Observation(n=513)
P valueHR (95% CI)
CR or uCR after maintenance
71.5% 51.5% P=0.0001
OS
Lancet 2010;377:42
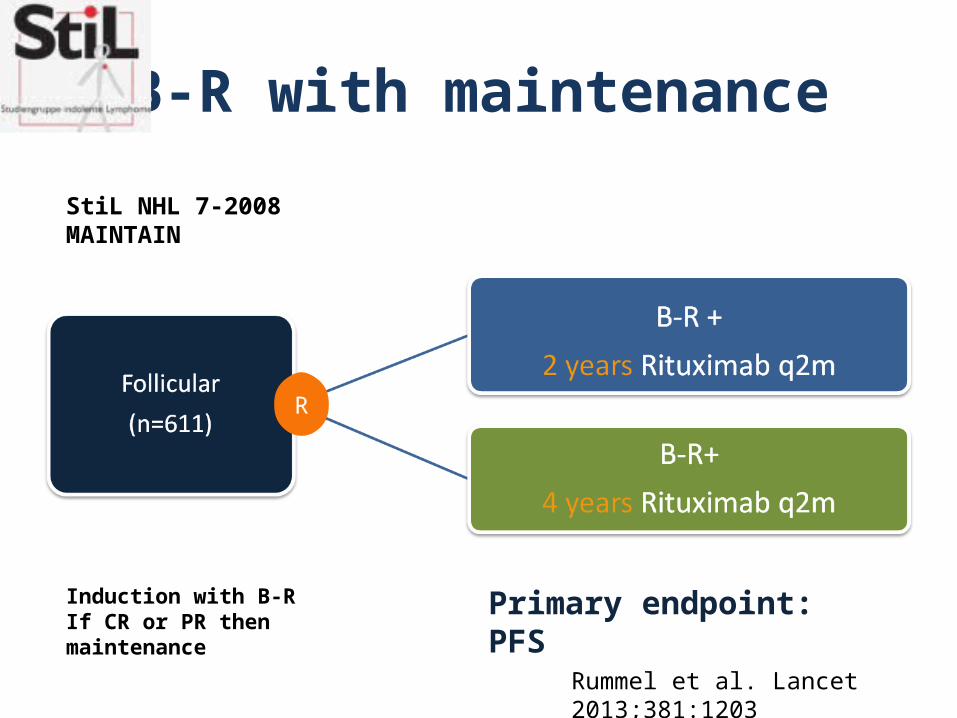
B-R with maintenance
StiL NHL 7-2008 MAINTAIN
R
Rummel et al. Lancet 2013;381:1203
Primary endpoint: PFSInduction with B-R If CR or PR then maintenance
Hodgkin’s lymphoma
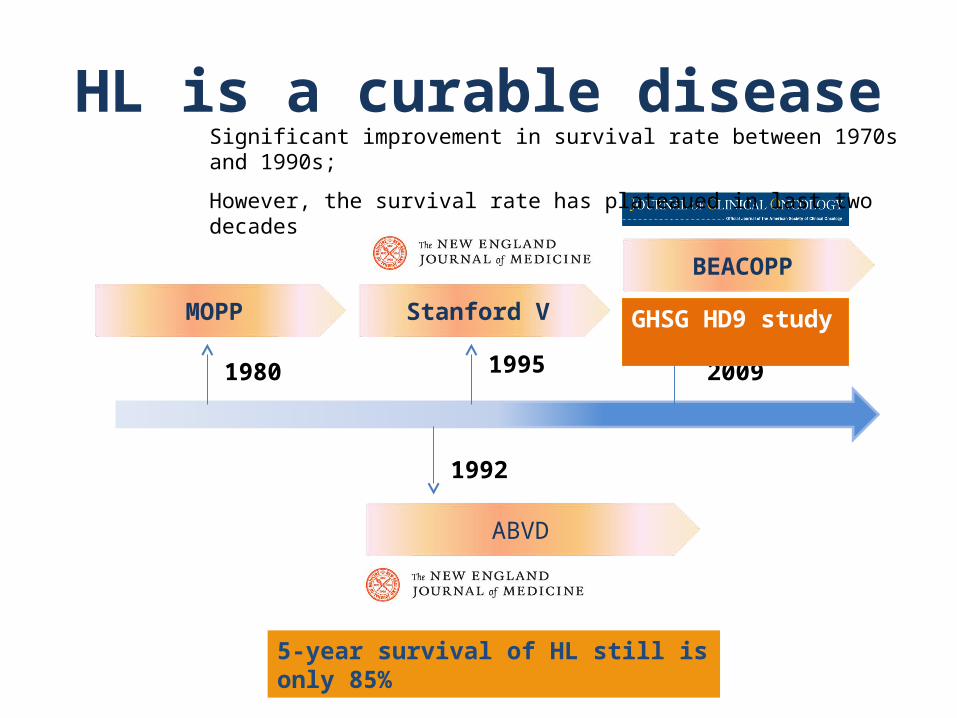
HL is a curable disease
1980 2009
GHSG HD9 study
1992
MOPP
BEACOPP
ABVD
Stanford V
1995
Significant improvement in survival rate between 1970s and 1990s;
However, the survival rate has plateaued in last two decades
5-year survival of HL still is only 85%
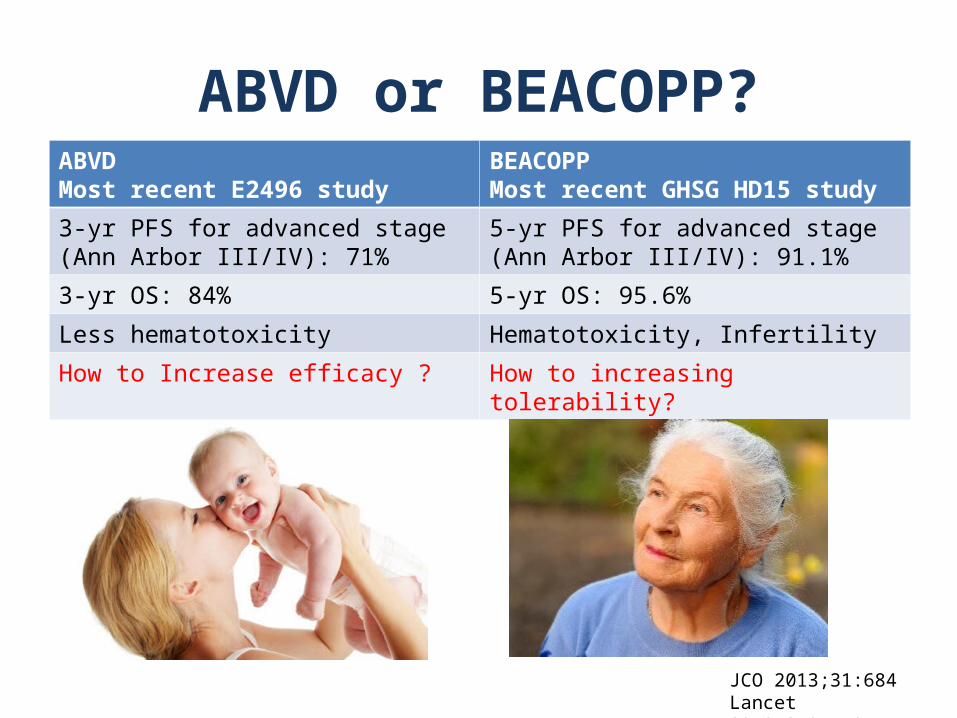
ABVD or BEACOPP?ABVDMost recent E2496 study
BEACOPPMost recent GHSG HD15 study
3-yr PFS for advanced stage (Ann Arbor III/IV): 71%
5-yr PFS for advanced stage (Ann Arbor III/IV): 91.1%
3-yr OS: 84% 5-yr OS: 95.6%
Less hematotoxicity Hematotoxicity, Infertility
How to Increase efficacy ? How to increasing tolerability?
JCO 2013;31:684Lancet 2012;379:1791
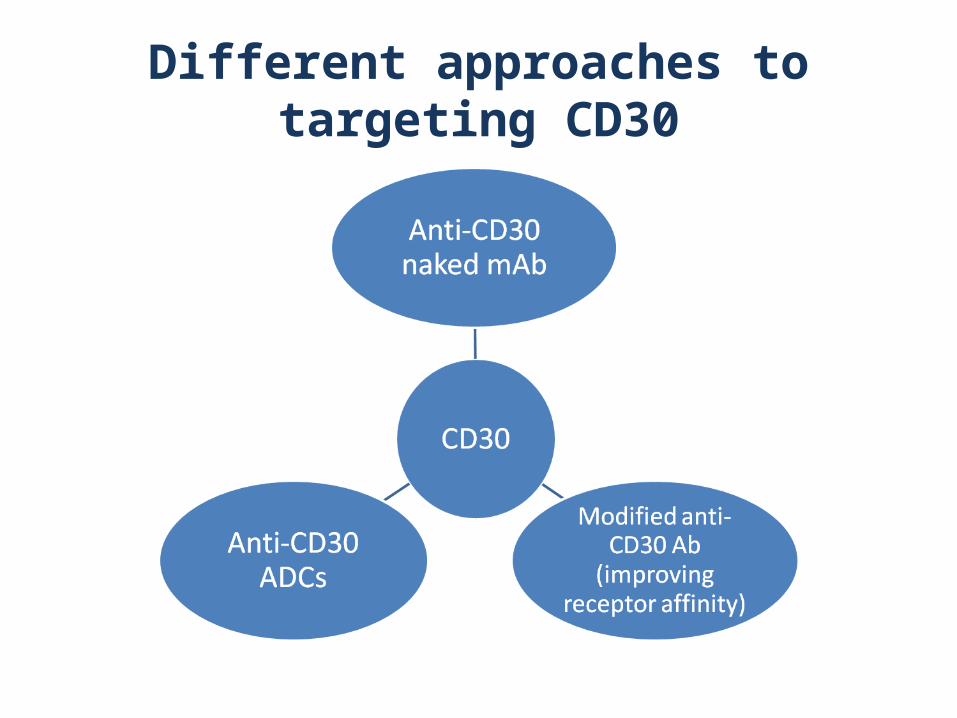
Different approaches to targeting CD30
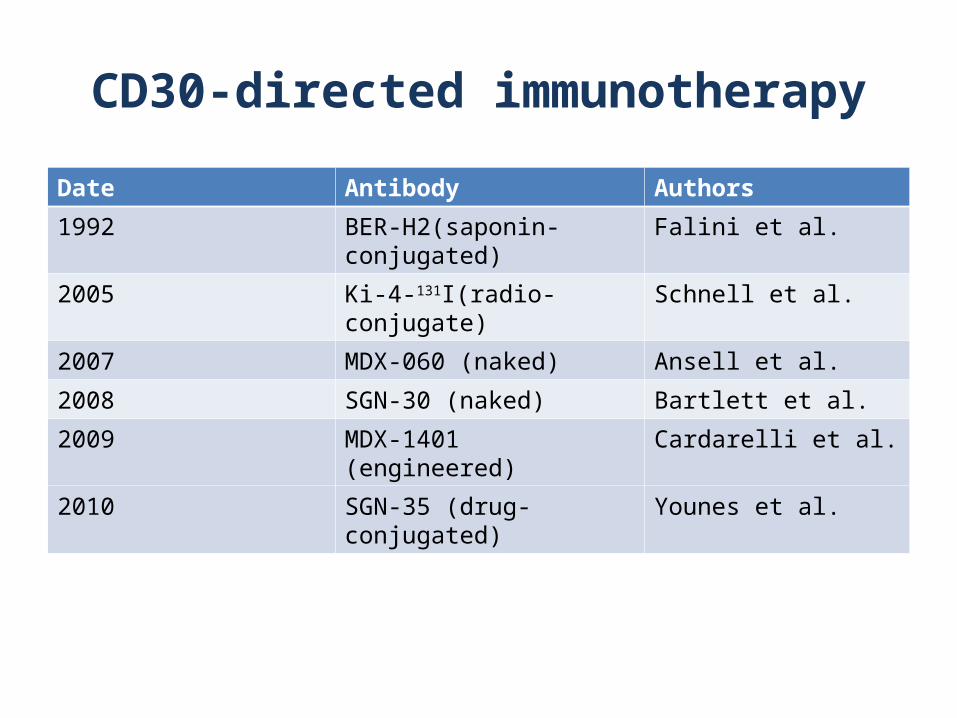
CD30-directed immunotherapy
Date Antibody Authors
1992 BER-H2(saponin-conjugated) Falini et al.
2005 Ki-4-131I(radio-conjugate) Schnell et al.
2007 MDX-060 (naked) Ansell et al.
2008 SGN-30 (naked) Bartlett et al.
2009 MDX-1401 (engineered) Cardarelli et al.
2010 SGN-35 (drug-conjugated) Younes et al.
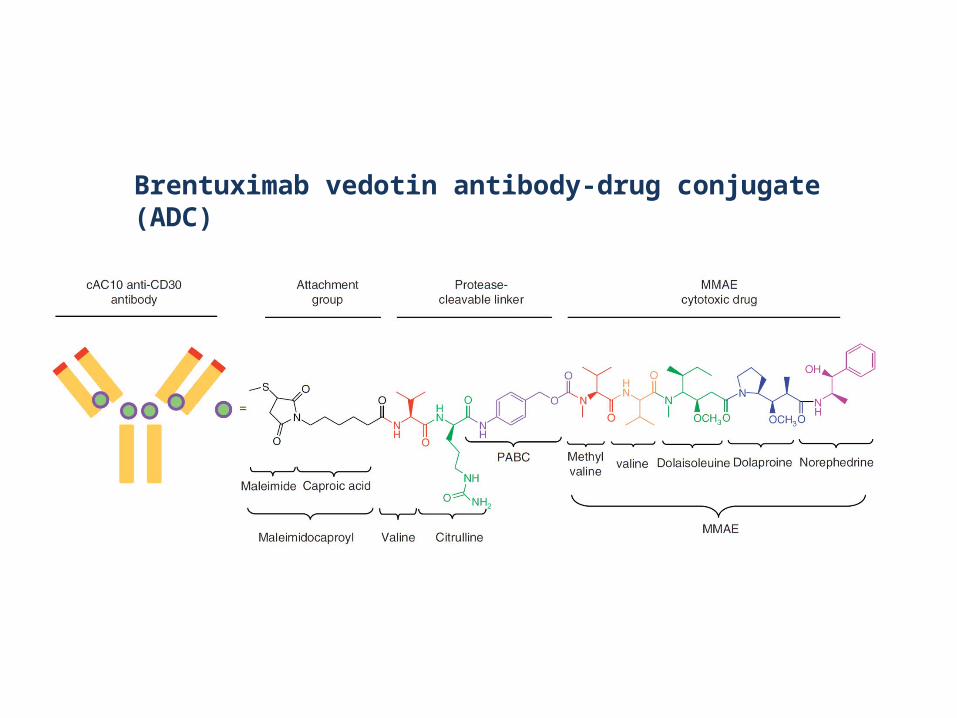
Brentuximab vedotin antibody-drug conjugate (ADC)
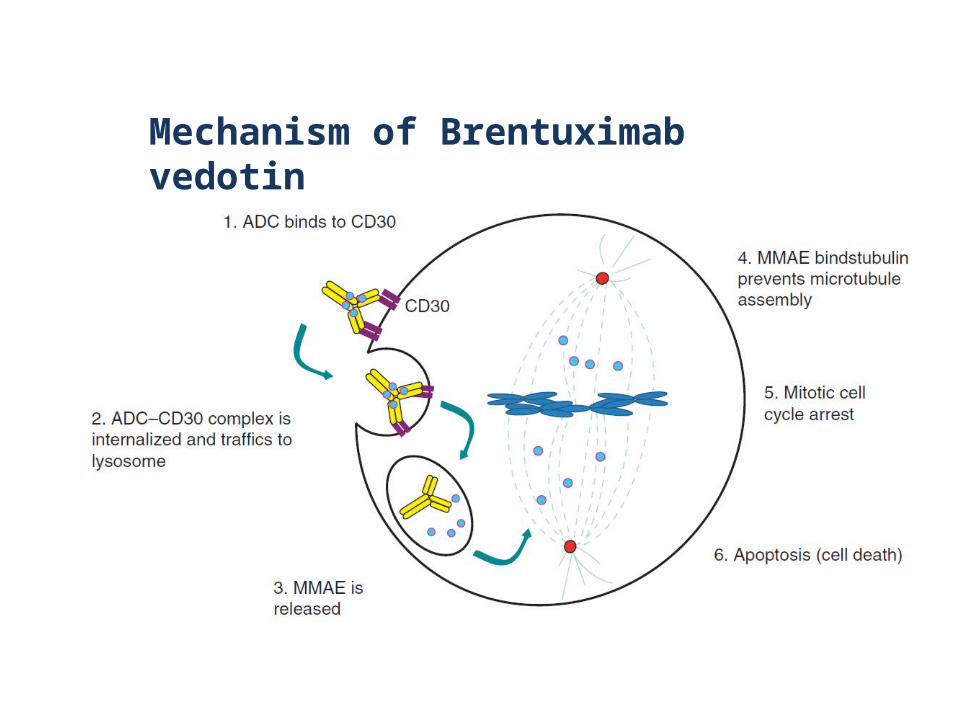
Mechanism of Brentuximab vedotin
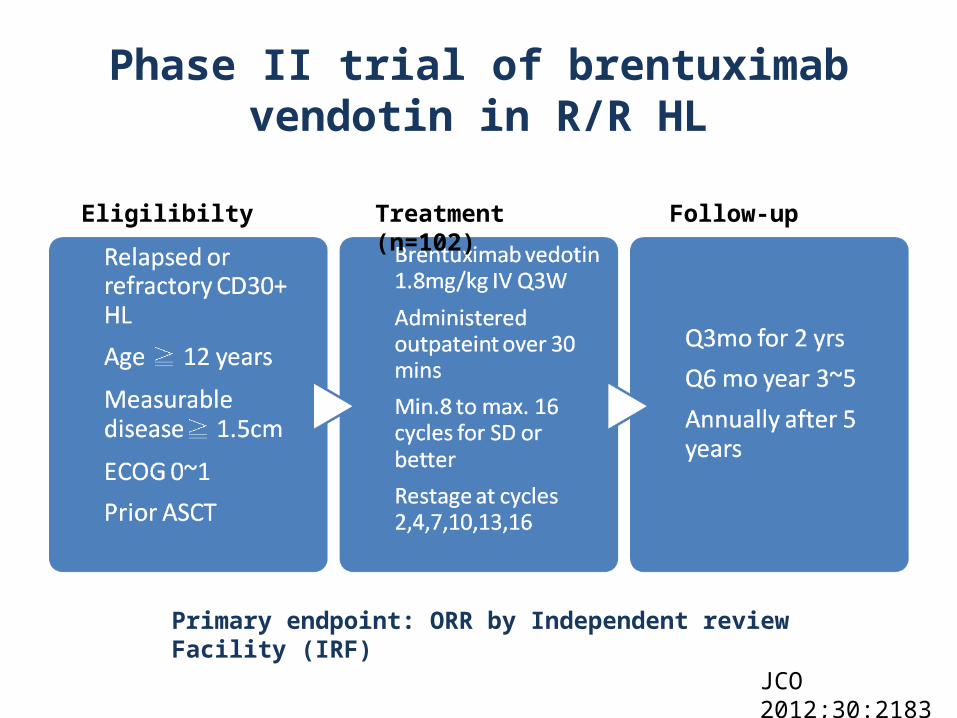
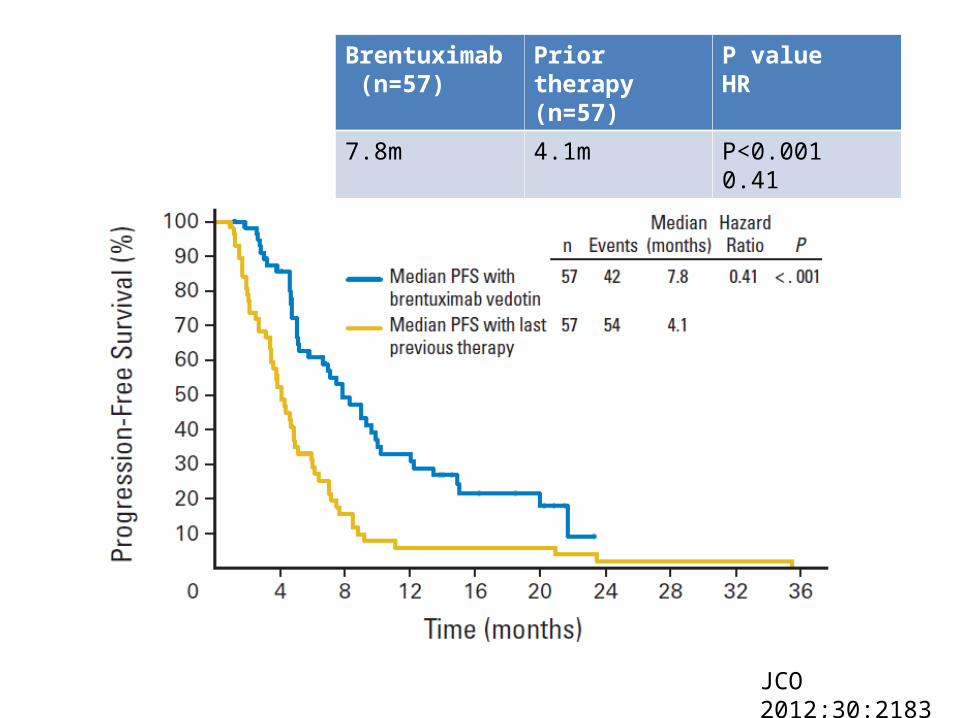
Phase II trial of brentuximab vendotin in R/R HL
Eligilibilty Treatment (n=102) Follow-up
Primary endpoint: ORR by Independent review Facility (IRF)
JCO 2012;30:2183
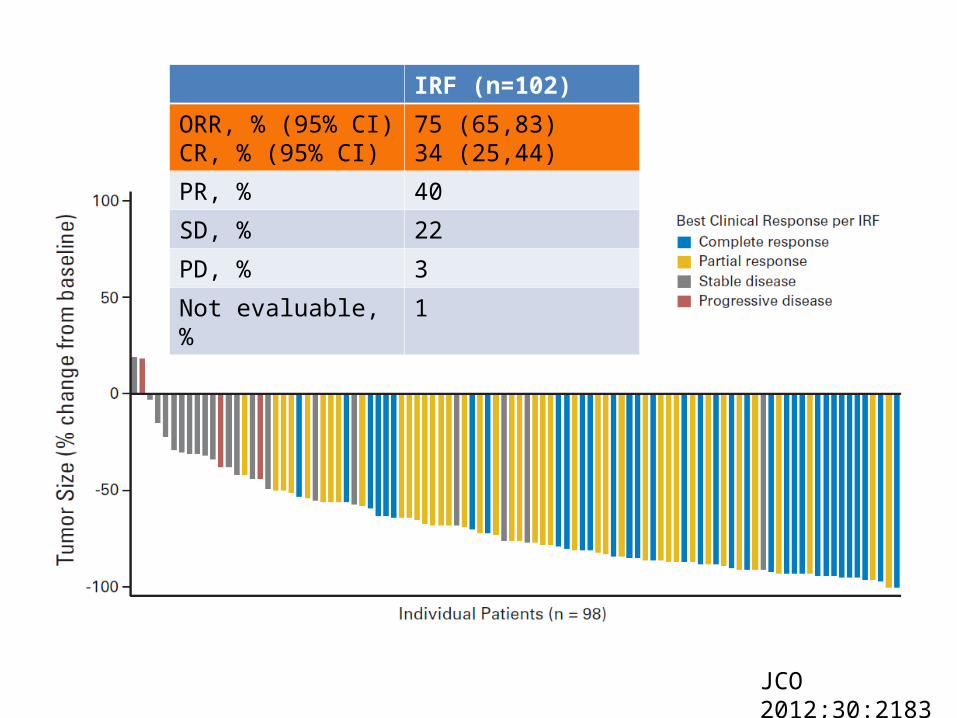
JCO 2012;30:2183
IRF (n=102)
ORR, % (95% CI)CR, % (95% CI)
75 (65,83)34 (25,44)
PR, % 40
SD, % 22
PD, % 3
Not evaluable, % 1
JCO 2012;30:2183
Brentuximab (n=57)
Prior therapy(n=57)
P valueHR
7.8m 4.1m P<0.0010.41
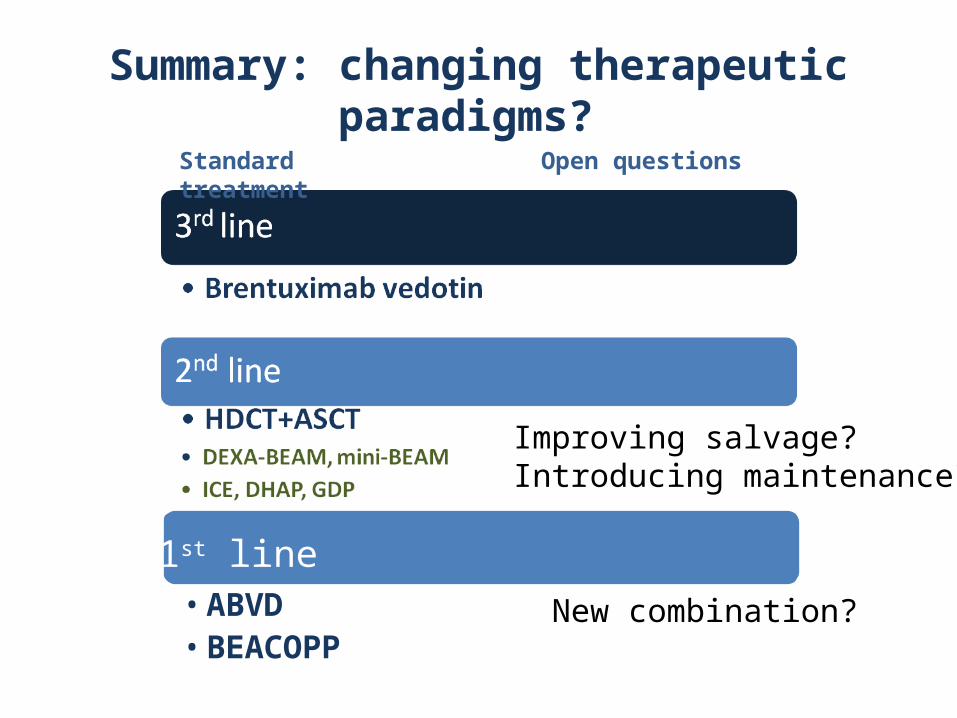
Summary: changing therapeutic paradigms?
1st line
Standard treatment Open questions
• ABVD• BEACOPP
Improving salvage?Introducing maintenance?
New combination?
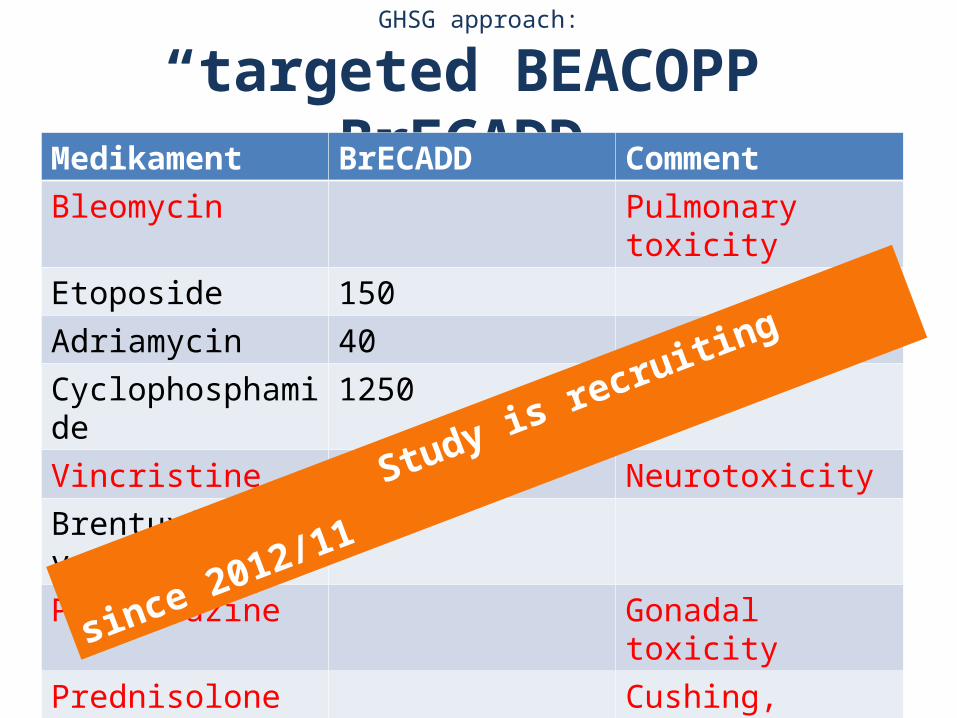
GHSG approach:
“targeted BEACOPP” BrECADD Medikament BrECADD Comment Bleomycin Pulmonary toxicityEtoposide 150Adriamycin 40Cyclophosphamide 1250Vincristine NeurotoxicityBrentuximab vedotin
1.8
Procarbazine Gonadal toxicityPrednisolone Cushing, infectionDacarbazine 2×250Dexamethasone 4×40
Study is recruiting since 2012/11
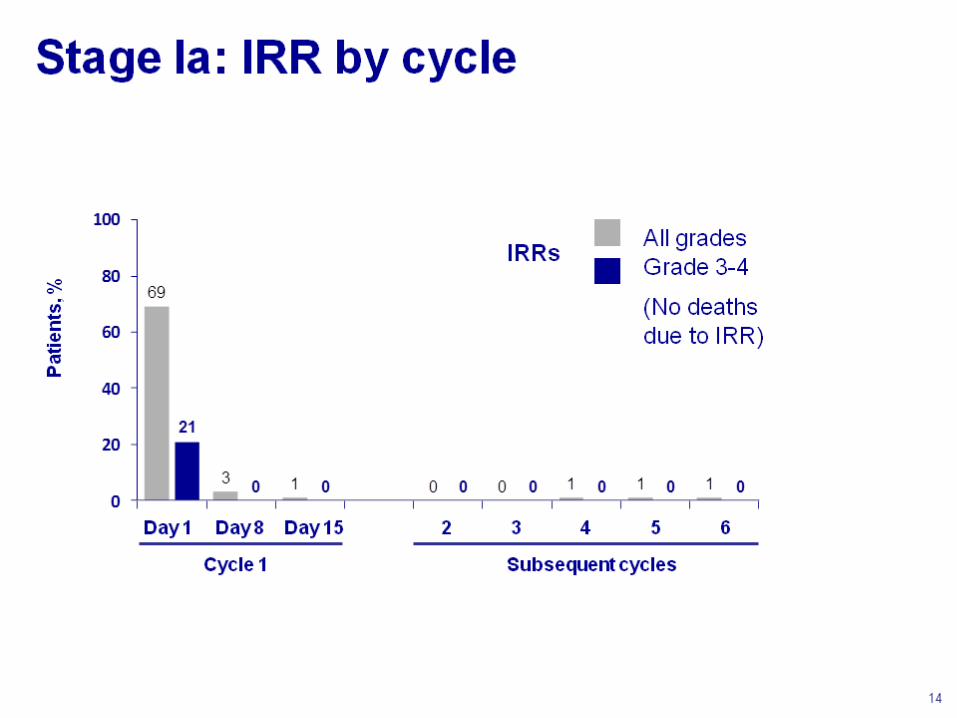
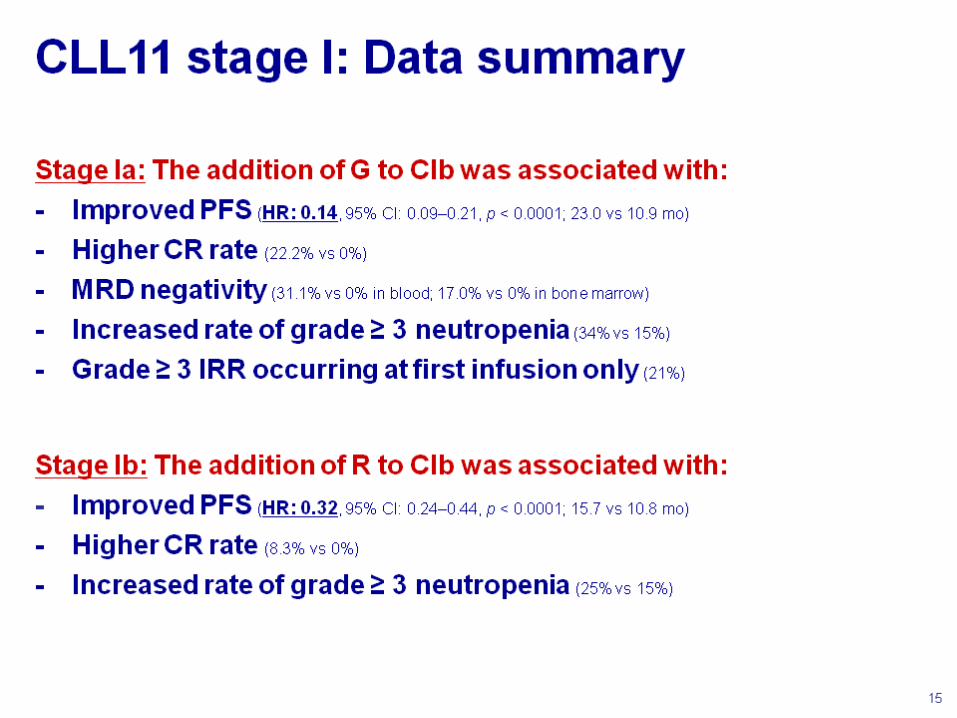
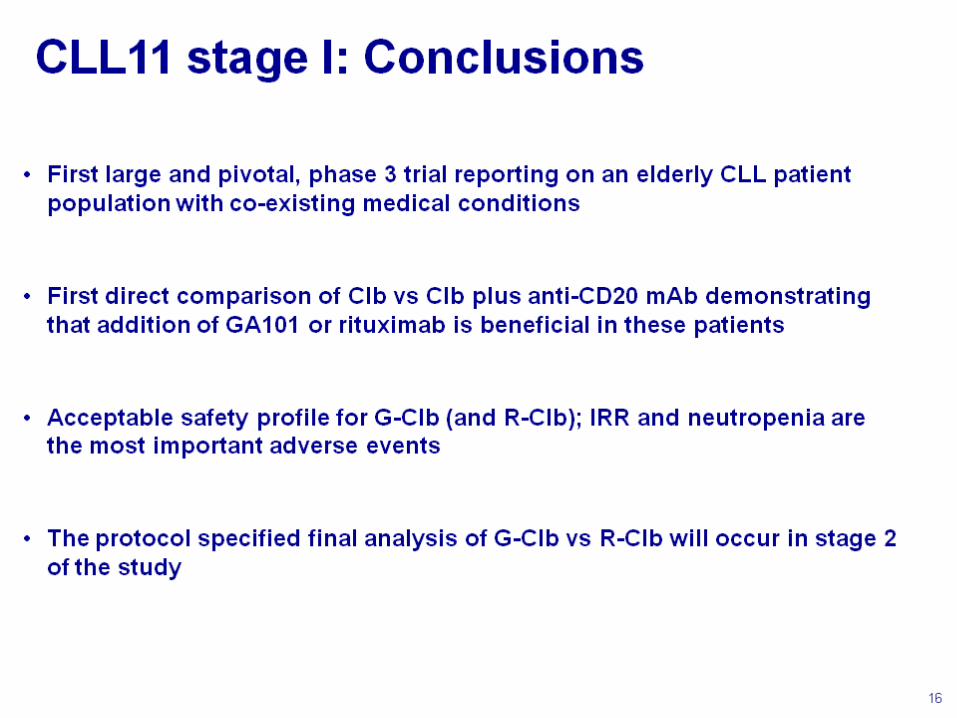
Chronic lymphocytic leukemia
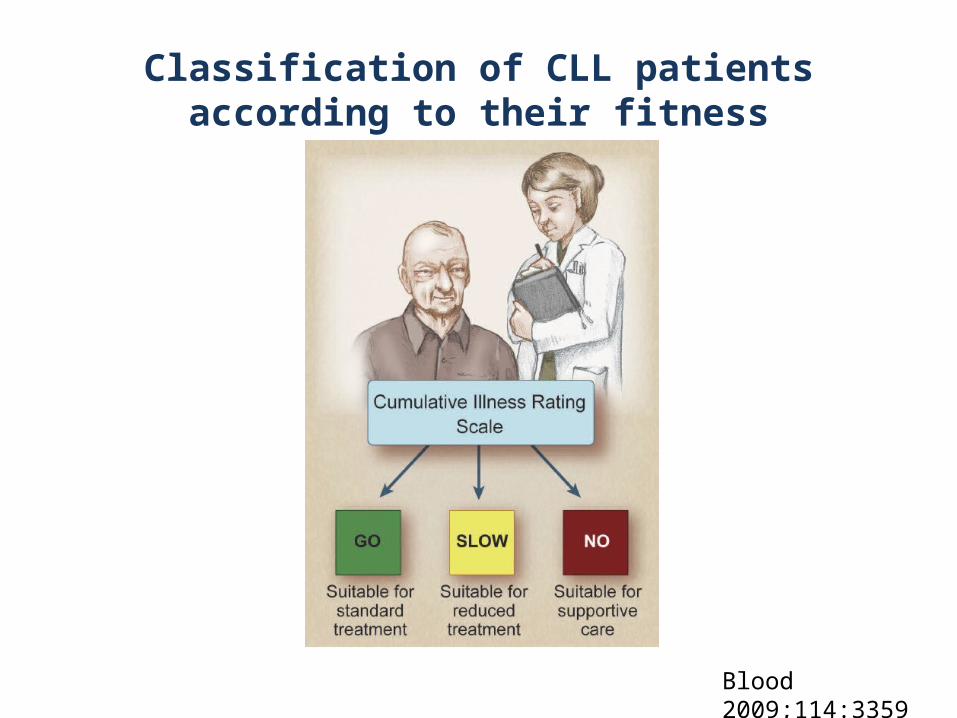
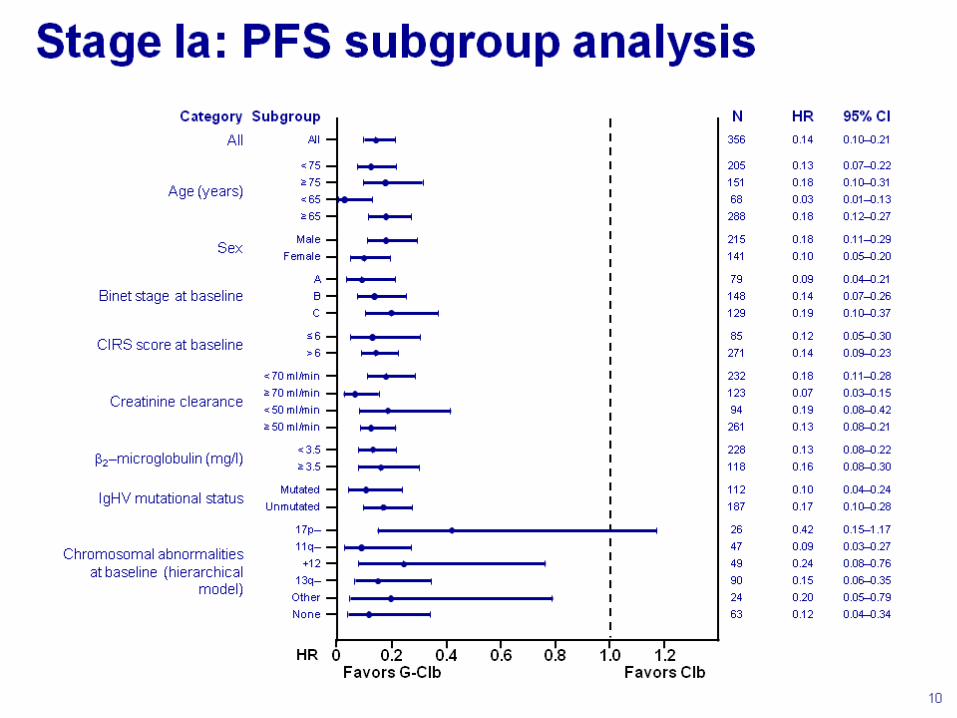
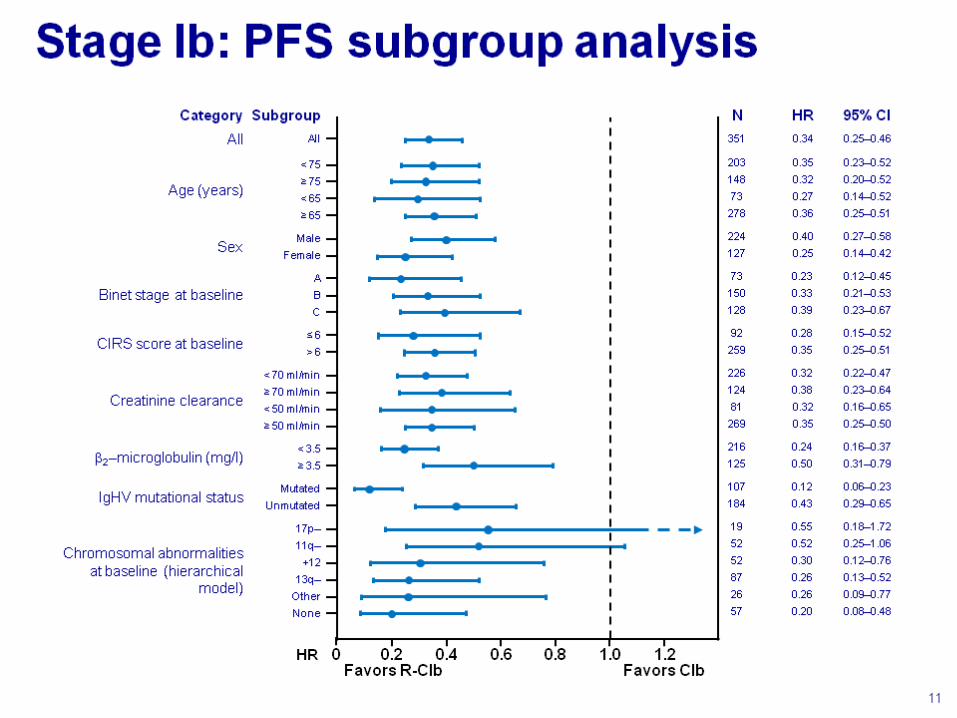
Classification of CLL patients according to their fitness
Blood 2009;114:3359
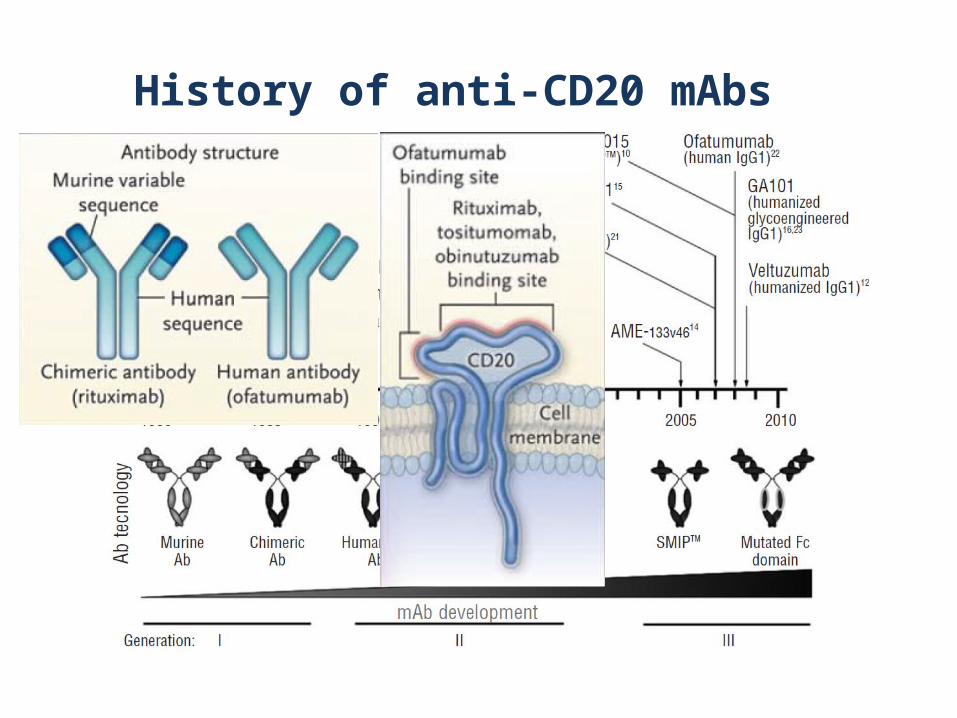
History of anti-CD20 mAbs
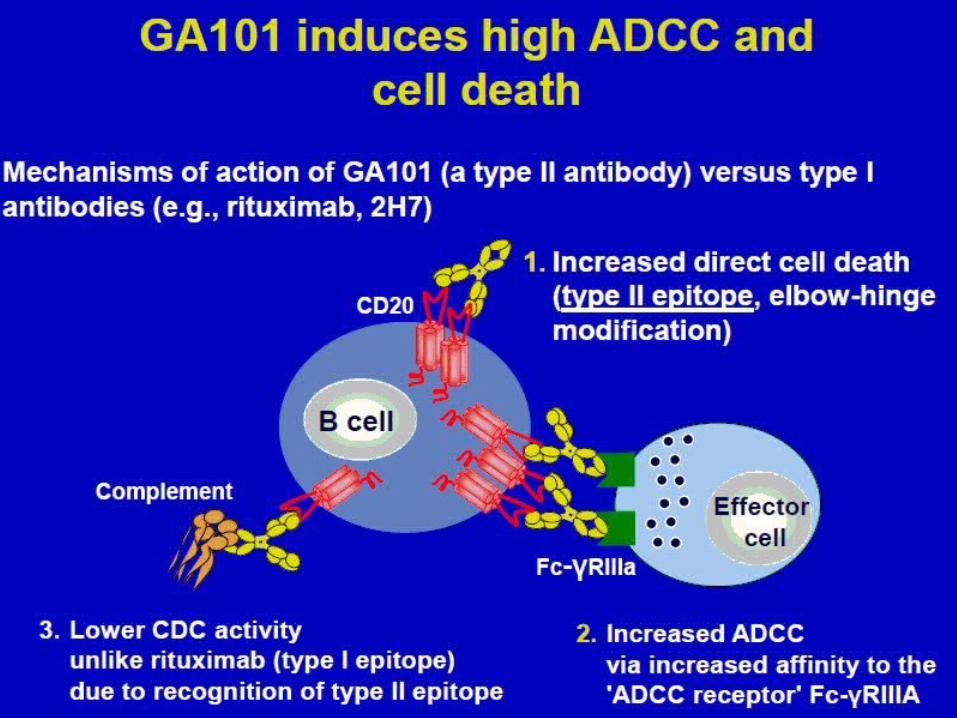
GA 101: type II, glycoenginered anti-CD20 mAb
• First type II, glycoengineered , humanized IgG1 anti-CD 20 mAb
• In preclinical studies comparing against rituximab, GA 101 provided:
Enhanced ADCC, oligosaccharides that enhance the interaction with FcγR, particularly FcγRIIIa, even in effector cells bearing the low affinity polymorphic variant of FcγRIIIa
Increased direct cell death induction
Decreased complement-dependent cytotoxicity
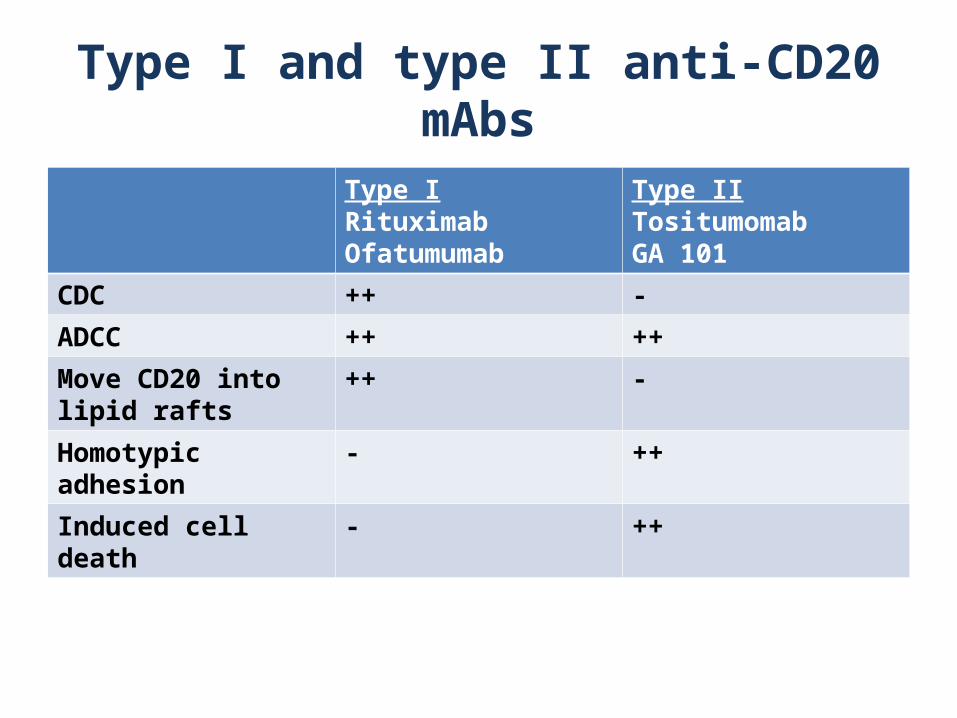
Type I and type II anti-CD20 mAbs
Type IRituximabOfatumumab
Type IITositumomabGA 101
CDC ++ -
ADCC ++ ++
Move CD20 into lipid rafts
++ -
Homotypic adhesion - ++
Induced cell death - ++
Summary of direct cell death with type II mAbs (GA 101)
• Most anti-CD20 mAbs in development are type I. Non of type I mAbs had proven to be superior to rituximab.
• The type II anti-CD20 mAb GA101 exhibit increased PCD, enhanced ADCC and lower CDC compared with type I mAbs
• GA 101 induced PCD via non-apoptotic pathways involving lysosomes nad ROS
• Loss of cell surface CD20 by ”shaving” involving phagocytosis and modulation on tumor surface may affect anti-CD20 efficacy of mAbs.

Thanks for your attention
comments and questions