Embed Size (px)
Citation preview

2014 SNMMI Highlights Lecture: Cardiovascular Imaging
From the Newsline Editor: The Highlights Lecture, presented at
the closing session of each SNMMI Annual Meeting, was origi-
nated and presented for more than 33 years by Henry N. Wagner,
Jr., MD. Beginning in 2010, the duties of summarizing selected
significant presentations at the meeting were divided annually
among 4 distinguished nuclear and molecular medicine subject
matter experts. The 2014 Highlights Lectures were delivered on
June 11 at the SNMMI Annual Meeting in St. Louis, MO. The
neuroscience presentation was included in the September Newsline
issue; others will appear in later issues. In this issue we feature the
lecture by Vasken Dilsizian, MD, who spoke on highlights in
cardiovascular imaging. Note that in the following presentation
summary, numerals in brackets represent abstract numbers as
published in The Journal of Nuclear Medicine (2014;55[suppl 1]).
It is an honor and privilege to summarize the highlights ofthe cardiovascular presentations at the 61st Annual Meet-ing of the SNMMI. This is a truly international meeting,
with abstracts coming from across the globe. North Amer-ican presenters led in the number of presentations, followedby colleagues from Asia and Europe. The 3 leading Europeancountries represented were Germany, The Netherlands, andFrance. Asian countries were led by presenters from Japan.One trend that we noted in the Cardiovascular Council wasthat the number of clinical presentations was almost 3 timeshigher than that of basic science presentations. We alsonoted a trend toward a transition from foci on myocardialperfusion imaging to other areas of molecular imaging. PETinstrumentation continues to grow as a focus in abstractsubmissions, despite the fact that we still have many moreSPECT than PET cameras (;12,000 and 2,000, respectively)in the clinical setting in the United States. This interest inPET and associated hybrid modalities most likely reflectsthe direction of future research in cardiovascular imaging.
PET and Myocardial Perfusion
One such area of increased interest in cardiac PET is myo-cardial perfusion. Two PET agents, 82Rb and 13N-ammonia,are now U.S. Food and Drug Administration (FDA) andCenters for Medicare & Medicaid approved for cardiacimaging. The advantages of PET over SPECT in this settinginclude higher sensitivity and spatial resolution, reducedartifacts as a result of high photon energy, robust andwell-validated attenuation correction, and, of course, theability to quantify absolute myocardial blood flow (MBF)and coronary flow reserve (CFR). Renaud et al. from theNational Cardiac PET Centre at the University of OttawaHeart Institute (ON, Canada) reported on “Rubidium-82PET versus thallium-201 SPECT for detection of coronaryartery disease in the Alternative Radiopharmaceutical forMyocardial Imaging (ARMI) trial” [241]. These research-ers showed that when using an automatic scoring programwith comparisons to a normal database, 82Rb PET sensitiv-ity and specificity were 83% and 94%, respectively, for
individuals with $50% stenosis and90% and 93%, respectively, for$70% stenosis. Corresponding 201TlSPECT values were lower, with sen-sitivity and specificity of 56% and85%, respectively, for individualswith $50% stenosis and 57% and83%, respectively, for$70% stenosis.
Another area that has been ad-dressed with frequency in the recentliterature is that of the added prog-nostic value of absolute MBF andCFR as assessed with either 82Rb or 13N-ammonia PET. In2011, Ziadi et al., also from the group at the University ofOttawa Heart Institute, documented the added value of tra-ditional summed stress scores when patients were furtherstratified according to CFR (J Am Coll Cardiol. 2011;58:740–708).
It is my pleasure to announce that the winner of theCardiovascular Council Clinical Young Investigator Awardis Nishant Shah, MD, who, with colleagues from theBrigham and Women’s Hospital (Boston, MA), reportedon “Prognostic value of PET-derived CFR for survival inpatients with dialysis-dependent end-stage renal disease(ESRD)” [26]. In this study, 196 patients with dialysis-dependent ESRD underwent 82Rb or 13N-ammonia rest/stress myocardial perfusion PET for evaluation of knownor suspected coronary artery disease (CAD). On the basis ofresulting CFR values, patients were classified as abnormal,normal, or intermediate. Data analysis at 3 years showed thatCFR as a continuous variable was independently associatedwith survival. Those with preserved flow reserve had muchhigher survival rates than those with abnormal flow reserve.
Danad et al. from the VU University Medical Center,(Amsterdam, The Netherlands), Turku University Hospital(Finland), and Uppsala University (Sweden) reported on“Quantitative cardiac PET imaging for diagnoses of hemo-dynamic significant epicardial disease” [24]. These inves-tigators posed a key question: Do we really need to have bothstress and rest images, or can we simply look at absoluteblood flow in the hyperemic state with PET, similar to the con-cept of stress-only imaging with SPECT? Can this approachbe sufficient for detecting flow-limiting CAD? This was awell-conducted study in which optimal cutoff values of 15O-water PET–determined hyperemic MBF and CFR were assessedin a large clinical cohort of 330 patients (990 vascular terri-tories) as a means of detecting flow-limiting coronary arterystenosis, using fractional flow reserve (FFR) as a compara-tive gold standard. The researchers showed that hyperemicMBF on PETwas more accurate than CFR in detecting flow-limiting stenosis, in both per-patient and per-vessel analyses.More important, among all patients with FFR-defined function-ally limiting stenosis, only 13% were missed by quantitative
Vasken Dilsizian, MD
Newsline 9N
NEW
SLIN
Eby on June 8, 2018. For personal use only. jnm.snmjournals.org Downloaded from
hyperemic MBF assessment with PET. 15O-water PET hy-peremic MBF .2.3 mL/g/min was found to exclude thepresence of flow-limiting stenosis with a high negative pre-dictive value (90% per patient and 95% per vessel).
Although the identification of these and similar PET-derived cutoff values is encouraging, uncertainty remains asto how these thresholds for hyperemic flow assessed with non-FDA approved 15O-water compare to other FDA-approvedflow tracers, such as 13N-ammonia and 82Rb, for evaluationof diagnostic accuracy in CAD detection. It is important toduplicate these findings with FDA-approved tracers.
Molecular Imaging: Beyond Perfusion
Many new and exciting areas of cardiac molecular imagingbeyond perfusion were addressed at this meeting, includingbut not limited to vascular imaging, myocardial innervation,cardiac sarcoidosis, angiogenesis, atherosclerotic plaque im-aging, and thrombus imaging. Very high quality presenta-tions were made in each of these categories. Although thelimitations of the lecture format preclude citation of each ofthese meritorious presentations, a select few will serve asexamples of new directions in research and clinical practice.
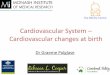
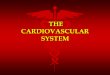
One such example also allows me to announce the winnerof the Cardiovascular Council Basic Young Investigator Award:Reza Golestani, MD, PhD. Golestani, from Yale University(New Haven, CT), with colleagues from Yale and LantheusMedical Imaging (North Billerica, CT), reported on “Matrixmetalloproteinase (MMP) imaging to predict aortic aneurysmrupture” [25]. These researchers created an angiotensin 2–induced abdominal aortic aneurysm (AAA) model in miceand explored the utility of MMP imaging in predicting AAAand rupture (Fig. 1).
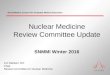
Angiogenesis can also serve as a target for vascular im-aging. Shi et al. from the University of Wisconsin (Madison)reported on “PETof AAAwith a 64Cu-labeled Fab fragment”[465]. In a murine model of AAA, 64Cu-NOTA-TRC105-Fabwas shown to clear rapidly from the blood with very lowintestinal uptake, making it a suitable tracer for identifyingangiogenesis in the aortic wall (Fig. 2). The researchersalso performed a blocking study to verify that these findingswere specific.
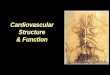
PET/MR imaging in large-vessel vasculitis is becom-ing much more clinically relevant. Einspieler et al. fromthe Technische Universitat Munchen (Germany) and theRheinische Friedrich-Wilhelms-Universitat (Bonn, Germany)reported on “Imaging large-vessel vasculitis with fully in-tegrated PET/MR: a pilot study” [185]. The research in-cluded 12 patients with histories of large-vessel vasculitis(2 Takayasu arteritis, 10 giant cell arteritis) who underwentPET/MR imaging after injection of 18F-FDG (Figs. 3 and4). Subsequent analyses demonstrated a much stronger andmore significant correlation between C-reactive proteinand the number of vessel segments affected by inflamma-tion as seen on hybrid PET/MR than seen on either PET orcontrast-enhanced MR angiography alone. Quantitativeevaluation revealed significantly higher standardized uptake
values (SUVs) in patients with vasculitis than in a matchedreference group.
Another area of research excitement and clinical rel-evance is that of cardiac innervation. Heart failure is charac-terized by increased sympathetic drive to the myocardium.Metaiodobenzylguanidine (MIBG) and hydroxyephedrine
FIGURE 1. Matrix metalloproteinase (MMP) imaging to predictaortic aneurysm rupture in a mouse model. Uptake of the noveltracer in the suprarenal aorta at 1 week was significantly higherin animals with aortic aneurysm atherosclerosis (AAA)/rupturethan in those without AAA. In mice with AAA, tracer uptake at 4weeks was correlated with MMP CD68 expression. No corre-lation was found between uptake and AAA size.
FIGURE 2. Angiogenesis as a target for vascular imaging.A: Aortic aneurysm (top) in a mouse model of atherosclerosisand corresponding normal aorta (bottom) in a sham-surgicalprocedure control animal. B: PET images acquired in a mousewith aortic aneurysm atherosclerosis (AAA) (top), in a blockingstudy performed to verify the specificity of imaging findings(middle), and in a sham-surgical procedure control animal(bottom).
10N THE JOURNAL OF NUCLEAR MEDICINE • Vol. 55 • No. 10 • October 2014
NEW
SLIN
Eby on June 8, 2018. For personal use only. jnm.snmjournals.org Downloaded from

(HED) are analogs of norepinephrine that can visualizemyocardial sympathetic innervation. In certain heart failurepatients, MIBG can help identify those with lower 1- and2-year mortality risks as indicated by a heart/mediastinal ratio$1.6. We are pleased that the FDA recently approved123I-MIBG to assess cardiac sympathetic innervation. Thepredominant focus of cardiac assessment has been on function,perfusion, and metabolism. Wewelcome the fact that the abilityto assess cardiac innervation is now in our armamentarium.
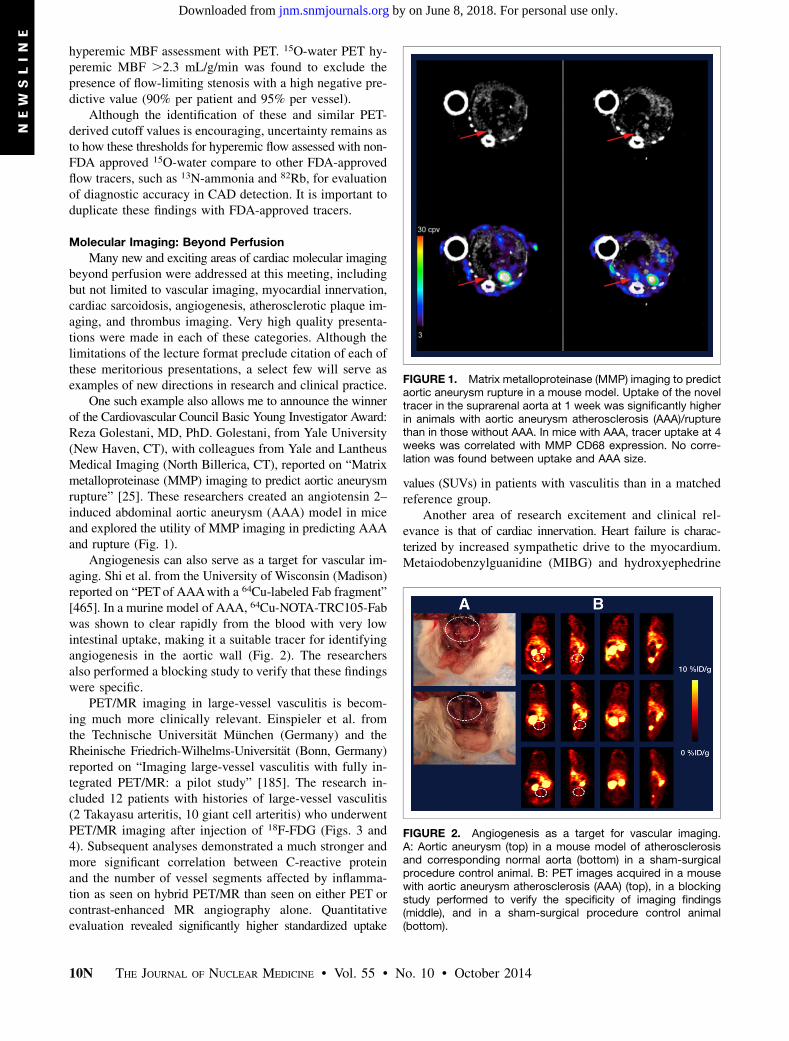
One of the challenging issues noted with 123I-MIBG im-aging is that of attenuation artifact, predominantly in theinferior region when patients are imaged in the supine po-sition. Tomiyama et al. from Hokkaido University (Sapporo,Japan) reported that “Prone position acquisition is more effec-tive than changing reconstruction method for regional myo-cardial 123I-MIBG SPECT uptake” [132]. These researchersfound that when patients were imaged in the prone position,attenuation artifact seen in the inferior region disappeared
(Fig. 5). This was confirmed with anelegant study using 11C-HED PETtechnology.
Fujita et al. from the Medical andPharmacological Research Center (Hakui,Japan) and Kanazawa Medical Uni-versity (Uchinada, Japan) reported on“Prediction of all-cause death using11C-HED PET in patients with leftventricular (LV) dysfunction” [183].This study included 51 patients withLV dysfunction (36 ischemic, 15 non-ischemic) who underwent 11C-HED PETimaging. Global LV myocardial reten-tion was calculated as a measure ofcardiac sympathetic neuronal integrity.Using a retention threshold of 9, theauthors showed that, similar to resultsseen with MIBG, patients with preserved
sympathetic innervation had lower mortality risk and thosewith LV dysfunction and retention ,9 had adverse prognosesover a 6-month follow-up period.
Another very important aspect of cardiac innervation re-search goes beyond simple diagnosis of myocardial denerva-tion and prognosis in heart failure to image-guided therapyof cardiac arrhythmias. I believe that a key component ofthe future of our field will be therapeutics and that whateverwe can do to contribute to advances in guiding and improvingtherapy will make our field even more important. Ben-Haimet al. from University College London Hospitals (UK),Royal Brompton Hospital (London, UK), and SpectrumDynamics (Caesarea, Israel) reported on “Localization ofganglionated plexi in patients with cardiac arrhythmia: Anew application for 123I-MIBG SPECT” [184]. These inves-tigators used 123I-MIBG SPECT guidance to detect andablate atrial fibrillation. At the University of MarylandMedical Center (Baltimore, MD), along with my colleagueTimm Dickfeld, MD, PhD, we first worked with this con-cept of image-guided therapeutics in the electrophysiologylaboratory nearly 10 years ago, using 18F-FDG PET, then 201TlSPECT, and, more recently, 123I-MIBG SPECT to identifyareas for ventricular tachycardia ablation (JACC CardiovascImaging. 2008;1:73–82; J Nucl Med. 2012;53:894–901).The study presented by Ben-Haim et al. is unique in focusingon atrial fibrillation. The study included 13 patients withcardiac arrhythmia (mean age, 60.3 years) who underwent123I-MIBG SPECTon a solid-state dedicated cardiac camera,with resulting images fused with CT or cardiac MR images.Focal 123I-MIBG uptake sites (higher than mediastinal ac-tivity) were documented in atrial fat pads. Figure 6 showsthe 123I-MIBG image superimposed on anatomic mapping.
Another area of clinical relevance that is continuingto grow is cardiac sarcoidosis. Last year a key article waspublished in Circulation, in which James A. White, MD,from the University of Western Ontario (London, Canada),and other Canadian researchers used hybrid PET/MR for
FIGURE 3. PET/MR imaging in large-vessel vasculitis. MR (top) and PET and fusedimages (bottom) acquired in a 58-year-old patient with giant cell arteritis showinflammation of the vessel wall in the descending thoracic aorta.
FIGURE 4. PET/MR imaging in large-vessel vasculitis. MR/MR angiography (left), PET (right), and fused images (middle)acquired in a 34-year-old patient with Takayasu arteritis. PETimaging shows pathologic 18F-FDG uptake in the ascendingaorta. MR/MR angiography shows severe stenosis of the leftsubclavian artery and both renal arteries.
Newsline 11N
NEW
SLIN
Eby on June 8, 2018. For personal use only. jnm.snmjournals.org Downloaded from
diagnosing active cardiac sarcoidosis (Circulation 2013;127:e639–e641). I really like this approach—perhaps the first clin-ical application of PET/MR in cardiology. 18F-FDG PET incardiac sarcoidosis produces “hot spot” images. MR is par-ticularly helpful for anatomic co-localization of the 18F-FDGPET signal within the heart, reflecting the inflammatory phaseof cardiac sarcoidosis. MR delayed enhancement, on theother hand, provides information on areas of fibrosis andscar as a consequence of cardiac sarcoidosis. It is reasonable,therefore, to have a hybrid system in which MR can showthe focus of prior injury or scar from sarcoidosis superim-posed on inflammatory markers seen with 18F-FDG. This
complete view can then be used to guide therapy (e.g., withcorticosteroids) and treat the inflammatory phase of cardiacsarcoidosis before scar tissue is formed.
Investigators at this meeting presented papers that ad-dressed this topic further. Manabe et al. from HokkaidoUniversity Graduate School of Medicine and Hokkaido Uni-versity Hospital (Sapporo, Japan) reported on “The effectsof the 18 hours fasting preparation on plasma free fatty acidand physiological myocardial 18F-FDG uptake in patients ofsuspected cardiac involvement sarcoidosis” [295]. We havebeen seeing a number of sarcoidosis patients in our institu-tion, and it is not uncommon to have images that are poor be-cause of inadequate dietary preparation. These researchersproposed prolonging the fasting preparation over 18 hours,compared with the usual 6–8 hours, with the aim of affect-ing plasma free fatty acid levels and improving image qual-ity. Figure 7 shows that myocardial uptake of 18F-FDG withthe shorter fasting time is “insufficient” for sarcoidosis as-sessment, whereas uptake in the myocardium is suppressedwith prolonged fasting, so that any signal can be confidentlyattributed to cardiac sarcoidosis.
The group working with Abass Alavi, MD, at the Uni-versity of Pennsylvania (Philadelphia) extended the conceptof simply identifying inflammatory markers in sarcoidosisto the use of 18F-FDG PET to assess treatment response.Salavati et al. reported on “Assessment of diagnostic per-formance of volumetric PET/CT parameters in treatment
FIGURE 5. Prone position acquisition in 123I-MIBG SPECT.123I-MIBG images acquired in the supine position with filteredbackprojection (FBP) (top) and ordered subset expectationmaximization (second from top) showed more attenuationartifact than 123I-MIBG images acquired with FBP in the proneposition (third from top). The authors validated the findings with11C-HED PET (bottom).
FIGURE 6. 123I-MIBG SPECT/CT superimposed on electro-anatomical mapping to guide and confirm successful atrial fibril-lation ablation. (A) Arrows point to ganglionated plexi (GP) localizedin a patient with cardiac arrhythmia. (B) Positive high-frequencystimulation (HFS) signal (pink dots) confirms epicardial GP locationsbefore ablation. (C) Negative HFS signal (blue dots) at ablated GPsites confirms successful ablation. ARGP 5 anterior right GP;SLGP5 superior left GP; ILGP5 inferior left GP; IRGP 5 inferiorright GP.
12N THE JOURNAL OF NUCLEAR MEDICINE • Vol. 55 • No. 10 • October 2014
NEW
SLIN
Eby on June 8, 2018. For personal use only. jnm.snmjournals.org Downloaded from
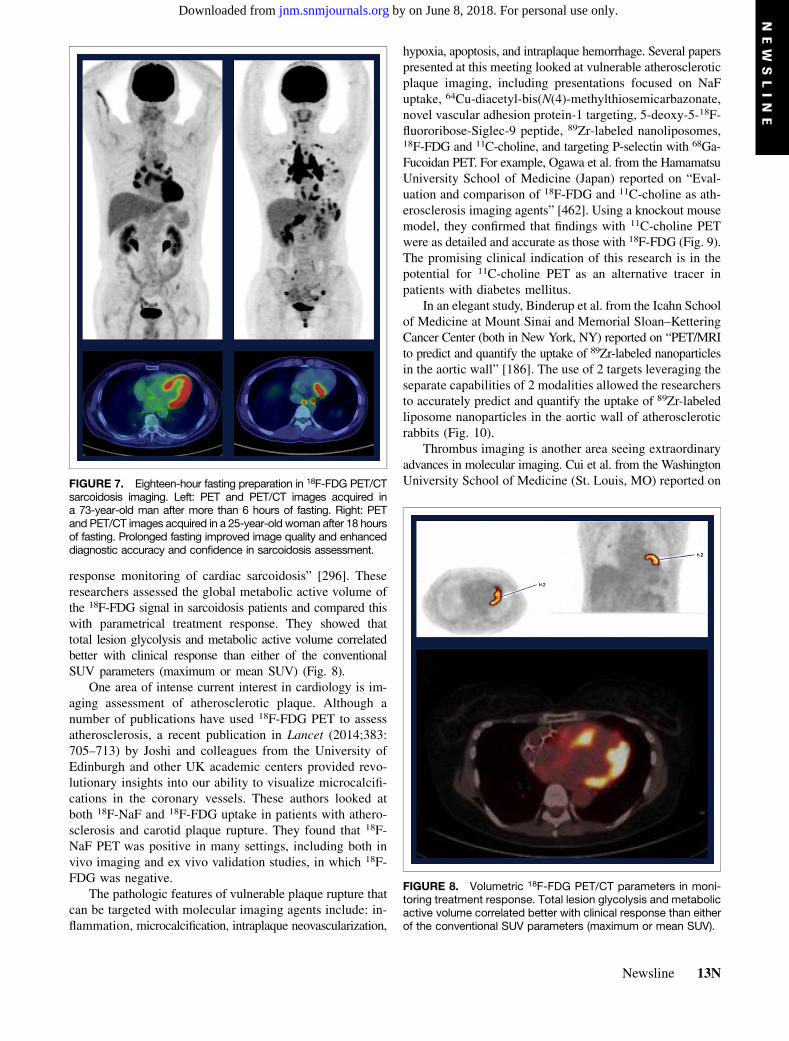
response monitoring of cardiac sarcoidosis” [296]. Theseresearchers assessed the global metabolic active volume ofthe 18F-FDG signal in sarcoidosis patients and compared thiswith parametrical treatment response. They showed thattotal lesion glycolysis and metabolic active volume correlatedbetter with clinical response than either of the conventionalSUV parameters (maximum or mean SUV) (Fig. 8).
One area of intense current interest in cardiology is im-aging assessment of atherosclerotic plaque. Although anumber of publications have used 18F-FDG PET to assessatherosclerosis, a recent publication in Lancet (2014;383:705–713) by Joshi and colleagues from the University ofEdinburgh and other UK academic centers provided revo-lutionary insights into our ability to visualize microcalcifi-cations in the coronary vessels. These authors looked atboth 18F-NaF and 18F-FDG uptake in patients with athero-sclerosis and carotid plaque rupture. They found that 18F-NaF PET was positive in many settings, including both invivo imaging and ex vivo validation studies, in which 18F-FDG was negative.
The pathologic features of vulnerable plaque rupture thatcan be targeted with molecular imaging agents include: in-flammation, microcalcification, intraplaque neovascularization,
hypoxia, apoptosis, and intraplaque hemorrhage. Several paperspresented at this meeting looked at vulnerable atheroscleroticplaque imaging, including presentations focused on NaFuptake, 64Cu-diacetyl-bis(N(4)-methylthiosemicarbazonate,novel vascular adhesion protein-1 targeting, 5-deoxy-5-18F-fluororibose-Siglec-9 peptide, 89Zr-labeled nanoliposomes,18F-FDG and 11C-choline, and targeting P-selectin with 68Ga-Fucoidan PET. For example, Ogawa et al. from the HamamatsuUniversity School of Medicine (Japan) reported on “Eval-uation and comparison of 18F-FDG and 11C-choline as ath-erosclerosis imaging agents” [462]. Using a knockout mousemodel, they confirmed that findings with 11C-choline PETwere as detailed and accurate as those with 18F-FDG (Fig. 9).The promising clinical indication of this research is in thepotential for 11C-choline PET as an alternative tracer inpatients with diabetes mellitus.
In an elegant study, Binderup et al. from the Icahn Schoolof Medicine at Mount Sinai and Memorial Sloan–KetteringCancer Center (both in New York, NY) reported on “PET/MRIto predict and quantify the uptake of 89Zr-labeled nanoparticlesin the aortic wall” [186]. The use of 2 targets leveraging theseparate capabilities of 2 modalities allowed the researchersto accurately predict and quantify the uptake of 89Zr-labeledliposome nanoparticles in the aortic wall of atheroscleroticrabbits (Fig. 10).
Thrombus imaging is another area seeing extraordinaryadvances in molecular imaging. Cui et al. from the WashingtonUniversity School of Medicine (St. Louis, MO) reported onFIGURE 7. Eighteen-hour fasting preparation in 18F-FDG PET/CT
sarcoidosis imaging. Left: PET and PET/CT images acquired ina 73-year-old man after more than 6 hours of fasting. Right: PETand PET/CT images acquired in a 25-year-old woman after 18 hoursof fasting. Prolonged fasting improved image quality and enhanceddiagnostic accuracy and confidence in sarcoidosis assessment.
FIGURE 8. Volumetric 18F-FDG PET/CT parameters in moni-toring treatment response. Total lesion glycolysis and metabolicactive volume correlated better with clinical response than eitherof the conventional SUV parameters (maximum or mean SUV).
Newsline 13N
NEW
SLIN
Eby on June 8, 2018. For personal use only. jnm.snmjournals.org Downloaded from

“Diagnosis of ventricular assist device (LVAD) thrombosisusing a fibrin-specific 99mTc imaging agent” [405]. The re-searchers used this agent to detect, localize, and quantifyintra-LVAD thrombosis. The incidence of heart failure isincreasing, with insufficient numbers of donors to meet thedemand for heart transplantation for those with advanceddisease. Because of the shortage of donor hearts, the role ofLVAD has been expanding in the management of advancedheart failure, both as a bridge to transplantation and as adestination therapy. With the extensive use of LVAD in lieuof transplantation comes a risk of infection and thrombusformation. Figure 11, with images acquired in excised LVADs,shows the potential for identifying early thrombus formation,which could facilitate more timely and appropriate inter-ventions. My own research group at the University of Mary-land School of Medicine has a recent article demonstratingthe potential role of 18F-FDG PET/CT for making early andaccurate diagnosis of LVAD infection as well as evaluationof response to therapy (JACC Cardiovasc Imaging. 2014;7:839–842).
Conclusion
I would like to extend heartfelt congratulations to allinvestigators who both presented and attended this scientificforum for working together for a shared goal of caring forour patients and advancing medical science by teaching and
learning from one another. A special acknowledgment andthanks go to my colleague Wengen Chen, MD, PhD, who,as an intern on the Cardiovascular Council, assisted me byattaining summary slides from investigators in preparationfor this talk.
Vasken Dilsizian, MDUniversity of Maryland School of Medicine
Baltimore, MD
FIGURE 9. 18F-FDG and 11C-choline as atherosclerosis imag-ing agents.” Left: Autoradiograms and 11C-choline PET imagesin fasted (left) and nonfasted (right) mice. Right: Autoradiogramsand 18F-FDG PET images in fasted (left) and nonfasted (right)mice. 11C-choline PET results were as detailed and accurate asthose with 18F-FDG.
FIGURE 10. PET/MR imaging and uptake of 89Zr-labelednanoparticles in the aortic wall. Left: In vivo PET/MR imagesin an atherosclerotic rabbit model showing uptake of 89Zr-labeled liposome nanoparticles. Middle: Ex vivo PET imagingwith arrows indicating uptake in the aortic wall. Right: Ex vivoMR imaging with arrows indicating uptake.
FIGURE 11. Diagnosis of ventricular assist device (LVAD)thrombosis using a fibrin-specific 99mTc imaging agent. Staticimages of thrombus in excised LVADs from 3 patients with heartfailure showing: no thrombus formation in a control (left); inci-dental thrombus formation (center); and significant thrombusformation (right).
14N THE JOURNAL OF NUCLEAR MEDICINE • Vol. 55 • No. 10 • October 2014
NEW
SLIN
Eby on June 8, 2018. For personal use only. jnm.snmjournals.org Downloaded from

Dilsizian Recognized with Blumgart Award
In a special session on June 8 at the 61st SNMMI AnnualMeeting in St. Louis, MO, Vasken Dilsizian, MD, a pro-fessor in the Department of Diagnostic Radiology and
Nuclear Medicine and the Department of Medicine at theUniversity of Maryland School of Medicine (Baltimore,MD), was honored by the SNMMI Cardiovascular Councilwith the Hermann Blumgart Award. The award recognizesa key contributor to the science of nuclear cardiology whois also an advocate for the field through involvement withthe society’s research and educational activities. It is thehighest award presented by the Cardiovascular Council.
Dilsizian is director of Cardiovascular Nuclear Medicineand PET Imaging at Maryland and chief of the Division ofNuclear Medicine. He received his medical degree fromTufts University (Boston, MA), followed by internship andresidency in internal medicine at Georgetown UniversityHospital (Washington, DC). He completed additional fellow-ships and residencies at Boston University Medical Centerand Boston City Hospital (MA), Massachusetts GeneralHospital (Boston), and the Nuclear Medicine Division at theNational Institutes of Health (NIH; Bethesda, MD). Formore than 13 years he was a clinical investigator at NIH andfrom 1992 to 2001 was Director of Nuclear Cardiology atthe NIH Clinical Center. In 2001 he joined the faculty of theUniversity of Maryland.
In presenting Dilsizian with the award, the Cardiovas-cular Council noted that he is an internationally recognizedleader in cardiovascular nuclear imaging, with a focus onmyocardial viability and left ventricular remodeling inheart failure. His research efforts, including basic scienceinvestigations, radiotracer development, and clinical trials,have resulted in more than 170 peer-reviewed publications,9 texts, and more than 30 contributed chapters. He hasserved in editorial capacities on almost every major peer-reviewed cardiovascular journal and is a section editor ofthe Journal of the American College of Cardiology, as-sociate editor of the Journal of American College ofCardiology–Cardiovascular Imaging, and editor-in-chiefof Current Cardiovascular Imaging Reports. He is a co-editor of the Atlas of Nuclear Cardiology (now in its fourthedition) and Cardiac CT, PET and MR (now in its secondedition).
Dilsizian has been involved in many councils, commit-tees, and task forces of the American College of Car-diology (ACC), American Heart Association, AmericanSociety of Nuclear Cardiology (ASNC), and the SNMMI.
He served as the 2013–2014 president of the SNMMI Car-diovascular Council. He is on the boards of directors ofSNMMI and ASNC and serves as chair of the ACC TaskForce on Clinical Competence and Training in NuclearCardiology, on the Cardiovascular and Renal Drugs Advi-sory Committee of the U.S. Food and Drug Administration,and on the Nuclear Regulatory Commission’s AdvisoryCommittee on the Medical Uses of Isotopes.
In his acceptance lecture, titled “Scientific ProgressThrough the Guidance and Wisdom of Mentors,” Dilsizianpaid tribute to Blumgart, who was chair of the Departmentof Medicine at Beth Israel Hospital (New York, NY) from1928 to 1962. In 1925 Blumgart performed the first diag-nostic procedure using radioactive indicators in humans (onhimself). With Otto C. Yens, then a medical student, hedeveloped the first instrumentation (a modified cloudchamber) used in a diagnostic procedure involving radio-active indicators. He was also a noted educator, traininggenerations of medical leaders at Beth Israel.
“I am deeply honored by this award,” Dilsizian toldNewsline. “I am keenly aware that we all follow in thefootsteps of pioneers like Blumgart and am inspired toimpart this spirit of continuous inquiry and innovation toour current generation of trainees. This is an extraordinarilyexciting time for our field, and I am energized about meet-ing the challenges that new instrumentation, tracers, andtechniques bring to our collaborative efforts to improvecardiovascular care for patients worldwide.”
Mehran Sadeghi, MD, Vasken Dilsizian, MD, Mark Travin,MD, and Thomas Schindler, MD
Newsline 15N
NEW
SLIN
Eby on June 8, 2018. For personal use only. jnm.snmjournals.org Downloaded from
2014;55:9N-15N.J Nucl Med. 2014 SNMMI Highlights Lecture: Cardiovascular Imaging
http://jnm.snmjournals.org/content/55/10/9N.citationThis article and updated information are available at:
http://jnm.snmjournals.org/site/subscriptions/online.xhtml
Information about subscriptions to JNM can be found at:
http://jnm.snmjournals.org/site/misc/permission.xhtmlInformation about reproducing figures, tables, or other portions of this article can be found online at:
(Print ISSN: 0161-5505, Online ISSN: 2159-662X)1850 Samuel Morse Drive, Reston, VA 20190.SNMMI | Society of Nuclear Medicine and Molecular Imaging
is published monthly.The Journal of Nuclear Medicine
© Copyright 2014 SNMMI; all rights reserved.
by on June 8, 2018. For personal use only. jnm.snmjournals.org Downloaded from