-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
1/20
Winning at Failure
Modern Management of
Cardiogenic Pulmonary Edema
Amal Mattu, MD, FAAEM, FACEP
Professor and Vice Chair
Department of Emergency Medicine
University of Maryland School of Medicine
Baltimore, Maryland
Case
! 65 yo. man presents with dyspnea Developed over the past 6
hours History of hypertension, tobacco use Diaphoretic, normal
mental statusAfebrile, HR 110, BP 180/110, RR 26,
pox 88%
Lungs crackles, JVD
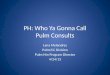
Case
Kerley B Lines
Cephalization
Case
! 100% NRB pulse ox 93%! Monitor, IV, ECG
Sinus tachycardia, no acute ST/T-waveabnormalities
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
2/20
Case
What is the optimal treatment in the first5-10 minutes??
a) morphineb) furosemidec) morphine + furosemided) nitroglycerin
+ (morphine + furosemide)e)
nesiritide + (morphine + furosemide)f) none of the above
OUTLINE
! Definition! Pathophysiology! Pharmacological management
Preload reductionAfterload reduction Inotropic support
! Noninvasive Positive Pressure Ventilation! Prehospital Issues!
Summary
CARDIOGENIC
PULMONARY EDEMA
! Definition: Leakage of fluid from the pulmonary
capillaries and venules into the alveolarspace as a result of
increased hydrostaticpressure
Inability of the LV to effectively handle itspulmonary venous
return
ANATOMY
lungs
Normal
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
3/20
PATHOLOGY
Pulmonaryedema!!
lungs
PHYSIOLOGY
preload
afterload
LV function
lungs
PATHOPHYSIOLOGY
preload
afterload
LV functionPulmonary edema!!
lungs
PATHOPHYSIOLOGY
preload
lungs
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
4/20
PATHOPHYSIOLOGY
1. increasedpreload
Pulmonary edema!!
lungs
PATHOPHYSIOLOGY
afterload
lungs
PATHOPHYSIOLOGY
2. increased
afterload
Pulmonary edema!!
lungs
PATHOPHYSIOLOGY
LV function
lungs
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
5/20
PATHOPHYSIOLOGY
3. decreasedLV function
Pulmonary edema!!
lungs
PATHOPHYSIOLOGY
2. increasedafterload
3. decreasedLV function
Pulmonary edema!!
lungs
1. increasedpreload
GOALS OF TREATMENT
1. decreasepreload
2. decreaseafterload
3. improveLV function
lungs
GOALS OF TREATMENT
lungs
body
Pulmonary edemaTotal body hypovolemia or euvolemia
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
6/20
CARDIOGENIC
PULMONARY EDEMA
! Note:more than 50% of patientswith cardiogenic pulmonary
edemaare euvolemic!!
! Treatment should be based notnecessarily on fluid removal, but
onfluid redistribution.
body
GOALS OF TREATMENT
Pulmonary edema
lungs
body
GOALS OF TREATMENT
lungs
body
CARDIOGENIC
PULMONARY EDEMA
! Causes Excessive venous return (preload) Excessive SVR
(afterload) LV dysfunction
" disorders of contractility" disorders of rate and rhythm
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
7/20
GOALS OF TREATMENT
1. decreasepreload
lungs
PRELOAD REDUCTION
! Traditional treatment Morphine Furosemide Nitrates
MORPHINE
!Advantages Histamine effect causes decrease in
preload
Anxiolysis may decrease catecholamines" decrease afterload
MORPHINE
! Disadvantages Side-effects may increasecatecholamines
" rash/urticaria from histamine release" nausea/vomiting
Respiratory depression with high doses Concerns if patient has
low blood pressure
" myocardial depressant Limited evidence (none?)to support
direct
hemodynamic benefits
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
8/20
MORPHINE
!Vismara, et al (Circulation, 1976) Effect of morphine on venous
tone in
patients with acute pulmonary edema
Evaluated venous pressure in the hand andforearm vessels
" venous pressure in the hand decreased, venousvolume in the
forearm increased
Does this correlate with decreasedpreload?
MORPHINE
! Lappas DG, et al (Anesthesiology, 1975) Filling pressures of
the heart and
pulmonary circulation in patients with CADafter intravenous
morphine
" 2 mg/kgIV morphine (5mg/min)" left and right heart filling
pressures increased" CI decreased
MORPHINE
! Timmis, et al, (Br Med J, 1980) 0.2 mg/kg IV morphine in AMI
patients
with severe LVF
15 and 45 minutes after injection, BP, HR,andCI decreased
No decrease in preload
MORPHINE
! Hoffman, et al (Chest, 1987) 57 patients with presumed
prehospital
diagnosis of pulmonary edema
38% subjective deterioration 46% objective deterioration No
patients receiving NTG without
morphine had deterioration
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
9/20
MORPHINE
! Sacchetti, et al (Am J Emerg Med,1999)
Odds ratios for intubation and ICUadmission for pulmonary edema
patients
Morphine 5 : 1
MORPHINE
! Peacock WF, et al (Emerg Med J, 2008) Morphine vs. no morphine
for acute
decompensated heart failure
" independent predictor of mortality (OR 4.84)" increased need
for mechanical ventilation, ICU
admission, prolonged hospitalization
MORPHINE
!Anxiolysis Decrease in catecholamines, afterload Why not use a
benzodiazepine???
" no concerns with rash/urticaria" no concerns with
nausea/vomiting" no concerns with respiratory depression"
no concerns with hypotension
SUMMARY MORPHINE
! Preload reduction Nitrates are superior
!Anxiolysis Side-effect profile favors benzodiazepines
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
10/20
CONCLUSION MORPHINE
Morphine has no rolein thetreatment of cardiogenicpulmonary
edema!
FUROSEMIDE
Wheres the debate??
FUROSEMIDE
! Preload reduction Diuresis
" increased afterload causes decreased RBF" delayed effect: 30
120 minutes
Direct vasoactivity" venodilation little evidence"
does this correlate with decreasedpreload?
FUROSEMIDE
! Pickkers P, et al (Circulation, 1997) Direct vascular effects
of furosemide on
the human forearm vascular bed anddorsal hand vein
" local administration of furosemide resultedin dose-dependent
venodilaton
Does this correlate with decreasedpreload?
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
11/20
FUROSEMIDE
! Kiely, et al (Circulation, 1973) Post-AMI CHF Furosemide
administered to 15 patients Significant reductions in filling
pressures
only in patients that had diuresis
FUROSEMIDE
! Ikram, et al (Clin Sci, 1980) IV furosemide administration in
acute CHF Significant reductions (17%) in CO during
first 90 minutes
CO gradually returned to baseline withdiuresis
FUROSEMIDE
! Nelson, et al (Eur Heart J, 1983) IV furosemide (1 mg/kg)
administration inAMI patients with LV failure
Initial adverse hemodynamic effects" decreases in CO and SV
during initial 90 minutes
Parameters returned to baseline over next60 90 minutes
FUROSEMIDE
! Francis, et al (Ann Intern Med, 1985) Class III or IV CHF
patients given IV furosemide Early adverse hemodynamic effects
" 20 minutes after administration!significant increase in HR,
SVR (afterload)!significant decrease in SV
Gradual return to baseline with diuresis
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
12/20
FUROSEMIDE
! Kraus, et al (Chest,1990) Effects of IV furosemide on PCWP
over 1 hour
in patients receiving nitrates and/or captopril
Furosemide alone or furosemide plus nitrates" increase in PCWP
over initial 15 minutes" then decrease PCWP with diuresis
If premedicatedwith nitrates plus captopril" immediate and
sustained decrease PCWP
SUMMARY FUROSEMIDE
! Decreases preload through diuresis Delayed effect
! No consistent data regarding immediatedirect preload reducing
effect
! Initial adverse hemodynamic effects Increased SVR Decreased
SV, CO
CONCLUSION
FUROSEMIDE
Furosemide should be considereda third-line medicationin
thetreatment of cardiogenicpulmonary edema!
NITROGLYCERIN
! Nitroglycerin vs. furosemide for preloadreduction
Cotter, et al (Lancet, 1998) Beltrame, et al (J Card Fail, 1998)
Kraus, et al (Chest, 1990) Hoffman, et al (Chest, 1987) Nelson, et
al (Lancet, 1983)
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
13/20
NITROGLYCERIN
!Advantages Rapid, reliable preload reduction Moderate/high
doses reduce SVR (afterload)
" maintains or improves SV and CO Multiple forms of
administration topical, SL,
IV (be aggressive!)
Short half-life; especially important ifprehospital
misdiagnosis
NITROGLYCERIN
! Caution in the presence of HypotensionAcute mitral
regurgitationAortic stenosis Pulmonary hypertension Patients
taking.
SUMMARY
NITROGLYCERIN
! Better than morphine or furosemide forpreload reduction
! Safer than morphine or furosemide inprehospital setting
! SL nitroglycerin provides rapid andeffective initiation of
treatment
Followed by topical NTG if moderate CPE Followed by IV NTG if
severe CPE
CONCLUSION
NITROGLYCERIN
Nitroglycerin should be first-lineprehospital and
emergencydepartment treatment formoderate CHF and
pulmonaryedema.
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
14/20
GOAL OF TREATMENT
2. decrease
afterloadlungs
AFTERLOAD REDUCTION
! Results in increased CO, restores renalblood flow
Nitroglycerin" SL and moderate/high dose IV" excellent single
agent for simultaneous preload
and afterload reduction
Nitroprusside" acute mitral regurgitation, severe
hypertension
HydralazineACE-inhibitorsfor acute CPE??
ACE-INHIBITORS
! Barnett, et al (Curr Ther Res, 1991) 25 mg SL captopril if BP
> 110 12.5 mg SL captopril if BP < 110 Decreased PCWP
(preload) noted by
10 minutes
No change in HR, MAP
ACE-INHIBITORS
! Barnett, et al (Curr Ther Res, 1991) 12 additional patients
with florid pulmonary
edema had significant improvement/completeresolution of dyspnea
by 15 minutes
" 8/12 patients abrupt increase in diuresiswithout the use of a
diuretic!(due to improvedrenal blood flow)
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
15/20
ACE-INHIBITORS
! Langes, et al (Curr Ther Res, 1993) IV captopril infusion in
moderate CHF or
pulmonary edema patients
Onset of action by 6 minutes Decreased PCWP (preload) Increased
CO No adverse effects
ACE-INHIBITORS
!Varriale, et al (Clin Cardiol, 1993) Hemodynamic response to
1.25 mg IV
enalaprilat in patients with severe CHF andsevere MR
Increased CO and SV Decreased MAP and SVR (afterload) Decreased
PCWP (preload) Decreased the magnitude of MR
ACE-INHIBITORS
! Sacchetti, et al (Am J Emerg Med,1999)
Odds ratios for intubation and ICUadmission for pulmonary edema
patients
SL captopril 0.28 : 1
ACE-INHIBITORS
! SL captopril Hamilton, et al (Acad Emerg Med, 1996) Haude, et
al (Int J Cardiol, 1990)
! IV enalaprilat Tohmo H, et al (Eur Heart J, 1994)Annane, et al
(Circulation, 1996)
! Dialysis patients with pulmonary edema Sacchetti A, et al (Am
J Emerg Med, 1993)
! SL and IV forms: hemodynamic and subjectiveimprovement can be
seen in 6 12 minutes!!
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
16/20
ACE-INHIBITORS
! Southall JC, et al (Acad Emerg Med, 2004) Safety of ED use of
SL captopril in NYHA
Class IV patients
" no increased incidence of hypotension or need
forvasopressors
" decreased ICU length of stay (29 hrs vs. 78 hrs.)
SUMMARY
ACE-INHIBITORS
! Rapid reduction in afterload and preload! Rapid reduction in
level of distress! Decreased need for intubation, ICU use
Bed availability, hospital costs! Combination with NTG exceeds
benefit of
either drug alone
!Acceptable alternative to IV NTG
CONCLUSION
ACE-INHIBITORS
ACE-inhibitors should beconsidered second-line agentsfor
moderate CHF or pulmonaryedema; first-line in patientsunable to
tolerate nitrates.
PRELOAD AND
AFTERLOAD REDUCTION
! Tei, et al (Circulation, 1995) Studied the effects of thermal
vasodilation
in 34 CHF patients (mean EF 25%)
Exposure to sauna for 15 minutes" significant decreases in PCWP
(preload)" significant decreases in SVR (afterload)" significant
decreases in MR" significant increases in CI, SV, and EF
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
17/20
GOAL OF TREATMENT
3. improveLV function
lungs
INOTROPIC SUPPORT
! Choices Catecholamines
" dopamine" dobutamine
Phosphodiesterase inhibitors (milrinone) IABP (bridging device
before PTCA/CABG)
CATECHOLAMINES
! Drawbacks Tachycardia/arrhythmias Increased MO2consumption,
ischemia Myocardial beta-receptors up-regulated in
severe CHF, tolerance develops
!standard doses are less effective!higher doses needed, more
adverse effects
Chronic beta-blocker use decreases efficacy
PHOSPHODIESTERASE
INHIBITORS (MILRINONE)
! Work independent of adrenoreceptor activityand plasma CA
levels
Work well even in patients on beta-blockers! Induce inotropic
support as well asdecreased
preload and afterload
! No development of tolerance!
Butno mortality benefit vs. dobutamine
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
18/20
CONCLUSION
INOTROPIC SUPPORT
Use what you are comfortablewith.
Consider use of milrinone forpulmonary edema
patientsunresponsive to DA/DBT.
NONINVASIVE POSITIVE
PRESSURE VENTILATION
! Maintains positive airway pressure duringentire respiratory
cycle
Maintains patency of stiff fluid-filled alveoli,prevents
collapse during exhalation
Increases intrathoracic pressure" decreases preload and
afterload (and increases CO)
SUMMARY NPPV
! Noninvasive positive pressureventilation is associated
with:
Decreased work of breathing Improved O2and CO2exchange Improved
preload, afterload, and CO Reduced need for intubation, ICU LOS
Reduced hospital costs Reduced mortality (?)
CONCLUSION NPPV
NPPV is an effective method ofproviding airway support
andaverting intubation in somepatients (but it must be
usedearly!!)
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
19/20
SUMMARY
! Nitroglycerin first-line agent IV nitroglycerin is excellent
single-agent
!ACE-inhibitors second-line agent In addition to or instead of
nitroglycerin
! Furosemide third-line agentAfter preload and afterload
reduction
SUMMARY
! Morphine just say no! Preload reduction NTG more
effectiveAnxiolysis BZDs have fewer side effects
! Nesiritide May prove useful for patients not
responding to optimal treatmentpending more studies
SUMMARY
! Inotropic support No data favors any specific agent Use what
you are comfortable with!
! NPPV consider earlyuse Decreased intubations, ICU length of
stay,
and hospital costs
Case
! 65 yo. man presents with dyspnea Developed over the past 6
hours History of hypertension, tobacco use Diaphoretic, normal
mental statusAfebrile, HR 110, BP 180/110, RR 26,
pox 88%
Lungscrackles, JVD
-
8/14/2019 3_12_Mattu_Cardiogenic Pulm Edema.pdf
20/20
Case
! 100% NRBpulse ox 93%! Monitor, IV, ECG
Sinus tachycardia, no acute ST/T-waveabnls.
Case
What is the optimal treatment in the first5-10 minutes??
1. noninvasive ventilation2. SL NTG q5 min (x 3-4 doses)3. 1.25
mg IV enalapril or 25 mg SL captopril
(OR rapid titration of high dose IV NTG)
4. furosemide AFTER above given
REMEMBER!
!More than 50% of patients withcardiogenic pulmonary edemaare
euvolemic!!
!Treatment should be based notnecessarily on fluid removal,but
on fluid redistribution.