Embed Size (px)
Citation preview


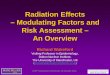
Definition ofDefinition ofHypercholesterolemiaHypercholesterolemia

Total cholesterol by age and sexTotal cholesterol by age and sexAverage distribution of plasma total cholesterol (means and selected percentiles)
Pla
sm
a to
tal c
ho
les
tero
l (m
g/d
L)
Age (years) Age (years)
320
280
240
200
160
120
0 10 20 30 40 50 60 70 0 10 20 30 40 50 60 70
White males White females
90th
Mean
50th
10th
90th
Mean
50th
10th

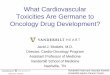
Risk Factors:Risk Factors: Serum CholesterolSerum Cholesterol(carried by LDL particles)(carried by LDL particles)
How do we know who is at risk?
ALSO Implicated:Family History
Smoking why?
Hypertension why?
Death rate per 1000 men
Percentilemmol/l
18
161412
10
86
4
2
05 15 25 35 45 55 65 75 85 954.1 4.8 5.3 5.8 6.5 7.8
Top 15% cholesterol = 43/1000
N = 100/1000 50%
Serum Cholesterol in N = 360,000 men over 6 years

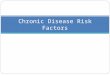
CHD Risk FactorsCHD Risk Factors
0
5
10
15
20
25
30
35
40
4.5 5 5.5 6 6.5 7 7.5 8 8.5 9
Low HDLCholesterol
Smoking
Hyperglycemia
Hypertension
No other riskfactors
Plasma Cholesterol (mmol/l)
%

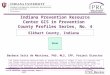
Note – those countries with risk also have serum cholesterol dietary fat & cholesterol intake
FinlandUSA
New ZeelandAustralia
UKIreland
CanadaNorway
Belgium-Lux.Yugoslavia
DenmarkNetherlands
West GermanyAustria
SwedenItaly
SwitzerlandPortugal
SpainFranceGreeceJapan
IsochemicHeart disease
Other possiblecoronary deaths
0 100 200 300 400 500 600Mortality rates per 100,000
Mortality rates due to coronary heart diseaseMortality rates due to coronary heart disease

2
1
0.5
100 200 300
Relative Risk of Death From CHD by blood cholesterolRelative Risk of Death From CHD by blood cholesterol (mg/dl)(mg/dl) 6 prospective studies6 prospective studies
100 200 300 100 200 300
2
1
0.5
Finland347 CHD
MRFIT (US)3,243 CHD
Whitehall (UK)455 CHD
Framingham (US)216 CHD
Israel615 CHD
Hawaii242 CHD

Ideal, Feasible And Existing Total Ideal, Feasible And Existing Total Serum Cholesterol Levels in AdultsSerum Cholesterol Levels in Adults
Ideal Mean 4.3 mMl
2.7 4.0 5.4 6.7 8.1
Feasible Mean 5.1 mM
Present Mean 5.7 mM
Total Serum Cholesterol mmol/L

CANADIAN HEART HEALTH SURVEYCANADIAN HEART HEALTH SURVEYPREVALENCE OF TOTAL CHOLESTEROL LEVELSPREVALENCE OF TOTAL CHOLESTEROL LEVELS
0
10
20
30
40
50
60
70
<5.2mmol/l
5.2-6.1mmol/l
>6.2mmol/l
MENWOMENTOTAL
%
52%57% 55%
30% 27%29%
18%16%17%

Classification Based on Total Blood CholesterolClassification Based on Total Blood Cholesterol mg/dl (mmol/L=mM)
Men & Women
Age
Desirable Moderate Risk
High Risk
18-30 <180
(4.6)
180-220
(4.6-5.7)
220+
(5.7)
30+ <200
(5.2)
200-240
(5.2-6.2)
240+
(6.2)

What is the risk of coronary heart disease in the next 6 years What is the risk of coronary heart disease in the next 6 years in these individuals?in these individuals? [ 1%, 5%, 10%, 15%, 25%, 35%, 60%, 90% ]
« WORST » SYSTOLICBLOOD
AGE SEX TOTAL HDL PRESSURE DIABETES SMOKING
1. 55 M 7.2 0.8 150 NO YES
2. 55 F 7.2 0.8 150 NO YES
3. 55 M 7.2 0.8 150 NO NO
4. 55 M 5.2 1.1 150 NO YES
5. 55 M 5.2 1.1 120 NO NO
6. 55 M 10.0 0.8 170 YES YES
7. 25 M 10.0 0.8 170 YES YES
8. 55 F 10.0 0.8 170 YES YES
9. 25 M 7.2 0.8 150 NO YES

What is the risk of coronary heart disease in the next 6 years What is the risk of coronary heart disease in the next 6 years in these individuals?in these individuals? [ 1%, 5%, 10%, 15%, 25%, 35%, 60%, 90% ]
« LEAST LIKELY » SYSTOLICBLOOD
AGE SEX TOTAL HDL PRESSURE DIABETES SMOKING
1. 55 M 7.2 0.8 150 NO YES
2. 55 F 7.2 0.8 150 NO YES
3. 55 M 7.2 0.8 150 NO NO
4. 55 M 5.2 1.1 150 NO YES
5. 55 M 5.2 1.1 120 NO NO
6. 55 M 10.0 0.8 170 YES YES
7. 25 M 10.0 0.8 170 YES YES
8. 55 F 10.0 0.8 170 YES YES
9. 25 M 7.2 0.8 150 NO YES

What is the risk of coronary heart disease in the next 6 years What is the risk of coronary heart disease in the next 6 years in these individuals?in these individuals? [ 1%, 5%, 10%, 15%, 25%, 35%, 60%, 90% ]
SYSTOLICBLOOD
AGE SEX TOTAL HDL PRESSURE DIABETES SMOKING
1. 55 M 7.2 0.8 150 NO YES
2. 55 F 7.2 0.8 150 NO YES
3. 55 M 7.2 0.8 150 NO NO
4. 55 M 5.2 1.1 150 NO YES
5. 55 M 5.2 1.1 120 NO NO
6. 55 M 10.0 0.8 170 YES YES
7. 25 M 10.0 0.8 170 YES YES
8. 55 F 10.0 0.8 170 YES YES
9. 25 M 7.2 0.8 150 NO YES
26%
35%

What is the risk of coronary heart disease in the next 6 years What is the risk of coronary heart disease in the next 6 years in these individuals?in these individuals? [ 1%, 5%, 10%, 15%, 25%, 35%, 60%, 90% ]
SYSTOLICBLOOD
AGE SEX TOTAL HDL PRESSURE DIABETES SMOKING
1. 55 M 7.2 0.8 150 NO YES
2. 55 F 7.2 0.8 150 NO YES
3. 55 M 7.2 0.8 150 NO NO
4. 55 M 5.2 1.1 150 NO YES
5. 55 M 5.2 1.1 120 NO NO
6. 55 M 10.0 0.8 170 YES YES
7. 25 M 10.0 0.8 170 YES YES
8. 55 F 10.0 0.8 170 YES YES
9. 25 M 7.2 0.8 150 NO YES
10%
15%
10%
5%
10%

LDLC = TC – HDL – (TG/2)
< 3.5 nM < 5.2 mM > 1.5 – 2.0 < 2.0 mM
ppt
Chylo LDL VLDLVLDL VLDLLDLHDL
95% Fasting NOApo B Chylos no apoB very littleParticles apoB in VLDL80-120 mg/dL
Calculation of LDL CholesterolCalculation of LDL Cholesterol

Calculation of Calculation of LDL CholesterolLDL Cholesterol
LDL C = TC – HDL C – (TG/2)
3.0 = 6.0 – 1.0 – (4.0/2)calculated(not direct)
apoB = < 120(direct)

LDL cholesterol and apoB LDL cholesterol and apoB distribution in CAD patientsdistribution in CAD patients

Threshold Effect of LDL CholesterolThreshold Effect of LDL CholesterolF
req
uen
cy
50LDL Cholesterol
56.5% of CAD had LDL C > 50th percentile, therefore no threshold for LDL C.
N
CAD

Threshold for LDL Particle NumberThreshold for LDL Particle Number
88% of CAD had LDL apoB > 50th percentile NA population.
Fre
qu
ency
50LDL apoB
N
CAD

Lipoprotein ScreeningLipoprotein Screening
Canadian Consensus Conference on Cholesterol• « As resources permit »• A priority for those with risk factors and established CHD
U.S. National Cholesterol Education Program• At least every five years for all adults aged 20 and over• More often as follow-up for those with elevated serum cholesterol
Canadian Cardiovascular Society• Within 24 hours of myocardial infraction, repeated 6-12 weeks after hospital discharge

CCCC recommendations: CCCC recommendations: Screening prioritiesScreening priorities
Screening for priority groups• Priority screening for individuals with:
•Coronary heart disease•Family history of hyperlipidemia or CHD at an early age•Hypertension•Diabetes•Renal failure•Abdominal obesity
Screening for all Canadians• As part of a periodic health examination

Interpretation Interpretation of Lipid Valuesof Lipid Values
Men and WomenAge 18-29
DRUGS?
DIETARY MODIFICATION
TG>200
HDL<35
LDL>115
39%
19%
180(4.6)
220(5.7)
Other risk factors
mg/dl(mM/L)
Other risk factors

Coronary Heart DiseaseCoronary Heart DiseaseMain Risk FactorsMain Risk Factors
Non-Modifiable Modifiable
Family History of CHD Dyslipidemia
Male Sex Hypertension
Age Diabetes
Smoking
Obesity

Normal Endothelial FunctionNormal Endothelial Function
EDRF
PC
EDRF
PC EDRF
PC
EDRF
EDRF EDRF

B
B
B
B
B
B
In One Door…In One Door…And Out the OtherAnd Out the Other

Tg Tg Tg TgTg Tg Tg Tg Tg Tg Tg Tg Tg Tg
CE CECE CE CE
B
CE CE CE CETg
B
VLDL
LDL

B
B
B
B
B
The Pathogenic PowerThe Pathogenic PowerOf Particle NumberOf Particle Number
B
BB
BB
B
B
B
B
B
B

B
B
B
BB
B
B
B
B
B
B
B
Oxidation of LDL ParticlesOxidation of LDL Particleswithin the vessel wallwithin the vessel wall
B
B

Hypertension Hypertension → Subintimal Thickening→ Subintimal Thickening

400
350
300
250
200
150
100
50
0
0 2 4 6 8 10
mo
l F
ibri
no
gen
X 1
012/c
m2
Perfusion Time (MIN)
n=17 n=20 n=22
*
*
*
High Shear,Non-ParallelSreamlines
Low Shear,ParallelSreamlines
Effect of Shear Rate and Flow Effect of Shear Rate and Flow Condition on Fibrinogen DepositionCondition on Fibrinogen Deposition

HyperapoB HyperapoB →→HyperthrombogenicityHyperthrombogenicity
↑ PAI-1↑ Fibrinogen↑ Factor VII↑ Factor VII c
+← ↑ FFA ← ↑
CE
B
TgCETg
B
CETg
B
CETg
B
CETg
B
CETg
B
CETg
B

B
B
B
B
B B B
Thicker ithThlower

CAD Mortality in NIDDMCAD Mortality in NIDDM
60
50
40
30
20
10
0
MortalityRate per
1000
0-3 4-7 8-11 13-15 18-19 20-23 0-3 4-7 8-11 13-15 18-19 20-23
Duration of Follow-up (years)
Men Women
DiabetesDiabetes
No Diabetes
No Diabetes

Can Glucose Glycate Glycosaminoglycans
which then Grab apoB?
B
B
B
B
BB B
B

Relative odds of developing IHD over a 5-yr follow-up Relative odds of developing IHD over a 5-yr follow-up period in a sample of 91 IHD cases and 91 matched controlsperiod in a sample of 91 IHD cases and 91 matched controls
The Quebec Cardiovascular Study
0
3
6
9
12
15
<72 72< <91 >91
Relative Odds
>50th<50th
Total HDL-C
Fasting Insulin (pmol/l)
1.0
3.8
4.4
8.7
6.3
14.1
RO adjusted for medication, systolic BP, family history of IHD

Why is smoking atherogenic?Why is smoking atherogenic?
Tg
B
CE
Tg
B
CE
Tg
B
CE

A Dysfunctional ArteryA Dysfunctional Artery↓EDRF
↑TF
↓t-PA ↑PAI-1 ↓EDRF ↓PC ↑TF
Tg
B
CE
Tg
B
CE
Tg
B
CE

Risk Factor – Obesity!Risk Factor – Obesity!
Although excess obesity is a risk factor, so is moderate obesity especially abdominal android obesity:
-“beer belly” -Men diabetes hypertension

BMI age men
CORONARY MORBIDITY AND MORTALITYCORONARY MORBIDITY AND MORTALITYASSOCIATED WITH RELATIVE WEIGHTASSOCIATED WITH RELATIVE WEIGHT
Metropolitan relative weight
Ag
e-ad
just
ed a
nn
ual
rat
e p
er 1
,000
35 -30 -25 -20 -15 -10 -
5 -
54-104 105-114 115-124 125-134 135-272
Men aged65-94 years(p<0.01)
Women aged65-94 years(p<0.05)
Men aged35-64 years(p<0.001)
Women aged35-64 years(p<0.001)

Alcohol
Obesity
DietSaturated Fat Salt
GeneticSusceptibility
Kidney Damage
Diabetes
HighBloodPressure
OC’s (female)
Smoking
Psycho-SocialFactorsFamily
History of CVD
DietaryCholesterol
PhysicalActivity
BloodLipids
AgeSex (male)
Lower S/E
CVDIHD
Stroke

RISK FACTORS FOR CORONARY ARTERY DISEASERISK FACTORS FOR CORONARY ARTERY DISEASE
Modifiable•Smoking (> 10 cigarettes / day)•Obesity, especially Android Obesity•Hypercholesterolemia and/or Low HDL cholesterol (< 1 mM) *: A high HDL cholesterol (>1.6 mM) is a negative risk factor (i.e. protective)•Hypertension (> 140/90 or treated)•Diabetes Mellitus
•*** MODIFIABLE BY DIETMODIFIABLE BY DIET
•Non Modifiable•Age (>45 in men, >55 in women)•Family history of premature coronary artery disease: Myocardial infarct or sudden death in a 1st degree parent < 55 years of age.•Gender (males are at increased risk