Embed Size (px)
Citation preview

N E W S L E T T E R A p r i l 2 0 1 6 E d i t i o n
SOGH is dedicated to enhancing the safety and quality of OB/GYN Hospital Medicine by promoting excellence through education, coordination of hospital teams, and
collaboration with healthcare delivery systems.
Newsletter articles and content © Society of OB/GYN Hospitalists
www.societyofobgynhospitalists.org
11200 Broadway, Suite 2743 Pearland, TX 77584
E-mail: [email protected] Twitter & Instagram: @SOGHofficial
SOGHNewsletter4.2016
“CODETHIS!”(CaseoftheMonth)MissedAbortion,RetainedPOCwithChorioamnionitistreatedwithD&C
byLori-LynneA.Webb,CPCandReneeAllen,MD,FACOGFebruary25,2016CaseExcerpt(summaryandnarrativeofactualcase):
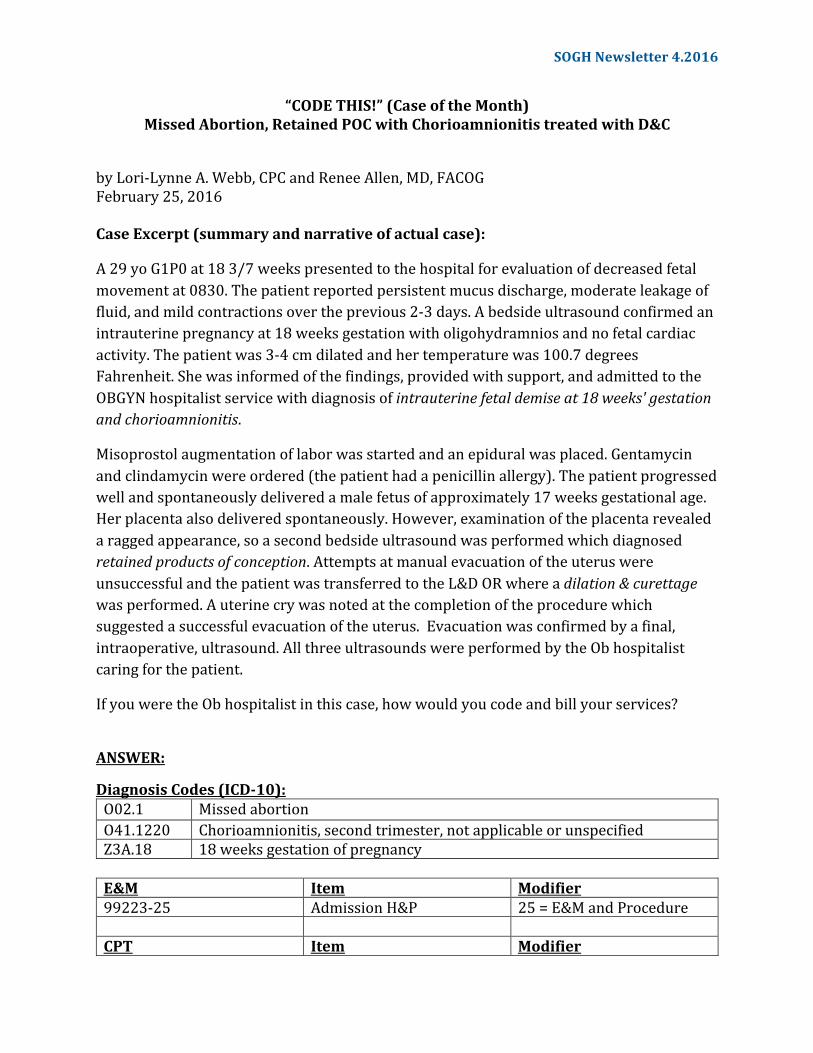
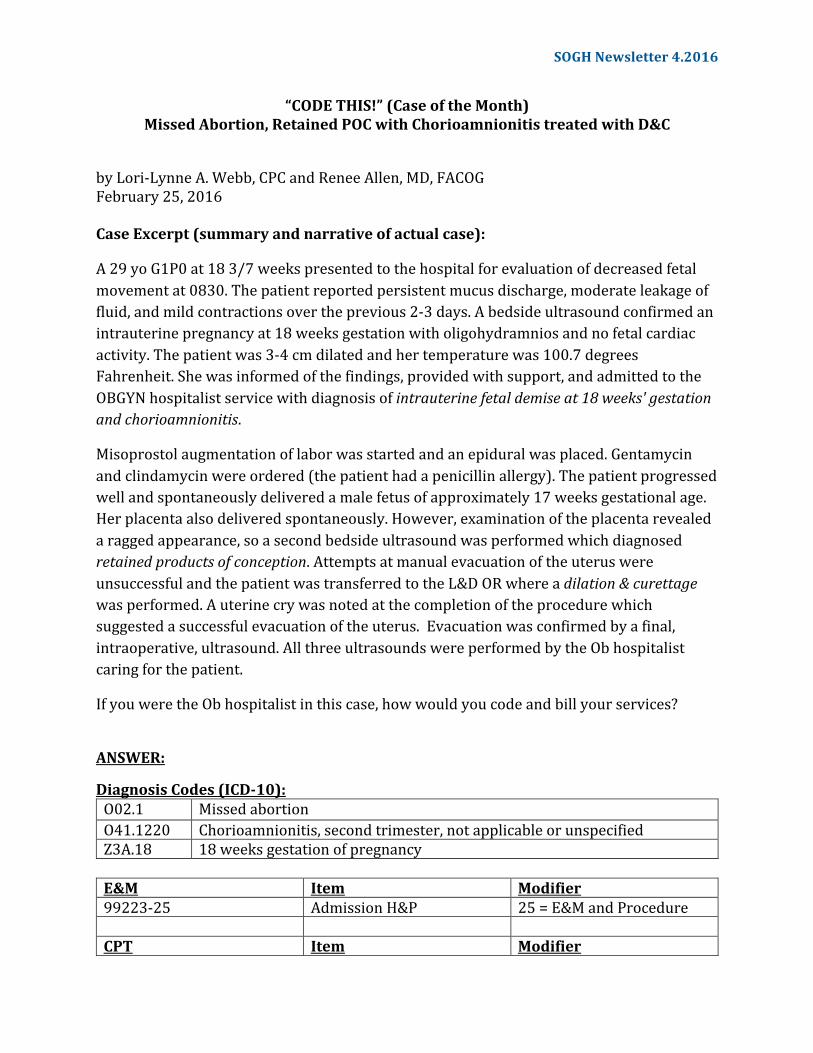
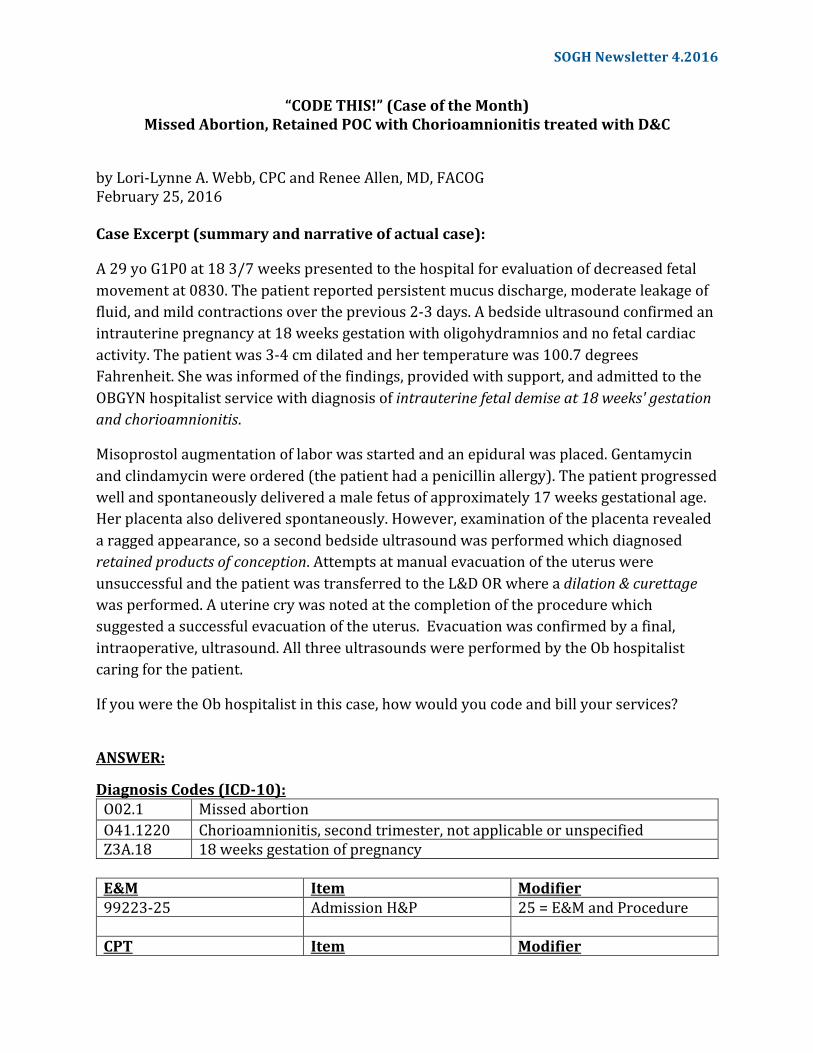
A29yoG1P0at183/7weekspresentedtothehospitalforevaluationofdecreasedfetalmovementat0830.Thepatientreportedpersistentmucusdischarge,moderateleakageoffluid,andmildcontractionsovertheprevious2-3days.Abedsideultrasoundconfirmedanintrauterinepregnancyat18weeksgestationwitholigohydramniosandnofetalcardiacactivity.Thepatientwas3-4cmdilatedandhertemperaturewas100.7degreesFahrenheit.Shewasinformedofthefindings,providedwithsupport,andadmittedtotheOBGYNhospitalistservicewithdiagnosisofintrauterinefetaldemiseat18weeks'gestationandchorioamnionitis.
Misoprostolaugmentationoflaborwasstartedandanepiduralwasplaced.Gentamycinandclindamycinwereordered(thepatienthadapenicillinallergy).Thepatientprogressedwellandspontaneouslydeliveredamalefetusofapproximately17weeksgestationalage.Herplacentaalsodeliveredspontaneously.However,examinationoftheplacentarevealedaraggedappearance,soasecondbedsideultrasoundwasperformedwhichdiagnosedretainedproductsofconception.AttemptsatmanualevacuationoftheuteruswereunsuccessfulandthepatientwastransferredtotheL&DORwhereadilation&curettagewasperformed.Auterinecrywasnotedatthecompletionoftheprocedurewhichsuggestedasuccessfulevacuationoftheuterus.Evacuationwasconfirmedbyafinal,intraoperative,ultrasound.AllthreeultrasoundswereperformedbytheObhospitalistcaringforthepatient.
IfyouweretheObhospitalistinthiscase,howwouldyoucodeandbillyourservices?
ANSWER:
DiagnosisCodes(ICD-10):O02.1 MissedabortionO41.1220 Chorioamnionitis,secondtrimester,notapplicableorunspecifiedZ3A.18 18weeksgestationofpregnancyE&M Item Modifier99223-25 AdmissionH&P 25=E&MandProcedure CPT Item Modifier
SOGHNewsletter4.2016
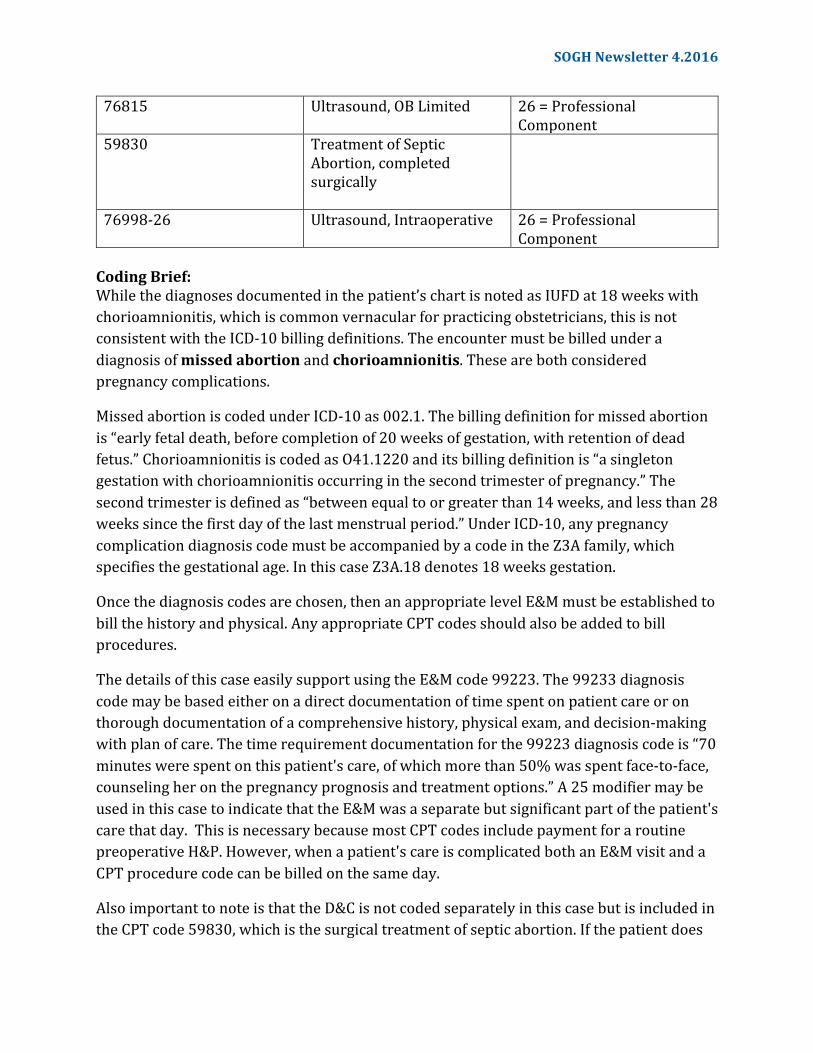
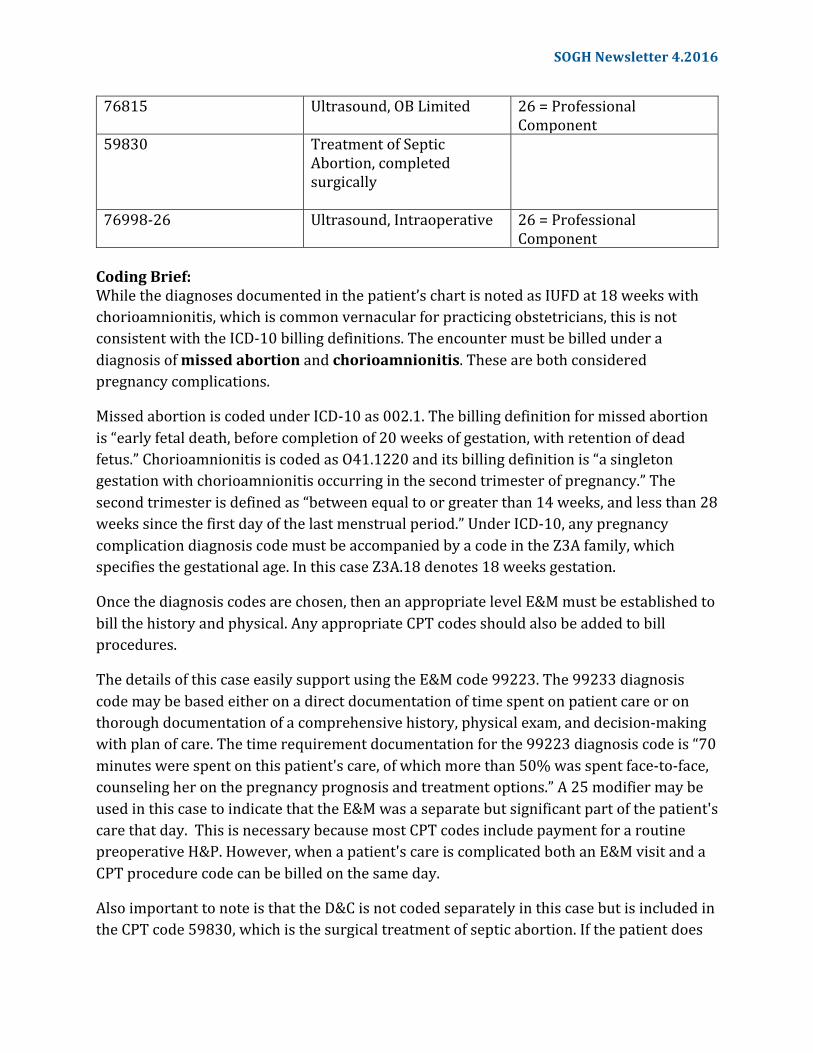
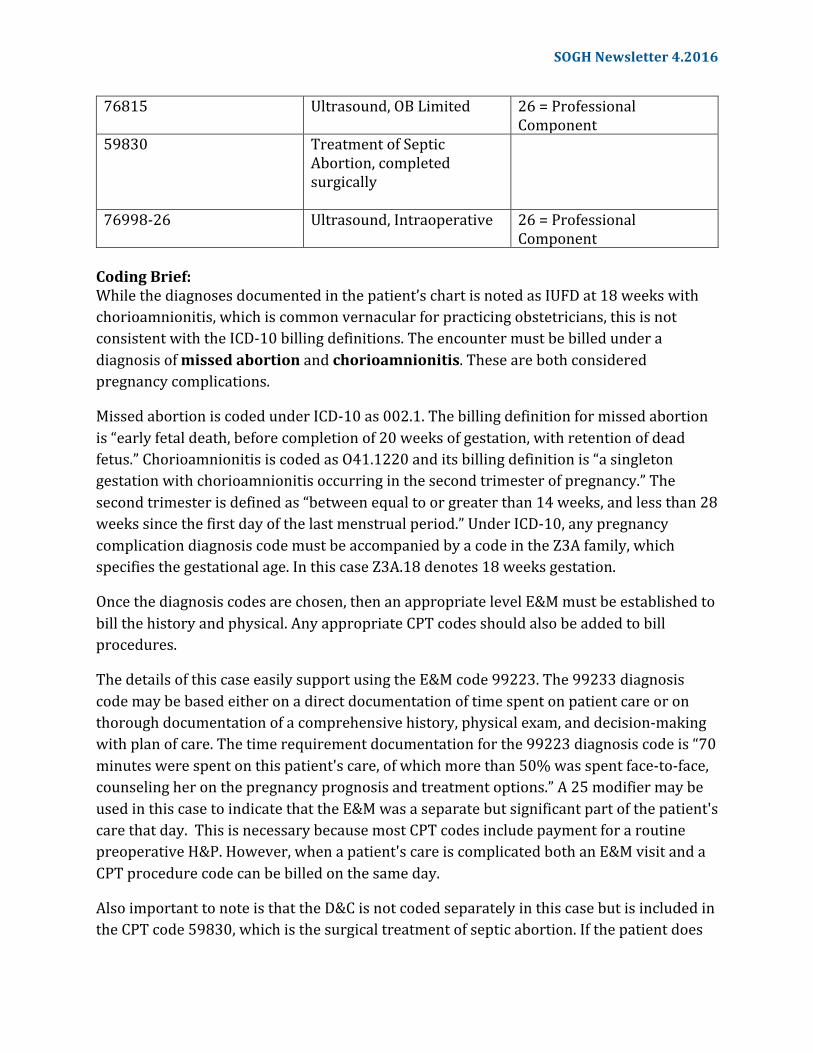
76815 Ultrasound,OBLimited 26=ProfessionalComponent
59830 TreatmentofSepticAbortion,completedsurgically
76998-26 Ultrasound,Intraoperative 26=ProfessionalComponent
CodingBrief:Whilethediagnosesdocumentedinthepatient’schartisnotedasIUFDat18weekswithchorioamnionitis,whichiscommonvernacularforpracticingobstetricians,thisisnotconsistentwiththeICD-10billingdefinitions.Theencountermustbebilledunderadiagnosisofmissedabortionandchorioamnionitis.Thesearebothconsideredpregnancycomplications.
MissedabortioniscodedunderICD-10as002.1.Thebillingdefinitionformissedabortionis“earlyfetaldeath,beforecompletionof20weeksofgestation,withretentionofdeadfetus.”ChorioamnionitisiscodedasO41.1220anditsbillingdefinitionis“asingletongestationwithchorioamnionitisoccurringinthesecondtrimesterofpregnancy.”Thesecondtrimesterisdefinedas“betweenequaltoorgreaterthan14weeks,andlessthan28weekssincethefirstdayofthelastmenstrualperiod.”UnderICD-10,anypregnancycomplicationdiagnosiscodemustbeaccompaniedbyacodeintheZ3Afamily,whichspecifiesthegestationalage.InthiscaseZ3A.18denotes18weeksgestation.
Oncethediagnosiscodesarechosen,thenanappropriatelevelE&Mmustbeestablishedtobillthehistoryandphysical.AnyappropriateCPTcodesshouldalsobeaddedtobillprocedures.
ThedetailsofthiscaseeasilysupportusingtheE&Mcode99223.The99233diagnosiscodemaybebasedeitheronadirectdocumentationoftimespentonpatientcareoronthoroughdocumentationofacomprehensivehistory,physicalexam,anddecision-makingwithplanofcare.Thetimerequirementdocumentationforthe99223diagnosiscodeis“70minuteswerespentonthispatient'scare,ofwhichmorethan50%wasspentface-to-face,counselingheronthepregnancyprognosisandtreatmentoptions.”A25modifiermaybeusedinthiscasetoindicatethattheE&Mwasaseparatebutsignificantpartofthepatient'scarethatday.ThisisnecessarybecausemostCPTcodesincludepaymentforaroutinepreoperativeH&P.However,whenapatient'scareiscomplicatedbothanE&MvisitandaCPTprocedurecodecanbebilledonthesameday.
AlsoimportanttonoteisthattheD&CisnotcodedseparatelyinthiscasebutisincludedintheCPTcode59830,whichisthesurgicaltreatmentofsepticabortion.Ifthepatientdoes
SOGHNewsletter4.2016
notrequireaD&Ctoremovetheretainedproductsofconceptionoranyothersurgicalintervention,thiswouldprecludetheuseofthe59830CPTcode.
Finally,theCPTcodeforeachultrasoundcanbesubmittedandbilledseparately.Billinganultrasounddoesrequirethateachultrasoundbedocumentedinaseparatereport.Inaddition,imagesmustbesavedaspartofthepatient’smedicalrecord.Assumingtheuseofanultrasoundmachineownedbythehospital,youmaybillfortheprofessionalcomponentonlyandnotthetechnicalcomponentorfacilityfee.Lori-LynneA.Webb,CPC,CCS-P,CCP,CHDA,COBGCandICD10CM/PCSAmbassador/TrainerisanE&M,andProcedurebasedCoding,Compliance,DataChargeentryandHIPAAPrivacyspecialist,withover20yearsofexperience.Lori-Lynne’scodingspecialtyisOB/GYNoffice&HospitalistServices,MaternalFetalMedicine,OB/GYNOncology,Urology,andgeneralsurgicalcoding.Shecanbereachedviae-mailatwebbservices.lori@gmail.comoryoucanalsofindcurrentcodinginformationonherblogsite:http://lori-lynnescodingcoachblog.blogspot.com/.Dr.RenéeAllenservedasco-authorofthiscolumn.SheistheSOGHLiaisontotheACOGCommitteeonHealthEconomicsandCoding.ShecurrentlyworksasanOB/GYNHospitalistwithMednax/ObstetrixatEastsideMedicalCenterinSnellville,Georgia.
Questionsregardingthiscase?Contactusatcoding@societyofobgynhospitalists.org.
SOGH Newsletter 4.2016
PracticeMattersbyJoanneRichards,MDFebruary19,2016OBHospitalistprogramsarearelativelynewdivisionofOB/GYN,evolvingasthenumberofprogramsincreaseduetoincreasingdemands.Hospitalsindifferentcommunitieshavedifferingneeds,callingforflexibilityinwhatdefinestheroleofanOb/Gynhospitalistineachprogram.Ourprogram,theObstetrixOBHospitalistGroupatGoodSamaritanHospitalinSanJose,CAismeshedwiththeMednax(formerlyObstetrix)MFMgroupinSanJose.BoththeOb/Gynhospitalists,andtheperinatologists(MFM)areemployedbyMednax.OurOBGYNhospitalistprogramisalsopartiallyfundedbyGoodSamaritanHospital.Unlikeotherhospitalistemployers,Mednaxisanationalmedicalgroupcomprisedofneonatal,anesthesia,perinatologyandpediatricphysiciansaswellasOBHospitalists.Benefitsandcompensationarecorporatebased,butourprogramisuniquetotheSanJoseMFMgroup.TheSanJose,CAOb/GynHospitalistgroupbeganinJanuary2007atGoodSamaritanHospital.ItwasdesignedbyDr.AlanFishman,clinicaldirectoroftheSanJoseMFMgroup.Priorto2007,ourprivatephysicianshandledallthepatientsintheirowncallgroups.TheysawallOBtriageandEDgynecologypatientsfortheirowngroupsaswellastakingarotationalcallforunassignedpatientsbothintheEDandL&D.Otherobstetriciansorregisterednursefirstassistants(RNFA)providedsurgicalassistance.Beforeitwasrolledout,Dr.FishmanmetwiththecommunityOb/Gynphysicianstodiscusshowthenewprogramwouldinterfacewiththeircurrentpracticesandhowtheuseofhospitalistscouldbenefitbothphysiciansandpatients.TheOb/GynhospitalistsattendedaneighthourorientationwiththeperinatologistsandMednaxcorporateofficewhichdetailedpatientmanagement,billing,call,andthegeneraloperationaldetailsoftheprogram.TheprogrambeganinJanuary,2007andhassinceexpandedtoencompassourcurrentresponsibilities.Weareagroupoffourfulltimeandtwoparttimeemployeesworkingwithfiveperinatologists.GoodSamaritanHospitalperforms300-400deliveriespermonth.Wehave14laborroomsand3laboranddeliveryoperatingrooms.Thereis24hourdedicatedOBanesthesiaontheflooraswell.TheOb/Gynhospitalistsprovide24hr/7daycoveragein24hrshifts.Weprovideobstetricservicesforpatientswhodonothaveaprovideronstaff,coverageforanystaffobstetricianwhorequestsourservices,includingassistanceinC-sections,andweprovideemergencygynecologicalservicestotheunassignedgynpatients.Wealsoperformin-hospitalgynconsultsforpatientswithnostaffproviderandmakeappropriatereferralsforoutpatientfollowup.Inaddition,wearethefirstrespondersforallobstetricsandgynecologicalemergencies,includinganyunattendeddeliveries.OurgroupperformstriageevaluationforalltheperinatalpatientspresentingtotheObstetricsEmergencyDepartment(OBED)aswellasforpatientsoftheprivatepracticesuponrequest.AllOBEDpatientsarerequiredtobeseenbyaphysicianpriortodischarge,exceptthosepresentingforlaborevaluations.Wehavenooutpatientresponsibilities,soallpatientsarereferredforappropriatefollow-uppriortotheir
SOGHNewsletter4.2016
“CODETHIS!”(CaseoftheMonth)MissedAbortion,RetainedPOCwithChorioamnionitistreatedwithD&C
byLori-LynneA.Webb,CPCandReneeAllen,MD,FACOGFebruary25,2016CaseExcerpt(summaryandnarrativeofactualcase):
A29yoG1P0at183/7weekspresentedtothehospitalforevaluationofdecreasedfetalmovementat0830.Thepatientreportedpersistentmucusdischarge,moderateleakageoffluid,andmildcontractionsovertheprevious2-3days.Abedsideultrasoundconfirmedanintrauterinepregnancyat18weeksgestationwitholigohydramniosandnofetalcardiacactivity.Thepatientwas3-4cmdilatedandhertemperaturewas100.7degreesFahrenheit.Shewasinformedofthefindings,providedwithsupport,andadmittedtotheOBGYNhospitalistservicewithdiagnosisofintrauterinefetaldemiseat18weeks'gestationandchorioamnionitis.
Misoprostolaugmentationoflaborwasstartedandanepiduralwasplaced.Gentamycinandclindamycinwereordered(thepatienthadapenicillinallergy).Thepatientprogressedwellandspontaneouslydeliveredamalefetusofapproximately17weeksgestationalage.Herplacentaalsodeliveredspontaneously.However,examinationoftheplacentarevealedaraggedappearance,soasecondbedsideultrasoundwasperformedwhichdiagnosedretainedproductsofconception.AttemptsatmanualevacuationoftheuteruswereunsuccessfulandthepatientwastransferredtotheL&DORwhereadilation&curettagewasperformed.Auterinecrywasnotedatthecompletionoftheprocedurewhichsuggestedasuccessfulevacuationoftheuterus.Evacuationwasconfirmedbyafinal,intraoperative,ultrasound.AllthreeultrasoundswereperformedbytheObhospitalistcaringforthepatient.
IfyouweretheObhospitalistinthiscase,howwouldyoucodeandbillyourservices?
ANSWER:
DiagnosisCodes(ICD-10):O02.1 MissedabortionO41.1220 Chorioamnionitis,secondtrimester,notapplicableorunspecifiedZ3A.18 18weeksgestationofpregnancyE&M Item Modifier99223-25 AdmissionH&P 25=E&MandProcedure CPT Item Modifier
SOGHNewsletter4.2016
76815 Ultrasound,OBLimited 26=ProfessionalComponent
59830 TreatmentofSepticAbortion,completedsurgically
76998-26 Ultrasound,Intraoperative 26=ProfessionalComponent
CodingBrief:Whilethediagnosesdocumentedinthepatient’schartisnotedasIUFDat18weekswithchorioamnionitis,whichiscommonvernacularforpracticingobstetricians,thisisnotconsistentwiththeICD-10billingdefinitions.Theencountermustbebilledunderadiagnosisofmissedabortionandchorioamnionitis.Thesearebothconsideredpregnancycomplications.
MissedabortioniscodedunderICD-10as002.1.Thebillingdefinitionformissedabortionis“earlyfetaldeath,beforecompletionof20weeksofgestation,withretentionofdeadfetus.”ChorioamnionitisiscodedasO41.1220anditsbillingdefinitionis“asingletongestationwithchorioamnionitisoccurringinthesecondtrimesterofpregnancy.”Thesecondtrimesterisdefinedas“betweenequaltoorgreaterthan14weeks,andlessthan28weekssincethefirstdayofthelastmenstrualperiod.”UnderICD-10,anypregnancycomplicationdiagnosiscodemustbeaccompaniedbyacodeintheZ3Afamily,whichspecifiesthegestationalage.InthiscaseZ3A.18denotes18weeksgestation.
Oncethediagnosiscodesarechosen,thenanappropriatelevelE&Mmustbeestablishedtobillthehistoryandphysical.AnyappropriateCPTcodesshouldalsobeaddedtobillprocedures.
ThedetailsofthiscaseeasilysupportusingtheE&Mcode99223.The99233diagnosiscodemaybebasedeitheronadirectdocumentationoftimespentonpatientcareoronthoroughdocumentationofacomprehensivehistory,physicalexam,anddecision-makingwithplanofcare.Thetimerequirementdocumentationforthe99223diagnosiscodeis“70minuteswerespentonthispatient'scare,ofwhichmorethan50%wasspentface-to-face,counselingheronthepregnancyprognosisandtreatmentoptions.”A25modifiermaybeusedinthiscasetoindicatethattheE&Mwasaseparatebutsignificantpartofthepatient'scarethatday.ThisisnecessarybecausemostCPTcodesincludepaymentforaroutinepreoperativeH&P.However,whenapatient'scareiscomplicatedbothanE&MvisitandaCPTprocedurecodecanbebilledonthesameday.
AlsoimportanttonoteisthattheD&CisnotcodedseparatelyinthiscasebutisincludedintheCPTcode59830,whichisthesurgicaltreatmentofsepticabortion.Ifthepatientdoes
SOGHNewsletter4.2016
notrequireaD&Ctoremovetheretainedproductsofconceptionoranyothersurgicalintervention,thiswouldprecludetheuseofthe59830CPTcode.
Finally,theCPTcodeforeachultrasoundcanbesubmittedandbilledseparately.Billinganultrasounddoesrequirethateachultrasoundbedocumentedinaseparatereport.Inaddition,imagesmustbesavedaspartofthepatient’smedicalrecord.Assumingtheuseofanultrasoundmachineownedbythehospital,youmaybillfortheprofessionalcomponentonlyandnotthetechnicalcomponentorfacilityfee.Lori-LynneA.Webb,CPC,CCS-P,CCP,CHDA,COBGCandICD10CM/PCSAmbassador/TrainerisanE&M,andProcedurebasedCoding,Compliance,DataChargeentryandHIPAAPrivacyspecialist,withover20yearsofexperience.Lori-Lynne’scodingspecialtyisOB/GYNoffice&HospitalistServices,MaternalFetalMedicine,OB/GYNOncology,Urology,andgeneralsurgicalcoding.Shecanbereachedviae-mailatwebbservices.lori@gmail.comoryoucanalsofindcurrentcodinginformationonherblogsite:http://lori-lynnescodingcoachblog.blogspot.com/.Dr.RenéeAllenservedasco-authorofthiscolumn.SheistheSOGHLiaisontotheACOGCommitteeonHealthEconomicsandCoding.ShecurrentlyworksasanOB/GYNHospitalistwithMednax/ObstetrixatEastsideMedicalCenterinSnellville,Georgia.
Questionsregardingthiscase?Contactusatcoding@societyofobgynhospitalists.org.
SOGH Newsletter 4.2016
discharge.Patientsmayreturntotheirownphysician,theMFMclinic(fortheperinatalpatients)orarereferredtoanotherphysicianorclinic.AspartoftheMFMteam,wehelptoadmitandstabilizehelicopterandambulancetransferstotheMFMservice.WeattendthedeliveryforthemajorityoftheMFMpatientsandperformdailyroundswiththeperinatologistonalltheirpatients.WealsoperformemergencygynsurgeryandsomescheduledD&Cfortheperinatologyservice.Wearepartoftheperinatologyteamandtheperinatolgistsprovideuswitharoundtheclockbackup.Ifweareoverextendedorifweencounteranysituationwe’renotcomfortablemanaging,theperinatologistprovidesassistance.WeoftenworkcloselywithMFMasmanyofourpatientshaveacuteand/orcomplicatedconditions.Asignificantbenefitofourcloseworkingrelationshipwiththeperinatologistsisbeingconstantlyeducatedoncurrentstandardsofpracticeforbothhighriskandnormalpregnancies.Itisanexcitingandintellectuallystimulatingpracticeenvironment.Sincetheprogram’sinception,therehasbeenlittleturnoverinemployees.Assuch,thehospitalistsareatightlyknitgroup.Wenotonlyworktogetherasateamofprofessionals,weworktogetherasfriends.Wesupporteachotherwhenpersonalcrisesarise;whichmakesforanincrediblycohesivegroup.Ourgroupisdedicatedtoprovidingthebestcarepossible.Werunaveryconscientiousservicethatisstaffedbyverytalentedphysicians.Wealsoshareacloserelationshipwiththeperinatologists,andhaveacooperativerelationship,notasubservientone.Ourgrouphaveelectedtobepaidhourlyandsoincentivecompensationdoesn'tapply.Ourfulltimeemployeesreceiveemployeebenefits,includingacontinuingeducationstipend.OurmalpracticecoverageispaidbyMednax.Sincewereceivehourlycompensation,wedonothavepaidtimeoff(PTO)orvacationpay.Ourprogramhasalreadyweatherednineyearssuccessfullyandcontinuestoevolve.Theprivatephysiciansutilizeourservicesregularlyforcoverage,OBEDevaluationsandsurgeryassists.Theyareverypleasedwiththeprogram,asarethenursingstaffandhospitaladministration.Wearecontinuouslysupportedandeducatedbytheperinatologistswithwhomwework,andhaveagreatrelationshipasahospitalistgroup.WehaveabusyL&DunitandMFM/antepartumservice;aswellasacceptingtransportsfromotherhospitals,sothejobhasafairamountofstress.Butattheendoftheshiftyoucanwalkawayknowingthatyou'vehelpedimprovethequalityofcareandsafetyofthepatientswe’veserved.
SOGHNewsletter4.2016
“CODETHIS!”(CaseoftheMonth)MissedAbortion,RetainedPOCwithChorioamnionitistreatedwithD&C
byLori-LynneA.Webb,CPCandReneeAllen,MD,FACOGFebruary25,2016CaseExcerpt(summaryandnarrativeofactualcase):
A29yoG1P0at183/7weekspresentedtothehospitalforevaluationofdecreasedfetalmovementat0830.Thepatientreportedpersistentmucusdischarge,moderateleakageoffluid,andmildcontractionsovertheprevious2-3days.Abedsideultrasoundconfirmedanintrauterinepregnancyat18weeksgestationwitholigohydramniosandnofetalcardiacactivity.Thepatientwas3-4cmdilatedandhertemperaturewas100.7degreesFahrenheit.Shewasinformedofthefindings,providedwithsupport,andadmittedtotheOBGYNhospitalistservicewithdiagnosisofintrauterinefetaldemiseat18weeks'gestationandchorioamnionitis.
Misoprostolaugmentationoflaborwasstartedandanepiduralwasplaced.Gentamycinandclindamycinwereordered(thepatienthadapenicillinallergy).Thepatientprogressedwellandspontaneouslydeliveredamalefetusofapproximately17weeksgestationalage.Herplacentaalsodeliveredspontaneously.However,examinationoftheplacentarevealedaraggedappearance,soasecondbedsideultrasoundwasperformedwhichdiagnosedretainedproductsofconception.AttemptsatmanualevacuationoftheuteruswereunsuccessfulandthepatientwastransferredtotheL&DORwhereadilation&curettagewasperformed.Auterinecrywasnotedatthecompletionoftheprocedurewhichsuggestedasuccessfulevacuationoftheuterus.Evacuationwasconfirmedbyafinal,intraoperative,ultrasound.AllthreeultrasoundswereperformedbytheObhospitalistcaringforthepatient.
IfyouweretheObhospitalistinthiscase,howwouldyoucodeandbillyourservices?
ANSWER:
DiagnosisCodes(ICD-10):O02.1 MissedabortionO41.1220 Chorioamnionitis,secondtrimester,notapplicableorunspecifiedZ3A.18 18weeksgestationofpregnancyE&M Item Modifier99223-25 AdmissionH&P 25=E&MandProcedure CPT Item Modifier
SOGHNewsletter4.2016
76815 Ultrasound,OBLimited 26=ProfessionalComponent
59830 TreatmentofSepticAbortion,completedsurgically
76998-26 Ultrasound,Intraoperative 26=ProfessionalComponent
CodingBrief:Whilethediagnosesdocumentedinthepatient’schartisnotedasIUFDat18weekswithchorioamnionitis,whichiscommonvernacularforpracticingobstetricians,thisisnotconsistentwiththeICD-10billingdefinitions.Theencountermustbebilledunderadiagnosisofmissedabortionandchorioamnionitis.Thesearebothconsideredpregnancycomplications.
MissedabortioniscodedunderICD-10as002.1.Thebillingdefinitionformissedabortionis“earlyfetaldeath,beforecompletionof20weeksofgestation,withretentionofdeadfetus.”ChorioamnionitisiscodedasO41.1220anditsbillingdefinitionis“asingletongestationwithchorioamnionitisoccurringinthesecondtrimesterofpregnancy.”Thesecondtrimesterisdefinedas“betweenequaltoorgreaterthan14weeks,andlessthan28weekssincethefirstdayofthelastmenstrualperiod.”UnderICD-10,anypregnancycomplicationdiagnosiscodemustbeaccompaniedbyacodeintheZ3Afamily,whichspecifiesthegestationalage.InthiscaseZ3A.18denotes18weeksgestation.
Oncethediagnosiscodesarechosen,thenanappropriatelevelE&Mmustbeestablishedtobillthehistoryandphysical.AnyappropriateCPTcodesshouldalsobeaddedtobillprocedures.
ThedetailsofthiscaseeasilysupportusingtheE&Mcode99223.The99233diagnosiscodemaybebasedeitheronadirectdocumentationoftimespentonpatientcareoronthoroughdocumentationofacomprehensivehistory,physicalexam,anddecision-makingwithplanofcare.Thetimerequirementdocumentationforthe99223diagnosiscodeis“70minuteswerespentonthispatient'scare,ofwhichmorethan50%wasspentface-to-face,counselingheronthepregnancyprognosisandtreatmentoptions.”A25modifiermaybeusedinthiscasetoindicatethattheE&Mwasaseparatebutsignificantpartofthepatient'scarethatday.ThisisnecessarybecausemostCPTcodesincludepaymentforaroutinepreoperativeH&P.However,whenapatient'scareiscomplicatedbothanE&MvisitandaCPTprocedurecodecanbebilledonthesameday.
AlsoimportanttonoteisthattheD&CisnotcodedseparatelyinthiscasebutisincludedintheCPTcode59830,whichisthesurgicaltreatmentofsepticabortion.Ifthepatientdoes
SOGHNewsletter4.2016
notrequireaD&Ctoremovetheretainedproductsofconceptionoranyothersurgicalintervention,thiswouldprecludetheuseofthe59830CPTcode.
Finally,theCPTcodeforeachultrasoundcanbesubmittedandbilledseparately.Billinganultrasounddoesrequirethateachultrasoundbedocumentedinaseparatereport.Inaddition,imagesmustbesavedaspartofthepatient’smedicalrecord.Assumingtheuseofanultrasoundmachineownedbythehospital,youmaybillfortheprofessionalcomponentonlyandnotthetechnicalcomponentorfacilityfee.Lori-LynneA.Webb,CPC,CCS-P,CCP,CHDA,COBGCandICD10CM/PCSAmbassador/TrainerisanE&M,andProcedurebasedCoding,Compliance,DataChargeentryandHIPAAPrivacyspecialist,withover20yearsofexperience.Lori-Lynne’scodingspecialtyisOB/GYNoffice&HospitalistServices,MaternalFetalMedicine,OB/GYNOncology,Urology,andgeneralsurgicalcoding.Shecanbereachedviae-mailatwebbservices.lori@gmail.comoryoucanalsofindcurrentcodinginformationonherblogsite:http://lori-lynnescodingcoachblog.blogspot.com/.Dr.RenéeAllenservedasco-authorofthiscolumn.SheistheSOGHLiaisontotheACOGCommitteeonHealthEconomicsandCoding.ShecurrentlyworksasanOB/GYNHospitalistwithMednax/ObstetrixatEastsideMedicalCenterinSnellville,Georgia.
Questionsregardingthiscase?Contactusatcoding@societyofobgynhospitalists.org.





























