Embed Size (px)
Citation preview

4/20/16
1
PupilsMore Than What Meets the Eye
Jordan Keith, OD, FAAOMinneapolis, MN
Maple Grove Fridley Maplewood
Greg Kraupa, OD
Jordan Keith , ODAshley Herde, OD
Tina McCarty, ODSteve Nauman, OD Mitch Albers, OD Brad Richter, OD
Objectives
§ Review anatomy
§ Normal pupils
§ Abnormal pupils
Fig 14-10
Light response
CN II = AFFERENT
CN III = EFFERENT
Parasympathetic pathway
1) Miosis
2) Accommodation
R L
Fig 14-9
Near response
4/20/16
2
Sympathetic pathway1) Mydriasis
2) Muller’s muscle
Fig 14-15
Normal
Normal Normal
Fig 14-10
Light responseCN II = AFFERENT
CN III = EFFERENT
R L
Anisocoria?
Afferent Disruption
4/20/16
3
Afferent Disruption Afferent Disruption
Fig 14-10
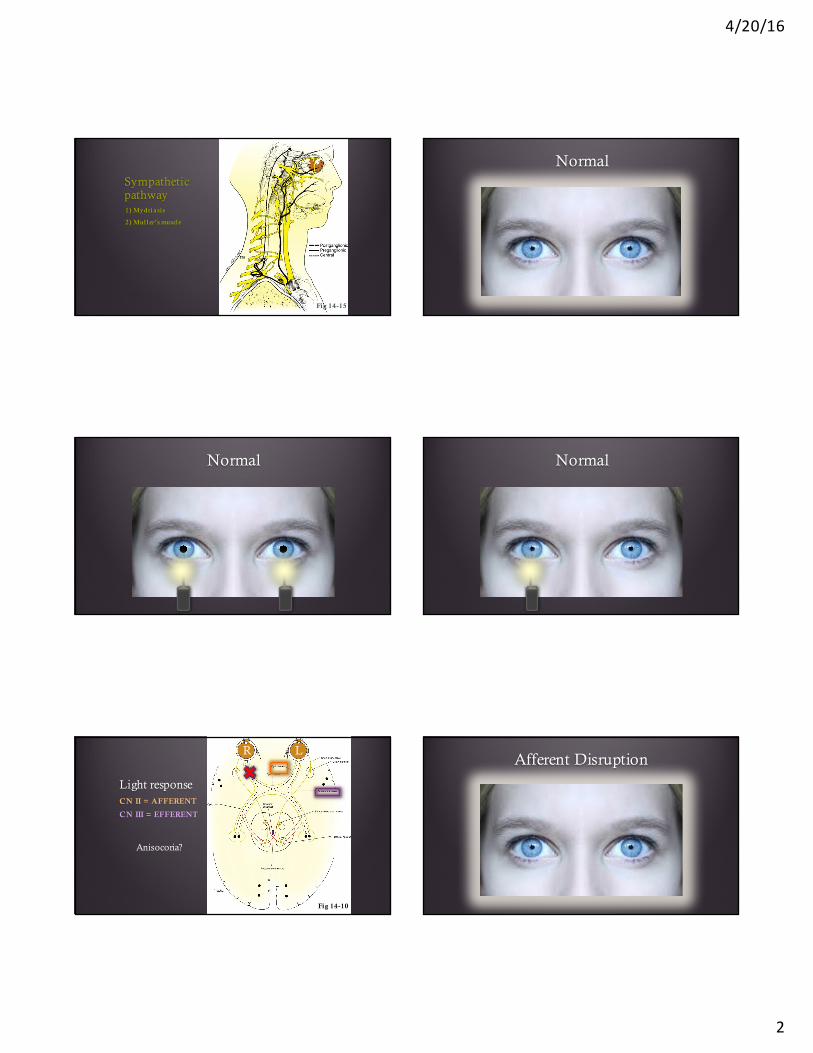
Light responseCN II = AFFERENT Disruption
1) Weaker direct response
2) (+) APD indicates unilateral or asymmetric retinal and/or prechiasmaloptic nerve disease
3) Anisocoria NEVER present
4) If disease equal and symmetric there will NOT be a (+) APD
R L Grading a (+) APD
APD Grade I: a weak init ial constrict ion and greater redilatat ion
Grade II: init ial stall and greater redilatat ion
Grade III: immediate pupillary dilatat ion
Grade IV: immediate pupillary dilatat ion following prolonged illumination of the good eye for 6 seconds
Grade V: immediate pupillary dilatat ion with no secondary constrict ion
Bell RA, et al. Arch Ophthalmol. 1993 Jul;111(7):938-42
Fig 14-10
Light responseCN II = AFFERENT
CN III = EFFERENT
R L
Anisocoria?
Efferent Disruption
4/20/16
4
Efferent Disruption Efferent Disruption
Fig 14-10
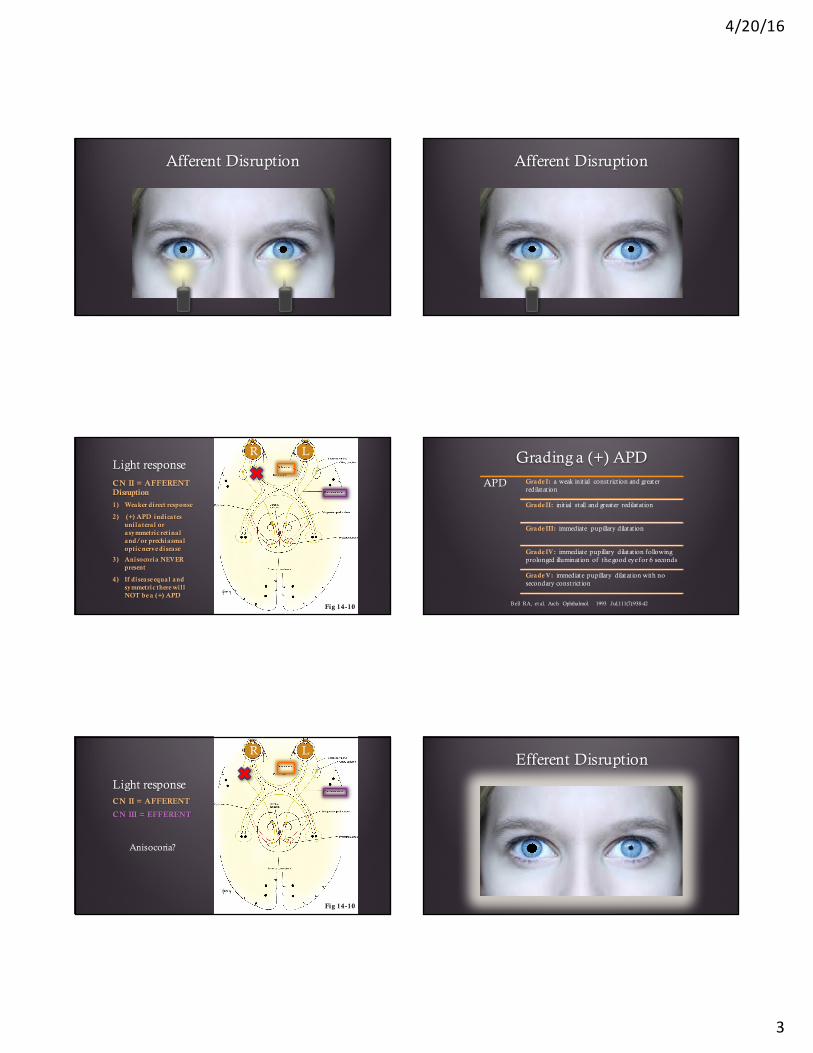
Light responseCN III = EFFERENT
Disruption
1) Poor direct response
2) Affected side stays dilated on swinging flashlight test
3) Anisocoria ALWAYS present
4) Accommodation can be affected
R L Clinical Presentations
Presentation
No Anisocoria
(+) APDAfferent disruption
Anisocoria
Pupil dilated (bigger difference in light)
Pupil miotic (bigger difference in night)
No Anisocoria(+) APD
Afferent disruption
Glaucoma
NAION/AAION
RD
Optic neuritis
Optic nerve compressive disease
Dense vitreous heme
Note: corneal scars , cataracts , amblyopia and maculopathy (unless severe)
do not cause an APD with a bright light source
Anisocoria
Pupil dilated (bigger difference in l ight)
Adie’s tonic pupil
Pupil involving CN III palsy
Pharmacologic
Trauma/mechanical
Pupil miotic (bigger difference in dark)
Horner’s syndrome
Uveitis
Argyll Robertson
4/20/16
5
35 year-old female / blurry vision OD 35 year-old female / blurry vision OD
35 year-old female / blurry vision OD
Fig 14-10
R L
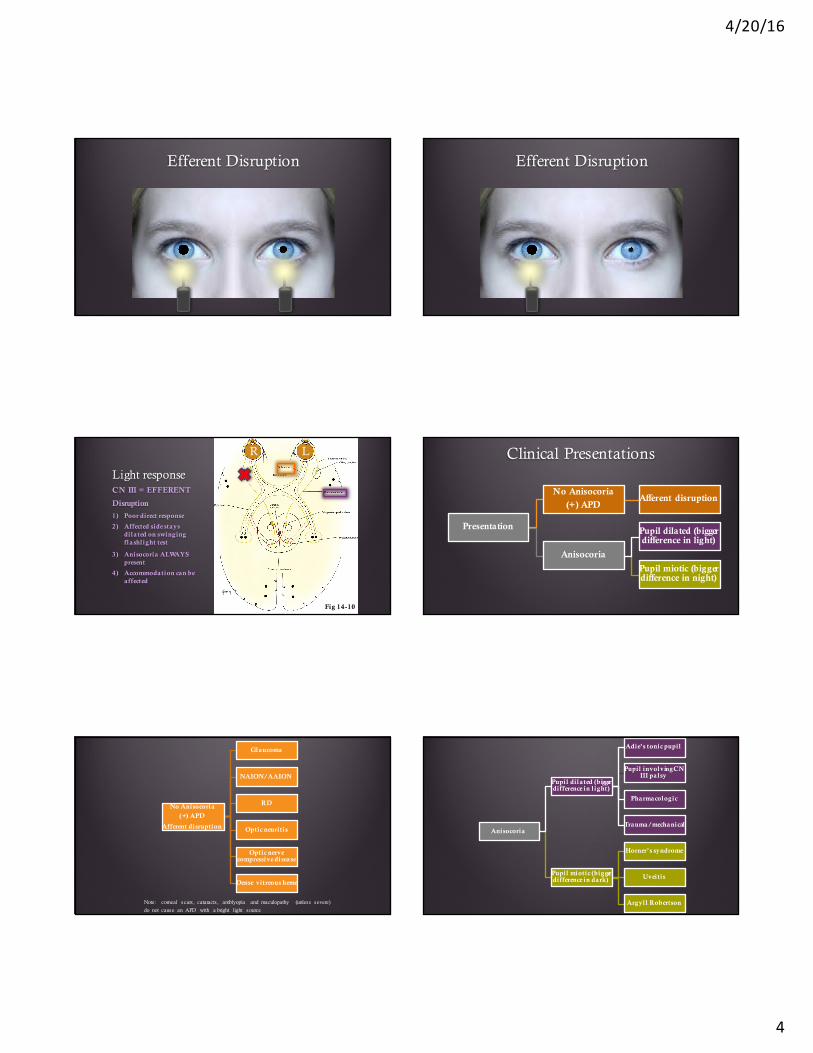
1) Acute dilated pupil (that constricts over time)
2) Female predominance (2.6:1)
3) Commonly young (20-40)
4) Typically unilateral (80%)
5) Minimal (if any) response to l ight
6) Vermiform movement with segmental paralysis
7) Poor accommodation
8) Damage to cil iary ganglion with unknown etiology
Adie’s Tonic Pupil
Adie’s Tonic Pupil
Video courtesy of Kyle Cheatham, OD, FAAO
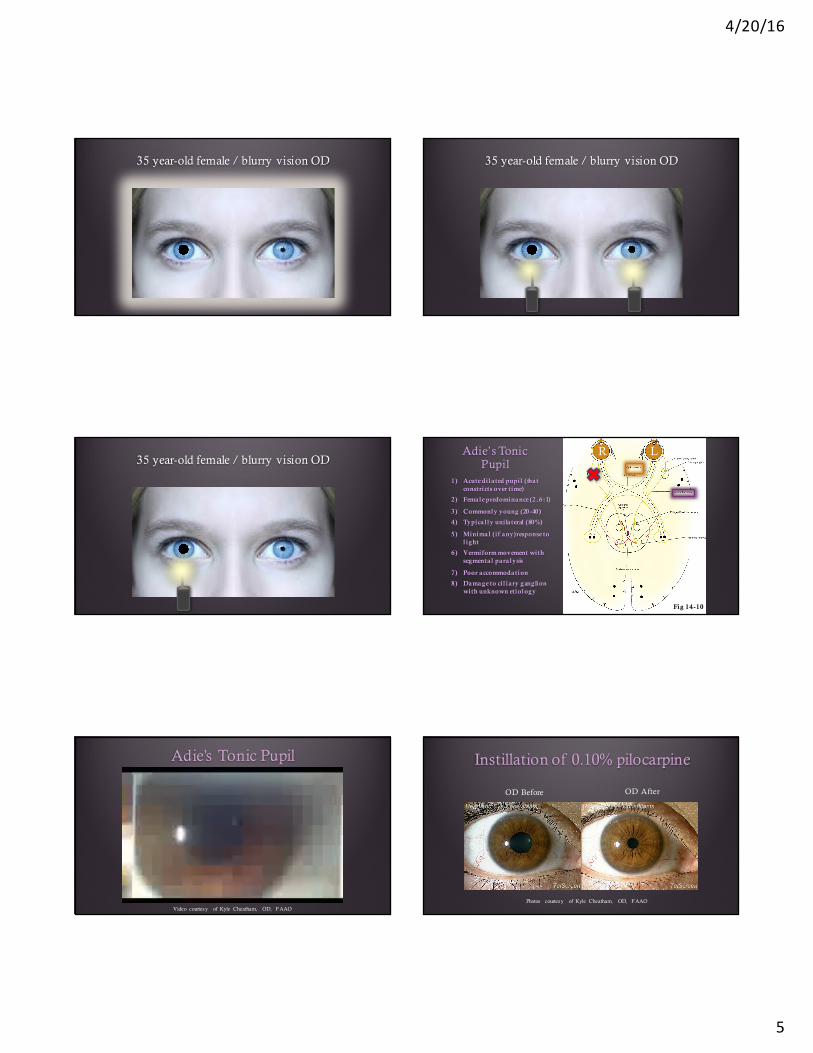
Instillation of 0.10% pilocarpine
OD Before OD After
Photos courtesy of Kyle Cheatham, OD, FAAO
4/20/16
6
Adie’s Tonic Pupil
§ Sphincter muscle has cholinergic hypersensitivity
§ Low concentrations of pilocarpine will cause constriction of an Adie’s tonic pupil and have minimal to no affect on a normal pupil
Bourgon P, et al. Am J Ophthalmol. 1978 Mar;85(3):373-7
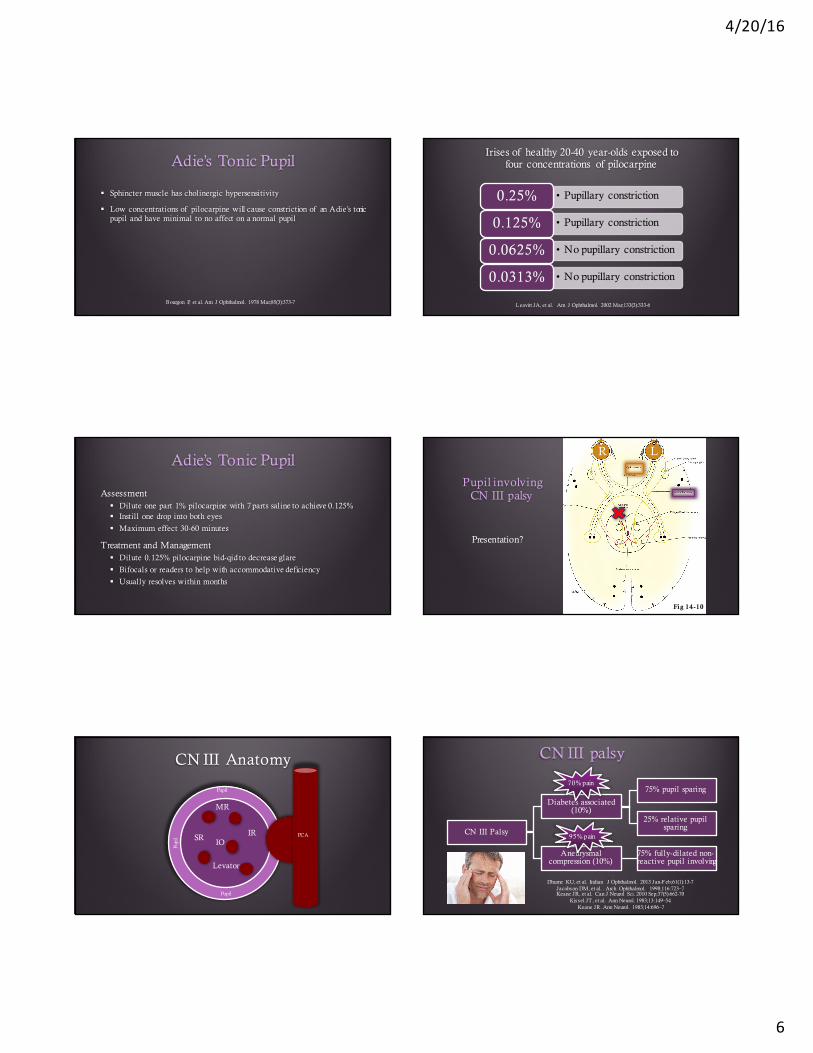
Irises of healthy 20-40 year-olds exposed to four concentrations of pilocarpine
• Pupillary constriction0.25%
• Pupillary constriction0.125%
• No pupillary constriction0.0625%
• No pupillary constriction0.0313%
Leavitt JA, et al. Am J Ophthalmol. 2002 Mar;133(3):333-6
Adie’s Tonic Pupil
Assessment§ Dilute one part 1% pilocarpine with 7 parts saline to achieve 0.125%§ Instill one drop into both eyes
§ Maximum effect 30-60 minutes
Treatment and Management§ Dilute 0.125% pilocarpine bid-qid to decrease glare
§ Bifocals or readers to help with accommodative deficiency
§ Usually resolves within months
Fig 14-10
Pupil involving CN III palsy
R L
Presentation?
CN III Anatomy
IR
MR
IOSR
Levator
Pupil
Pupi
l
Pupil
Pupil
PCA
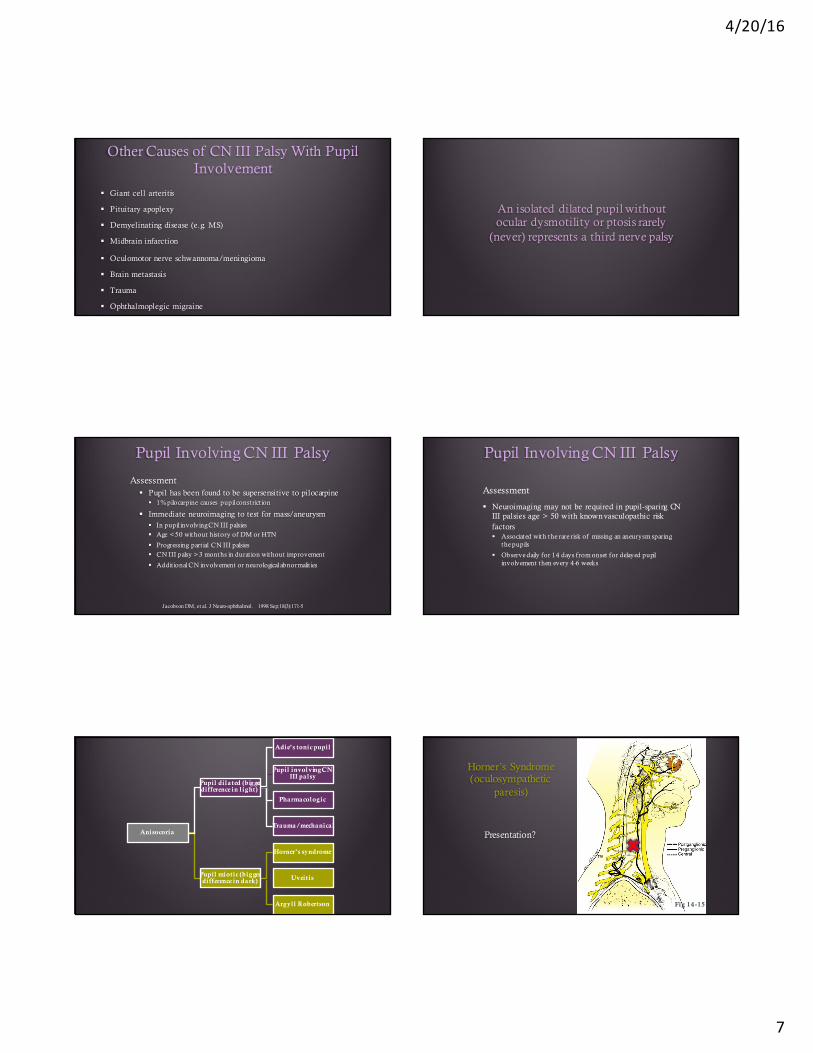
CN III palsy
CN III Palsy
Diabetes associated (10%)
75% pupil sparing
25% relative pupil sparing
Aneurysmal compression (10%)
75% fully-dilated non-reactive pupil involving
Dhume KU, et al. Indian J Ophthalmol. 2013 Jan-Feb;61(1):13-7Jacobson DM, et al. . Arch Ophthalmol. 1998;116:723–7Keane JR, et al. Can J Neurol Sci. 2010 Sep;37(5):662-70
Kissel JT, et al. Ann Neurol. 1983;13:149–54Keane JR. Ann Neurol. 1983;14:696–7
70% pain
95% pain
4/20/16
7
Other Causes of CN III Palsy With Pupil Involvement
§ Giant cell arteritis
§ Pituitary apoplexy
§ Demyelinating disease (e.g. MS)
§ Midbrain infarction
§ Oculomotor nerve schwannoma/meningioma
§ Brain metastasis
§ Trauma
§ Ophthalmoplegic migraine
An isolated dilated pupil without ocular dysmotility or ptosis rarely
(never) represents a third nerve palsy
Pupil Involving CN III Palsy
Assessment§ Pupil has been found to be supersensitive to pilocarpine
§ 1% pilocarpine causes pupil constrict ion
§ Immediate neuroimaging to test for mass/aneurysm§ In pupil involving CN III palsies § Age < 50 without history of DM or HTN
§ Progressing part ial CN III palsies § CN III palsy > 3 months in duration without improvement
§ Addit ional CN involvement or neurological abnormalit ies
Jacobson DM, et al. J Neuro-ophthalmol. 1998 Sep;18(3):171-5
Pupil Involving CN III Palsy
Assessment
§ Neuroimaging may not be required in pupil-sparing CN III palsies age > 50 with known vasculopathic risk factors § Associated with the rare risk of missing an aneurysm sparing
the pupils
§ Observe daily for 14 days from onset for delayed pupil involvement then every 4-6 weeks
Anisocoria
Pupil dilated (bigger difference in l ight)
Adie’s tonic pupil
Pupil involving CN III palsy
Pharmacologic
Trauma/mechanical
Pupil miotic (bigger difference in dark)
Horner’s syndrome
Uveitis
Argyll Robertson
Horner’s Syndrome(oculosympathetic
paresis)
Presentation?
Fig 14-15
4/20/16
8
Horner’s Syndrome Horner’s Syndrome
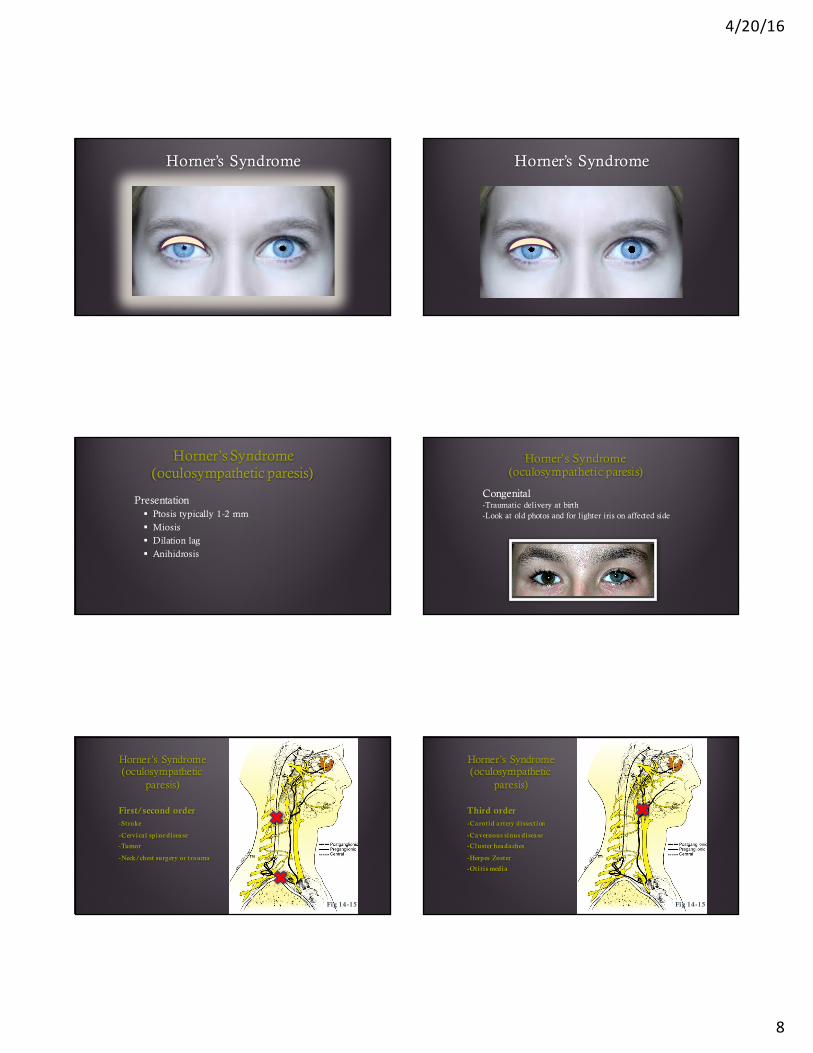
Horner’s Syndrome(oculosympathetic paresis)
Presentation§ Ptosis typically 1-2 mm
§ Miosis
§ Dilation lag
§ Anihidrosis
Horner’s Syndrome(oculosympathetic paresis)
Congenital-Traumatic delivery at birth-Look at old photos and for lighter iris on affected side
Horner’s Syndrome(oculosympathetic
paresis)
First/second order-Stroke
-Cervical spine disease
-Tumor
-Neck/chest surgery or trauma
Fig 14-15
Horner’s Syndrome(oculosympathetic
paresis)
Third order-Carotid artery dissection
-Cavernous sinus disease
-Cluster headaches
-Herpes Zoster
-Otitis media
Fig 14-15
4/20/16
9
Horner’s Syndrome(oculosympathetic paresis)
Assessment§ 4-10% cocaine/hydroxyamphetamine
§ Gold standard
§ 0.5% apraclonidine (Iopidine)§ Proposed substitute
§ Causes reversal of anisocoria
Koc F, et al. Br J Ophthalmol. Nov 2005; 89(11): 1442-44Brown SM, Aouchiche R, Freedman KA. Arch Ophthalmol 2003;121:1201–3
Bacal DA, et al. Arch Ophthalmol 2004;122:276–9Morales J, et al. Arch Ophthalmol 2000;118:951–4
Kawasaki A, et al. Klin Monbl Augenheilkd. May 2008;225(5):520-2
Horner’s Syndrome(oculosympathetic paresis)
Treatment and Managment
§ Old cases more likely benign § Monitor if signs point to congenital
§ New onset cases require more extensive diagnostic workup § CT scan of chest to evaluate lung apex
§ MRI/MRA head and neck § Carotid doppler if carotid artery dissect ion is suspected (neck pain)
§ 0.5% apraclonodine tid in affected eye can be used to raise ptosis
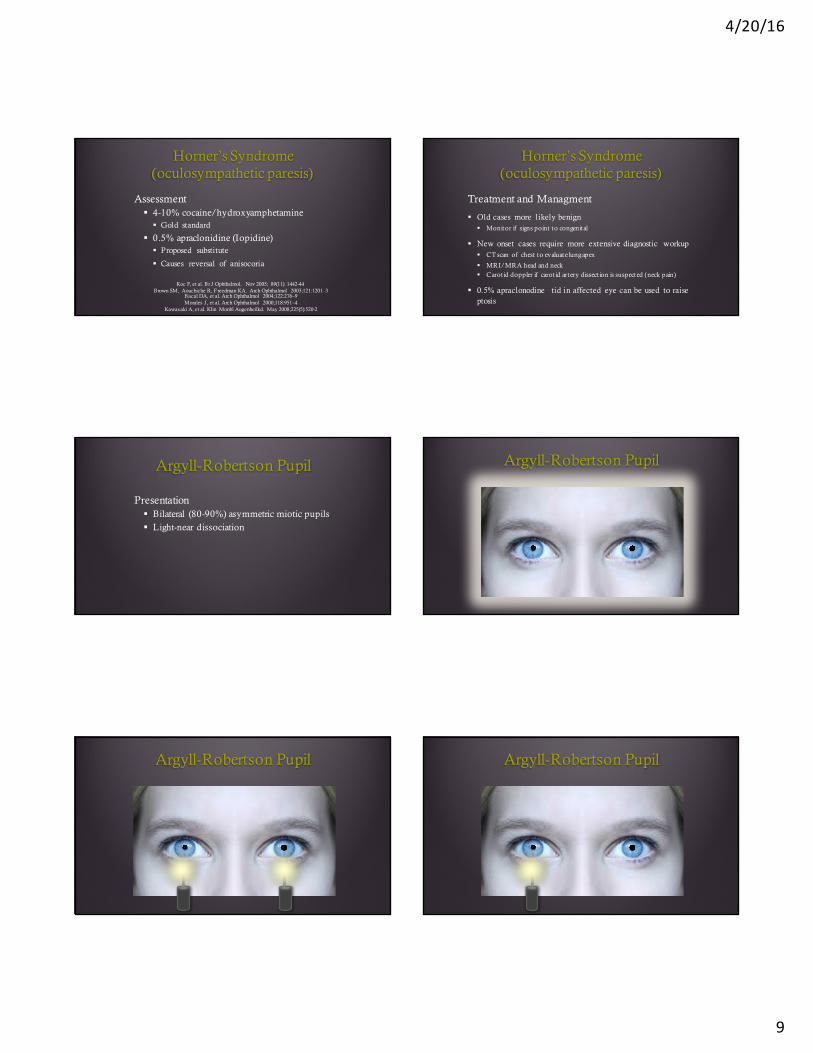
Argyll-Robertson Pupil
Presentation§ Bilateral (80-90%) asymmetric miotic pupils
§ Light-near dissociation
Argyll-Robertson Pupil
Argyll-Robertson Pupil Argyll-Robertson Pupil
4/20/16
10
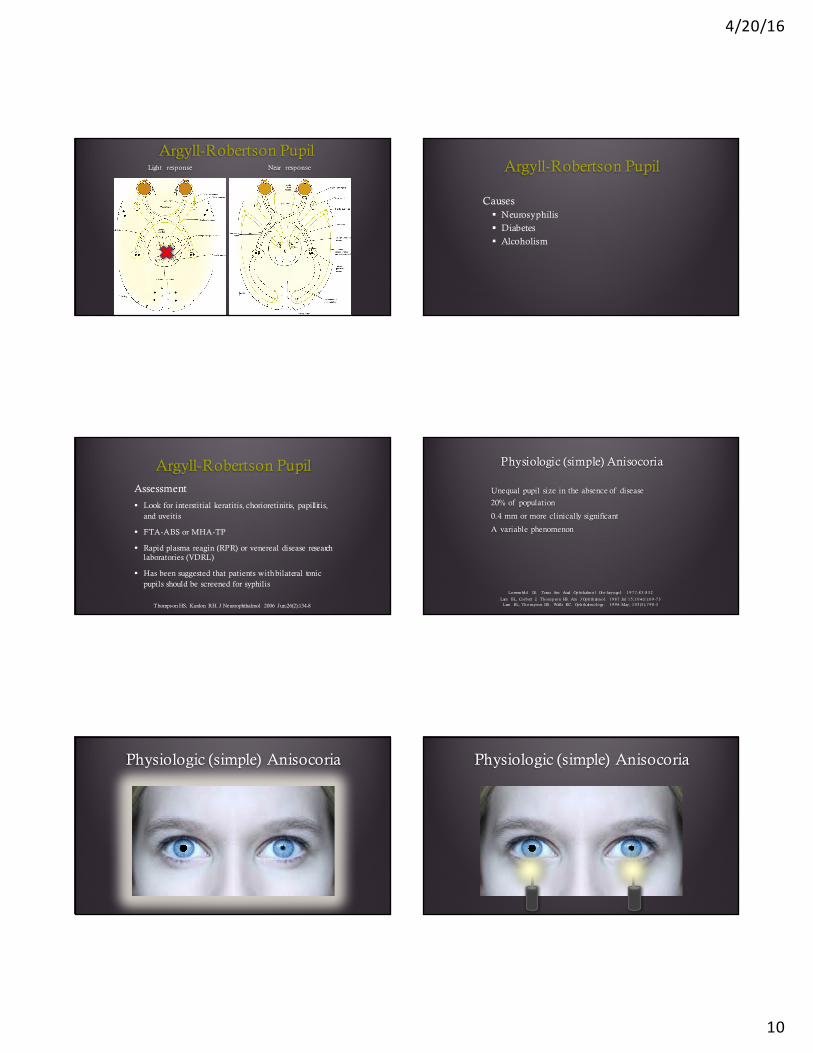
Argyll-Robertson PupilLight response Near response Argyll-Robertson Pupil
Causes§ Neurosyphilis
§ Diabetes
§ Alcoholism
Argyll-Robertson PupilAssessment
§ Look for interstitial keratitis, chorioretinitis, papillitis, and uveitis
§ FTA-ABS or MHA-TP
§ Rapid plasma reagin (RPR) or venereal disease research laboratories (VDRL)
§ Has been suggested that patients with bilateral tonic pupils should be screened for syphilis
Thompson HS, Kardon RH. J Neuroophthalmol 2006 Jun;26(2):134-8
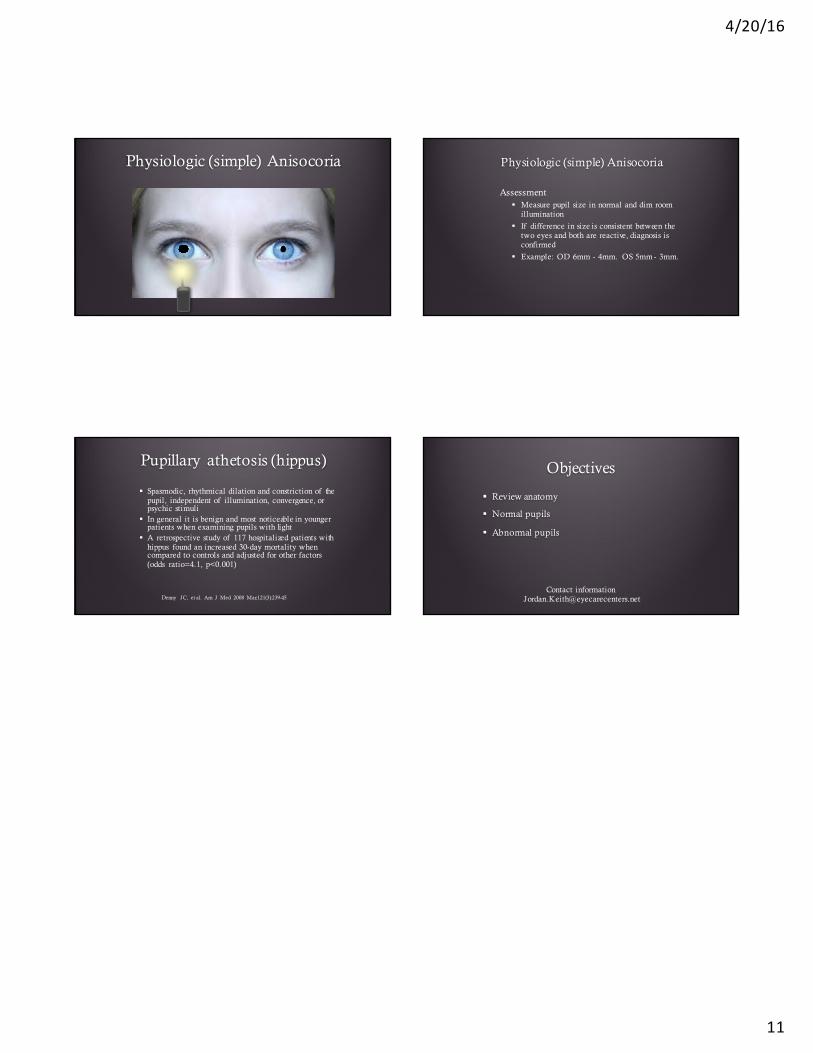
Physiologic (simple) Anisocoria
Unequal pupil size in the absence of disease
20% of population
0.4 mm or more clinically significant
A variable phenomenon
Loewenfeld IE. Trans Am Acad Op hthalm ol Oto -lary ngo l. 1 9 7 7 ;8 3 :8 3 2
Lam BL, Corb ett J, Thom p son HS. Am J Op hthalm ol. 1 9 8 7 Ju l 1 5 ;1 0 4 (1 ):6 9 -7 3Lam BL, Thom p son HS, Walls RC. Op hthalm ology . 1 9 9 6 May ; 1 0 3 (5 ):7 9 0 -3
Physiologic (simple) Anisocoria Physiologic (simple) Anisocoria
4/20/16
11
Physiologic (simple) Anisocoria Physiologic (simple) Anisocoria
Assessment § Measure pupil size in normal and dim room
illumination
§ If difference in size is consistent between the two eyes and both are reactive, diagnosis is confirmed
§ Example: OD 6mm - 4mm. OS 5mm - 3mm.
Pupillary athetosis (hippus)
§ Spasmodic, rhythmical dilation and constriction of the pupil, independent of illumination, convergence, or psychic stimuli
§ In general it is benign and most noticeable in younger patients when examining pupils with light
§ A retrospective study of 117 hospitalized patients with hippus found an increased 30-day mortality when compared to controls and adjusted for other factors (odds ratio=4.1, p<0.001)
Denny JC, et al. Am J Med 2008 Mar;121(3):239-45
Objectives
§ Review anatomy
§ Normal pupils
§ Abnormal pupils
Contact [email protected]





























