Embed Size (px)
Citation preview
725
Epidemiology• Centralnervoussystemmetastases
arecommon,affectingasmanyas25%ofpatientswithcancer.
• Mostcentralnervousmetastasesinvolvethebrain.
• Lessoften,thedura,leptomeninges,skullbase,orcranialnervesmaybeaffected.
• Theterms“neoplasticmeningitis”and“carcinomatousmeningitis”refertothedisseminationofcancercellswithintheleptomeningealspace.
• Themostfrequentprimarytumortypesthatgiverisetobrainmetastasesincludelungcancer,melanoma,breastcancer,andrenalcellcarcinoma.
Diagnosis• Brainmetastasesarebestdetected
withcontrast-enhancedmagneticresonanceimaging.
• Metastasesgenerallyappearasenhancing,well-circumscribedlesionswithorwithoutsurroundingvasogenicedema.
• Biopsyorresectionmaybeindicatedtoconfirmthediagnosis,particularlyinapatientwithasinglelesionandnocancerdiagnosisornoknownmetastaticdisease.
• Neoplasticmeningitisofteneludesearlydetection;meningealenhancementisonlyvisibleonmagneticresonanceimaginginabout50%ofcases,andcerebralspinalfluidcytologymaybenegativeinitiallyin40%to50%ofcases.
Prognosis• Themostimportantfactorsthat
predictlongersurvivalofpatients
withbrainmetastasesincludeage<65years,goodperformancestatus,controloftheprimarycancer,andlackofextracranialmetastases.
Treatment• Themoststandardtreatmentfor
brainmetastasesiswhole-brainradiotherapy(WBRT).
• Patientswithagoodprognosisandalimitednumberofbrainmetastasesmaybenefitfrommoreaggressivetherapysuchassurgery(especiallyforasinglebrainmetastasis)orstereotacticradiosurgery(SRS),withorwithoutadjuvantWBRT.
• AfterWBRTalone,thefollowingobservationshavebeenmade:○Atleast60%ofsymptomatic
patientsimprovesignificantly.○Mediansurvivaltimeistypically3
to6months.○Onethirdtoonehalfofpatients
dieofbrainmetastases,andtheremainderdieofsystemicdisease.
○Approximatelyonequarterofbrainmetastaseshaveacompleteresponseandonethirdhaveapartialresponse.
○One-yearactuariallocalcontrolprobabilitymaybeaslowas14%orashighas71%.
• AmongpatientswithnewlydiagnosedbrainmetastasesselectedforsurgeryorSRSwithorwithoutWBRT,thefollowingobservationshavebeenmade:○Mediansurvivaltimeis
approximately9to11months.○One-yearactuariallocalcontrol
ratesareapproximately:
○35%forsurgeryalone.○85%forsurgeryandadjuvant
WBRT.○75%to90%forSRSwithor
withoutadjuvantWBRT.○Theincreasedlocalcontrol
achievablewithsurgeryplusWBRTorwithSRSmayonlybemeaningfulinpatientslikelytoliveatleast6to12monthsfromthestandpointoftheirextracranialdisease.
○Systemictherapyisnotgenerallyusedasaprimarytreatmentforbrainmetastases,butithassomeefficacyonitsown.
○Thereisincreasinginterestincombiningsystemicagentswithradiationtherapy.
• Intrathecalchemotherapyplaysamajorroleinthemanagementofneoplasticmeningitis,aloneorincombinationwithradiotherapy.
• Craniospinalradiotherapycausessignificantacutetoxicityandlong-lastingmyelosuppression.
• Accordingly,neoplasticmeningitismaybemanagedwithuseofintrathecalchemotherapycombinedwithmorelimitedradiotherapy.
• Examplesoflimitedradiotherapyincludethefollowing:○Lumbarfieldsforgrossdiseasein
thecaudaequina○Skullbasefieldsforcranialnerve
involvement○WBRTinpatientswith
hydrocephalusorsignificantheadachestemmingfromdiffusebrainleptomeningealinvolvement
S U M M A R Y O F K E Y P O I N T S
50 Brain Metastases and Neoplastic MeningitisPennyK.Sneed,NorbertKased,andJamesL.Rubenstein

PartII:ProblemsCommontoCancerandItsTherapy726
but individual tumor cells may pass through to lodge in the brain. Tumor emboli may also break off from lung metastases or primary lung cancers to travel to the brain via the arterial circulation. Cells from pelvic or abdominal cancers may gain access to the posterior fossa or leptomeninges through Batson’s vertebral venous plexus without passing through the lungs.5 Intracranial spread may also occur via direct extension from bone or dural metastases or perineural extension along cranial nerves. The distribution of metastases is roughly proportional to the relative blood flow to different regions; approximately 80% of brain metastases are located in the cerebral hemispheres, 10% to 15% in the cerebellum, and 1% to 5% in the brain stem.5,6 Posterior fossa metastases appear to arise disproportion-ately from pelvic or abdominal primary tumors.5
Most brain metastases are very well circumscribed. Although extensive associated edema may be present, the tumor cells do not tend to infiltrate into surrounding brain tissue, in contrast to primary malignant brain tumors. Most brain metastases are solid, but they may appear to be heterogeneously enhancing or cystic because of necrosis, keratin deposits in squamous cell carcinoma, or mucin secre-tion from adenocarcinomas. Brain metastases may be hemorrhagic, particularly from melanoma, renal cell carcinoma, choriocarcinoma, and, less frequently, bronchogenic carcinoma.9
Single brain metastases are more common than multiple metasta-ses in patients with renal cell, gastrointestinal, or unknown primary cancers.6 In the era of computed tomographic (CT) imaging, it appeared that about 50% of patients with brain metastasis had a single brain lesion.5 More recently, in the era of MRI, this number has decreased to approximately 25% to 35%, with improved sensitiv-ity for detecting smaller metastases.10 Of note, the term “solitary brain metastasis” implies that a single brain metastasis is the only known site of metastatic disease.
Clinical PresentationThe possibility of brain metastases should be suspected in any patient with cancer who experiences new neurologic signs or symptoms. Two thirds of patients with cancer found to have brain metastases at autopsy had experienced neurologic symptoms from the metastases,11 and only 10% of a series of 729 patients diagnosed between 1973 and 1993 by CT or MRI were asymptomatic.6 The most common presenting symptoms are headache (24% to 53%), focal weakness (16% to 40%), altered mental status (24% to 31%), seizures (15% to 16%), and ataxia (9% to 20%).6,12 Symptoms may worsen gradu-ally from a growing tumor and associated edema. Less often, acute neurologic symptoms may occur as a result of hemorrhage of a brain metastasis.
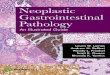
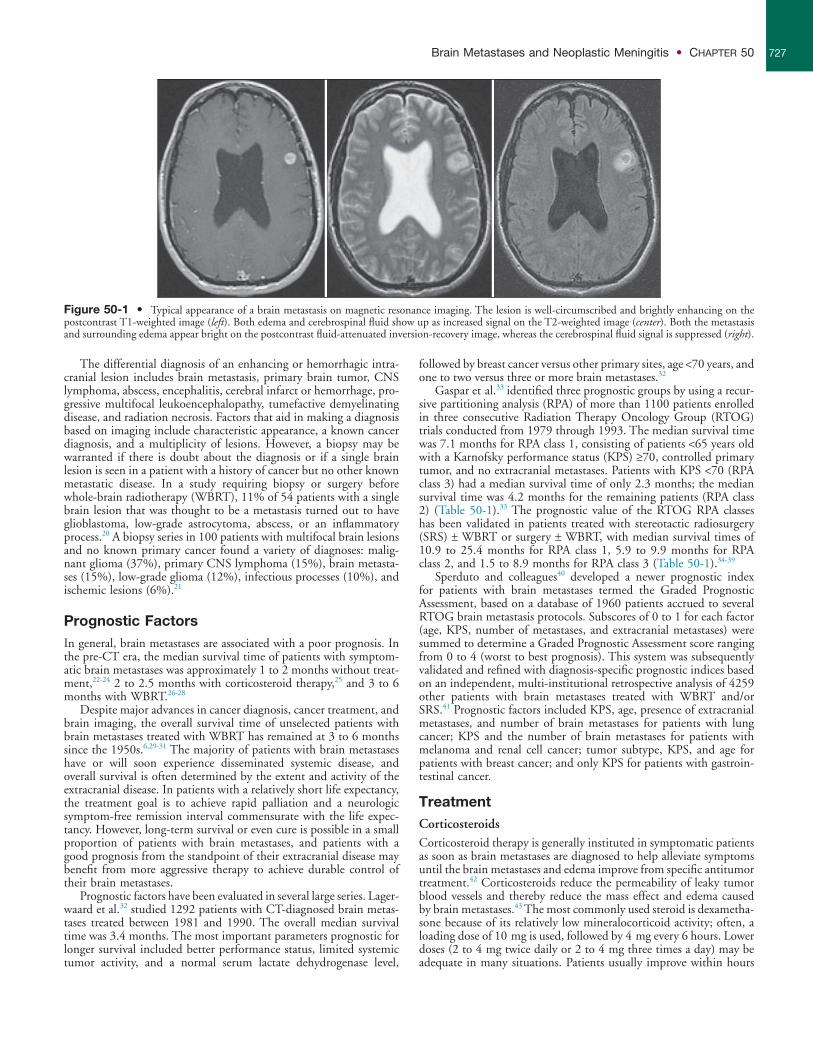
DiagnosisIt is widely accepted that MRI is the best diagnostic test to detect brain metastases. Standard imaging includes T2-weighted and pre- and postgadolinium-enhanced T1-weighted sequences; a postcon-trast fluid-attenuated inversion-recovery sequence is also helpful in visualizing small metastases near cerebrospinal fluid (CSF) spaces (Fig. 50-1). Gadolinium-enhanced MRI is much more sensitive than nonenhanced MRI or contrast-enhanced CT imaging.13,14 In one study, 17 of 55 patients (31%) with a single metastasis based on contrast-enhanced CT were found to have multiple metastases on contrast-enhanced MRI.15 The sensitivity of MRI is improved by using “triple-dose” gadolinium (0.3 mmol/kg instead of 0.1 mmol/kg gadoteridol)16 and by using contiguous axial 3-mm slices and coronal three-dimensional spoiled gradient echo recovery volume imaging so that small lesions are not missed between slices. Func-tional imaging techniques such as positron emission tomography, magnetic resonance spectroscopy, and perfusion and diffusion MRI may aid in distinguishing metastatic lesions from necrosis, primary brain tumor, or nonmalignant processes.17-19
INTRODUCTIONCentral nervous system (CNS) metastases result from the intracranial spread of tumor cells that originate outside of the CNS. Most CNS metastases involve the brain parenchyma, dura, or leptomenin-ges; less commonly, the skull base, cranial nerves, or dural sinuses are involved. This chapter deals with brain parenchymal and lepto-meningeal metastases, also known as neoplastic or carcinomatous meningitis.
BRAIN METASTASES
EpidemiologyBrain metastases appear to be more common than primary malignant brain tumors, although the exact incidence is unknown. In a Memo-rial Sloan Kettering Cancer Center autopsy series, 24% of patients with cancer had CNS metastases and 15% had brain metastases.1 One population-based study in the Netherlands found that brain metas-tases developed in 8.5% of 2724 patients with melanoma, lung, breast, colorectal, or renal cell carcinoma. The 5-year cumulative incidence of brain metastases was 7.4% in patients with melanoma and 16.3%, 9.8%, 5.0%, and 1.2% for patients with lung, renal cell, breast, or colorectal carcinoma, respectively.2 Similarly, the population-based incidence of brain metastasis among patients with cancer within the Metropolitan Detroit Cancer Surveillance System diag-nosed between 1973 and 2001 was 6.9% for patients with melanoma and 19.9%, 6.5%, 5.1%, and 1.8% for patients with lung, renal cell, breast, and colorectal cancer, respectively.3 The incidence of brain metastases appears to be increasing as a result of improvements in cancer management that are leading to longer survival time, as well as increased lesion detection with contrast-enhanced, high-resolution magnetic resonance imaging (MRI),4 although Schouten et al.2 found no evidence of increasing brain metastasis incidence during 1986 through 1995.
The most common primary tumors responsible for brain metas-tases include lung cancer (constituting approximately 40% to 50% of cases), breast cancer (15%), melanoma (10%), and unknown primary (5% to 10%), followed by renal cell carcinoma, colorectal cancer, gynecologic cancers, and other miscellaneous tumors.5,6 Brain metastases may arise from any primary cancer, but certain tumors such as melanoma and carcinomas of the lung, kidney, and breast have a tendency to spread to the CNS. On the contrary, some tumors rarely metastasize to the brain, such as prostate, oro-pharyngeal, and skin carcinomas. In children, the most common solid malignancies responsible for brain metastases include sarcomas, neuroblastomas, and germ cell tumors.7
Cancer may spread to the brain at various points in the course of disease. Synchronous brain metastases, found within 1 month of the primary cancer diagnosis, occur in up to one third of patients.2 More commonly, brain metastases are discovered after the diagnosis of cancer, often after other systemic metastases have developed, at a median of less than 1 year after lung cancer diagnosis and 2 to 3 years after diagnosis of melanoma, breast cancer, gynecologic cancer, or renal cell carcinoma.6 Overall, the median time from primary diag-nosis to diagnosis of brain metastases is 12 months.6
PathophysiologyBrain metastases arise primarily from arterial hematogenous spread to the brain. Tumor cells tend to become trapped where blood vessels decrease in caliber at the gray/white matter junction and distal-most vasculature (the border or “watershed” zones between arterial territo-ries).8 Metastatic cells then adhere to the endothelial cells, penetrate into the brain parenchyma, and proliferate. Larger aggregates of tumor cells that gain access to the venous circulation are filtered out in lung capillaries before entering the systemic arterial circulation,
BrainMetastasesandNeoplasticMeningitis • CHAPTER50 727
Figure 50-1 • Typical appearance of a brain metastasis on magnetic resonance imaging. The lesion is well-circumscribed and brightly enhancing on the postcontrast T1-weighted image (left). Both edema and cerebrospinal fluid show up as increased signal on the T2-weighted image (center). Both the metastasis and surrounding edema appear bright on the postcontrast fluid-attenuated inversion-recovery image, whereas the cerebrospinal fluid signal is suppressed (right).
The differential diagnosis of an enhancing or hemorrhagic intra-cranial lesion includes brain metastasis, primary brain tumor, CNS lymphoma, abscess, encephalitis, cerebral infarct or hemorrhage, pro-gressive multifocal leukoencephalopathy, tumefactive demyelinating disease, and radiation necrosis. Factors that aid in making a diagnosis based on imaging include characteristic appearance, a known cancer diagnosis, and a multiplicity of lesions. However, a biopsy may be warranted if there is doubt about the diagnosis or if a single brain lesion is seen in a patient with a history of cancer but no other known metastatic disease. In a study requiring biopsy or surgery before whole-brain radiotherapy (WBRT), 11% of 54 patients with a single brain lesion that was thought to be a metastasis turned out to have glioblastoma, low-grade astrocytoma, abscess, or an inflammatory process.20 A biopsy series in 100 patients with multifocal brain lesions and no known primary cancer found a variety of diagnoses: malig-nant glioma (37%), primary CNS lymphoma (15%), brain metasta-ses (15%), low-grade glioma (12%), infectious processes (10%), and ischemic lesions (6%).21
Prognostic FactorsIn general, brain metastases are associated with a poor prognosis. In the pre-CT era, the median survival time of patients with symptom-atic brain metastases was approximately 1 to 2 months without treat-ment,22-24 2 to 2.5 months with corticosteroid therapy,25 and 3 to 6 months with WBRT.26-28
Despite major advances in cancer diagnosis, cancer treatment, and brain imaging, the overall survival time of unselected patients with brain metastases treated with WBRT has remained at 3 to 6 months since the 1950s.6,29-31 The majority of patients with brain metastases have or will soon experience disseminated systemic disease, and overall survival is often determined by the extent and activity of the extracranial disease. In patients with a relatively short life expectancy, the treatment goal is to achieve rapid palliation and a neurologic symptom-free remission interval commensurate with the life expec-tancy. However, long-term survival or even cure is possible in a small proportion of patients with brain metastases, and patients with a good prognosis from the standpoint of their extracranial disease may benefit from more aggressive therapy to achieve durable control of their brain metastases.
Prognostic factors have been evaluated in several large series. Lager-waard et al.32 studied 1292 patients with CT-diagnosed brain metas-tases treated between 1981 and 1990. The overall median survival time was 3.4 months. The most important parameters prognostic for longer survival included better performance status, limited systemic tumor activity, and a normal serum lactate dehydrogenase level,
followed by breast cancer versus other primary sites, age <70 years, and one to two versus three or more brain metastases.32
Gaspar et al.33 identified three prognostic groups by using a recur-sive partitioning analysis (RPA) of more than 1100 patients enrolled in three consecutive Radiation Therapy Oncology Group (RTOG) trials conducted from 1979 through 1993. The median survival time was 7.1 months for RPA class 1, consisting of patients <65 years old with a Karnofsky performance status (KPS) ≥70, controlled primary tumor, and no extracranial metastases. Patients with KPS <70 (RPA class 3) had a median survival time of only 2.3 months; the median survival time was 4.2 months for the remaining patients (RPA class 2) (Table 50-1).33 The prognostic value of the RTOG RPA classes has been validated in patients treated with stereotactic radiosurgery (SRS) ± WBRT or surgery ± WBRT, with median survival times of 10.9 to 25.4 months for RPA class 1, 5.9 to 9.9 months for RPA class 2, and 1.5 to 8.9 months for RPA class 3 (Table 50-1).34-39
Sperduto and colleagues40 developed a newer prognostic index for patients with brain metastases termed the Graded Prognostic Assessment, based on a database of 1960 patients accrued to several RTOG brain metastasis protocols. Subscores of 0 to 1 for each factor (age, KPS, number of metastases, and extracranial metastases) were summed to determine a Graded Prognostic Assessment score ranging from 0 to 4 (worst to best prognosis). This system was subsequently validated and refined with diagnosis-specific prognostic indices based on an independent, multi-institutional retrospective analysis of 4259 other patients with brain metastases treated with WBRT and/or SRS.41 Prognostic factors included KPS, age, presence of extracranial metastases, and number of brain metastases for patients with lung cancer; KPS and the number of brain metastases for patients with melanoma and renal cell cancer; tumor subtype, KPS, and age for patients with breast cancer; and only KPS for patients with gastroin-testinal cancer.
TreatmentCorticosteroidsCorticosteroid therapy is generally instituted in symptomatic patients as soon as brain metastases are diagnosed to help alleviate symptoms until the brain metastases and edema improve from specific antitumor treatment.42 Corticosteroids reduce the permeability of leaky tumor blood vessels and thereby reduce the mass effect and edema caused by brain metastases.43 The most commonly used steroid is dexametha-sone because of its relatively low mineralocorticoid activity; often, a loading dose of 10 mg is used, followed by 4 mg every 6 hours. Lower doses (2 to 4 mg twice daily or 2 to 4 mg three times a day) may be adequate in many situations. Patients usually improve within hours
PartII:ProblemsCommontoCancerandItsTherapy728
the 1950s and 1960s. In these early studies, significant symptomatic improvement was noted in about 60% of patients, and the median survival time ranged from about 3 to 6 months with WBRT26-28 compared with an expected median survival time of 1 to 2 months without treatment.22-24
SELECTEDRANDOMIZEDTRIALSOFWBRTALONEMultiple large phase 3 randomized trials of WBRT have been con-ducted by the RTOG since 1970 (Table 50-2). The first two trials compared various WBRT fractionation schemes in more than 1800 patients treated from 1971 through 1976 and gathered a wealth of data.29,48 Complete or partial response of specific neurologic symp-toms was observed in 60% to 90% of symptomatic patients; 47% to 52% of patients improved to a higher neurologic function class; the median duration of improvement was 10 to 12 weeks; and 75% to 80% of patients’ remaining survival time was spent in an improved or stable neurologic state. The overall median survival times were 4.1 months in the first study and 3.4 months in the second study, and
after the first dose, attaining maximal benefit after approximately 3 to 7 days. After patients become asymptomatic or reach maximal benefit, the dose should be gradually tapered and either discontinued or else maintained at the lowest dose level needed to manage symp-toms. If headaches recur or neurologic symptoms worsen during the course of the taper, the dose should be increased as needed and then the taper should proceed more gradually. Occasionally patients experi-ence steroid-withdrawal symptoms of depression, fatigue, nausea, or poor appetite, necessitating reinstitution of low-dose dexamethasone or hydrocortisone and a slow taper in the low-dose range.
Steroids have numerous adverse effects, particularly with long-term usage. Common short-term adverse effects include insomnia, increased appetite, fluid retention, mood changes, acne, and exacer-bation of diabetes, and some of the serious long-term adverse effects include significant weight gain, steroid myopathy, immunosuppres-sion, and aseptic necrosis of the femoral heads. Of note, steroid myopathy can cause fairly profound weakness in large proximal muscles, making it difficult for patients to get up and walk; this dysfunction may be mistaken as a sign of progression of CNS metas-tases and as an indication to continue or increase the use of steroids when it is actually a complication of steroid therapy.
Anticonvulsant AgentsSeizures are very unlikely to occur from infratentorial metastases, but they may be triggered by supratentorial metastases. About 15% of patients with brain metastases present with seizures when they first are seen by a clinician, and 30% to 40% experience seizures at some point in their disease course.44 An anticonvulsant agent such as phe-nytoin, carbamazepine, or levetiracetam should be prescribed for any patient with brain metastases who experiences a seizure. Prophylactic anticonvulsant agents are not recommended; prospective and retro-spective studies and metaanalyses have failed to demonstrate a benefit for prophylactic anticonvulsant agents in patients with brain metastases.43-46 In addition, anticonvulsant agents may have adverse side effects or cause serious allergic reactions such as Stevens-Johnson syndrome. Importantly, certain anticonvulsant agents such as phe-nytoin can reduce the efficacy of corticosteroids and can activate the cytochrome P450 enzyme system.47 This latter property can affect patients undergoing chemotherapy by altering the metabolism of some chemotherapeutic agents, thus requiring chemotherapy dose adjustment.
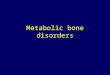
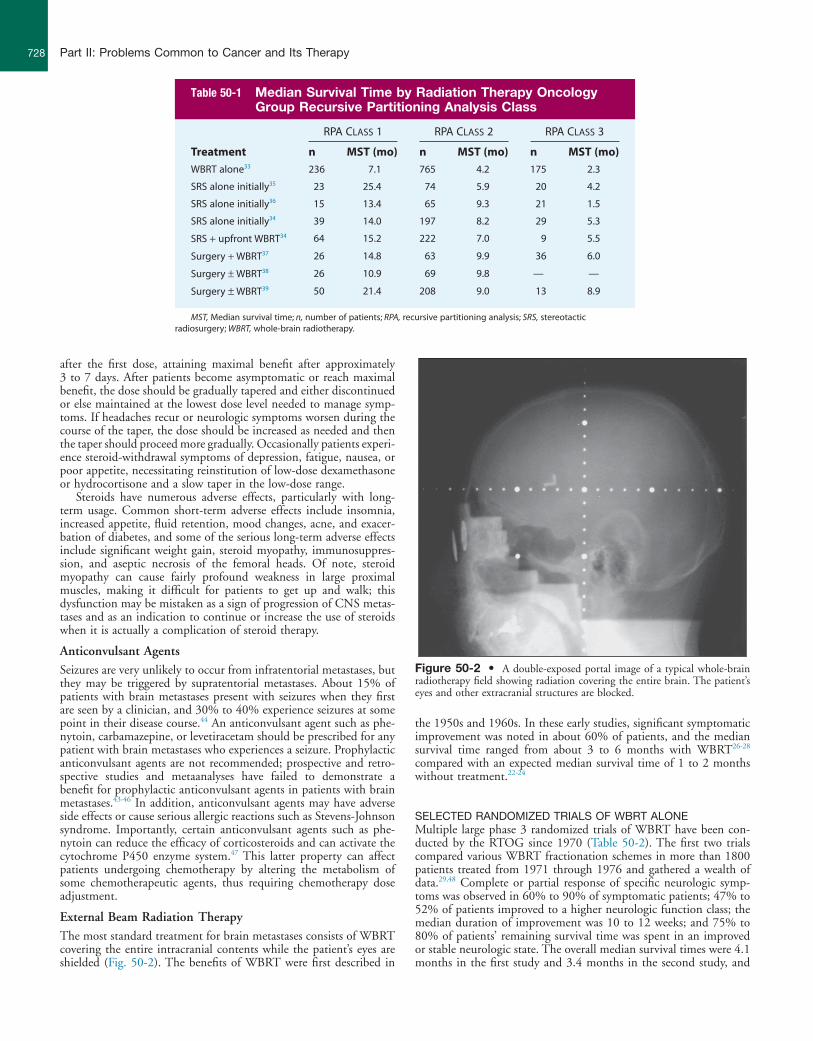
External Beam Radiation TherapyThe most standard treatment for brain metastases consists of WBRT covering the entire intracranial contents while the patient’s eyes are shielded (Fig. 50-2). The benefits of WBRT were first described in
Figure 50-2 • A double-exposed portal image of a typical whole-brain radiotherapy field showing radiation covering the entire brain. The patient’s eyes and other extracranial structures are blocked.
Table 50-1 Median Survival Time by Radiation Therapy Oncology Group Recursive Partitioning Analysis Class
RPA CLASS 1 RPA CLASS 2 RPA CLASS 3
Treatment n MST (mo) n MST (mo) n MST (mo)
WBRT alone33 236 7.1 765 4.2 175 2.3
SRS alone initially35 23 25.4 74 5.9 20 4.2
SRS alone initially36 15 13.4 65 9.3 21 1.5
SRS alone initially34 39 14.0 197 8.2 29 5.3
SRS + upfront WBRT34 64 15.2 222 7.0 9 5.5
Surgery + WBRT37 26 14.8 63 9.9 36 6.0
Surgery ± WBRT38 26 10.9 69 9.8 — —
Surgery ± WBRT39 50 21.4 208 9.0 13 8.9
MST, Median survival time; n, number of patients; RPA, recursive partitioning analysis; SRS, stereotactic radiosurgery; WBRT, whole-brain radiotherapy.
BrainMetastasesandNeoplasticMeningitis • CHAPTER50 729
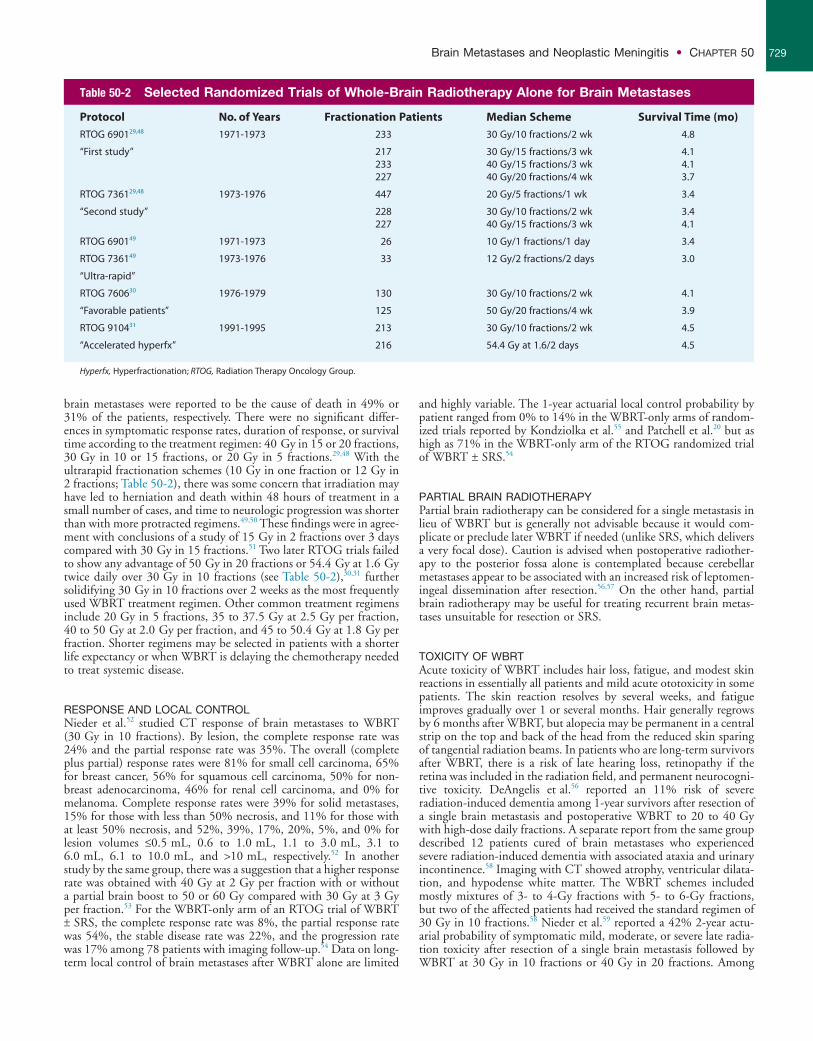
Table 50-2 Selected Randomized Trials of Whole-Brain Radiotherapy Alone for Brain Metastases
Protocol No. of Years Fractionation Patients Median Scheme Survival Time (mo)
RTOG 690129,48 1971-1973 233 30 Gy/10 fractions/2 wk 4.8
“First study” 217 30 Gy/15 fractions/3 wk 4.1233 40 Gy/15 fractions/3 wk 4.1227 40 Gy/20 fractions/4 wk 3.7
RTOG 736129,48 1973-1976 447 20 Gy/5 fractions/1 wk 3.4
“Second study” 228 30 Gy/10 fractions/2 wk 3.4227 40 Gy/15 fractions/3 wk 4.1
RTOG 690149 1971-1973 26 10 Gy/1 fractions/1 day 3.4
RTOG 736149 1973-1976 33 12 Gy/2 fractions/2 days 3.0
“Ultra-rapid”
RTOG 760630 1976-1979 130 30 Gy/10 fractions/2 wk 4.1
“Favorable patients” 125 50 Gy/20 fractions/4 wk 3.9
RTOG 910431 1991-1995 213 30 Gy/10 fractions/2 wk 4.5
“Accelerated hyperfx” 216 54.4 Gy at 1.6/2 days 4.5
Hyperfx, Hyperfractionation; RTOG, Radiation Therapy Oncology Group.
brain metastases were reported to be the cause of death in 49% or 31% of the patients, respectively. There were no significant differ-ences in symptomatic response rates, duration of response, or survival time according to the treatment regimen: 40 Gy in 15 or 20 fractions, 30 Gy in 10 or 15 fractions, or 20 Gy in 5 fractions.29,48 With the ultrarapid fractionation schemes (10 Gy in one fraction or 12 Gy in 2 fractions; Table 50-2), there was some concern that irradiation may have led to herniation and death within 48 hours of treatment in a small number of cases, and time to neurologic progression was shorter than with more protracted regimens.49,50 These findings were in agree-ment with conclusions of a study of 15 Gy in 2 fractions over 3 days compared with 30 Gy in 15 fractions.51 Two later RTOG trials failed to show any advantage of 50 Gy in 20 fractions or 54.4 Gy at 1.6 Gy twice daily over 30 Gy in 10 fractions (see Table 50-2),30,31 further solidifying 30 Gy in 10 fractions over 2 weeks as the most frequently used WBRT treatment regimen. Other common treatment regimens include 20 Gy in 5 fractions, 35 to 37.5 Gy at 2.5 Gy per fraction, 40 to 50 Gy at 2.0 Gy per fraction, and 45 to 50.4 Gy at 1.8 Gy per fraction. Shorter regimens may be selected in patients with a shorter life expectancy or when WBRT is delaying the chemotherapy needed to treat systemic disease.
RESPONSEANDLOCALCONTROLNieder et al.52 studied CT response of brain metastases to WBRT (30 Gy in 10 fractions). By lesion, the complete response rate was 24% and the partial response rate was 35%. The overall (complete plus partial) response rates were 81% for small cell carcinoma, 65% for breast cancer, 56% for squamous cell carcinoma, 50% for non-breast adenocarcinoma, 46% for renal cell carcinoma, and 0% for melanoma. Complete response rates were 39% for solid metastases, 15% for those with less than 50% necrosis, and 11% for those with at least 50% necrosis, and 52%, 39%, 17%, 20%, 5%, and 0% for lesion volumes ≤0.5 mL, 0.6 to 1.0 mL, 1.1 to 3.0 mL, 3.1 to 6.0 mL, 6.1 to 10.0 mL, and >10 mL, respectively.52 In another study by the same group, there was a suggestion that a higher response rate was obtained with 40 Gy at 2 Gy per fraction with or without a partial brain boost to 50 or 60 Gy compared with 30 Gy at 3 Gy per fraction.53 For the WBRT-only arm of an RTOG trial of WBRT ± SRS, the complete response rate was 8%, the partial response rate was 54%, the stable disease rate was 22%, and the progression rate was 17% among 78 patients with imaging follow-up.54 Data on long-term local control of brain metastases after WBRT alone are limited
and highly variable. The 1-year actuarial local control probability by patient ranged from 0% to 14% in the WBRT-only arms of random-ized trials reported by Kondziolka et al.55 and Patchell et al.20 but as high as 71% in the WBRT-only arm of the RTOG randomized trial of WBRT ± SRS.54
PARTIALBRAINRADIOTHERAPYPartial brain radiotherapy can be considered for a single metastasis in lieu of WBRT but is generally not advisable because it would com-plicate or preclude later WBRT if needed (unlike SRS, which delivers a very focal dose). Caution is advised when postoperative radiother-apy to the posterior fossa alone is contemplated because cerebellar metastases appear to be associated with an increased risk of leptomen-ingeal dissemination after resection.56,57 On the other hand, partial brain radiotherapy may be useful for treating recurrent brain metas-tases unsuitable for resection or SRS.
TOXICITYOFWBRTAcute toxicity of WBRT includes hair loss, fatigue, and modest skin reactions in essentially all patients and mild acute ototoxicity in some patients. The skin reaction resolves by several weeks, and fatigue improves gradually over 1 or several months. Hair generally regrows by 6 months after WBRT, but alopecia may be permanent in a central strip on the top and back of the head from the reduced skin sparing of tangential radiation beams. In patients who are long-term survivors after WBRT, there is a risk of late hearing loss, retinopathy if the retina was included in the radiation field, and permanent neurocogni-tive toxicity. DeAngelis et al.56 reported an 11% risk of severe radiation-induced dementia among 1-year survivors after resection of a single brain metastasis and postoperative WBRT to 20 to 40 Gy with high-dose daily fractions. A separate report from the same group described 12 patients cured of brain metastases who experienced severe radiation-induced dementia with associated ataxia and urinary incontinence.58 Imaging with CT showed atrophy, ventricular dilata-tion, and hypodense white matter. The WBRT schemes included mostly mixtures of 3- to 4-Gy fractions with 5- to 6-Gy fractions, but two of the affected patients had received the standard regimen of 30 Gy in 10 fractions.58 Nieder et al.59 reported a 42% 2-year actu-arial probability of symptomatic mild, moderate, or severe late radia-tion toxicity after resection of a single brain metastasis followed by WBRT at 30 Gy in 10 fractions or 40 Gy in 20 fractions. Among

PartII:ProblemsCommontoCancerandItsTherapy730
enrolled in the surgery arm of the trial had longer functionally inde-pendent survival (median, 7.5 vs. 3.5 months for surgery + WBRT vs. WBRT alone; P = .06) and longer survival time (median, 10 vs. 6 months; P = .04). The survival benefit was seen only in patients without active extracranial disease, in whom the median survival time was 12 months versus 7 months for WBRT alone (P = .02); the median survival time was 5 months for patients with active extracranial disease regardless of the treatment arm. Age >60 years was also confirmed as an unfavorable prognostic factor (P = .003; hazard ratio = 2.74).65
A third trial failed to show a benefit for surgery in addition to WBRT (30 Gy in 10 fractions over 2 weeks) (Table 50-3).66 The median survival times were 5.6 months among 41 patients randomly assigned to surgery + WBRT versus 6.3 months for 43 patients ran-domly assigned to WBRT alone (10 of whom had surgery before or after WBRT). No difference in the duration of functional indepen-dence was found between the two treatment arms.66 However, overall, these studies and previous nonrandomized experience67-69 support the use of surgery in patients with good performance status and a single brain metastasis.
RANDOMIZEDTRIALOFSURGERYWITHORWITHOUTWBRTPostoperative WBRT may help prevent recurrence at the resection cavity and prevent appearance of new intracranial metastases by treat-ing microscopic metastases elsewhere in the brain and any tumor cells disseminated at the time of surgery. Patchell et al.70 followed up on retrospective studies suggesting a benefit for WBRT after resection of a brain metastasis by performing a randomized trial (Table 50-3). Ninety-five adults were randomly assigned to observation versus post-operative WBRT with 50.4 Gy in 28 fractions after complete resec-tion of a single brain metastasis. The observation arm had a significantly increased risk of local failure (46% for observation vs. 10% for WBRT), distant brain failure (37% vs. 14%), and any brain failure (70% vs. 18%), along with a shorter time to local failure (median, 6.2 vs. >12 months; P < .001; hazard ratio 6.03) and a shorter time to any brain failure (median, 6.0 vs. >16.1 months; P < .001; hazard ratio 4.94). Patients randomized to observation were more likely to die of neurologic causes (44% vs. 14%; P = .003) but, interestingly, had similar duration of functional independence (median, 8.0 months for observation vs. 8.5 months for WBRT; P = 0.61) and a similar survival time (median, 9.9 vs. 11.0 months; P = 0.39).70
RANDOMIZEDTRIALOFSURGERYORSRSWITHORWITHOUTWBRTA phase 3 European Organization for Research and Treatment of Cancer study reported on the outcomes of 359 patients with one to three brain metastases treated with either SRS (n = 199) or surgery (n = 160) who were randomly assigned to WBRT (30 Gy in 10 frac-tions) versus observation (Table 50-3).71 When observation was com-pared with WBRT, no significant differences were found in median time to the World Health Organization performance status >2 (10.0 vs. 9.5 months), median overall survival (10.7 vs. 10.9 months), or the percentage of patients alive and functionally independent at 2 years (22.3% vs. 22.7%, respectively). The addition of WBRT to surgery reduced the 2-year relapse rate both at local sites (59% to 27%; P < .001) and at distant sites (42% to 23%; P = .008). In the SRS group, WBRT also significantly decreased local and distant brain failure (local, 31% to 19%, P = .04, and distant, 48% to 33%, P = .023). At 2 years, 22.3% of observation patients versus 22.6% of WBRT patients were alive and functionally independent. Patients enrolled in the observation arm required more salvage therapy (51% of patients) than did patients enrolled in the WBRT arm (16% of patients). Finally, death from intracranial progression was also more frequent in the observation arm relative to the WBRT arm (44% vs. 28%).71
112 patients on the WBRT-only arm of an RTOG randomized trial, Andrews et al.54 reported one case of grade 3 and one case of grade 4 late CNS toxicity and one case of grade 3 late ototoxicity.
Two prospective, randomized controlled studies assessed neuro-cognitive function in patients with brain metastases treated with SRS ± WBRT. Aoyama and colleagues60 assessed neurocognitive function through the Mini-Mental State Examination (MMSE). After treat-ment, 53% of the SRS + WBRT group versus 50% of the SRS-alone group had improvement >3 points. However, the average time until MMSE deterioration was 16.5 months in the WBRT + SRS group versus 7.6 months in the SRS-alone group (P = .05); this finding was attributed to the higher rates of brain tumor recurrence in the latter group. The authors concluded that brain tumor control is the most important factor for stabilizing neurocognitive function but that “the long-term adverse effects of WBRT on neurocognitive function might not be negligible.”60
In 2009, a group from the MD Anderson Cancer Center com-pared neurocognitive function as their primary end point in a pro-spective, randomized trial of SRS + WBRT versus SRS alone, using the Hopkins Verbal Learning Test–Revised (HVLT-R) total recall at 4 months.61 The authors found that patients treated with SRS + WBRT were significantly more likely to show a decline in learning and memory function at 4 months, and they recommended initial treatment with SRS alone in conjunction with close follow-up to better preserve learning and memory.
Finally, Sun et al.62 compared neurocognitive function in a group of patients with stage III non–small cell lung cancer (SCLC) who completed definitive therapy without progression and were randomly assigned to prophylactic WBRT or observation. The authors used the MMSE, the Activities of Daily Living Scale, and the HVLT to assess neurocognitive function. At 1 year, there were no significant differences in the MMSE or Activities of Daily Living Scale scores, but the WBRT group had a greater decline in both immediate recall (P = .03) and delayed recall (P = .008) on the HVLT.
SurgerySurgery has important roles to play in certain subsets of patients, including confirming the diagnosis when needed, relieving mass effect from a large, symptomatic lesion, improving the likelihood of durable local control for a single metastasis, and salvaging a metastasis that failed to respond to prior therapy. Surgical resection may also be useful for lesions with considerable peritumoral edema despite use of steroids or for lesions causing refractory seizures, even if the lesion is sufficiently small that SRS would be a therapeutic option.63 Resection of brain metastases has become safer with advances in neuroimaging and neurosurgery such as image guidance, preoperative and intraop-erative functional mapping, and intraoperative ultrasound and MRI.64
RANDOMIZEDTRIALSOFWBRTWITHORWITHOUTSURGERYThree prospective randomized trials have been performed to evaluate the addition of surgery to WBRT (Table 50-3). Patchell et al.20 reported on 48 patients with a single brain metastasis who were randomly assigned to biopsy and WBRT versus resection and WBRT with 36 Gy in 12 fractions. Patients who underwent resection had significantly improved local control (80% for resection and WBRT vs. 48% for biopsy and WBRT; P < .02), duration of functional independence (median, 38 weeks vs. 8 weeks; P < .005), and survival (median, 40 weeks vs. 15 weeks; P < .01). Factors associated with longer survival included younger age, no extracranial disease, surgical resection, and a longer interval from primary diagnosis to brain metastasis diagnosis.20
A trial performed in the Netherlands randomly assigned 63 evalu-able patients with a single brain metastasis to surgery + WBRT versus WBRT alone (40 Gy at 2 Gy twice daily) (Table 50-3).65 Patients
BrainMetastasesandNeoplasticMeningitis • CHAPTER50 731
tion of all brain metastases was significantly associated with pro-longed survival.75
TOXICITYOFSURGERYThe morbidity and mortality associated with surgical resection of brain metastases have decreased over the years as techniques have improved. Lang and Sawaya64 estimated the 30-day mortality rate to be about 4% to 5% after surgery for brain metastasis (essentially identical to the 30-day mortality rate in patients managed with WBRT alone). The most common types of postoperative morbidity include wound infection, hemorrhage, meningitis, pneumonia, deep venous thrombosis, and pulmonary embolism, which occur in about 10% to 15% of patients.64,76 One surgical series reported that 0 to 13% of patients worsened neurologically, 65% to 84% improved, and 11% to 22% remained stable after resection of single or multiple brain metastasis.72 Paek et al.74 reported outcomes in patients who underwent resection of one (n = 191) or multiple (n = 17) newly diagnosed (n = 149) or recurrent (n = 59) brain metastases at a single institution using modern neurosurgical techniques. The 30-day mor-tality rate was 1.9%, with two deaths from hemorrhage in the resec-tion cavity, one death from a pulmonary embolism, and one death from bowel perforation with sepsis. The median hospital stay was 3
SURGERYFORMULTIPLEMETASTASESSurgical resection may also be used successfully to manage the cases of selected patients with more than one brain metastasis. Bindal et al.72 reported a median survival time of 14 months among 26 patients with multiple brain metastases who underwent resection of all of their brain lesions in a single operation, identical to the survival time of matched patients who had resection of a single metastasis. The complication rate was 9% per craniotomy, the 30-day mortality rate was 4%, and only 6% of symptomatic patients worsened, whereas 83% improved and 11% remained stable.72 A different group describ-ing results of surgery and WBRT noted significantly poorer survival among 18 patients with multiple brain metastases compared with 28 patients with a single metastasis, but apparently only one patient with multiple metastases had gross total resection of all (two) metastases, and this patient survived 46 months.73 In a later series, Paek et al.74 reported a median survival time of 8 months after surgery for approx-imately 103 patients with a newly diagnosed single metastasis versus 11 months after surgery for 46 patients with newly diagnosed mul-tiple brain metastases (only nine of whom had multiple brain metas-tases resected); most patients underwent postoperative WBRT. A German group reported on 177 patients with brain metastases who were treated with surgical resection, including 57 with more than one brain metastasis.75 On univariate but not multivariate analysis, resec-
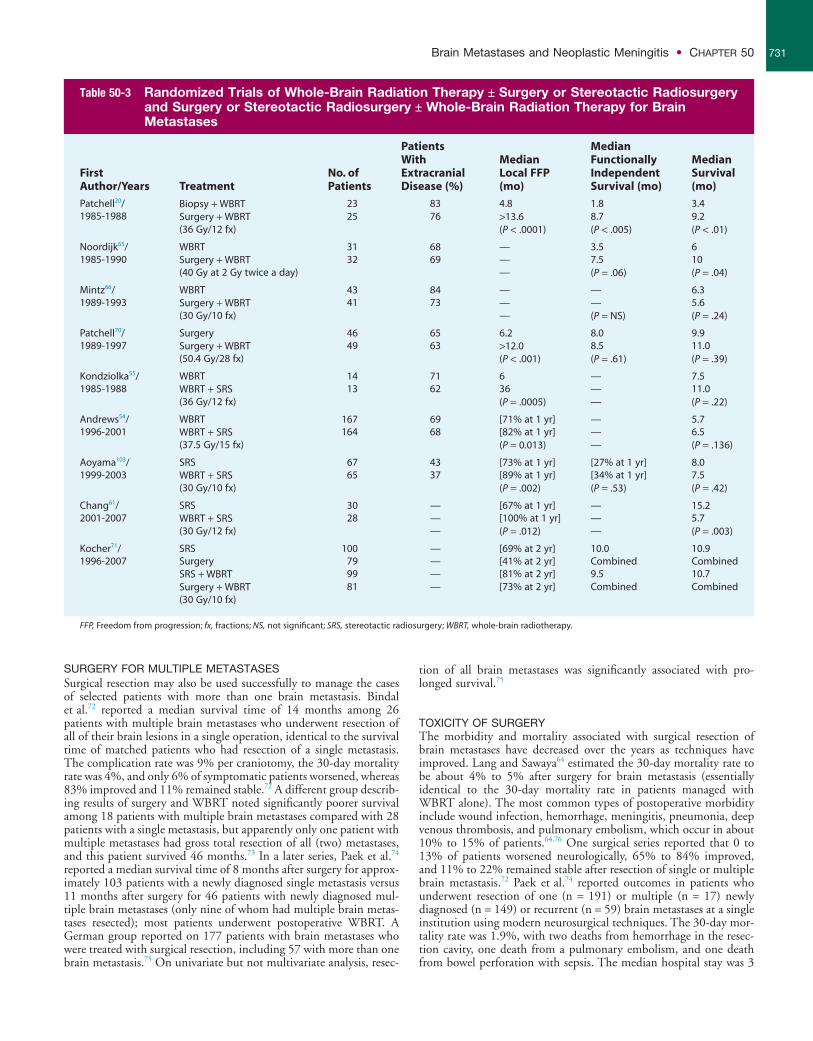
Table 50-3 Randomized Trials of Whole-Brain Radiation Therapy ± Surgery or Stereotactic Radiosurgery and Surgery or Stereotactic Radiosurgery ± Whole-Brain Radiation Therapy for Brain Metastases
First Author/Years Treatment
No. of Patients
Patients With Extracranial Disease (%)
Median Local FFP (mo)
Median Functionally Independent Survival (mo)
Median Survival (mo)
Patchell20/1985-1988
Biopsy + WBRT 23 83 4.8 1.8 3.4Surgery + WBRT 25 76 >13.6 8.7 9.2(36 Gy/12 fx) (P < .0001) (P < .005) (P < .01)
Noordijk65/1985-1990
WBRT 31 68 — 3.5 6Surgery + WBRT 32 69 — 7.5 10(40 Gy at 2 Gy twice a day) — (P = .06) (P = .04)
Mintz66/1989-1993
WBRT 43 84 — — 6.3Surgery + WBRT 41 73 — — 5.6(30 Gy/10 fx) — (P = NS) (P = .24)
Patchell70/1989-1997
Surgery 46 65 6.2 8.0 9.9Surgery + WBRT 49 63 >12.0 8.5 11.0(50.4 Gy/28 fx) (P < .001) (P = .61) (P = .39)
Kondziolka55/1985-1988
WBRT 14 71 6 — 7.5WBRT + SRS 13 62 36 — 11.0(36 Gy/12 fx) (P = .0005) — (P = .22)
Andrews54/1996-2001
WBRT 167 69 [71% at 1 yr] — 5.7WBRT + SRS 164 68 [82% at 1 yr] — 6.5(37.5 Gy/15 fx) (P = 0.013) — (P = .136)
Aoyama103/1999-2003
SRS 67 43 [73% at 1 yr] [27% at 1 yr] 8.0WBRT + SRS 65 37 [89% at 1 yr] [34% at 1 yr] 7.5(30 Gy/10 fx) (P = .002) (P = .53) (P = .42)
Chang61/2001-2007
SRS 30 — [67% at 1 yr] — 15.2WBRT + SRS 28 — [100% at 1 yr] — 5.7(30 Gy/12 fx) — (P = .012) — (P = .003)
Kocher71/1996-2007
SRS 100 — [69% at 2 yr] 10.0 10.9Surgery 79 — [41% at 2 yr] Combined CombinedSRS + WBRT 99 — [81% at 2 yr] 9.5 10.7Surgery + WBRT 81 — [73% at 2 yr] Combined Combined(30 Gy/10 fx)
FFP, Freedom from progression; fx, fractions; NS, not significant; SRS, stereotactic radiosurgery; WBRT, whole-brain radiotherapy.
PartII:ProblemsCommontoCancerandItsTherapy732
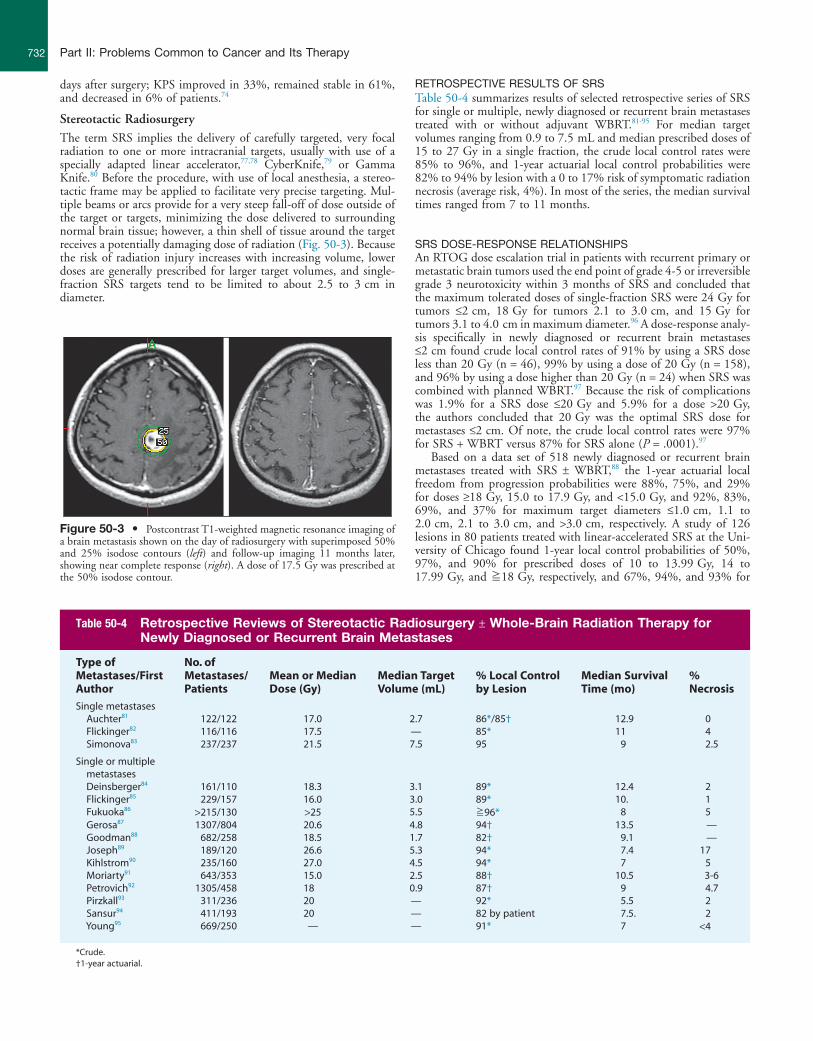
RETROSPECTIVERESULTSOFSRSTable 50-4 summarizes results of selected retrospective series of SRS for single or multiple, newly diagnosed or recurrent brain metastases treated with or without adjuvant WBRT.81-95 For median target volumes ranging from 0.9 to 7.5 mL and median prescribed doses of 15 to 27 Gy in a single fraction, the crude local control rates were 85% to 96%, and 1-year actuarial local control probabilities were 82% to 94% by lesion with a 0 to 17% risk of symptomatic radiation necrosis (average risk, 4%). In most of the series, the median survival times ranged from 7 to 11 months.
SRSDOSE-RESPONSERELATIONSHIPSAn RTOG dose escalation trial in patients with recurrent primary or metastatic brain tumors used the end point of grade 4-5 or irreversible grade 3 neurotoxicity within 3 months of SRS and concluded that the maximum tolerated doses of single-fraction SRS were 24 Gy for tumors ≤2 cm, 18 Gy for tumors 2.1 to 3.0 cm, and 15 Gy for tumors 3.1 to 4.0 cm in maximum diameter.96 A dose-response analy-sis specifically in newly diagnosed or recurrent brain metastases ≤2 cm found crude local control rates of 91% by using a SRS dose less than 20 Gy (n = 46), 99% by using a dose of 20 Gy (n = 158), and 96% by using a dose higher than 20 Gy (n = 24) when SRS was combined with planned WBRT.97 Because the risk of complications was 1.9% for a SRS dose ≤20 Gy and 5.9% for a dose >20 Gy, the authors concluded that 20 Gy was the optimal SRS dose for metastases ≤2 cm. Of note, the crude local control rates were 97% for SRS + WBRT versus 87% for SRS alone (P = .0001).97
Based on a data set of 518 newly diagnosed or recurrent brain metastases treated with SRS ± WBRT,88 the 1-year actuarial local freedom from progression probabilities were 88%, 75%, and 29% for doses ≥18 Gy, 15.0 to 17.9 Gy, and <15.0 Gy, and 92%, 83%, 69%, and 37% for maximum target diameters ≤1.0 cm, 1.1 to 2.0 cm, 2.1 to 3.0 cm, and >3.0 cm, respectively. A study of 126 lesions in 80 patients treated with linear-accelerated SRS at the Uni-versity of Chicago found 1-year local control probabilities of 50%, 97%, and 90% for prescribed doses of 10 to 13.99 Gy, 14 to 17.99 Gy, and ≧18 Gy, respectively, and 67%, 94%, and 93% for
days after surgery; KPS improved in 33%, remained stable in 61%, and decreased in 6% of patients.74
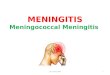
Stereotactic RadiosurgeryThe term SRS implies the delivery of carefully targeted, very focal radiation to one or more intracranial targets, usually with use of a specially adapted linear accelerator,77,78 CyberKnife,79 or Gamma Knife.80 Before the procedure, with use of local anesthesia, a stereo-tactic frame may be applied to facilitate very precise targeting. Mul-tiple beams or arcs provide for a very steep fall-off of dose outside of the target or targets, minimizing the dose delivered to surrounding normal brain tissue; however, a thin shell of tissue around the target receives a potentially damaging dose of radiation (Fig. 50-3). Because the risk of radiation injury increases with increasing volume, lower doses are generally prescribed for larger target volumes, and single-fraction SRS targets tend to be limited to about 2.5 to 3 cm in diameter.
Figure 50-3 • Postcontrast T1-weighted magnetic resonance imaging of a brain metastasis shown on the day of radiosurgery with superimposed 50% and 25% isodose contours (left) and follow-up imaging 11 months later, showing near complete response (right). A dose of 17.5 Gy was prescribed at the 50% isodose contour.
Table 50-4 Retrospective Reviews of Stereotactic Radiosurgery ± Whole-Brain Radiation Therapy for Newly Diagnosed or Recurrent Brain Metastases
Type of Metastases/First Author
No. of Metastases/Patients
Mean or Median Dose (Gy)
Median Target Volume (mL)
% Local Control by Lesion
Median Survival Time (mo)
% Necrosis
Single metastases Auchter81 122/122 17.0 2.7 86*/85† 12.9 0 Flickinger82 116/116 17.5 — 85* 11 4 Simonova83 237/237 21.5 7.5 95 9 2.5
Single or multiple metastases
Deinsberger84 161/110 18.3 3.1 89* 12.4 2 Flickinger85 229/157 16.0 3.0 89* 10. 1 Fukuoka86 >215/130 >25 5.5 ≧96* 8 5 Gerosa87 1307/804 20.6 4.8 94† 13.5 — Goodman88 682/258 18.5 1.7 82† 9.1 — Joseph89 189/120 26.6 5.3 94* 7.4 17 Kihlstrom90 235/160 27.0 4.5 94* 7 5 Moriarty91 643/353 15.0 2.5 88† 10.5 3-6 Petrovich92 1305/458 18 0.9 87† 9 4.7 Pirzkall93 311/236 20 — 92* 5.5 2 Sansur94 411/193 20 — 82 by patient 7.5. 2 Young95 669/250 — — 91* 7 <4
*Crude.†1-year actuarial.

BrainMetastasesandNeoplasticMeningitis • CHAPTER50 733
minimum tumor doses of ≤12 Gy, 12.1 to 18 Gy, and >18 Gy, respectively.98
RANDOMIZEDTRIALSOFWBRTWITHORWITHOUTSRSThe first reported randomized trial of WBRT (30 Gy in 12 fractions) ± SRS boost (16 Gy) was performed in patients with KPS ≧70 and two to four brain metastases ≤2.5 cm in diameter.55 The study only accrued 27 patients because of early stopping rules based on a signifi-cant difference in brain control between the two arms. Compared with WBRT alone, SRS + WBRT yielded significantly improved time to local failure (median, 36 vs. 6 months; P = .0005) and time to any brain failure (median, 34 vs. 5 months; P = .002). Survival was not significantly different for the two arms (median, 7.5 months for WBRT vs. 11 months for WBRT + SRS; P = .22) (Table 50-3). Mul-tiple patients for whom WBRT alone failed underwent salvage SRS.55
A 2004 RTOG trial randomly assigned 331 patients with KPS ≧70 and one to three newly diagnosed brain metastases to WBRT (37.5 Gy in 15 fractions) ± SRS boost within 1 week after WBRT from 1996 to 2001.54 Treatment arms were fairly well balanced in comparing WBRT alone to WBRT + SRS, with KPS of 90 to 100 in 63% versus 57%, age <65 years in 60% versus 66%, primary disease controlled or absent in 75% versus 77%, extracranial metas-tases in 69% versus 68%, and a single brain metastasis in 56% versus 56% of patients, respectively. Patients in the SRS treatment arm had significantly improved KPS at 6 months (P = .033), decreased steroid use at 6 months (P = .016), and improved local control (with 1-year local control probabilities of 71% for WBRT alone vs. 82% for WBRT + SRS; P = .013). Although survival was not significantly different between the two groups overall (5.7 months for WBRT alone vs. 6.5 months for WBRT + SRS; P = 0.136) (Table 50-3), a statistically significant difference in survival was found for patients with a single metastasis (4.9 months for WBRT alone vs. 6.5 months for WBRT + SRS; P = .039).54
SRSWITHOUTWBRTFORNEWLYDIAGNOSEDBRAINMETASTASESBecause of concern about potential late toxicity of WBRT, multiple groups have tried managing patients by using SRS alone initially, followed by later salvage surgery, SRS, WBRT, or chemotherapy as needed,34,36,93,99-102 laying the groundwork for later randomized trials. Survival was similar for SRS alone initially versus SRS with upfront WBRT for three of five studies (~5 vs. ~6 months;93 11.3 vs. 11.1 months;99 and 8.2 vs. 8.6 months34). In one study, median survival time was thought to be shorter in the WBRT group because of worse prognostic factors in this group,100 and in the fifth study, there was a trend toward longer survival time in patients treated with SRS + WBRT versus SRS alone.102 Multivariate analyses adjusting for known prognostic factors confirmed that the omission of upfront WBRT had no influence on survival time.34,93,99,100 Local control was slightly worse for SRS alone initially, with 1-year actuarial local freedom from progression probabilities of 89% versus 92%,93 71% versus 79%,99 and approximately 62% versus 75%.100 Because of a much greater risk of developing new brain metastases when upfront WBRT was omitted, brain freedom from progression was signifi-cantly shorter for SRS alone initially: median, 8.3 versus 15.9 months99 and 9.2 versus 35.1 months.100 In one series, the median brain freedom from progression allowing for salvage therapy was 19.8 months for SRS alone initially versus 18.1 months for SRS with upfront WBRT, and only 26% of patients receiving SRS alone ulti-mately received WBRT.99
RANDOMIZEDTRIALSOFSRSWITHORWITHOUTWBRTThe first prospective randomized trial comparing SRS alone (n = 67) to WBRT plus SRS (n = 65) was reported by Aoyama et al.103 Patients
with KPS ≥70 and one to four brain metastases <3 cm were accrued between 1999-2003 at 11 institutions. The WBRT dose was 30 Gy in 10 fractions, and SRS-alone doses were 22 to 25 Gy for lesions ≤2 cm and 18 to 20 Gy for lesions >2 cm, with a 30% dose reduction for SRS + WBRT. The median survival times were similar for the two groups (8.0 months for SRS alone vs. 7.5 months for WBRT + SRS; P = .42). Intracranial control was significantly lower in the SRS-alone arm, with 1-year local control probabilities of 73% versus 89% (P = .002), 1-year freedom from new brain metastasis probabilities of 36% versus 58% (P = .003), and 1-year overall brain freedom from pro-gression probabilities of 24% versus 53% (P < .001) for SRS alone versus WBRT + SRS, respectively. Most new brain metastases were asymptomatic. Salvage therapy for brain metastases was given in 29 patients enrolled in the SRS-alone arm versus 10 patients enrolled in the WBRT + SRS arm. There was no significant difference in func-tional independent survival (27% vs. 34% at 1 year; P = .53) or neurologic preservation (70% vs. 72% at 1 year; P = .99) for SRS alone versus WBRT + SRS, respectively. Deterioration of neurologic function occurred in 21 patients who received SRS alone and in 22 patients who received WBRT + SRS; the deterioration was attributed to new or original brain metastases in 18 patients who received SRS alone versus 13 patients who received WBRT + SRS. Leukoencepha-lopathy occurred in two patients who received SRS alone versus seven patients who received WBRT + SRS. The authors concluded that SRS alone “could be a treatment option, provided that frequent monitoring of brain tumor status is conducted.”103
Chang et al.61 published results of a prospective, randomized trial assessing outcomes in 58 RPA class 1-2 patients with one to three newly diagnosed brain metastases treated from 2001 to 2007 with SRS ± WBRT, with stratification by RPA class, histology, and number of metastases. The primary end point was neurocognitive function, as discussed in the section on “Toxicity of WBRT.” The WBRT dose was 30 Gy in 12 fractions, and SRS-alone doses were prescribed in accordance with RTOG 90-05. When comparing SRS alone with SRS + WBRT, survival time was longer (median, 15.2 vs. 5.7 months; 1-year survival, 63% vs. 21%; P = .003), whereas local and distant brain control were worse (1-year local control, 67% vs. 100%, P = .012; distant brain tumor control, 45% vs. 73%, P = .02; and 1-year freedom from CNS recurrence, 27% vs. 73%, respectively, P = .0003). Salvage therapy was given in 87% of the patients who received SRS alone versus 7% of patients who received SRS + WBRT. The authors concluded by suggesting that initial treatment with SRS alone for newly diagnosed brain metastases in conjunction with close surveillance could be used as a reasonable treatment strategy.
SRSFORMULTIPLEMETASTASESThe randomized trials assessing SRS ± upfront WBRT excluded patients with more than three to four metastases. However, a multi-institutional prospective Japanese study (JLGK0901) examined out-comes in patients with 1 to 10 brain metastases who were treated with SRS alone initially.104 This select cohort of patients had newly diagnosed brain metastases, with the largest lesion <10 mL, total tumor volume <15 mL, no evidence of leptomeningeal disease, and KPS >70. Patients were followed up closely with MRI after initial SRS and were treated with salvage SRS or WBRT as deemed appro-priate. The trial included 778 patients (280 with 1 lesion [group A], 135 with 2 lesions [group B], 148 with 3 to 4 lesions [group C], 93 with 5 to 6 lesions [group D], and 122 with 7 to 10 lesions [group E]). No significant differences in median survival times were found among the different groups (10.0, 8.3, 8.3, 7.1, and 7.4 months for groups A through E, respectively) or in 1-year functional preservation rate (91%, 93%, 81%, 84%, and 86%, respectively). The 1-year freedom from new metastasis probabilities were 72%, 54%, 44%, 51%, and 66% in groups A through E. Significant differences were found between groups A and B (P = .0003) and groups B and C (P = .0047). This study demonstrated that selected patients with up

PartII:ProblemsCommontoCancerandItsTherapy734
average of 4% of patients (Table 50-4), causing headaches, seizures, or neurologic deficits. Symptoms usually respond to steroids, but surgery may be needed if a patient requires a prolonged course of steroids, tolerates steroids poorly or continues to have symptoms while taking steroids, or if there is uncertainty about whether a lesion represents a progressive tumor versus a radiation effect.
BrachytherapyBrachytherapy—that is, the insertion of radioactive sources directly inside a tumor or tumor bed—allows delivery of a high dose of radia-tion to the target with steep dose fall-off. Temporary brachytherapy has been applied to brain metastases by using high-activity sources, often within afterloading catheters inserted into a gross tumor or a resection cavity, or by using a balloon within a resection cavity inflated with radioactive liquid. Permanent brachytherapy is generally accomplished by lining a tumor bed with low-activity radiation sources intraoperatively after resection of a metastasis. Several groups have described outcomes using permanent brachytherapy.108-115 In patients treated for recurrent brain metastases, crude local freedom from progression ranged from 60% to 95% and median survival from 6 to 14.8 months. Among patients treated for newly diagnosed brain metastases, local freedom from progression ranged from 80% to 95% and median survival ranged from 8 to 17 months (except for an outlier median survival of 68.2 months in five patients). The inci-dence of symptomatic radiation necrosis ranged from 0 to 30%.
Systemic TherapyChemotherapyChemotherapy has generally been considered to be relatively ineffec-tive for brain metastases, presumably because the blood-brain barrier prevents adequate access of chemotherapy to these tumors. However, some chemotherapeutic agents partially or even readily cross the blood-brain barrier; the fact that brain metastases enhance with con-trast material is proof that the blood-brain barrier is broken down within metastases. The chemosensitivity of the primary tumor is another critical factor in determining the potential efficacy of che-motherapy for brain metastases.116,117 The responsiveness of brain metastases to chemotherapy is similar to that of the primary tumor and extracranial metastases. Primary SCLC, lymphoma, germ cell tumors, and breast cancer are relatively chemosensitive,118 whereas non–small cell lung carcinoma (NSCLC) and melanoma are less chemosensitive.
The role of primary systemic therapy in patients with brain metas-tases is generally limited to persons with a chemosensitive primary tumor who have good performance status and multiple, small, asymptomatic lesions.119 Although systemic treatment in conjunction with radiation therapy improves imaging response rates, it has not been shown to improve survival in patients with brain metastases.120 More commonly, systemic agents are used as salvage after more con-ventional treatment (e.g., surgery, SRS, and WBRT) have failed. A comprehensive review on the role of chemotherapy in brain metas-tases is beyond the scope of this chapter. The reader is directed to the selected references for trials assessing chemotherapy for brain metas-tases from a variety of primary sites,121-129 as well as specific primary sites including NSCLC,130-140 SCLC,141-146 melanoma,122,147-152 and breast cancer.121-123,125,126,153-159
Molecularly Targeted TherapySeveral molecularly targeted agents are being investigated for the treatment of brain metastases. These agents include antiangiogenic drugs, immunomodulatory agents, and inhibitors of epidermal growth factor receptor (EGFR), BRAF, Gamma-secretase/notch, histone deacetylases, poly(adenosine diphosphate-ribose) polymerase, mammalian target of rapamycin, and protein kinase C beta.160 The use of some of these agents as they relate to specific histologies is discussed in this section.
to 10 newly diagnosed metastases could be reasonably treated with SRS alone initially.
SRSCOMPAREDWITHSURGERYSRS has potential advantages over surgery in that it is less invasive and can more easily address inaccessible and/or multiple lesions. In addition, the border between the metastasis and normal brain tissue may receive a sufficient dose to decrease the risk of local recurrence. The major disadvantages of SRS are that it is generally applicable only to lesions <2.5 to 3.0 cm and results in slow tumor shrinkage over weeks or months rather than relieving the mass effect immediately.
The European Organization for Research and Treatment of Cancer study discussed in the section on “Randomized Trial of Surgery or SRS With or Without WBRT”71 did not directly compare SRS and surgery, and there remains an absence of data to date from prospective randomized trials. Thus several authors have compared results cited in the literature for surgical patients with their own results for similar subsets of patients treated with SRS. Auchter et al.81 reported a four-institution experience of SRS and WBRT in 122 adults who met selection criteria similar to those used in randomized trials of WBRT with or without surgical resection: KPS ≥70 and newly diagnosed, surgically resectable single brain metastases with “nonsensitive” histology (excluding lymphoma, leukemia, multiple myeloma, SCLC, and germ cell tumors) and no urgent indication for resection. Local control was achieved in 86% of lesions with a 1-year actuarial local control probability of 85%, a median duration of functional independence of 10.1 months, and median survival time of 12.9 months (Table 50-4), comparable with the results of the “surgery + WBRT” arms of the randomized trials reported by Patchell et al.20 and Noordijk et al.65 (Table 50-3).
Three other retrospective comparisons of SRS and surgery are summarized in this section with somewhat differing results.76,105,106 Bindal et al. 105 reported 61% versus 87% crude local control rates for SRS (± WBRT) versus surgery (± WBRT) and median survival times of 7.5 months versus 16.4 months, respectively. Muacevic et al.76 compared outcomes for patients with single metastases ≤3.5 cm in diameter treated with SRS alone (56 patients) or with surgery with WBRT (52 patients). One-year local freedom from progression probabilities were 83% for SRS versus 75% for surgery with WBRT (P = .49); new brain metastases developed in 11 (20%) of the patients treated with SRS versus 6 (12%) of the patients treated with surgery + WBRT, but salvage SRS was successful in all 6 patients treated with SRS who were offered salvage therapy. Median survival times were 8.0 months after SRS versus 15.6 months after surgery with WBRT. Death rates from neurologic causes and complication rates were similar for the two treatment approaches, and steroid requirements tended to be less among the patients treated with SRS.76
A third retrospective study compared patients with single metas-tases who were candidates for either surgery or SRS.106 Most patients received adjuvant WBRT. Pretreatment performance status was worse in the SRS group. Crude local control rates were 100% versus 85% (P = .02) and 1-year survival probabilities were 56% versus 62% for SRS versus surgery (univariate P = .15; multivariate P = .62 with adjustment for age, performance status, and systemic disease status). Short-term and long-term complications occurred in 0% versus 13.5% and 17.4% versus 17.6% of patients treated with SRS versus surgery.106
TOXICITYOFSRSAcute complications of SRS occur in about 10% of patients, includ-ing seizures, headaches, exacerbation of preexisting neurologic defi-cits, nausea, and hemorrhage.76,93,107 Complications may include transient perifocal edema responding to a short course of steroids in 7% to 18% of patients76 or symptomatic late radiation effect in an

BrainMetastasesandNeoplasticMeningitis • CHAPTER50 735
of patients with breast cancer. Leptomeningeal dissemination has also been documented in less common neoplasms such as sarcomas, squa-mous cell carcinomas, and germ cell tumors. Primary tumors of the central nervous system such as medulloblastoma or ependymoma often seed the leptomeningeal space as well.172-176
PathophysiologyThe biological basis for dissemination and multifocal seeding of the leptomeninges by malignant cells is not well understood. Several distinct pathways have been proposed: (1) The most obvious pathway for leptomeningeal contamination is as a consequence of drop metas-tases that may occur during resection of metastatic foci within the brain, especially after resection of posterior fossa tumors; (2) direct extension from the cerebrum; (3) infiltration through arachnoid vessels or the choroid plexus after hematogenous dissemination of the tumor; (4) direct extension along peripheral nerves to the subarach-noid space or perivenous spread from the bone marrow within the skull; (5) extension along perineural or perivascular lymphatics; and (6) subependymal or choroid plexus metastases with subsequent escape into the CSF.177 Spread of tumor cells along the meningeal surface is facilitated by bulk CSF flow. In turn, meningeal deposits may also invade parenchyma, as well as cranial or spinal nerve roots. The most frequently affected regions of the CNS are the basilar cis-terns, the posterior fossa, and the cauda equina, where gravity pro-motes deposition of circulating cells.
Clinical PresentationLeptomeningeal dissemination of cancer elicits several distinct neu-rologic presentations. First, local tumor infiltration in the brain or spinal cord may cause headache, alterations in mental status, cranial nerve deficits causing diplopia, hearing loss, decreased taste, and problems with swallowing and hoarseness, as well as incontinence, lower motor neuron weakness, and back or radicular pain. Second, metabolic dysfunction caused by disturbances in regional blood flow in the affected nervous tissue may cause seizures, isolated neurologic deficits, including strokelike symptoms, and even generalized enceph-alopathy. Third, obstruction of normal CSF flow pathways by focal tumor deposits may cause increased intracranial pressure and hydrocephalus.172-176,178
DiagnosisCSF EvaluationA high index of suspicion is required to make an early diagnosis of neoplastic meningitis; a detailed examination of CSF ultimately is required. Routine measurements include opening pressure, cell count, differential, protein, glucose, and cytologic evaluation of the CSF.172 Patients with carcinomatous meningitis typically have elevated CSF opening pressure, increased CSF protein, and decreased CSF glucose.179 Although the CSF is abnormal in terms of protein or glucose concentration in most patients with neoplastic meningitis, cytologic evaluation of the CSF, the gold standard, is an insensitive test; 40% to 50% of patients with neoplastic meningitis have negative CSF cytology on initial lumbar puncture.172 Although repeat CSF cytological evaluations over time will increase diagnostic sensitivity, the eventual conversion to positive cytology usually occurs in pace with neurologic deterioration as a result of overt tumor progression. Because of the importance of early diagnosis and intervention, there has been significant effort to identify surrogate biomarkers for CNS and leptomeningeal metastases. For example, Posner’s group demon-strated that carcinoembryonic antigen, as well as the enzymatic activ-ity of beta-glucuronidase, could be detected in the CSF in patients with brain and leptomeningeal metastases.180 The presence of these markers was shown to precede clinical detection of neoplastic men-ingitis and to rise and fall in parallel with the clinical course. Several
The antiangiogenic agent bevacizumab has been studied in the treatment of brain metastases from NSCLC. One group reported the safety and moderate efficacy in terms of imaging and clinical response in this setting.161 Also, sunitinib and sorafenib (which are antiangio-genic agents) have been used in patients with brain metastases from renal cell carcinoma, albeit with limited efficacy.162,163 The use of the small-molecule EGFR inhibitor erlotinib has also been used because patients with brain metastases from NSCLC may have activating mutations of EGFR. One group was able to demonstrate encouraging objective CNS radiographic responses by using erlotinib in patients with EGFR-mutant metastatic lung cancer.164
In patients with metastatic HER2-positive breast cancer to the brain, lapatinib (a small-molecule dual inhibitor of HER2 and EGFR) has been used with some efficacy, although it remains inves-tigational.155,165 A newer immunomodulatory agent, ipilimumab, has been investigated in the management of brain metastases from mela-noma. It functions as a negative regulator of the antitumor T-cell response by blocking cytotoxic T-lymphocyte antigen-4 and thus acts as a T-cell potentiator.119 The results of a phase 2 study investigating the use of ipilimumab as a single agent for patients with brain metas-tases from melanoma were recently reported and describe objective responses in some patients.166
Follow-up and Salvage TherapyIn patients who are doing reasonably well from the standpoint of their systemic disease, we recommend follow-up MRI every 3 months after treatment for brain metastases to detect new or recurrent brain metastases that may need to be addressed with salvage therapy. Of note, a contrast-enhancing lesion seen after high-dose external beam radiation, SRS, or brachytherapy could represent radiation necrosis rather than recurrent tumor, and additional analyses may be needed before considering retreatment.167 The same therapeutic options available for newly diagnosed brain metastases may be considered for new, progressive, or recurrent metastases, although the type of previ-ous therapy given may influence therapeutic options at recurrence. In general, retreatment options include WBRT, SRS, surgery (espe-cially for a single large or symptomatic lesion), perhaps with perma-nent brachytherapy to help prevent local recurrence, and chemotherapy. If repeat WBRT is given, lower doses and smaller fraction sizes are generally used, such as 20 to 25 Gy in 10 fractions or 30 Gy at 1.0 Gy twice daily. Results are similar to those reported for a first course of WBRT, with symptomatic improvement in 42% to 75% of patients and median or mean survival of 3.2 to 5 months after reirradiation.168-171
NEOPLASTIC MENINGITISDissemination of cancer cells into the leptomeningeal space is an extremely serious complication that affects approximately 5% to 10% of patients with cancer. With incremental improvements in outcomes in systemic cancer, the incidence of metastatic disease to the lepto-meninges appears to be on the rise. Neoplastic meningitis presents significant diagnostic and therapeutic challenges; early diagnosis can be elusive, and effective control for leptomeningeal carcinoma is usually difficult to achieve. With current therapies, the median sur-vival time is 3 to 6 months.
EpidemiologyVirtually any type of cancer can disseminate into the leptomeningeal space. Acute leukemias and intermediate or high-grade lymphomas are common causes of neoplastic meningitis. Among solid tumors, melanoma and small cell carcinoma exhibit the strongest propensity for leptomeningeal dissemination, with this complication developing in up to 25% of patients with metastatic disease from these diagnoses. Ultimately, carcinomatous meningitis develops in between 2% to 5%

PartII:ProblemsCommontoCancerandItsTherapy736
of the disease in the neuraxis. For example, in patients presenting with cranial nerve deficits, one approach is to treat only the base of the skull with radiation. In patients who present with cauda equina syndrome, external beam irradiation may be directed to the lumbo-sacral spine. The best palliation for patients who present with seizure or hydrocephalus caused by extensive cranial leptomeningeal disease may be achieved with whole-brain irradiation.173-176
Intrathecal ChemotherapyThe most reliable means of administering intrathecal chemotherapy is to use an implanted subcutaneous reservoir and ventricular catheter (Ommaya device). Although subarachnoid injections of chemother-apy result in high local CSF concentrations, studies of lumbar admin-istration suggest that 10% to 15% of lumbar punctures fail to completely deliver all of the drug to the subarachnoid space.176 In addition, retrospective analysis suggests that intraventricular admin-istration may result in prolonged remission in patients with lepto-meningeal leukemia compared with administration by lumbar puncture.182 Chemotherapeutic agents administered into the ventricle are carried through the neuraxis by bulk CSF flow. CSF flow abnor-malities are common in patients with leptomeningeal metastases, who frequently present with hydrocephalus and increased intracranial pressure as a result of disease that impedes CSF flow. Radionuclide ventriculography in patients with neoplastic meningitis has demon-strated that as many as 70% have ventricular outlet obstruction, abnormal flow in the spinal canal, or impaired flow over the CSF convexities.183 These CSF flow abnormalities may be reversed with local irradiation. Because of the potential risk of irreversible neuro-toxicity from high sustained concentrations of intrathecal chemo-therapy, a CSF flow study is recommended for every patient beginning intrathecal chemotherapy via a ventricular catheter.173,174
Methotrexate and cytarabine are the most widely used agents for intrathecal chemotherapy. Intraventricular injection of methotrexate results in therapeutic concentrations >1 µmol/L that persist for up to 48 hours; serum levels peak at approximately 0.1 µmol/L and fall more slowly. Treatment of active neoplastic meningitis typically con-sists of twice-weekly intrathecal therapy until the CSF clears, followed by weekly and then monthly maintenance therapy until disease pro-gression. The combination of twice-weekly methotrexate plus radia-tion results in an approximate 50% rate of disease stability or clinical improvement. Response should be assessed both in the ventricle and in the lumbar sac where cytology is more likely to be positive. Intra-thecal administration of methotrexate can cause myelosuppression and mucositis; these toxicities can be attenuated by leucovorin. Leu-covorin does not efficiently cross the blood-brain barrier in amounts sufficient to interfere with intra-CNS effects of methotrexate.
Cytosine arabinoside (Ara-C) is also commonly used but may have less efficacy in the treatment of neoplastic meningitis. Ara-C is inac-tivated by deamination by the enzyme cytidine deaminase. Low CNS levels of this enzyme result in relatively slow deamination of Ara-C within the brain and CSF, resulting in an extended half-life in the CNS compartment.176 Thiotepa, a cell cycle nonspecific alkylating agent, is another commonly used intrathecal drug.181 Other intrathe-cal agents that have been studied in this context include mafospha-mide,184 topotecan,185 etoposide,186 interferon alpha,187 and 5-fluoro-2′ deoxyuridine.188 Further investigation of these agents is warranted.
Treatment-Related ToxicityPlacement of an intraventricular catheter is associated with <1% risk of perioperative hemorrhage. Extended use of the device is associated with a ≥5% risk of infection, usually with Staphylococcus epidermidis or Staphylococcus aureus. Impaired CSF flow of chemotherapy as a result of obstruction may result in seizures, as well as acute arach-noiditis, characterized by nausea, vomiting, and mental status changes. For this reason many practitioners obtain a radionuclide CSF flow study before initiation of intra-Ommaya chemotherapy.
other biomarkers have been examined in patients with carcinomatous meningitis, including lactate dehydrogenase, beta-human chorionic gonadotropin, alkaline phosphatase, vascular endothelial growth factor, myelin basic protein, creatinine kinase, and others. The utility of these biomarkers is still under investigation.179 The use of other diagnostic tools such as polymerase chain reactions, fluorescence in-situ hybridization, immunohistochemical examinations of the CSF, and cytogenetic analysis may also enhance detection.181
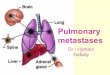
Radiologic FeaturesGenerally, an MRI of the entire neuraxis is advisable. The most fre-quent radiographic presentation is hydrocephalus without an identifi-able mass lesion. Leptomeningeal contrast enhancement is suggestive of neoplastic meningitis (Fig. 50-4) but may also be seen after lumbar puncture or with infection, inflammatory disease, trauma, subdural hematoma, or changes occurring after a craniotomy.172 The enhance-ment pattern may be focal (including tumor nodules) or diffuse.181 Although gadolinium-enhanced MRI is more sensitive than CT in identifying leptomeningeal enhancement, only approximately 50% of patients with neoplastic meningitis and spinal symptoms have abnormal imaging studies.172
TreatmentCurrent therapeutic goals for most patients with neoplastic meningi-tis are to prevent further neurologic deterioration, cytoreduce the leptomeningeal tumor burden, and prolong survival. Typically, untreated carcinomatous meningitis is associated with an advanced stage of systemic disease, often with concomitant parenchymal brain metastases and with an anticipated survival time of 4 to 6 weeks. Because of the inefficient regenerative capacity of the CNS, early aggressive intervention is critical to preserve neurologic function. Therapeutic intervention relies on traditional approaches with radia-tion and/or chemotherapy with the goal of treating the entire neuraxis.
Radiation TherapyRadiation therapy is the most effective means of palliation, with the focus on symptomatic sites and regions where imaging studies have demonstrated bulk disease. Craniospinal axis irradiation results in substantial acute toxicity, with nausea, vomiting, marked fatigue, and myelosuppression. A negative impact on bone marrow function of long duration also occurs, compromising the safe administration of subsequent myelosuppressive chemotherapy. One strategy is to selec-tively apply external beam irradiation to symptomatic sites of disease and to rely on intrathecal chemotherapy to suppress the remainder
Figure 50-4 • Leptomeningeal enhancement from carcinomatous men-ingitis on postcontrast T1-weighted magnetic resonance imaging. Note the enhancement of the acoustic nerves and cerebellar folia (arrows).

BrainMetastasesandNeoplasticMeningitis • CHAPTER50 737
Finally, in the current era of targeted therapeutics, there is increas-ing interest in the use of biological therapies for leptomeningeal disease, particularly small molecule protein kinase inhibitors or monoclonal antibodies against tumor-associated cell surface mole-cules. An increasing amount of evidence indicates that when these agents are administered systemically they penetrate the leptomenin-geal space inefficiently. For example, relatively low CSF levels of monoclonal antibodies that target CD20 in B-cell lymphomas or of small molecules that inhibit the bcr-abl tyrosine kinase have been documented after systemic administration.190,191 Direct intra-CSF administration of monoclonal antibodies and immunotoxins is an area of current early-phase investigation in the treatment and/or prophylaxis of neoplastic meningitis.190,192 A phase 1 dose escalation study formally evaluated the safety and efficacy of intrathecal admin-istration of an anti-CD20 antibody in 10 patients with recurrent CNS and intraocular lymphoma.193 Responses were identified in patients with meningeal, parenchymal, and intraocular disease. Another group reported promising results of targeted iodine-131–radiolabeled monoclonal antibodies administered to 52 patients with neoplastic meningitis.194 Some groups have also documented responses to trastuzumab, a humanized antibody directed to HER2, in patients with leptomeningeal carcinomatosis from HER2-overexpressing primary breast cancer.195-197
Ultimately the most significant toxicity associated with the treatment of leptomeningeal carcinomatosis is the development of necrotizing leukoencephalopathy, which is most common in patients who have been treated with intrathecal methotrexate after cranial irradiation. Initial findings are imaging changes, usually symmetric abnormalities in white matter. Many of these patients subsequently experience progressive dementia that can progress to substantial debility and death.176
Systemic Chemotherapy and New ApproachesA significant fraction of contrast-enhancing tumor visualized on neu-roimaging studies is theoretically accessible by systemic chemother-apy that is able to reach this fraction of tumor supplied by an abnormally permeable neovasculature. However, water-soluble che-motherapy drugs are limited by the intact blood-brain barrier and systemic therapy fails to treat microscopic, nonenhancing disease both in brain parenchyma and in the subarachnoid space. One excep-tion is the use of high-dose systemic administration of methotrexate that results in therapeutic levels in the CSF for a longer duration than the intrathecal route. This therapeutic strategy has been shown to be active in persons with neoplastic meningitis in both lymphoma and in solid tumors. Moreover, systemic administration of methotrexate at high doses overcomes the problems associated with CSF flow obstruction that may compromise subarachnoid administration. However, because administration of high-dose methotrexate requires detailed inpatient monitoring of fluid status, urine alkalinization, and renal function, systemic administration of methotrexate at high doses is not appropriate or practical for all patients.189
The complete reference list is available online at www.expertconsult.com.
R E F E R E N C E S2. Schouten LJ, Rutten J, Huveneers HAM, Twijnstra
A. Incidence of brain metastases in a cohort of patients with carcinoma of the breast, colon, kidney, and lung and melanoma. Cancer 2002;94(10):2698–705.
3. Barnholtz-Sloan JS, Sloan AE, Davis FG, et al. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metro-politan Detroit Cancer Surveillance System. J Clin Oncol 2004;22(14):2865–72.
5. Delattre JY, Krol G, Thaler HT, Posner JB. Distribution of brain metastases. Arch Neurol 1988;45(7):741–4.
20. Patchell RA, Tibbs PA, Walsh JW, et al. A randomized trial of surgery in the treatment of single metastases to the brain. N Engl J Med 1990;322(8):494–500.
26. Chao JH, Phillips R, Nickson JJ. Roentgen-ray therapy of cerebral metastases. Cancer 1954; 7(4):682–9.
29. Borgelt B, Gelber R, Kramer S, et al. The palliation of brain metastases: final results of the first two studies by the Radiation Therapy Oncology Group. Int J Radiat Oncol Biol Phys 1980; 6(1):1–9.
30. Kurtz JM, Gelber R, Brady LW, et al. The pallia-tion of brain metastases in a favorable patient population: a randomized clinical trial by the Radiation Therapy Oncology Group. Int J Radiat Oncol Biol Phys 1981;7(7):891–5.
33. Gaspar L, Scott C, Rotman M, et al. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int J Radiat Oncol Biol Phys 1997;37(4):745–51.
34. Sneed PK, Suh JH, Goetsch SJ, et al. A multi-institutional review of radiosurgery alone vs. radio-surgery with whole brain radiotherapy as the initial
management of brain metastases. Int J Radiat Oncol Biol Phys 2002;53(3):519–26.
40. Sperduto PW, Berkey B, Gaspar LE, et al. A new prognostic index and comparison to three other indices for patients with brain metastases: an analy-sis of 1,960 patients in the RTOG database. Int J Radiat Oncol Biol Phys 2008;70(2):510–14.
41. Sperduto PW, Kased N, Roberge D, et al. Summary report on the graded prognostic assessment: An accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J Clin Oncol 2012;30(4):419–25.
42. Ryken TC, McDermott M, Robinson PD, et al. The role of steroids in the management of brain metastases: a systematic review and evidence-based clinical practice guideline. J Neurooncol 2010; 96(1):103–14.
45. Glantz MJ, Cole BF, Friedberg MH, et al. A randomized, blinded, placebo-controlled trial of divalproex sodium prophylaxis in adults with newly-diagnosed brain tumors. Neurology 1996; 46(4):985–91.
48. Coia LR. The role of radiation therapy in the treat-ment of brain metastases. Int J Radiat Oncol Biol Phys 1992;23(1):229–38.
54. Andrews DW, Scott CB, Sperduto PW, et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: phase III results of the RTOG 9508 randomised trial. Lancet 2004;363(9422):1665–72.
55. Kondziolka D, Patel A, Lunsford LD, et al. Stereo-tactic radiosurgery plus whole brain radiotherapy versus radiotherapy alone for patients with multi-ple brain metastases. Int J Radiat Oncol Biol Phys 1999;45(2):427–34.
60. Aoyama H, Tago M, Kato N, et al. Neurocognitive function of patients with brain metastasis who
received either whole brain radiotherapy plus ste-reotactic radiosurgery or radiosurgery alone. Int J Radiat Oncol Biol Phys 2007;68(5):1388–95.
61. Chang EL, Wefel JS, Hess KR, et al. Neurocogni-tion in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: a randomised controlled trial. Lancet Oncol 2009;10(11):1037–44.
65. Noordijk EM, Vecht CJ, Haaxma-Reiche H, et al. The choice of treatment of single brain metastasis should be based on extracranial tumor activity and age. Int J Radiat Oncol Biol Phys 1994;29(4): 711–17.
66. Mintz AH, Kestle J, Rathbone MP, et al. A ran-domized trial to assess the efficacy of surgery in addition to radiotherapy in patients with a single cerebral metastasis. Cancer 1996;78(7):1470–6.
70. Patchell RA, Tibbs PA, Regine WF, et al. Postop-erative radiotherapy in the treatment of single metastases to the brain: a randomized trial. JAMA 1998;280(17):1485–9.
71. Kocher M, Soffietti R, Abacioglu U, et al. Adjuvant whole-brain radiotherapy versus observation after radiosurgery or surgical resection of one to three cerebral metastases: results of the EORTC 22952–26001 study. J Clin Oncol 2011;29(2):134–41.
76. Muacevic A, Kreth FW, Horstmann GA, et al. Surgery and radiotherapy compared with gamma knife radiosurgery in the treatment of solitary cere-bral metastases of small diameter. J Neurosurg 1999;91(1):35–43.
81. Auchter RM, Lamond JP, Alexander 3rd E, et al. A multiinstitutional outcome and prognostic factor analysis of radiosurgery for resectable single brain metastasis. Int J Radiat Oncol Biol Phys 1996;35(1):27–35.
82. Flickinger JC, Kondziolka D, Lunsford LD, et al. A multi-institutional experience with stereotactic
PartII:ProblemsCommontoCancerandItsTherapy738
radiosurgery for solitary brain metastasis. Int J Radiat Oncol Biol Phys 1994;28(4):797–802.
93. Pirzkall A, Debus J, Lohr F, et al. Radiosurgery alone or in combination with whole-brain radio-therapy for brain metastases. J Clin Oncol 1998;16(11):3563–9.
96. Shaw E, Scott C, Souhami L, et al. Single dose radiosurgical treatment of recurrent previously irradiated primary brain tumors and brain metas-tases: final report of RTOG protocol 90–05. Int J Radiat Oncol Biol Phys 2000;47(2):291–8.
99. Sneed PK, Lamborn KR, Forstner JM, et al. Radio-surgery for brain metastases: is whole brain radio-therapy necessary? Int J Radiat Oncol Biol Phys 1999;43(3):549–58.
103. Aoyama H, Shirato H, Tago M, et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: a randomized controlled trial. JAMA 2006;295(21):2483–91.
104. Serizawa T, Hirai T, Nagano O, et al. Gamma knife surgery for 1-10 brain metastases without prophylactic whole-brain radiation therapy: analy-sis of cases meeting the Japanese prospective multi-institute study (JLGK0901) inclusion criteria. J Neurooncol 2010;98(2):163–7.
111. McDermott MW, Cosgrove GR, Larson DA, et al. Interstitial brachytherapy for intracranial metasta-ses. Neurosurg Clin N Am 1996;7(3):485–95.
116. Soffietti R, Costanza A, Laguzzi E, et al. Radio-therapy and chemotherapy of brain metastases. J Neurooncol 2005;75(1):31–42.
117. van den Bent MJ. The role of chemotherapy in brain metastases. Eur J Cancer 2003;39(15): 2114–20.
118. Soffietti R, Cornu P, Delattre JY, et al. EFNS Guidelines on diagnosis and treatment of brain metastases: report of an EFNS Task Force. European Journal of Neurology 2006;13(7): 674–81.
119. Grimm SA. Treatment of brain metastases: chemo-therapy. Curr Oncol Rep 2012;14(1):85–90.
120. Mehta MP, Paleologos NA, Mikkelsen T, et al. The role of chemotherapy in the management of newly diagnosed brain metastases: a systematic review and evidence-based clinical practice guideline. J Neurooncol 2010;96(1):71–83.
122. Franciosi V, Cocconi G, Michiara M, et al. Front-line chemotherapy with cisplatin and etoposide for patients with brain metastases from breast carci-noma, nonsmall cell lung carcinoma, or malignant melanoma. Cancer 1999;85(7):1599–605.
128. Antonadou D, Paraskevaidis M, Sarris G, et al. Phase II randomized trial of temozolomide and concurrent radiotherapy in patients with brain metastases. J Clin Oncol 2002;20(17):3644–50.
145. Postmus PE, Haaxma-Reiche H, Smit EF, et al. Treatment of brain metastases of small-cell lung
cancer: comparing teniposide and teniposide with whole-brain radiotherapy—a phase III study of the European Organization for the Research and Treatment of Cancer Lung Cancer Cooperative Group. J Clin Oncol 2000;18(19):3400–8.
150. Agarwala SS, Kirkwood JM, Gore M, et al. Temo-zolomide for the treatment of brain metastases associated with metastatic melanoma: a phase II study. J Clin Oncol 2004;22(11):2101–7.
172. Chamberlain M. Neoplastic meningitis: a guide to diagnosis and treatment. Curr Opin Neurol 2000;13(6):641–8.
178. DeAngelis LM. Current diagnosis and treatment of leptomeningeal metastasis. J Neurooncol 1998;38(2-3):245–52.
189. Glantz MJ, Cole BF, Recht L, et al. High- dose intravenous methotrexate for patients with nonleukemic leptomeningeal cancer: is intrathecal chemotherapy necessary? J Clin Oncol 1998; 16(4):1561–7.
190. Rubenstein JL, Combs D, Rosenberg J, et al. Rituximab therapy for CNS lymphomas: targeting the leptomeningeal compartment. Blood 2003; 101(2):466–8.
193. Rubenstein JL, Fridlyand J, Abrey L, et al. Phase I study of intraventricular administration of ritux-imab in patients with recurrent CNS and intraocu-lar lymphoma. J Clin Oncol 2007;25(11): 1350–6.
BrainMetastasesandNeoplasticMeningitis • CHAPTER50 738.e1
R E F E R E N C E S1. Posner JB, Chernik NL. Intracranial metastases
from systemic cancer. Adv Neurol 1978;19: 579–92.
2. Schouten LJ, Rutten J, Huveneers HAM, Twijnstra A. Incidence of brain metastases in a cohort of patients with carcinoma of the breast, colon, kidney, and lung and melanoma. Cancer 2002;94(10):2698–705.
3. Barnholtz-Sloan JS, Sloan AE, Davis FG, et al. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metro-politan Detroit Cancer Surveillance System. J Clin Oncol 2004;22(14):2865–72.
4. Seute T, Leffers P, ten Velde GPM, Twijnstra A. Detection of brain metastases from small cell lung cancer. Cancer 2008;112(8):1827–34.
5. Delattre JY, Krol G, Thaler HT, Posner JB. Distribution of brain metastases. Arch Neurol 1988;45(7):741–4.
6. Nussbaum ES, Djalilian HR, Cho KH, Hall WA. Brain metastases histology, multiplicity, surgery, survival. Cancer 1996;78(8):1781–8.
7. Graus F, Walker RW, Allen JC. Brain metastases in children. J Pediatr 1983;103(4):558–61.
8. Hwang TL, Close TP, Grego JM, et al. Predilection of brain metastasis in gray and white matter junc-tion and vascular border zones. Cancer 1996; 77(8):1551–5.
9. Hojo S, Hirano A. Pathology of metastases affect-ing the central nervous system. In: Takakura K, Sano K, Hojo S, et al, editors. Metastatic Tumors of the Central Nervous System. Tokyo: Igaku-Shoin; 1982. p. 5–35.
10. Abe E, Aoyama H. The role of whole brain radiation therapy for the management of brain metastases in the era of stereotactic radiosurgery. Curr Oncol Rep 2012;14(1):79–84.
11. Cairncross JG, Kim J-H, Posner JB. Radiation therapy for brain metastases. Ann Neurol 1980;7(6):529–41.
12. Posner JB. Management of central nervous system metastases. Semin Oncol 1977;4(1):81–91.
13. Sze G, Milano E, Johnson C, Heier L. Detection of brain metastases: comparison of contrast-enhanced MR with unenhanced MR and enhanced CT. Am J Neuroradiol 1990;11(4):785–91.
14. Davis PC, Hudgins PA, Peterman SB, Hoffman Jr JC. Diagnosis of cerebral metastases double-dose delayed CT vs contrast-enhanced MR imaging. Am J Neuroradiol 1991;12(2):293–300.
15. Schellinger PD, Meinck HM, Thron A. Diagnostic accuracy of MRI compared to CCT inpatients with brain metastases. J Neurooncol 1999;44(3): 275–81.
16. Yuh WTC, Fisher DJ, Runge VM, et al. Phase III multicenter trial of high-dose gadoteridol in MR evaluation of brain metastases. Am J Neuroradiol 1994;15(6):1037–51.
17. Cha S, Knopp EA, Johnson G, et al. Intracranial mass lesions: dynamic contrast-enhanced susceptibility-weighted echo-planar perfusion MR imaging. Radiology 2002;223(1):11–29.
18. Law M, Cha S, Knopp EA, et al. High-grade gliomas and solitary metastases: differentiation by using perfusion and proton spectroscopic MR imaging. Radiology 2002;222(3):715–21.
19. Schaefer PW, Budzik Jr RF, Gonzalez RG. Imaging of cerebral metastases. Neurosurg Clin N Am 1996;7(3):393–423.
20. Patchell RA, Tibbs PA, Walsh JW, et al. A randomized trial of surgery in the treatment of single metastases to the brain. N Engl J Med 1990;322(8):494–500.
21. Franzini A, Leocata F, Giorgi C, et al. Role of stereotactic biopsy in multifocal brain lesions: con-siderations on 100 consecutive cases. J Neurol Neurosurg Psychiatry 1994;57(8):957–60.
22. Lang EF, Slater J. Metastatic brain tumors. Results of surgical and nonsurgical treatment. Surg Clin North Am 1964;44:865–72.
23. Markesbery WR, Brooks WH, Gupta GD, Young AB. Treatment for patients with cerebral metasta-ses. Arch Neurol 1978;35(11):754–6.
24. Richards P, McKissock W. Intracranial metastases. Br Med J 1963;1(5322):15–18.
25. Horton J, Baxter DH, Olson KB. The manage-ment of metastases to the brain by irradiation and corticosteroids. American Journal of Roentgenol-ogy 1971;111(2):334–6.
26. Chao JH, Phillips R, Nickson JJ. Roentgen-ray therapy of cerebral metastases. Cancer 1954;7(4): 682–9.
27. Chu FCH, Hilaris BB. Value of radiation therapy in the management of intracranial metastases. Cancer 1961;14:577–81.
28. Order SE, Hellman S, von Essen CF, Kligerman MM. Improvement in quality of survival following whole-brain irradiation for brain metastasis. Radi-ology 1968;91(1):149–53.
29. Borgelt B, Gelber R, Kramer S, et al. The palliation of brain metastases: final results of the first two studies by the Radiation Therapy Oncology Group. Int J Radiat Oncol Biol Phys 1980; 6(1):1–9.
30. Kurtz JM, Gelber R, Brady LW, et al. The pallia-tion of brain metastases in a favorable patient population: a randomized clinical trial by the Radiation Therapy Oncology Group. Int J Radiat Oncol Biol Phys 1981;7(7):891–5.
31. Murray KJ, Scott C, Greenberg HM, et al. A ran-domized phase III study of accelerated hyperfrac-tionation versus standard in patients with unresected brain metastases: a report of the Radia-tion Therapy Oncology Group (RTOG) 9104. Int J Radiat Oncol Biol Phys 1997;39(3):571–4.
32. Lagerwaard FJ, Levendag PC, Nowak PJCM, et al. Identification of prognostic factors in patients with brain metastases: a review of 1292 patients. Int J Radiat Oncol Biol Phys 1999;43(4):795–803.
33. Gaspar L, Scott C, Rotman M, et al. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int J Radiat Oncol Biol Phys 1997;37(4):745–51.
34. Sneed PK, Suh JH, Goetsch SJ, et al. A multi-institutional review of radiosurgery alone vs. radio-surgery with whole brain radiotherapy as the initial management of brain metastases. Int J Radiat Oncol Biol Phys 2002;53(3):519–26.
35. Kocher M, Maarouf M, Bendel M, et al. Linac radiosurgery versus whole brain radiotherapy for brain metastases. Strahlenther Onkol 2004; 180(5):263–7.
36. Lutterbach J, Cyron D, Henne K, Ostertag CB. Radiosurgery followed by planned observation in patients with one to three brain metastases. Neu-rosurgery 2003;52(5):1066–73.
37. Agboola O, Benoit B, Cross P, et al. Prognostic factors derived from recursive partitioning analysis (RPA) of Radiation Therapy Oncology Group (RTOG) brain metastases trials applied to surgi-cally resected and irradiated brain metastatic cases. Int J Radiat Oncol Biol Phys 1998;42(1):155–9.
38. Regine WF, Rogozinska A, Kryscio RJ, et al. Recursive partitioning analysis classifications I and II: applicability evaluated in a randomized trial for resected single brain metastases. Am J Clin Oncol 2004;27(5):505–9.
39. Tendulkar RD, Liu SW, Barnett GH, et al. RPA classification has prognostic significance for surgi-cally resected single brain metastasis. Int J Radiat Oncol Biol Phys 2006;66(3):810–17.
40. Sperduto PW, Berkey B, Gaspar LE, et al. A new prognostic index and comparison to three other
indices for patients with brain metastases: an analy-sis of 1,960 patients in the RTOG database. Int J Radiat Oncol Biol Phys 2008;70(2):510–14.
41. Sperduto PW, Kased N, Roberge D, et al. Summary report on the graded prognostic assessment: An accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J Clin Oncol 2012;30(4):419–25.
42. Ryken TC, McDermott M, Robinson PD, et al. The role of steroids in the management of brain metastases: a systematic review and evidence-based clinical practice guideline. J Neurooncol 2010; 96(1):103–14.
43. Batchelor T, DeAngelis LM. Medical management of cerebral metastases. Neurosurg Clin N Am 1996;7(3):435–46.
44. Cohen N, Strauss G, Lew R, et al. Should prophylactic anticonvulsants be administered to patients with newly-diagnosed cerebral metastases? A retrospective analysis. J Clin Oncol 1988;6(10): 1621–4.
45. Glantz MJ, Cole BF, Friedberg MH, et al. A randomized, blinded, placebo-controlled trial of divalproex sodium prophylaxis in adults with newly-diagnosed brain tumors. Neurology 1996;46(4):985–91.
46. Kargiotis O, Markoula S, Kyritsis AP. Epilepsy in the cancer patient. Cancer Chemotherapy and Pharmacology 2011;67(3):489–501.
47. Glantz MJ, Cole BF, Forsyth PA, et al. Practice parameter: anticonvulsant prophylaxis in patients with newly diagnosed brain tumors. Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2000;54(10):1886–93.
48. Coia LR. The role of radiation therapy in the treat-ment of brain metastases. Int J Radiat Oncol Biol Phys 1992;23(1):229–38.
49. Borgelt B, Gelber R, Larson M, et al. Ultra-rapid high dose irradiation schedules for the palliation of brain metastases: final results of the first two studies by the Radiation Therapy Oncology Group. Int J Radiat Oncol Biol Phys 1981; 7(12):1633–8.
50. Hindo WA, DeTrana FAIII, Lee M-S, Hendrickson FR. Large dose increment irradiation in treatment of cerebral metastases. Cancer 1970;26(1):138–41.
51. Young DF, Posner JB, Chu F, Nisce L. Rapid-course radiation therapy of cerebral metastases: results and complications. Cancer 1974;34(4):1069–76.
52. Nieder C, Berberich W, Schnabel K. Tumor-related prognostic factors for remission of brain metastases after radiotherapy. Int J Radiat Oncol Biol Phys 1997;39(1):25–30.
53. Nieder C, Berberich W, Nestle U, et al. Relation between local result and total dose of radiotherapy for brain metastases. Int J Radiat Oncol Biol Phys 1995;33(2):349–55.
54. Andrews DW, Scott CB, Sperduto PW, et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: phase III results of the RTOG 9508 randomised trial. Lancet 2004;363(9422):1665–72.
55. Kondziolka D, Patel A, Lunsford LD, et al. Stereo-tactic radiosurgery plus whole brain radiotherapy versus radiotherapy alone for patients with multi-ple brain metastases. Int J Radiat Oncol Biol Phys 1999;45(2):427–34.
56. DeAngelis LM, Mandell LR, Thaler HT, et al. The role of postoperative radiotherapy after resec-tion of single brain metastases. Neurosurgery 1989;24(6):798–805.
57. van der Ree RC, Dippel DW, Avezaat CJ, et al. Leptomeningeal metastasis after surgical resection
PartII:ProblemsCommontoCancerandItsTherapy738.e2
of brain metastases. J Neurol Neurosurg Psychiatry 1999;66(2):225–7.
58. DeAngelis LM, Delattre JY, Posner JB. Radiation-induced dementia in patients cured of brain metas-tases. Neurology 1989;39(6):789–96.
59. Nieder C, Schwerdtfeger K, Steudel W-I, Schnabel K. Patterns of relapse and late toxicity after resection and whole-brain radiotherapy for solitary brain metastases. Strahlenther Onkol 1998;174(5):275–8.
60. Aoyama H, Tago M, Kato N, et al. Neurocognitive function of patients with brain metastasis who received either whole brain radiotherapy plus ste-reotactic radiosurgery or radiosurgery alone. Int J Radiat Oncol Biol Phys 2007;68(5):1388–95.
61. Chang EL, Wefel JS, Hess KR, et al. Neurocogni-tion in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irra-diation: a randomised controlled trial. Lancet Oncol 2009;10(11):1037–44.
62. Sun A, Bae K, Gore EM, et al. Phase III trial of prophylactic cranial irradiation compared with observation in patients with locally advanced non-small-cell lung cancer: neurocognitive and quality-of-life analysis. J Clin Oncol 2011;29(3):279–86.
63. Sills AK. Current treatment approaches to surgery for brain metastases. Neurosurgery 2005;57(5 Suppl):S24–32; discussion S1–4.
64. Lang FF, Sawaya R. Surgical management of cerebral metastases. Neurosurg Clin N Am 1996;7(3):459–84.
65. Noordijk EM, Vecht CJ, Haaxma-Reiche H, et al. The choice of treatment of single brain metastasis should be based on extracranial tumor activity and age. Int J Radiat Oncol Biol Phys 1994;29(4): 711–17.
66. Mintz AH, Kestle J, Rathbone MP, et al. A ran-domized trial to assess the efficacy of surgery in addition to radiotherapy in patients with a single cerebral metastasis. Cancer 1996;78(7):1470–6.
67. Hendrickson FR, Lee M-S, Larson M, Gelber RD. The influence of surgery and radiation therapy on patients with brain metastases. Int J Radiat Oncol Biol Phys 1983;9(5):623–7.
68. Patchell RA, Cirrincione C, Thaler HT, et al. Single brain metastases: surgery plus radiation or radiation alone. Neurology 1986;36(4):447–53.
69. Sause WT, Crowley JJ, Morantz R, et al. Solitary brain metastasis: results of an RTOG/SWOG protocol evaluation surgery + RT versus RT alone. Am J Clin Oncol 1990;13(5):427–32.
70. Patchell RA, Tibbs PA, Regine WF, et al. Postop-erative radiotherapy in the treatment of single metastases to the brain: a randomized trial. JAMA 1998;280(17):1485–9.
71. Kocher M, Soffietti R, Abacioglu U, et al. Adjuvant whole-brain radiotherapy versus observation after radiosurgery or surgical resection of one to three cerebral metastases: results of the EORTC 22952–26001 study. J Clin Oncol 2011;29(2):134–41.
72. Bindal RK, Sawaya R, Leavens ME, Lee JJ. Surgi-cal treatment of multiple brain metastases. J Neu-rosurg 1993;79(2):210–16.
73. Hazuka MB, Burleson WD, Stroud DN, et al. Multiple brain metastases are associated with poor survival in patients treated with surgery and radio-therapy. J Clin Oncol 1993;11(2):369–73.
74. Paek SH, Audu PB, Sperling MR, et al. Reevalua-tion of surgery for the treatment of brain metasta-ses: review of 208 patients with single or multiple brain metastases treated at one institution with modern neurosurgical techniques. Neurosurgery 2005;56(5):1021–34.
75. Stark AM, Tscheslog H, Buhl R, et al. Surgical treatment for brain metastases: prognostic factors and survival in 177 patients. Neurosurg Rev 2005;28(2):115–9.
76. Muacevic A, Kreth FW, Horstmann GA, et al. Surgery and radiotherapy compared with gamma
knife radiosurgery in the treatment of solitary cere-bral metastases of small diameter. J Neurosurg 1999;91(1):35–43.
77. Kooy HM. Linear accelerators in stereotactic radiosurgery. In: Alexander 3rd E, Loeffler JS, Lunsford LD, editors. Stereotactic Radiosurgery. New York: McGraw-Hill; 1993. p. 67–76.
78. Chang Z, Wang Z, Wu QJ, et al. Dosimetric characteristics of Novalis Tx system with high definition multileaf collimator. Med Phys 2008;35(10):4460–3.
79. Hara W, Soltys SG, Gibbs IC. CyberKnife robotic radiosurgery system for tumor treatment. Expert Rev Anticancer Ther 2007;7(11):1507–15.
80. Wu A, Lindner G, Maitz AH, et al. Physics of gamma knife approach on convergent beams in stereotactic radiosurgery. Int J Radiat Oncol Biol Phys 1990;18(4):941–9.
81. Auchter RM, Lamond JP, Alexander 3rd E, et al. A multiinstitutional outcome and prognostic factor analysis of radiosurgery for resectable single brain metastasis. Int J Radiat Oncol Biol Phys 1996;35(1):27–35.
82. Flickinger JC, Kondziolka D, Lunsford LD, et al. A multi-institutional experience with stereotactic radiosurgery for solitary brain metastasis. Int J Radiat Oncol Biol Phys 1994;28(4):797–802.
83. Simonova G, Liscak R, Novotny Jr J, Novotny J. Solitary brain metastases treated with the Leksell gamma knife: prognostic factors for patients. Radiother Oncol 2000;57(2):207–13.
84. Deinsberger R, Tidstrand J. LINAC radiosurgery as single treatment in cerebral metastases. J Neu-rooncol 2006;76(1):77–83.
85. Flickinger JC, Lunsford LD, Somaza S, Kondziolka D. Radiosurgery: its role in brain metastasis management. Neurosurg Clin N Am 1996;7(3):497–504.
86. Fukuoka S, Seo Y, Takanashi M, et al. Radiosurgery of brain metastases with the Gamma Knife. Stereotact Funct Neurosurg 1996;66(Suppl. 1):193–200.
87. Gerosa M, Nicolato A, Foroni R, et al. Gamma knife radiosurgery for brain metastases: a primary therapeutic option. J Neurosurg 2002;97(Suppl. 5):515–24.
88. Goodman KA, Sneed PK, McDermott MW, et al. Relationship between pattern of enhancement and local control of brain metastases after radiosurgery. Int J Radiat Oncol Biol Phys 2001;50(1): 139–46.
89. Joseph J, Adler JR, Cox RS, Hancock SL. Linear accelerator-based stereotaxic radiosurgery for brain metastases: the influence of number of lesions on survival. J Clin Oncol 1996;14(4):1085–92.
90. Kihlstrom L, Karlsson B, Lindquist C. Gamma Knife surgery for cerebral metastases. Implications for survival based on 16 years experience. Stereo-tact Funct Neurosurg 1993;61(Suppl. 1):45–50.
91. Moriarty TM, Loeffler JS, Black PM, et al. Long-term follow-up of patients treated with stereotactic radiosurgery for single or multiple brain metasta-ses. In: Kondziolka D, editor. Radiosurgery 1995, vol. 1. Basel: Karger; 1996. p. 83–91.
92. Petrovich Z, Yu C, Giannotta SL, et al. Survival and pattern of failure in brain metastasis treated with stereotactic gamma knife radiosurgery. J Neu-rosurg 2002;97(Suppl. 5):499–506.
93. Pirzkall A, Debus J, Lohr F, et al. Radiosurgery alone or in combination with whole-brain radio-therapy for brain metastases. J Clin Oncol 1998;16(11):3563–9.
94. Sansur CA, Chin LS, Ames JW, et al. Gamma knife radiosurgery for the treatment of brain metastases. Stereotact Funct Neurosurg 2000;74(1):37–51.
95. Young RF. Radiosurgery for the treatment of brain metastases. Semin Surg Oncol 1998;14(1):70–8.
96. Shaw E, Scott C, Souhami L, et al. Single dose radiosurgical treatment of recurrent previously
irradiated primary brain tumors and brain metas-tases: final report of RTOG protocol 90–05. Int J Radiat Oncol Biol Phys 2000;47(2):291–8.
97. Shehata MK, Young B, Reid B, et al. Stereotatic radiosurgery of 468 brain metastases ≤2 cm: implications for SRS dose and whole brain radia-tion therapy. Int J Radiat Oncol Biol Phys 2004;59(1):87–93.
98. Schomas DA, Roeske JC, MacDonald RL, et al. Predictors of tumor control in patients treated with linac-based stereotactic radiosurgery for metastatic disease to the brain. Am J Clin Oncol 2005;28(2):180–7.
99. Sneed PK, Lamborn KR, Forstner JM, et al. Radio-surgery for brain metastases: is whole brain radio-therapy necessary? Int J Radiat Oncol Biol Phys 1999;43(3):549–58.
100. Chidel MA, Suh JH, Reddy CA, et al. Application of recursive partitioning analysis and evaluation of the use of whole brain radiation among patients treated with stereotactic radiosurgery for newly diagnosed brain metastases. Int J Radiat Oncol Biol Phys 2000;47(4):993–9.
101. Hasegawa T, Kondziolka D, Flickinger JC, et al. Brain metastases treated with radiosurgery alone: an alternative to whole brain radiotherapy? Neuro-surgery 2003;52(6):1318–26.
102. Wang LG, Guo Y, Zhang X, et al. Brain metastasis: experience of the Xi-Jing hospital. Stereotact Funct Neurosurg 2002;78(2):70–83.
103. Aoyama H, Shirato H, Tago M, et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: a randomized controlled trial. JAMA 2006;295(21):2483–91.
104. Serizawa T, Hirai T, Nagano O, et al. Gamma knife surgery for 1-10 brain metastases without prophylactic whole-brain radiation therapy: analy-sis of cases meeting the Japanese prospective multi-institute study (JLGK0901) inclusion criteria. J Neurooncol 2010;98(2):163–7.
105. Bindal AK, Bindal RK, Hess KR, et al. Surgery versus radiosurgery in the treatment of brain metastasis. J Neurosurg 1996;84(5): 748–54.
106. O’Neill BP, Iturria NJ, Link MJ, et al. A comparison of surgical resection and stereotactic radiosurgery in the treatment of solitary brain metastases. Int J Radiat Oncol Biol Phys 2003;55(5):1169–76.
107. Shiau C-Y, Sneed PK, Shu H-KG, et al. Radiosur-gery for brain metastases: relationship of dose and pattern of enhancement to local control. Int J Radiat Oncol Biol Phys 1997;37(2):375–83.
108. Bernstein M, Cabantog A, Laperriere N, et al. Brachytherapy for recurrent single brain metastasis. Can J Neurol Sci 1995;22(1):13–6.
109. Bogart JA, Ungureanu C, Shihadeh E, et al. Resec-tion and permanent I-125 brachytherapy without whole brain irradiation for solitary brain metastasis from non-small cell lung carcinoma. J Neurooncol 1999;44(1):53–7.
110. Huang K, Sneed PK, Kunwar S, et al. Surgical resection and permanent iodine-125 brachyther-apy for brain metastases. J Neurooncol 2009; 91(1):83–93.
111. McDermott MW, Cosgrove GR, Larson DA, et al. Interstitial brachytherapy for intracranial metasta-ses. Neurosurg Clin N Am 1996;7(3):485–95.
112. Ostertag CB, Kreth FW. Interstitial iodine-125 radiosurgery for cerebral metastases. Br J Neuro-surg 1995;9(5):593–603.
113. Rogers LR, Rock JP, Sills AK, et al. Results of a phase II trial of the GliaSite radiation therapy system for the treatment of newly diagnosed, resected single brain metastases. J Neurosurg 2006;105(3):375–84.
114. Ruge MI, Suchorska B, Maarouf M, et al. Stereo-tactic 125 iodine brachytherapy for the treatment
BrainMetastasesandNeoplasticMeningitis • CHAPTER50 738.e3
of singular brain metastases: closing a gap? Neuro-surgery 2011;68(5):1209.
115. Schulder M, Black PM, Shrieve DC, et al. Permanent low-activity iodine–125 implants for cerebral metastases. J Neurooncol 1997;33(3): 213–321.
116. Soffietti R, Costanza A, Laguzzi E, et al. Radio-therapy and chemotherapy of brain metastases. J Neurooncol 2005;75(1):31–42.
117. van den Bent MJ. The role of chemotherapy in brain metastases. Eur J Cancer 2003;39(15): 2114–20.
118. Soffietti R, Cornu P, Delattre JY, et al. EFNS Guidelines on diagnosis and treatment of brain metastases: report of an EFNS Task Force. Euro-pean Journal of Neurology 2006;13(7):674–81.
119. Grimm SA. Treatment of brain metastases: chemo-therapy. Curr Oncol Rep 2012;14(1):85–90.
120. Mehta MP, Paleologos NA, Mikkelsen T, et al. The role of chemotherapy in the management of newly diagnosed brain metastases: a systematic review and evidence-based clinical practice guideline. J Neurooncol 2010;96(1):71–83.
121. Cocconi G, Lottici R, Bisagni G, et al. Combina-tion therapy with platinum and etoposide of brain metastases from breast carcinoma. Cancer Invest 1990;8(3-4):327–34.
122. Franciosi V, Cocconi G, Michiara M, et al. Front-line chemotherapy with cisplatin and etoposide for patients with brain metastases from breast carci-noma, nonsmall cell lung carcinoma, or malignant melanoma. Cancer 1999;85(7):1599–605.
123. Newton HB, Slivka MA, Volpi C, et al. Intra-arterial carboplatin and intravenous etoposide for the treatment of metastatic brain tumors. J Neu-rooncol 2003;61(1):35–44.
124. Abrey LE, Olson JD, Raizer JJ, et al. A phase II trial of temozolomide for patients with recurrent or progressive brain metastases. J Neurooncol 2001;53(3):259–65.
125. Christodoulou C, Bafaloukos D, Kosmidis P, et al. Phase II study of temozolomide in heavily pre-treated cancer patients with brain metastases. Ann Oncol 2001;12(2):249–54.
126. Christodoulou C, Bafaloukos D, Linardou H, et al. Temozolomide (TMZ) combined with cispla-tin (CDDP) in patients with brain metastases from solid tumors: a Hellenic Cooperative Oncology Group (HeCOG) Phase II study. J Neurooncol 2005;71(1):61–5.
127. Caraglia M, Addeo R, Costanzo R, et al. Phase II study of temozolomide plus pegylated liposomal doxorubicin in the treatment of brain metastases from solid tumours. Cancer Chemother Pharma-col 2006;57(1):34–9.
128. Antonadou D, Paraskevaidis M, Sarris G, et al. Phase II randomized trial of temozolomide and concurrent radiotherapy in patients with brain metastases. J Clin Oncol 2002;20(17):3644–50.
129. Verger E, Gil M, Yaya R, et al. Temozolomide and concomitant whole brain radiotherapy in patients with brain metastases: a phase II randomized trial. Int J Radiat Oncol Biol Phys 2005;61(1): 185–91.
130. Malacarne P, Santini A, Maestri A. Response of brain metastases from lung cancer to systemic chemotherapy with carboplatin and etoposide. Oncology 1996;53(3):210–13.
131. Minotti V, Crino L, Meacci ML, et al. Chemotherapy with cisplatin and teniposide for cerebral metastases in non-small cell lung cancer. Lung Cancer 1998;20(2):93–8.
132. Bernardo G, Cuzzoni Q, Strada MR, et al. First-line chemotherapy with vinorelbine, gemcitabine, and carboplatin in the treatment of brain metasta-ses from non-small-cell lung cancer: a phase II study. Cancer Invest 2002;20(3):293–302.
133. Cortes J, Rodriguez J, Aramendia JM, et al. Front-line paclitaxel/cisplatin-based chemotherapy in
brain metastases from non-small-cell lung cancer. Oncology 2003;64(1):28–35.
134. Fujita A, Fukuoka S, Takabatake H, et al. Combi-nation chemotherapy of cisplatin, ifosfamide, and irinotecan with rhG-CSF support in patients with brain metastases from non-small cell lung cancer. Oncology 2000;59(4):291–5.
135. Dziadziuszko R, Ardizzoni A, Postmus PE, et al. Temozolomide in patients with advanced non-small cell lung cancer with and without brain metastases. A phase II study of the EORTC Lung Cancer Group (08965). Eur J Cancer 2003;39(9):1271–6.
136. Giorgio CG, Giuffrida D, Pappalardo A, et al. Oral temozolomide in heavily pre-treated brain metas-tases from non-small cell lung cancer: phase II study. Lung Cancer 2005;50(2):247–54.
137. Robinet G, Thomas P, Breton JL, et al. Results of a phase III study of early versus delayed whole brain radiotherapy with concurrent cisplatin and vinorelbine combination in inoperable brain metastasis of non-small-cell lung cancer: Groupe Francais de Pneumo-Cancerologie (GFPC) Proto-col 95-1. Ann Oncol 2001;12(1):59–67.
138. Guerrieri M, Wong K, Ryan G, et al. A randomised phase III study of palliative radiation with con-comitant carboplatin for brain metastases from non-small cell carcinoma of the lung. Lung Cancer 2004;46(1):107–11.
139. Cortot AB, Geriniere L, Robinet G, et al. Phase II trial of temozolomide and cisplatin followed by whole brain radiotherapy in non-small-cell lung cancer patients with brain metastases: a GLOT-GFPC study. Ann Oncol 2006;17(9):1412–17.
140. Barlesi F, Gervais R, Lena H, et al. Pemetrexed and cisplatin as first-line chemotherapy for advanced non-small-cell lung cancer (NSCLC) with asymp-tomatic inoperable brain metastases: a multicenter phase II trial (GFPC 07-01). Ann Oncol 2011;22(11):2466–70.
141. Twelves CJ, Souhami RL, Harper PG, et al. The response of cerebral metastases in small cell lung cancer to systemic chemotherapy. Br J Cancer 1990;61(1):147–50.
142. Korfel A, Oehm C, von Pawel J, et al. Response to topotecan of symptomatic brain metastases of small-cell lung cancer also after whole-brain irra-diation. a multicentre phase II study. Eur J Cancer 2002;38(13):1724–9.
143. Groen HJ, Smit EF, Haaxma-Reiche H, Postmus PE. Carboplatin as second line treatment for recur-rent or progressive brain metastases from small cell lung cancer. Eur J Cancer 1993;29A(12):1696–9.
144. Postmus PE, Smit EF, Haaxma-Reiche H, et al. Teniposide for brain metastases of small-cell lung cancer: a phase II study. European Organization for Research and Treatment of Cancer Lung Cancer Cooperative Group. J Clin Oncol 1995; 13(3):660–5.
145. Postmus PE, Haaxma-Reiche H, Smit EF, et al. Treatment of brain metastases of small-cell lung cancer: comparing teniposide and teniposide with whole-brain radiotherapy—a phase III study of the European Organization for the Research and Treat-ment of Cancer Lung Cancer Cooperative Group. J Clin Oncol 2000;18(19):3400–8.
146. Pietanza MC, Kadota K, Huberman K, et al. Phase II trial of temozolomide in patients with relapsed sensitive or refractory small cell lung cancer, with assessment of methylguanine-DNA methyltrans-ferase as a potential biomarker. Clin Cancer Res 2012;18(4):1138–45.
147. Chang J, Atkinson H, A’Hern R, et al. A phase II study of the sequential administration of dacarba-zine and fotemustine in the treatment of cerebral metastases from malignant melanoma. Eur J Cancer 1994;30A(14):2093–5.
148. Jacquillat C, Khayat D, Banzet P, et al. Final report of the French multicenter phase II study of the
nitrosourea fotemustine in 153 evaluable patients with disseminated malignant melanoma including patients with cerebral metastases. Cancer 1990; 66(9):1873–8.
149. Mornex F, Thomas L, Mohr P, et al. [Randomised phase III trial of fotemustine versus fotemustine plus whole brain irradiation in cerebral metastases of melanoma]. Cancer Radiotherapie 2003;7(1): 1–8.
150. Agarwala SS, Kirkwood JM, Gore M, et al. Temo-zolomide for the treatment of brain metastases associated with metastatic melanoma: a phase II study. J Clin Oncol 2004;22(11):2101–7.
151. Strauss SJ, Marples M, Napier MP, et al. A phase I (tumour site-specific) study of carboplatin and temozolomide in patients with advanced mela-noma. Br J Cancer 2003;89(10):1901–5.
152. Margolin K, Atkins B, Thompson A, et al. Temo-zolomide and whole brain irradiation in melanoma metastatic to the brain: a phase II trial of the Cyto-kine Working Group. J Cancer Res Clin Oncol 2002;128(4):214–18.
153. Rosner D, Nemoto T, Lane WW. Chemotherapy induces regression of brain metastases in breast carcinoma. Cancer 1986;58(4):832–9.
154. Boogerd W, Dalesio O, Bais EM, van der Sande JJ. Response of brain metastases from breast cancer to systemic chemotherapy. Cancer 1992;69(4): 972–80.
155. Lin NU, Eierman W, Greil R, et al. Randomized phase II study of lapatinib plus capecitabine or lapatinib plus topotecan for patients with HER2-positive breast cancer brain metastases. J Neuroon-col 2011;105(3):613–20.
156. Arslan C, Dizdar O, Altundag K. Systemic treatment in breast-cancer patients with brain metastasis. Expert Opinion on Pharmacotherapy 2010;11(7):1089–100.
157. Ekenel M, Hormigo AM, Peak S, et al. Dramatic regression of multiple brain metastases from breast cancer with Capecitabine: another arrow at the bow? J Neurooncol 2006;24(4):223–7.
158. Fabi A, Vidiri A, Ferretti G, et al. Dramatic regres-sion of multiple brain metastases from breast cancer with Capecitabine: another arrow at the bow? Cancer Invest 2006;24(4):466–8.
159. Wang MLH, Yung WK, Royce ME, et al. Capecitabine for 5-fluorouracil-resistant brain metastases from breast cancer. Am J Clin Oncol 2001;24(4):421–4.
160. Preusser M, Capper D, Ilhan-Mutlu A, et al. Brain metastases: pathobiology and emerging targeted therapies. Acta Neuropathologica 2012;123(2): 205–22.
161. De Braganca KC, Janjigian YY, Azzoli CG, et al. Efficacy and safety of bevacizumab in active brain metastases from non-small cell lung cancer. J Neurooncol 2010;100(3):443–7.
162. Gore ME, Hariharan S, Porta C, et al. Sunitinib in metastatic renal cell carcinoma patients with brain metastases. Cancer 2011;117(3):501–9.
163. Stadler WM, Figlin RA, McDermott DF, et al. Safety and efficacy results of the advanced renal cell carcinoma sorafenib expanded access program in North America. Cancer 2010;116(5):1272–80.
164. Grommes C, Oxnard GR, Kris MG, et al. “Pulsa-tile” high-dose weekly erlotinib for CNS metasta-ses from EGFR mutant non-small cell lung cancer. Neurooncology 2011;13(12):1364–9.
165. Lin NU, Diéras V, Paul D, et al. Multicenter phase II study of lapatinib in patients with brain metastases from HER2-positive breast cancer. Clin Cancer Res 2009;15(4):1452–9.
166. Margolin K, Ernstoff MS, Hamid O, et al. Ipilim-umab in patients with melanoma and brain metas-tases: an open-label, phase 2 trial. Lancet Oncol 2012;13(5):459–65.
167. Sundaresan N, Galicich JH, Deck MDF, Tomita T. Radiation necrosis after treatment of solitary intra-
PartII:ProblemsCommontoCancerandItsTherapy738.e4
cranial metastases. Neurosurgery 1981;8(3): 329–33.
168. Cooper JS, Steinfeld AD, Lerch IA. Cerebral metastases: value of reirradiation in selected patients. Radiology 1990;174(3 Pt 1):883–5.
169. Hazuka MB, Kinzie JJ. Brain metastases: results and effects of re-irradiation. Int J Radiat Oncol Biol Phys 1988;15(2):433–7.
170. Kurup P, Reddy S, Hendrickson FR. Results of re-irradiation for cerebral metastases. Cancer 1980;46(12):2587–9.
171. Wong WW, Schild SE, Sawyer TE, Shaw EG. Analysis of outcome in patients reirradiated for brain metastases. Int J Radiat Oncol Biol Phys 1996;34(3):585–90.
172. Chamberlain M. Neoplastic meningitis: a guide to diagnosis and treatment. Curr Opin Neurol 2000;13(6):641–8.
173. Grossman SA, Krabak MJ. Leptomeningeal carci-nomatosis. Cancer Treat Rev 1999;25(2):103–19.
174. National Comprehensive Cancer Network. Lepto-meningeal metastases (version 2.2013). Accessed 4/27/2013. http://www.nccn.org/professionals/physician_gls/pdf/cns.pdf.
175. Jayson GC, Howell A. Carcinomatous meningitis in solid tumors. Ann Oncol 1996;7(8):773–86.
176. Posner JB. Neurologic complications of cancer. Philadelphia: F. A. Davis Company; 1995.
177. Kesari S, Batchelor TT. Leptomeningeal metasta-ses. Neurologic Clinics 2003;21(1):25–66.
178. DeAngelis LM. Current diagnosis and treatment of leptomeningeal metastasis. J Neurooncol 1998;38(2-3):245–52.
179. Pavlidis N. The diagnostic and therapeutic man-agement of leptomeningeal carcinomatosis. Ann Oncol 2004;15(Suppl 4):285–91.
180. Schold SC, Wasserstrom WR, Fleisher M, et al. Cerebrospinal fluid biochemical markers of central
nervous system metastases. Ann Neurol 1980;8(6): 597–604.
181. Gleissner B, Chamberlain MC. Neoplastic menin-gitis. Lancet Neurol 2006;5(5):443–52.
182. Bleyer WA, Poplack DG. Intraventricular versus intralumbar methotrexate for central-nervous- system leukemia: prolonged remission with the Ommaya reservoir. Med Pediatr Oncol 1979; 6(3):207–13.
183. Grossman SA, Trump DL, Chen DC, et al. Cerebrospinal fluid flow abnormalities in patients with neoplastic meningitis. An evaluation using 111indium-DTPA ventriculography. Am J Med 1982;73(5):641–7.
184. Blaney SM, Balis FM, Berg S, et al. Intra-thecal mafosfamide: a preclinical pharmacology and phase I trial. J Clin Oncol 2005;23(7): 1555–63.
185. Blaney SM, Heideman R, Berg S, et al. Phase I clinical trial of intrathecal topotecan in patients with neoplastic meningitis. J Clin Oncol 2003; 21(1):143–7.
186. Chamberlain MC, Tsao-Wei DD, Groshen S. Phase II trial of intracerebrospinal fluid etoposide in the treatment of neoplastic meningitis. Cancer 2006;106(9):2021–7.
187. Chamberlain MC. A phase II trial of intra-cerebrospinal fluid alpha interferon in the treat-ment of neoplastic meningitis. Cancer 2002; 94(10):2675–80.
188. Nakagawa H, Miyahara E, Suzuki T, et al. Continuous intrathecal administration of 5-fluoro-2′-deoxyuridine for the treatment of neoplastic meningitis. Neurosurgery 2005;57(2):266–80.
189. Glantz MJ, Cole BF, Recht L, et al. High- dose intravenous methotrexate for patients with nonleukemic leptomeningeal cancer: is intrathecal
chemotherapy necessary? J Clin Oncol 1998; 16(4):1561–7.
190. Rubenstein JL, Combs D, Rosenberg J, et al. Rituximab therapy for CNS lymphomas: targeting the leptomeningeal compartment. Blood 2003; 101(2):466–8.
191. Petzer AL, Gunsilius E, Hayes M, et al. Low con-centrations of STI571 in cerebrospinal fluid: a case report. Br J Haematol 2002;117(3):623–5.
192. Laske DW, Muraszko KM, Oldfield EH, et al. Intraventricular immunotoxin therapy for lepto-meningeal neoplasia. Neurosurgery 1997;41(5): 1039–51.
193. Rubenstein JL, Fridlyand J, Abrey L, et al. Phase I study of intraventricular administration of ritux-imab in patients with recurrent CNS and intraocu-lar lymphoma. J Clin Oncol 2007;25(11): 1350–6.
194. Coakham HB, Kemshead JT. Treatment of neo-plastic meningitis by targeted radiation using (131)I-radiolabelled monoclonal antibodies. Results of responses and long term follow-up in 40 patients. J Neurooncol 1998;38(2-3):225–32.
195. Stemmler HJ, Schmitt M, Harbeck N, et al. Appli-cation of intrathecal trastuzumab (Herceptintrade mark) for treatment of meningeal carcinomatosis in HER2-overexpressing metastatic breast cancer. Oncol Rep 2006;15(5):1373–7.
196. Platini C, Long J, Walter S. Meningeal carcinoma-tosis from breast cancer treated with intrathecal trastuzumab. Lancet Oncol 2006;7(9):778–80.
197. Oliveira M, Braga S, Passos-Coelho JL, et al. Complete response in HER2+ leptomeningeal carcinomatosis from breast cancer with intrathecal trastuzumab. Breast Cancer Res Treat 2011; 127(3):841–4.