-
8/9/2019 8.Chest Trauma
1/51
Editors: Collins, Jannette; Stern, Eric J.
Title: Chest Radiology: The Essentials, 2nd Edition
Copyright 2008 Lippincott Williams & Wilkins
> Table of Contents > Chapter 8 - Chest Trama
Chapter 8Chest Trauma
Learning Objectives
!" #$entify a %i$ene$ me$iastinm on a posttramachest ra$iograph
an$ state the $ifferential $iagnosisincl$ing aortic'arterial in(ry)
*enos in(ry) an$fractre of sternm or thoracic spine+"
2" #$entify an$ $escribe the in$irect an$ $irect signs ofaortic
in(ry on contrast-enhance$ chest compte$tomography CT+"
," #$entify) $escribe the featres of) an$ state thesignificance
of chronic tramatic pse$oanerysm ofthe aorta on a chest ra$iograph)
CT) or magneticresonance imaging"
" #$entify fractre$ ribs) cla*icle) spine) sternm) an$scapla on
a chest ra$iograph or CT"
." /ame fi*e common cases of abnormal lngopacification on a
posttrama chest ra$iograph or CT"
" #$entify an abnormally positione$ $iaphragm or lossof
$efinition of a $iaphragm on a posttrama chestra$iograph an$ sggest
the $iagnosis of rptre$$iaphragm"
1" ecogni3e an$ $escribe the signs of $iaphragmaticrptre on a
chest CT"
8" #$entify pnemothora4) pnemopericar$im) an$
pnemome$iastinm on a chest ra$iograph or CT"5" #$entify the
fallen lng sign on a chest ra$iograph or
-
8/9/2019 8.Chest Trauma
2/51
CT an$ sggest the $iagnosis of tracheobronchialtear"
!0" #$entify a ca*itary lesion on a posttrama chestra$iograph or
CT an$ sggest the $iagnosis of
laceration %ith pnematocele formation"!!" ecogni3e an$
$istingish bet%een laceration an$
contsion on a chest ra$iograph or CT"
6ach year in the 7nite$ tates) more than ,00)000patients are
hospitali3e$ an$ 2.)000 people $ie as a$irect reslt of chest trama
!+" Thoracic in(ry accontsfor 2.9 of all tramatic $eaths) an$
sbstantial chesttrama is a factor in .09 of fatal traffic acci$ents
2+":ost of the chest trama seen in ci*ilian poplations isblnt chest
trama 509+) sally a reslt of motor*ehicle crashes an$ falls ,+" The
inci$ence of penetratingtrama is stabili3ing or $ecreasing) an$
many penetrating%on$s to the chest can be treate$ by tbe
thoracostomyalone +"
;fter a patient has been clinically e*alate$ an$stabili3e$) a
chest ra$iograph is sally obtaine$" Thesera$iographs are often
compromise$ by limite$ e4posrecapability) lo% lng *olmes) poor or
absent patientcooperation) obscration of thoracic anatomy by
portionsof e4ternal monitoring an$ spport $e*ices o*erlying
thepatient) sboptimal patient positioning) an$ magnificationan$
$istortion of the me$iastinm" #n one st$y)
compte$ tomography CT+ %as sperior to spine chestra$iography in
sho%ing fin$ings of chest trama) an$ theCT fin$ings inflence$
patient management in asignificant nmber of patients .+" This
chapter re*ie%sthe chest ra$iographic an$ CT fin$ings of blnt trama
tothe chest"
Aortic and reat !essel "njur#
Tramatic rptre of the aorta alone acconts for !9 offatalities
reslting from motor *ehicle crashes) an$ 8.9
-
8/9/2019 8.Chest Trauma
3/51
to 509 of patients %ith tramatic aortic rptre $iebefore reaching
a me$ical facility +" #n clinical series)509 of aortic rptres occr
at the aortic isthms) (st$istal to the origin of the left sbcla*ian
artery 1)8)5)!0+
-
8/9/2019 8.Chest Trauma
4/51
lympha$enopathy) an$ persistent left-si$e$ sperior *enaca*a
!2+"
=otential pitfalls in CT interpretation incl$ehemome$iastinm
case$ by sternal or *ertebral bo$y
fractre) left pleral effsion %ith left lo%er lobesbsegmental
atelectasis ?@srron$ing? the aorta)plsation artifacts)
atherosclerotic plaAes) prominent$cts arterioss) an$ pse$ointimal
flaps secon$ary to*olme a*eraging of the left brachiocephalic
*ein
as it crosses in front of the aortic arch" These pitfallsha*e
become less of a problem %ith the se of
mlti$etector CT an$ fast scanning techniAes"
="!2
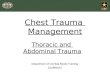
$"%&E '(). Aortic laceration. A:;nteroposterior
;=+ spine chest ra$iograph of a yong %oman aftera motor *ehicle
crash sho%s nonspecific %i$ening ofthe me$iastinm" *:;ortogram
sho%s aorticlaceration at the aortic isthms arrow+) the mostcommon
site of aortic in(ry in patients %ho sr*i*e toreach a me$ical
facility" eprinte$ %ith permissionfrom Collins B" Chest trama
imaging in the intensi*ecare nit" Respir Care.
!555!5+D!0?E!0,"+
-
8/9/2019 8.Chest Trauma
5/51
-
8/9/2019 8.Chest Trauma
6/51
%eeks to months to resol*e) sometimes %ith resi$alscarring
-
8/9/2019 8.Chest Trauma
7/51
TA*LE '() CEST &A-"O&A+"CS"S O$ AO&T"C "J%&/
Wi$ening of the me$iastinmFbscration of the aortic arch;bnormal
aortic contorJemothora4ib fractresTracheal shift to the rightLeft
apical cap
Kepression of the left mainstem bronchs belo%
0$egrees/asogastric tbe $isplacement to the
right=nemothora4=lmonary contsionWi$ene$ left paraspinos line
-
8/9/2019 8.Chest Trauma
8/51
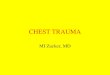
$"%&E '(0. -escending aortic laceration. A:;=spine chest
ra$iograph sho%s $iffse opacity of bothhemithoraces" *:CT image
sho%s periaortichematoma H+ an$ irreglar contor of the
$escen$ingaorta arrow+" Coronal 1C2an$ sagittal 1-2reformatte$ CT
images sho% a pse$oanerysm of the$escen$ing aorta arrows+"
-
8/9/2019 8.Chest Trauma
9/51
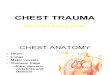
$"%&E '(3. 4ediastinal hematoma. A:;= spine
chest ra$iograph of a patient in*ol*e$ in a motor*ehicle crash
sho%s nonspecific %i$ening of theme$iastinm" *:CT scan sho%s bloo$
in theme$iastinm H+" /ote the preser*ation of a fat planebet%een
the me$iastinal bloo$ an$ the normal aorta)%hich in the absence of
sternal or spine fractrein$icates that the blee$ing %as *enos an$
notarterial"
-
8/9/2019 8.Chest Trauma
10/51
$"%&E '(5. Aortic laceration. A:;= spine chest
ra$iograph of a patient in*ol*e$ in a motor *ehiclecrash sho%s a
%i$e me$iastinm an$ an abnormalaortic contor" The trachea is
$isplace$ to the right"*:CT scan sho%s bloo$ srron$ing the aorta)
along%ith $isrption of the aorta at the le*el of the isthmsarrow+"
C:agittal reformatte$ CT sho%s an aorticpse$oanerysm arrows+"
-
8/9/2019 8.Chest Trauma
11/51
$"%&E '(6. 4ediastinal 7at. A:CT chest scot *ie%sho%s a %i$e
me$iastinm" *:;4ial CT sho%sabn$ant me$iastinal fat F+) some normal
lymph
no$es) an$ no aortic in(ry or me$iastinal mass"
$"%&E '(8. Lung laceration. A:;= spine chestra$iograph of a
patient in*ol*e$ in a motor *ehicle
crash sho%s a %i$e pper me$iastinm an$ lack of$efinition of the
aortic arch" *:CT sho%s airspaceopacity %ith central lcency)
consistent %ith lacerationan$ pnematocele formation) a$(acent to
the pperme$iastinm arrow+"
-
8/9/2019 8.Chest Trauma
12/51
Tracheobronchial "njur#The inci$ence of tracheobronchial in(ry
TH#+ is reporte$as 0"9 to !".9 in clinical series of ma(or blnt
trama
2.+" Hlnt trama mst be se*ere to case air%ayrptre) an$ in(ry to
other strctres sch as thethoracic cage) lngs) an$ great *essels is
likely" When theintrathoracic trachea or bronchi are in(re$) the
aorta isthe most commonly associate$ in(re$ strctre 2+" TH#is
associate$ %ith a ,09 o*erall mortality
rate) mostly from associate$ in(ries 21+"
-
8/9/2019 8.Chest Trauma
13/51
$"%&E '('. Concurrent subclavian arter# and
aortic injuries. A:;= spine chest ra$iograph of apatient
in*ol*e$ in a motor *ehicle crash sho%s a %i$epper me$iastinm
arrows+ an$ left%ar$ shift of thetrachea" *:CT scan sho%s
me$iastinal hematoma H+an$ pse$oanerysm of the right sbcla*ian
arteryarrow+" C:Coronal reformatte$ CT scan sho%s a rightsbcla*ian
artery pse$oanerysm arrow+ (stbeyon$ its origin from the right
brachiocephalic
artery" -:; more posterior coronal reformatte$ imagesho%s an
acte laceration of the aorta arrow+"
-
8/9/2019 8.Chest Trauma
14/51
$"%&E '(. +ulmonar# contusion. A:CT scan of a
-year-ol$ boy after a motor *ehicle crash sho%sbilateral
peripheral areas of airspace opacity) anopacifie$ accessory a3ygos
lobe) an$ a rightpnemothora4" *:CT at a le*el inferior to
1A2sho%sbilateral peripheral) nonsegmental areas of airspaceopacity
typical of plmonary contsions" eprinte$%ith permission from Collins
B" Chest trama imagingin the intensi*e care nit" Respir
Care.!555!
5+D!0?E!0,"+
-
8/9/2019 8.Chest Trauma
15/51
$"%&E '()
-
8/9/2019 8.Chest Trauma
16/51
arrows+) representing resi$al scarring"
$"%&E '()). +ulmonar# laceration.CT scan of apatient
in*ol*e$ in a motor *ehicle crash sho%s $enseopacity in the right
lng %ith central lcenciesarrows+) consistent %ith laceration an$
pnematocele
formation an$ srron$ing hemorrhage" /ote a largeright
pnemothora4 P+"
$"%&E '()0. +ulmonar# laceration.CT scan sho%s
a lo%-$ensity area %ith an air?Efli$ le*el in the
rightpara*ertebral area arrow+) typical of a shearing type
-
8/9/2019 8.Chest Trauma
17/51
ptre of the cer*ical trachea may occr as a?@clothesline in(ry?
%hen the neck is e4ten$e$ onhigh-spee$ contact %ith ropes) %ires)
or cables byin$i*i$als ri$ing many types of recreational *ehicles
orrnning" Tracheal laceration may also occr in a motor*ehicle crash
%hen the neck of a $ri*er strikes the top ofthe steering %heel)
compressing the air%ay against the
of plmonary laceration" This shol$ not be confse$%ith a loclate$
pnemothora4"
$"%&E '()3. $at emboli=ation s#ndrome. A:;=spine chest
ra$iograph of a yong %oman shortlyafter a motor *ehicle crash sho%s
clear lngs" The
patient sstaine$ mltiple long bone fractres thatreAire$ open
re$ction an$ internal fi4ation" /ote thehigh position of the
en$otracheal tbe arrow+" *:;=spine chest ra$iograph obtaine$ 12
hors later sho%sbilateral airspace opacities) %ith a perihilar
an$basilar pre$ominance) an$ sparing of the lng apices"eprinte$
%ith permission from Collins B" Chesttrama imaging in the intensi*e
care nit" Respir
Care.!555 !5+D!0?E!0,"+
-
8/9/2019 8.Chest Trauma
18/51
spine"
=athologically) tracheal in(ry most commonly presents asa
trans*erse tear bet%een the tracheal rings or a
longit$inal tear in the posterior membranos segment"Complete
separation of the trachea may occr) bt air%aycontinity can still be
maintaine$ by peritracheobronchialtisse" #n(ry to the me$iastinal
trachea or ma(or bronchipro$ces
pnemome$iastinm that rapi$ly e4ten$s into the neckan$ face)
shol$ers) an$ chest %all
-
8/9/2019 8.Chest Trauma
19/51
%ith rib fractres" =nemothora4 is seen in 09 to !009of cases of
TH# ,0+) bt it may not be present if theoter a$*entitial slee*e of
the bronchs remains intactan$ there is no air leak ,!+" #n most
cases)
pnemothoraces %ill respon$ to chest tbe placement)
sore-e4pansion of the lng $oes not e4cl$etracheobronchial in(ry"
Jo%e*er) a pnemothora4 that$oes not resol*e %ith fnctioning tbe
$rainage is thesine Aa non of me$iastinal air%ay in(ry ,2+"
$"%&E '()6. Acute tracheal injur#. A:CT scan ofa patient
in*ol*e$ in a motor *ehicle crash sho%s anen$otracheal tbe %ithin
the trachea solid arrow+ an$a cr*ilinear collection of air
posterior to the trachea
dashed arrows+" *:CT scan at a more inferior le*el
-
8/9/2019 8.Chest Trauma
20/51
;n in$ication of tracheal tear is ele*ation of the hyoi$bone
abo*e the le*el of C,) as seen on a lateralra$iograph of the
cer*ical spine ,,+" This occrs as areslt of in(re$ infrahyoi$
msclatre) casingnoppose$ ele*ation of the hyoi$ bone by
sprahyoi$msclatre" ;nother sign of tracheal transection is
acteo*er$istension of the en$otracheal tbe cff) to the point%here
it e4cee$s the normal $iameter of the trachea
-
8/9/2019 8.Chest Trauma
21/51
!19 to 09 ha*e highly sggesti*e ra$iographic fin$ings)1)8+"
Chest ra$iographic fin$ings of rptre incl$ea normal appearing
$iaphragm) pnemothora4)
$isplacement of stomach) li*er) spleen) colon) or smallbo%el
into the thora4
-
8/9/2019 8.Chest Trauma
22/51
-
8/9/2019 8.Chest Trauma
23/51
C:CT at a le*el inferior to 1*2sho%spnemome$iastinm) %ith air
otlining the aorta)sperior *ena ca*a) plmonary artery) an$
thyms"
$"%&E '()'. $allen lung sign. CT of a patient %ithan acte
tramatic fractre of the right main bronchssho%s a large right
pnemothora4 P+) a right chest
tbe arrow+) an$ collapse$ ?@fallen right lng?
FL+ positione$ in the posterior an$ lateral righthemithora4"
/ormally %ith pnemothora4) thecollapse$ lng recoils in%ar$ to%ar$
the hilm"
$"%&E '(). $ractured bronchus intermedius.CT
-
8/9/2019 8.Chest Trauma
24/51
of a yong %oman in*ol*e$ in a motor *ehicle crashsho%s leakage
of air from a fractre$ bronchsinterme$is to the pleral space
arrows+ an$
me$iastinm arrowheads+) reslting in pnemothora4an$
pnemome$iastinm) respecti*ely" eprinte$%ith permission from Collins
B" Chest trama imagingin the intensi*e care nit" Respir
Care.!555!5+D!0?E!0,+"
$"%&E '(0
-
8/9/2019 8.Chest Trauma
25/51
$"%&E '(0). -iahragm ruture.;= spine chestra$iograph of a
patient in*ol*e$ in a motor *ehiclecrash sho%s a mass in the left
lo%er hemithora4representing herniate$ non?Eair-fille$
stomach)sperior $isplacement of an intragastric nasogastrictbe
arrow+) an$ right%ar$ shift of the me$iastinm"
TA*LE '(0 &A-"OLO"C $"-"SO$ -"A+&A4 &%+T%&E
Findings on chest radiographyKisplacement of stomach) li*er)
spleen) colon) or
small bo%el into the thora4perior $isplacement of an
intragastric
nasogastric tbe#psilateral pleral effsionHasilar opacity casing
inability to *isali3e the
$iaphragm#rreglar or lmpy $iaphragm contor
-
8/9/2019 8.Chest Trauma
26/51
Kirect signsDKiaphragmatic $iscontinity#ntrathoracic herniation
of ab$ominal contents
Waistlike constriction of bo%el ?@collarsign? +
Kepen$ent *iscera sign#n$irect signsD
Li*er lacerationJemoperitonemJemothora4plenic lacerationenal
contsionLo%er lobe atelectasisLo%er rib fractres
="!,
$"%&E '(00. %nreaired diahragm ruture. A:
-
8/9/2019 8.Chest Trauma
27/51
:lti$etector CT has been sho%n to be sefl in makingthe $iagnosis
of acte $iaphragm rptre) an$ it issperior to con*entional CT becase
*olmetric $ataacAisition pro*i$es high-Aality sagittal an$
coronalreconstrctions" ;cAisition of $ata $ring a singlebreath-hol$
$ecreases slice misregistration .0+"#n$i*i$al $iagnostic
sensiti*ity for $etecting
$iaphragmatic rptre on CT scanning is .9 to 1,9)an$ specificity
is 89 to 509 .!+" :ost in(ries in*ol*ethe posterolateral aspect of
the $iaphragm" Kirect CTfin$ings associate$ %ith acte rptre
incl$e$iaphragmatic $iscontinity
-
8/9/2019 8.Chest Trauma
28/51
normal increase in $iaphragmatic $efects %ith age that isnot
relate$ to trama .,+
-
8/9/2019 8.Chest Trauma
29/51
-
8/9/2019 8.Chest Trauma
30/51
-
8/9/2019 8.Chest Trauma
31/51
conseAence"
+leural 4ani7estations o7 ChestTrauma=nemothora4 is seen on
chest ra$iography in almost09 of patients %ith blnt chest trama an$
in p to209 of patients %ith penetrating chest in(ries .5)0+"The
most common case in blnt t rama is assme$ to bea rib fractre that
penetrates the *isceral pleraho%e*er) pnemothora4 in the absence of
rib fractres isoccasionally seen in a$lts an$ is commonly seen
inchil$ren" =leral air %ill rise to the most non$epen$entportion of
the thora4D at the ape4 in the pright patientan$ at the anterior)
ca$al aspect of the pleral space inthe spine patient" a$iographic
signs of pnemothora4in the spine patient incl$e a+ the $eep slcs
sign)%hich is a $eep) lcent costophrenic slcs
-
8/9/2019 8.Chest Trauma
32/51
an$ posterior aspects of the hemi$iaphragm" CT is mchmore
sensiti*e for $iagnosing pnemothora4 in the spinepatient than is
chest ra$iography !)2+ an$ i$entifiespnemothoraces that cannot be
seen on con*entional
spine ra$iographs in !09 to .09 of patients %ho ha*esstaine$
blnt trama to the chest !)2),+"
$"%&E '(08. &ib 7ractures and 7lail chest. CT of
apatient in*ol*e$ in a motor *ehicle crash sho%s aloclate$ right
hemothora4) right chest %allhematoma) an$ nmeros fractre$ right
ribs"
-
8/9/2019 8.Chest Trauma
33/51
=nemome$iastinm may occr in association %ithpnemothora4" #t can
be $iagnose$ on chest ra$iographsby the
presence of abnormal lcencies in the me$iastinm thathighlight
the contors of the aorta an$ plmonary arteryan$ $isplace the
me$iastinal plera laterally) an$ by the?@continos $iaphragm sign)?
%hich is pro$ce$ bythe presence of air bet%een the pericar$im an$
the$iaphragm" =nemome$iastinm can be easily i$entifie$on chest CT
an$ may signal the presence of an n$erlyinglaceration of the
pharyn4) esophags) or tracheobronchial
air%ay"
$"%&E '(09. Sternal 7racture.CT sho%s acomminte$ fractre of
the sternm arrow+ an$retrosternal hematoma H+" /ote preser*ation of
the
fat plane bet%een the hematoma an$ the great*essels"
="!,
$"%&E '(0'. Sternal 7racture.agittal reformatte$CT sho%s a
fractre of the sternm arrow+ an$posterior $isplacement of the
inferior fractre
fragment from the manbrim"
-
8/9/2019 8.Chest Trauma
34/51
=leral effsions that $e*elop in the acte posttramaticsetting
sally represent hemothora4) an$ a rapi$lye4pan$ing pleral effsion
is most likely to be case$ byarterial blee$ing" CT can be helpfl in
$istingishinghematoma from other pleral collections by sho%ing
thehigh CT attenation of bloo$ +
-
8/9/2019 8.Chest Trauma
35/51
$"%&E '(3
-
8/9/2019 8.Chest Trauma
36/51
-
8/9/2019 8.Chest Trauma
37/51
Cardiac TraumaThe heart an$ pericar$im are fairly %ell protecte$
fromnonpenetrating in(ry) an$ $ocmente$ tramatic in(ryis ncommon"
The chest ra$iograph plays a relati*elyminor role in the e*alation
of myocar$ial in(ry" #tsgreatest *ale is in $etecting associate$
in(ries) sch as
rib fractres) sternal fractres) an$ plmonary contsion"
ra$iograph sho%s a large left apical) lateral) an$basilar
pnemothora4 an$ associate$ right%ar$ shiftof the me$iastinm"
$"%&E '(33. -ee sulcus sign" ;= spine chestra$iograph sho%s
a large left basilar pnemothora4arrows+ $espite a left chest tbe"
This case illstratesthe importance of incl$ing the entire lng base
on
spine chest ra$iographs" Fther%ise) the presence orsi3e of a
large basilar pnemothora4 may not be
-
8/9/2019 8.Chest Trauma
38/51
api$ accmlation of bloo$ in the pericar$ial space cancase
car$iac tampona$e an$ se*ere hemo$ynamiccompromise" He$si$e
sonographic e*alation of the heartis the metho$ of choice to Aickly
an$ nonin*asi*ely$etect pericar$ial fli$" CT is also *ery sensiti*e
for
$etecting pericar$ial fli$ an$ may in$icate
pericar$ialhemorrhage) as $etermine$ by the high CT attenation
ofthe fli$
-
8/9/2019 8.Chest Trauma
39/51
*al*e apparats can reslt in congesti*e heart failre":itral
regrgitation from the latter may case asymmetricplmonary e$ema)
classically of the right pper lobe as areslt of the $irection of
the regrgitant (et"
=nemopericar$im can occr %hen air enters throgh apericar$ial
$isrption in the presence of pnemothora4
-
8/9/2019 8.Chest Trauma
40/51
Car$iac contsion may reslt from blnt chest trama in89 to 19 of
patients .)+" The $iagnosis is sallyma$e from electrocar$iography)
nclear car$iac imaging)or echocar$iography" The right *entricle is
the mostfreAently in(re$) as it comprises almost three timesmore
e4pose$ anterior srface of the heart than $oes theleft *entricle
!+" Chest ra$iography an$ CT can sho%seAelae of car$iac contsion)
sch as congesti*e heartfailre) *entriclar anerysm) or massi*e
car$iacenlargement"
Esohageal "njur#6sophageal tears are more common in patients
%ithpenetrating trama an$ occr in fe%er than !9 of blnttrama cases
1+" Thoracic esophageal tears fromtrama are case$ almost e4clsi*ely
by gnshot %on$s!+" 6sophageal $isrption can occr from crshing ofthe
esophags bet%een the spine an$ trachea) traction
from hypere4tension) an$ $irect penetration by cer*icalspine
fractre fragments 8+" :ost tears occr in thecer*ical an$ pper
thoracic esophags) bt they also mayoccr (st abo*e the
gastroesophageal (nction" Thethoracic esophags lies to the left of
the trachea at thethoracic inlet bt mo*es to the right as it
passesposterior to the aortic arch at the le*el of the carina"
Theesophags crosses back to the left as it enters the
stomach" ;ccor$ingly) rptres of the mi$- to $istalesophags sally
present %ith a right-si$e$ pleral
chest ra$iograph of a patient in*ol*e$ in a motor*ehicle crash
sho%s air srron$ing the heart P+"/ote right pnemothora4) bilateral
parenchymal
opacification) an$ bilateral sbctaneos emphysema"*:CT sho%s
pnemopericar$im P+) bilateralpnemothoraces) pnemome$iastinm)
pleraleffsion) an$ sbctaneos emphysema"
-
8/9/2019 8.Chest Trauma
41/51
effsion) an$ effsions case$ by rptre at thegastroesophageal
(nction occr more commonly on theleft"
Chest ra$iography in patients %ith esophageal rptrecan sho%
persistent se*ere pnemome$iastinm orpnemothora4) pleral effsion) a
%i$ene$ paraspinalline) an$ retrocar$iac lng opacification" CT
scans cansho% similar fin$ings) in a$$ition to leakage of
oralcontrast from the $isrpte$ esophags into theme$iastinm or
pleral space an$ changes ofme$iastinitis" The areas of greatest
esophageal
thickening on CT often
$"%&E '(39. *roncho(leural(cutaneous 7istula.
A:;= pright chest ra$iograph of a 25-year-ol$ manin*ol*e$ in a
motor *ehicle crash sho%s mltiple rightrib fractres creating a
?@flail chest)? pleralopacification consistent %ith hemothora4)
opacificationof the right lng from parenchymal in(ry) an$nmeros
collections of air %ithin the soft tisses ofthe right chest %all
arrows+" *:CT sho%scommnication bet%een the air%ays an$ chest
%allhematoma arrows+" eprinte$ %ith permission fromCollins B" Chest
trama imaging in the intensi*e carenit" Respir Care.!555
!5+D!0?E!0,"+
-
8/9/2019 8.Chest Trauma
42/51
represent the le*el of perforation" The perforation
itself)ho%e*er) may be obscre$ by e$ema) an$ hemorrhagean$ is sally
not *isali3e$" The $iagnosis is confirme$
at floroscopy sing %ater-solble contrast material or%ith
en$oscopy"
So7t Tissue "njuries o7 the Chest?allThe chest %all has a rich
*asclar net%ork establishe$ bythe intercostal an$ internal mammary
arteries" ibfractres can lacerate intercostal arteries or *eins)
tear
intercostal mscles) or reslt in blee$ing from the ra%srface of
the bone" #n a$$ition) branches of the lateralthoracic artery that
spply the pectoral mscles an$anastomose %ith chest %all *essels can
be lacerate$ an$blee$" ; large amont of bloo$ can collect in
thesbctaneos or e4trapleral spaces of the chest)especially in the
el$erly becase of skin an$sbctaneos tisse la4ity" CT scanning can
easily
$istingish chest %all from parenchymal or me$iastinalin(ry)
%hereas this $ifferentiation may not be possible%ith chest
ra$iography" Fn CT) soft tisse hematomas ofthe chest %all are
rea$ily $istingishe$ from parenchymalin(ry) an$ sbctaneos air is
$istingishe$ frompnemothora4" CT scanning sho%s
broncho-pleral-ctaneos fistlae) %hich may not be appreciate$ on
thechest ra$iograph
-
8/9/2019 8.Chest Trauma
43/51
gol$ stan$ar$ for the $iagnosis of acte aortic in(ry" CTpro*i$es
a look at the entire chest in a$$ition to theaorta) %hich is a
$istinct a$*antage o*er con*entionalaortography" #n a$$ition to
sho%ing fractres) CT also
sho%s relate$ soft tisse in(ries) sch as great *esselin(ry from
fractre-$islocation of the cla*icle an$splenic'li*er laceration
from a$(acent rib fractres" #nsome cases) CT sho%s $irect signs of
t racheobronchial)esophageal) or $iaphragmatic in(ry" Chest CT can
beperforme$ Aickly on all trama patients %ho are referre$for
ab$ominal CT as a means of $etecting serios chestin(ries early"
&e7erences
!" shettry M) Holman :" Chest trama";ssessment) $iagnosis) an$
management" Clin ChestMed.!55!.D!,1?E!"
$"%&E '(3'. *reast hematoma.CT of a %omanin*ol*e$ in a motor
*ehicle crash sho%s a high-attenation collection of bloo$ in the
right breastarrows+) a reslt of shearing stress pro$ce$ by a
seat belt"
-
8/9/2019 8.Chest Trauma
44/51
-
8/9/2019 8.Chest Trauma
45/51
!!" :ir*is 6) Hi$%ell B) H$$emeyer 67) et al" Maleof chest
ra$iography in e4cl$ing tramatic aorticrptre" Radiology.
!581!,D81?E5,"
!2" Jarley K=) :ena #" Car$iac an$ *asclar seAelaeof sternal
fractres" Tra!ma.!582D..,?E..."
!," =armley C
-
8/9/2019 8.Chest Trauma
46/51
2!" Toombs HK) an$ler C:) Lester G" Compte$tomography of chest
trama" Radiology.!58!!0D1,,?E1,8"
22" Wagner H) Cra%for$ WF Br) chimpf =="Classification of
parenchymal in(ries of the lng"Radiology. !588!1D11?E82"
2," Joff B) hotts K) 6$$y M;) :orris B; Br" Ftcomeof isolate$
plmonary contsion in blnt tramapatients" (m "!rg. !550D!,8?E!2"
2"
-
8/9/2019 8.Chest Trauma
47/51
ma(or bronchi" Thorac Cardio&asc "!rg.!5.5,8D.8?E80"
,!" Chesterman BT) atsangi =/" ptre of the
trachea an$ bronchi by close$ in(ry" Thora).!52!D2!?E21"
,2" elly B=) Webb W) :ol$er =M) et al" :anagementof air%ay
trama" #" Tracheobronchial in(ries" (nnThorac
"!rg.!58.0D..!?E..."
,," =olansky ;) esnick K) offerman ;) Ka*i$son
T:" Jyoi$ bone ele*ationD a sign of trachealtransection"
Radiology. !58!.0D!!1?E!20"
," ollins B) Tocino #" 6arly ra$iographic signs oftracheal
rptre" (R (m Roentgenol.!585!8D5.?E58"
,." Fh )
-
8/9/2019 8.Chest Trauma
48/51
(R (m Roentgenol. !582!,8D,,?E,1"
0" 6strera ;) Lan$ay :B) :cClellan$ /" Hlnttramatic rptre of the
right hemi$iaphragmD
e4perience in !2 patients" (nn Thorac "!rg.!58.,5D.2.?E.,0"
!" Gorin ;) Gar3on ;;" Kiagnostic problems intramatic
$iaphragmatic hernia" Tra!ma.!51!D20?E,!"
2" Joo$ :" Tramatic $iaphragmatic hernia" (nn
Thorac "!rg.!51!!2D,!!?E,2"
," earney =;) ohana W) Hrney 6" Hlntrptre of the $iaphragmD
mechanism) $iagnosis an$treatment" (nn %merg
Med.!585!8D!,2?E!,,0"
" Wienceck G) Wilson
-
8/9/2019 8.Chest Trauma
49/51
-
8/9/2019 8.Chest Trauma
50/51
Thorac $maging.!5812D!?E!!"
.8" Jarris K) Jarris BJ Br" The pre*alence an$significance of
misse$ scaplar fractres in blnt chest
trama" (R (m Roentgenol. !588!.!D11?E1.0"
.5" ;shbagh KG) =eters G/) Jalgrimson
-
8/9/2019 8.Chest Trauma
51/51