Embed Size (px)
Citation preview
10.1192/bjp.166.5.654Access the most recent version at DOI: 1995, 166:654-659.BJP
S H Jones, G Thornicroft, M Coffey and G DunnGlobal Assessment of Functioning (GAF).A brief mental health outcome scale-reliability and validity of the
Referenceshttp://bjp.rcpsych.org/content/166/5/654#BIBLThis article cites 0 articles, 0 of which you can access for free at:
permissionsReprints/
[email protected] To obtain reprints or permission to reproduce material from this paper, please write
to this article atYou can respond http://bjp.rcpsych.org/letters/submit/bjprcpsych;166/5/654
from Downloaded
The Royal College of PsychiatristsPublished by on July 7, 2014http://bjp.rcpsych.org/
http://bjp.rcpsych.org/site/subscriptions/ go to: The British Journal of PsychiatryTo subscribe to

British Journal of Psychiatry(1995), 166, 654—659
As changes continue to occur apace in the provisionof mental health services, the need for quickand accurate indicators of severity of mentalillness is increasing. Such measures are potentiallyuseful in tracking the mental health of individualclients and also for initial evaluations of characteristics of client populations attending particularservices. DSM—III—R (American Psychiatric
Association, 1987)provides a rating scale, the GlobalAssessment of Functioning (GAF), for measurement
of overall psychiatric disturbance. Like the earlierGlobal Assessment Scale (GAS) (Endicott et a!,1976), the GAF has a number of ranked sentencesdescriptive of psychiatric disturbance, associatedwith numerical ratings.
Dworkin et a! (1990) used the GAS with multipleraters in a large sample of chronically mentally illpatients. They found that this scale was reliable both
within and between raters over the course of their18-month study. There have been an increasingnumber of studies that have employed the GAS asan outcome/severity measure for a range of patientgroups. Use of GAF has been less common, althoughthere are exceptions (e.g. Lyness eta!, 1993; Shanks,1994). Furthermore, there are few reports thataddress the issue of the reliability and validity ofOAF for a chronically mentally ill population.Shanks (1994) reported that clinician's ratings of casevignettes using GAF achieved acceptable levels of
reliability and validity, but felt that the implicationsof such results for the use of OAF in clinical practicewere limited. A further issue with respect to OAFis that in its original form it confounds twoareas of functioning: symptomatology and socialfunctioning. As Goldman eta! (1992) indicate, it hasbeen suggested that these two areas be separated inratings.
In the present study the OAF was used toassess severity of disturbance in a sample ofchronically mentally ill patients, assessed over6 months. In addition to original GAF scores,separate ratings are taken for symptoms andsocial functioning. As noted above it is importantto have some indication of the validity of thesemeasures: patients were rated therefore on a threepoint measure of support needs used routinely withinthe clinical team and on changes in antipsychoticmedication. If valid, then GAF scores would beexpected to be associated in a logical mannerwith changes in support needs, which reflectthe practical clinical response to perceived changesin levels of disturbance among clients. Associationwith medication changes would be expected tobe lower, as the team's aim is to maintainpatients on minimum effective doses; hence nonpharmacological responses will normally formthe first interventions to initial indications ofincreasing disturbance.
654
A Brief Mental Health Outcome ScaleReliability and Validity of the Global Assessment of Functioning (GAF)
STEVEN H. JONES, GRAHAM THORNICROFT, MICHAEL COFFEY and GRAHAM DUNN
Background.The GlobalAssessmentof Functioning(GAF)is a quickand simplemeasureofoverallpsychologicaldisturbance.However,thereis littleresearchonthe reliabilityandvalidityof this measure in severely mentally ill populations.Method. Multidisciplinarykeyworkers assessed103 patients at monthly intervals over a6-month period. Overall GAF scores were obtained, with additionalseparate ratings forsymptomsand disability.These were comparedwith changesin antipsychoticmedicationand supportneedsover the same period.Results.Satisfactoryreliabilitywas obtainedfor totalGAFscoreandfor symptomanddisabilitymeasures, in spite of raters having only one brief training session.All GAF scores wereassociated with current support needs of patients. Symptom and disability scores were associatedwith changesin antipsychoticmedicationin the previousmonth. Only symptomscorewasassociatedwith increasesin antipsychoticmedicationat time of rating.Conclusion.GAF provedto be a reliableand, within the limitsof the indicatorsused, a validmeasureof psychiatricdisturbancein our sampleof the severelymentallyill. Difterencesinrelationshipsbetween the three GAF scores and medication/supportneeds indicate theusefulnessof obtainingallthreescoresfor monitoringlevelsandtypeof psychiatricdisturbancein this population.

655BRIEF MENTAL HEALTH OUTCOME SCALE
Two further OAF ratings were also made foreach patient: symptoms (OAFSYM) and disability(OAFDIS), following Goldman et a! (1992). Sinceeach of the above nine descriptors confoundssymptoms and disability, the symptom scale isformed by taking the part of each descriptor thatdeals only with symptoms; the remaining aspectsof disturbance are then described in the disabilityscale.
Procedure
Instruments were described to raters in a brief grouptraining session of approximately 30 minutes. Anyraters added after this first session were givenindividual instruction in the use of these measures.Ratings took place on the first Friday of each month,over a 6-month period. Ratings were made withrespect to the patient's lowest level of functioningat the time of rating. Each patient was rated by theirkeyworker (clinician from any discipline responsiblefor co-ordination of care for that patient).
It was not possible to obtain complete rating setsfor any of the six ratings recorded. Numbers variedfrom a maximum of 92 in month 5 to a minimumof 56 in month 6 out of a possible 103 ratings.
Statistical analysis
Data were analysed by means of mixed effectsanalysis of variance models using the REMLprogram (Scottish Agricultural Statistical Service,University of Edinburgh). The use of REML in theanalysis of reliability studies is described in Dunn(1989, 1992). This approach allows for the estimationof both variance components and fixed effects inrepeated data in which not all patients have acomplete set of observations. Patient number wasincluded in all models as a random effect. Rateridentity was also included as a random effect for theestimation of reliability coefficients. Time of rating(e.g. months 1—6)was included as a fixed factor inall of the following analyses, although in no case wasits effect statistically significant.
Results
Table 1 presents mean scores for GAFF, OAFSYMand GAFDIS over the 6-month period of the study.This indicates apparently similar levels of overalldisturbance, symptoms and disabilities. These scoresindicate at least moderate levels of disturbance in themajority of patients, which would be consistent withthe predominance of psychotic illnesses in the groupstudied.
Method
A total of 103 patients were assessed over a 6-monthperiod. These were all patients attending the DistrictServices Centre of the Maudsley Hospital. They hadthe following diagnoses: schizophrenia (n = 75);manic-depressive psychosis (n = 13);major depression(n = 6); dysthymia (n = 1); personality disorder(n = 6); and obsessionalcompulsivedisorder (n = 2).
Raters
A total of 12raters took part in this study. They wereall members of the multidisciplinary mental healthteam treating the above patients. This groupcomprised five nurses, four psychiatrists, twooccupational therapists and one psychologist.
Instruments
Support needs (SUPP) were allocated according toa three-point scale. High support needs (scored 3)were indicated by daily attendance, poor socialsupport, complex family circumstance/no family,poor physical state, high risk to self or others.Medium support needs (scored 2) were indicated byweekly attendance, medium social support, mediumfamily circumstances, medium physical state, mediumrisk to self or others. Low support needs (scored1)were indicated by monthly attendance, good socialsupport, good family circumstance, good physicalstate, low risk to self or others.
Antipsychotic medication (MED) was also ratedaccording to a three-point scale: increased (3 points),remained the same (2 points), decreased (1 point)over the preceding month. Changes in other typesof medication were not scored.
OAF consists of nine behavioural descriptorsranging from “¿�absentor minimal symptoms (e.g.mild anxiety before an exam) - . . no morethan everyday problems―to “¿�persistentdanger ofseverely hurting self or others - . . or persistentinability to maintain minimal personal hygiene orserious suicidal act with clear expectation of death―.Patients are rated between 0 (most severe) and90 (least severe), each descriptor having a ninepoint range. Therefore raters have two decisionsto make: they have to decide which of the descriptorsis the best summary of the particular client'sproblems and then for that descriptor they usethe nine-point scale to indicate the severity of theproblems indicated. Final score was coded as OAFTotal (GAFF).
Patients

GAFT52.4(14.6)GAFSYM53.8(15.2)GAFDIS55.2(15.2)
RaterGAFTGAFSYMGAFDIS1—2.74—1.89—4.3322.441.822.593—0.042.921.3041.171.110.955—8.07—2.69—7.99612.809.4810.1472.482.440.878—10.80—7.44—8.6894.22—0.884.70101.330.820.50115.222.845.3012—8.02—9.53—5.35se.'4.374.344.28
656 JONES ET AL
Patient = 127.00 (s.c. 20.46) and ‘¿�Error'= 53.19 (s.c.4.08). The reliability coefficients for randomly selectedraters for each assessment, or for a single rater to makeall assessments, are 127.00/(127.00+39.93+53.19)=0.58 and 127.O0/(l27.00 + 53. l9)= 0.70, respectively.
The above results indicate that rater effects are asignificant source of variation in the assessments.This was confirmed by the following. IndividualRater effects (BLUPs, best unbiased linear predictors)were also produced by the REML analyses, togetherwith the standard errors for the differences betweenpairs ofraters(seeTable 2). The difference between anytwo raters represents their constant bias, relative toeach other. In the case of GAFF, the maximumrelative bias was about 23.5 points (s.c. about 4.5).For GAFSYM, the maximum relative bias was about18 (s.c. about 4.5). Finally, for GAFDIS themaximum relative bias was about 18.5 (s.c. about4.5).
These apparently large rater effects are likely tohave arisen from the fact that the study was notdesigned as a formal generalisability study in whicha selection of raters rated each of the 103 patients;the values given in Table 2 probably reflect changesin patient means rather than biases. In fact most ofthe patients (84%) will have been rated by only onerater (their keyworker). These patients are essentiallynested within raters . The rater effects and patientdifferences will, therefore, be partially confounded.On the assumption that the rater effects werenegligible the above analyses were repeated afterdropping Rater as a random effect. If, indeed,the dropped rater effects were confounded withpatient differences, rather than inflating measurementerror, we would expect the new patient variance components to be higher. This was the case. For GAFFthe variance components were 167.20 (s.c. 25.39) and53.68 (s.c. 4.07) for Patient and ‘¿�Error',respectively.The corresponding reliability coefficient is 167.20/(l67.20+53.68)=0.76. For GAPSYM the variancecomponents were 160.50 (s.c. 24.96) and 66.85 (s.c.5.08) for Patient and ‘¿�Error', respectively. Thereliability of GAFSYM is therefore 160.50/(l60.50+66.85)= 0.71. Similarly, the variance components ofGAPDIS were 161.80 (s.c. 24.76) and 56.34 (s.c.4.29) for Patient and ‘¿�Error'respectively, witha corresponding reliability of 161.80/(161.80 +56.34) = 0.74. These reliabilities arc quite satisfactory. A similar analysis for SUPP gave areliability of 0.55 (equivalent to a weighted kappa).
RelationshipbetweenGAP and supportneeds
Separate analyses were carried out for each of thethree GAF measures in relation to current support
Table 1Mean(s.d.)forGAFscoresaveragedoverthe
six (monthly) rating periods
GAFF, total Global Assessment of Functioning(GAF) score; GAFSYM. GAF symptom score;GAFDIS,GAFdisabilityscore.
Reliability
Separate analyses were carried out for GAFF,GAFSYM and GAFDIS. Models included Patient(1—103)and Rater (1—12)as random effects, withtime (1-6) as a fixed factor. For GAFF the estimatedvariance components for Rater, Patient and ‘¿�Error'were 52.27 (s.e. 27.43), 127.90 (s.c. 20.45) and 49.34(s.c.3.77),respectively.The reliability(generalisability) of a rating in which each assessment foreach patient is made by a randomly chosen rater isthereforegivenbytheratiol27.90/(52.27+127.90+49.34)= 0.56. If a single rater were to rate all patientsthe rater component could be dropped from thisexpression, yielding a reliability (generalisability)coefficient of l27.90/(l27.90 + 49.34) = 0.72.
The corresponding variance components forGAFSYM were: Rater = 32.76 (s.c. 19.65), Patient =139.60(s.c.22.69)and ‘¿�Error'= 63.75(s.c.4.88).The reliability for an assessment made by a randomlyselectedraterisl39.60/(139.60+32.76+63.75)=0.59; that for ratings when all made by the same rateris 139.60/(l39.60+63.75)=0.69. The variance components for GAFDIS were: Rater = 39.93 (s.c. 22.19),
Table 2Ratereffects on GAFT, GAFSYMand GAFDIS(BLUPs,
measuredas deviationsfroman overallmean)
1. Averagestandarderrorof differencesbetweenanypairof raters.GAFT, totalGlobalAssessmentof Functioning(GAF)score;GAFSYM, GAF symptom score; GAFDIS, GAF disability score.
657BRIEF MENTAL HEALTH OUTCOME SCALE
I'@ ‘¿�—‘—@@!r.@ i'@@ (O@LC)Ió C@―*1― 00@@ C
Iu; C@C@C@'I @w It―C@JC'1C@J
.@@ @tn@— <@@ I()00CO NLL@ 0
‘¿�D I@ W'D@ e@@-: 00 1C')@ @8 1c') @,. LUE i i i i @c@ I I I
@ Ea@ WIC@4 *:t@@ c'4@ . -
@0@@ @.COLg) °‘E N@1@@@ NO)CO a0.@ C'INO) NIL)@— C
! IB v-4@@ 0 C@1OC') tj.@ I@@ U@ I
a i 0 U.@ .@ I ‘¿�-@ U,
°@! <@ a@ I 8@8@ (D@ 888@2 I dad @CC - I! @‘¿� I c@dda @.C@ >
a@o C@ a°@n 0
@ I@@@ -@ E L'@.@
a I a@@@ U)@@ LC@N@[email protected] I a NC-JCN <C-a@ a C@C@4C@1
@0 I •¿�.‘Cl) ‘¿�5@0 I W@E 0 00
e@@@ C .9 aI@@@ I Lob'-&@ IC,,@ @C.C a c.@icó,.: @E@00@ ,_@6,-I ‘¿� -U-@@ .@ @I
< WI WI 0_w@ NLOC'-l @!@ @i C―lC)O@D I C-'INO <@ a@ ‘¿�@PON
@ 1c@4 ,.-,[email protected] L@@2@ I
c-@I@ II ..0,,, a@@@ I !C'@ ,@ I .5 a
@ I 888@@ I 8@8 u.,2E8'@@ c@c@ó@ I oac;
@W =
@ En@@
@ 1e4 @—¿�C0C')@ a@ c@inO< I ‘¿�LC)CO@CO@ @li I °@@
c,,@2@ ‘¿�@‘@‘@<@D0@ 1u;@u.E a@
2@ I.o@ I OC°@ @(D@' @a@@a3 I aa@ 11)00)@o@ Icy))C'@L@)F-a IC') @@‘N
@ @I ‘¿�@-@
C, C'@1 @j p
a@ •¿�@ c1j @a)co@ @,.a@@ cOCOC')@@ . @<C@ @:
@ c@@@ <Ea 0@ C'iC@C'i@@ I@ C U.@@ I
g@ @‘¿�‘a @Et@ 2 @0C C0@ I I I@
@@ 8@8 :@8@1 a@ 888@soa5@ 0.
a@aa@ I@@@
@ I c;ao@ “¿�@I 000 c@V oa<!@5 ‘¿�V OsC W*.(D@@ C
to@@ @0@
‘¿�— I@ co 0 N @—¿� C@ @l C@) (“4CD a@0@ 4@@ .2@ si@@LU i ui @.- d•U:-@ I ‘¿�@,:,.@,.:
@@ @u@&@ I@D@
N@ c@[email protected]') @aCE@ a@0.@ r@)c',ico@ E@
@ I cóIsiL@@@ 0@ cóioLg)2'@@ = It―@@Cl) ‘¿�-I III‘¿�-@ &I@ ‘¿�@@‘ @I
—¿� 0.1 C@U)& @I@ ° @IU)@@@ a @c'@1 oc@@@:
C/) I@ N 0)@@ U)@ C@4It)@ I 00)0 L0C@4C')
E5!@.@ .@ I I@ E'o-@ .@ I@ I I@@ I
@u) I@ to
@a E@ 888@ I 888@ —¿� .@ I@@@@@ I dOO @‘¿�!‘[email protected] U)@ 000
@ Oa 5‘¿�C [email protected] 5C o.@ aC.t)a(5 @@!EE .@aa@
!a@@.@ C@4@
I@@@ @U) 5@
h-cnO@ t:[email protected]. LL.U.<<< <<< .C.D(@W@@ (DC.@(D .-r@iW C

SUPP2MED2123s.e.2123s.e.2GAFT20.00—3.59—10.601.880.00—1.474.492.58GAFSVM20.00—5.26—12.572.000.00—0.183.472.77GAFDIS20.00—4.05—6.441.820.00—1.411.442.47
658 JONES ET AL
Table 5Estimatedjointeffects' of SUPP2andMED2on GAFscoresin precedingmonth(GAFT1,GAFSYM1andGAFDIS1)
1. Measured as contrasts from level 1 of SUPP2 and MED2. as appropriate.2. Average standard error of difference between pairs of effects.GAFT2.current total GlobalAssessmentof Functioning(GAF)score; GAFSYM2,current GAFsymptom score; GAFDIS2,current GAFdisability score; GAFF1, total score in precedingmonth; GAFSYM1•¿�GAFsymptom score in precedingmonth; GAFDIS1•¿�GAFdisabilityscore in precedingmonth; SUPP2.current level of support needs; MED2, current needsfor antipsychotic medication.
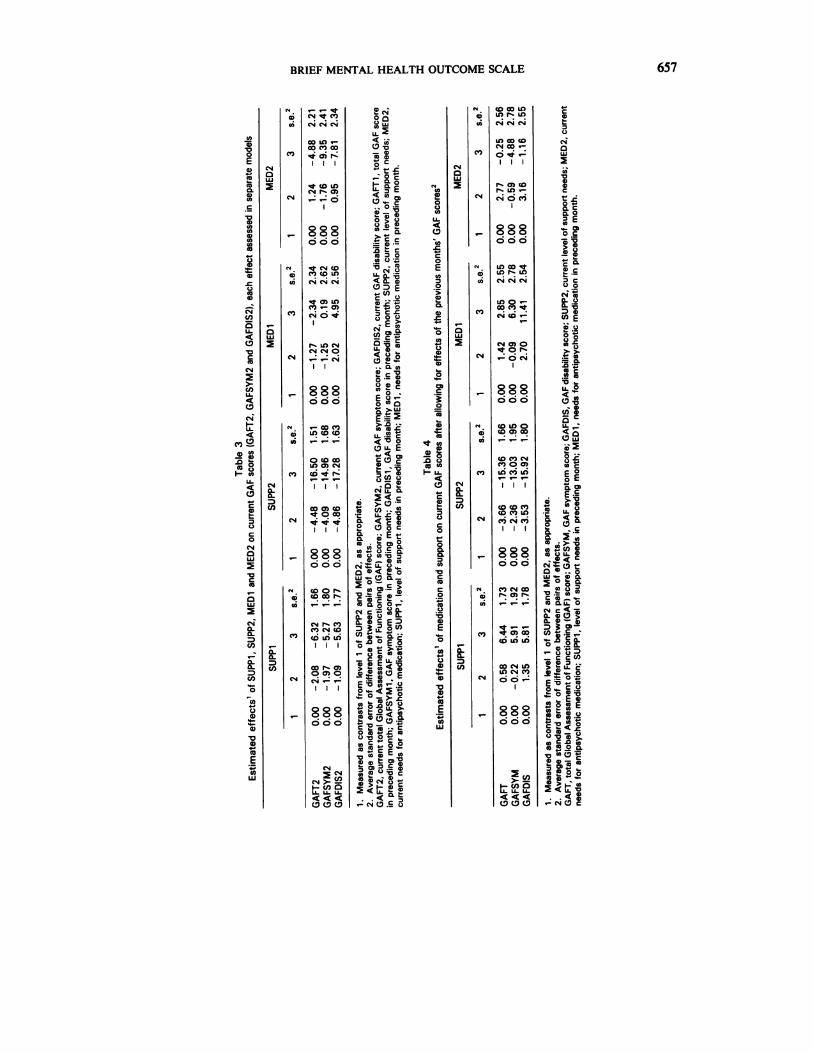
(SUPP2), current medication (MED2), support inthe preceding month (SUPP1) and medication in thepreceding month (MEDI). In this, and all the followinganalyses, time is fitted as a fixed effect, and Patientand Rater as random effects. The remaining effectsarc fixed. The estimated effects are shown in Table 3.Large negative associations were noted betweenSUPP2 and all OAF measures. Smaller associations,but of the same sign, were noted between SUPP1and OAF measures. MED1 did not have a consistentassociation with OAF scores. MED2, when analysedas a separate factor, was found to be negativelyassociated with OAF scores, particularly GAFSYM.
Current total OAF score (OAFT2) was next usedas the dependent variable, with factors SUPP1,SUPP2, MED1 and MED2 simultaneously enteredas fixed effects, covarying for OAF score (OAVF1)in preceding month. The results are shown in Table 4.This indicated no significant effects for time, MED1or MED2. Increases in support in the precedingmonth were associated with increased current GAFtotal (improved functioning). The clearest effect wasthat of lower OAF total (OAFT2) being associatedwith higher SUPP2.
Current OAFSYM and OAFDIS scores (GAFSYM2and OAFDIS2, respectively) were also entered asdependent variables (in separate analyses) withSUPP1, SUPP2, MED1 and MED2 as simultaneousfactors and the appropriate prior OAFSYM andOAFDIS scores (OAFSYM1 and GAFDIS1, respectively) entered as covariates. As above, SUPP1 waspositively associated with current OAF scores of bothtypes, while the relationship for SUPP2 was largerand of the opposite sign. Similarly, MEDI waspositively associated with current OAF (particularlysymptoms), while MED2 was modestly negativelyassociated. These results (Table 4) suggest thatincreased support and medication in the previousmonth leads to decreased psychological disturbanceas measured by OAF. Increases in disturbance lead
to immediate changes in support and, to a lesserextent, to increases in medication.
Finally, we examined the relationship betweenpreceding OAF scores (GAFT1, GAFSYM1 andOAFDIS1) and support level at the point of rating(SUPP2) and antipsychotic medication, also at thepoint of rating (MED2). The OAF scores were usedas the dependent variables in the REML runs, withSUPP2 and MED2 as predictive factors (fixedeffects). The estimated effects for SUPP2 and MED2are shown in Table 5. These estimates indicate asubstantial relationship between SUPP2 and all OAFscores, this being largest for OAFSYM and smallestfor GAFDIS. In all cases a decreased OAF score wasassociated with an increase in the clinically identifiedsupport needs of the client. There was no significantrelationship between OAF scores and MED2 forthese comparisons.
Discussion
The current data indicate that OAF is a reliablemeasure of disturbance of psychological functioningin a cohort of long-term mentally ill patients.Following Goldman et a! (1992), the GAF wasadministered as both an overall scale and as twoseparate measures assessing symptoms and disability.Reliability of ratings was satisfactory in all cases,indicating the viability of these more specific scalesfor use in clinical practice. It should be emphasisedthat these reliability figures were obtained for ratersgiven only limited training in the use of the abovemeasures. It is therefore possible to be relativelyconfident, in contrast to Shanks (1994), that thesefigures represent a realistic estimate of reliabilityfigures in general clinical practice.
It is clear that a reliable measure can derive itsreliability from a number of sources, some havingno association with validity of the measurementbeing taken. In the case of global measures it is

659BRIEF MENTAL HEALTH OUTCOME SCALE
necessary to be alert to the possibility that reliabilityfigures may derive from insensitivity of measurement.Therefore, in the current study, OAF scores wereassessed in relation to two indicators of clinical needroutinely used in clinical practice by the multidisciplinary team. These were the level of supportrequired by a given patient and the changes madeto antipsychotic medication.
When considered as separate factors it was foundthat support levels in both current and precedingmonth were negatively associated with all three OAFscores. Thus greater psychological disturbance, asindicated by symptoms, disability or total OAFscore, was associated with higher levels of clinicalsupport offered by the clinical team. Currentmedication levelsshowed a similar negative associationwith OAF scores, this being clearest in relation toincreased symptomatology rather than disability.
When all factors were considered simultaneously,the strongest single association found was thatbetween current support level and all three OAFscores. When REML estimates control for precedingmonth's OAF score level the relationship betweencurrent OAF and prior support becomes positive,suggesting that early increases in support level arefollowed by improved functioning in subsequentmonths. Current medication is no longer associatedwith total OAF score in this analysis, suggesting itmay be an artefact of the large association withcurrent support. When symptom and disability scoresare analysed in a similar manner, the relationshipwith support levels reflects those for total OAF score.However, for both there is a positive relationshipwith medication in the previous month, whenpreceding OAF scores are controlled for. Thisindicates that increases in antipsychotic medicationin the previous month are followed by improvedlevels of current functioning, as measured by bothsymptom and disability scores. Association betweencurrent medication and OAF remains negative forsymptom score, but is minimal for disability.
The OAF has been shown to be a reliable, quickmeasure of disturbance in functioning, which can be
readily used by multidisciplinary raters, without theneed for extensive training. Whereas more detailedmeasures of symptomatology and social functioningare widely available, they are little used in routineclinical practice due to the resources and trainingrequired (e.g. Wykes & Sturt, 1986). Hence, inaddition to being a useful quick measure inpopulation-based surveys (Phelan et a!, 1994), theOAF has a role as a routine measure in clinicalpractice, which then facilitates monitoring ofindividual patients over time and oflevels of morbidityin particular clinical services. The current dataindicate that it is worthwhile obtaining all three OAFscores when assessing patients, as their relationshipswith medication, and to a lesser degree with priorsupport levels, differ.
References
AMERICAN PSYCHIATRICASSOCIATION(1987) Diagnactic and StatictkulManual of Mental Disorders (3rd edn, revised) (DSM—IH—R).Washington, DC: APA.
Dui'n@,G. (1989) The Design and Analysis of Reliability Studies.London: Edward Arnold.
(1992) The design and analysis of reliability studies.Statistical Methods in Medical Research, 1, 123-157.
DwoRICIN, R. J., FRIEDMAN, L. C., Thsci@ow, R. L., et al (1990)The longitudinal use of the Global Assessment scale in multiplerater situations. Community Mental Health Journal, 26,335—344.
ENI)ICoT'r, J., SprrzaR, R. L., FutIss, J. L., et al (1976) The
global assessmentscale.Archives of General Psychiatry, 33,766—771.
GOLDMAN, H. H., SKODOL, A. E. & LAVE, T. R. (1992) Revisingaxis V for DSM-IV: A reviewof measuresof social functioning.AmericanJournalof Psychiatry,149, 1148-1156.
LmEss, J. M., CAINE,E. D., CONWELL,Y., et al(1993) Depressivesymptoms, medical illness and functional status in depressedpsychiatric patients. American Journal of Psychiatry, 150,910—915.
PHEL&N, M., WYERs, T. & GOLDMAN, H. (1994) Global functioning
scales: A review. Social Psychiatry and PsychiatricEpidemiology, 29, 205-211.
Siwncs, J. (1994) How are things? Developing outcome measuresfor mental health services. Health Trends (in press).
WYKES, T. & STURT, E. (1986) The measurement of social
behaviourin psychiatricpatients:An assessmentof the reliabilityand validity of SBS. British Journal of Psychiatry, 148, 1-11.
Steven H. Jones, PhD, Graham Thornicroft, FRCPsych,Graham Dunn, PhD, Institute of Psychiatry, London;Michael Coffey, RMN, Maudsley Hospital, London
Correspondence: Dr Jones, Department of Psychology, Institute of Psychiatry, DeCrespigny Park, London SE5 8AF
(First received14 June 1994,accepted12 September1994)





























