Embed Size (px)
Citation preview
American Journal of Medical Genetics 130A:172–175 (2004)
Clinical ReportA Case of Adams–Oliver Syndrome WithAssociated Brain and Pulmonary Involvement:Further Evidence of Vascular Pathology?Anthony Joseph Piazza,1* Dwain Blackston,2 and Augusto Sola1
1Division of Neonatal-Perinatal Medicine, Department of Pediatrics, Emory University School of Medicine Atlanta, Georgia2Division of Genetics, Emory University School of Medicine Atlanta, Georgia
We report on a case of Adams–Oliver syndrome(AOS) with typical skin and limb defects alongwith the unique findings of pulmonary hyper-tension and central nervous system (CNS) in-volvement. Adams–Oliver syndrome has a widespectrum of physical anomalies ranging fromcharacteristic aplasia cutis congenita (ACC),transverse limb defects, and cutis marmoratatelangiectica to extensive lethal anomalies. Whilepulmonary hypertension is usually not associatedwith AOS, the abnormal endothelial regulation ofvascular tone seen in the pulmonary vasculaturemay enhance current pathophysiologic conceptsof vascular abnormalities in AOS. There is accu-mulating evidence of significant CNS defects inAOS. This infant had hypoplastic corpus callosumand focal findings in the periventricular whitematter. Evaluation for pulmonary hypertensionand CNS anomalies in patients suspected to haveAOS, can help identify those who are at risk foracute morbidities and associated developmentaldelays. � 2004 Wiley-Liss, Inc.
KEY WORDS: Adams–Oliver syndrome; aplasiacutis congenita; central nervoussystem; cutis marmorata telan-giectica congenita; terminaltransverse limb defect; pulmon-ary artery hypertension
INTRODUCTION
In 1945 Dr. Adams and Dr. Oliver described eight membersof a family with aplasia cutis congenita (ACC) and terminaltransverse limb defects. Since then, Adams–Oliver syndrome(AOS) has been described with a wide spectrum of phenotypesfrom minor skin and limb defects to lethal anomalies. Thesyndrome is associated with varying modes of inheritance,including autosomal dominant, autosomal recessive, and newmutations [Scribanu and Temtamy, 1975; Bamforth et al.,1994; Elliott and Teebi, 1997; Tekin et al., 1999]. Many leading
theories explain AOS associated physical anomalies by impli-cating in-utero vascular compromise leading to the defects[Hoyme et al., 1982; Toriello et al., 1988; Swartz et al., 1999].Only two previous cases of AOS with pulmonary hypertensionhave been reported. One case of pulmonary hypertensiondeveloped secondary to a cardiac defect [Toriello et al., 1988]. Asecond report describes a patient that developed late onsetpulmonary hypertension [Swartz et al., 1999]. Our patient notonly demonstrates the unique findings of pulmonary hyperten-sion during the newborn period but also central nervoussystem (CNS) abnormalities.
CLINICAL REPORT
This is the first-born infant of a 39-year-old whose pregnancywas complicated by gestational hypertension. Maternal familyhistory was unremarkable for dysmorphologies, mental re-tardation, and consanguinity. A cesarean section for severepregnancy-induced hypertension delivered a 35-week, smallfor gestational age, male with good Apgars. He was admitted tothe neonatal intensive care unit with echocardiogram docu-mented pulmonary hypertension. Aside from the gestationalhypertension, no other etiology for the growth restriction wasidentified. There was an area of ‘‘skin breakdown’’ on the scalpwith no history of scalp monitoring, delivery instrumentation,or herpes infection. The patient was discharged on day of life13. Two weeks later he was admitted to our hospital because ofcontinued murmur, persistence of scalp lesion, and seizures.
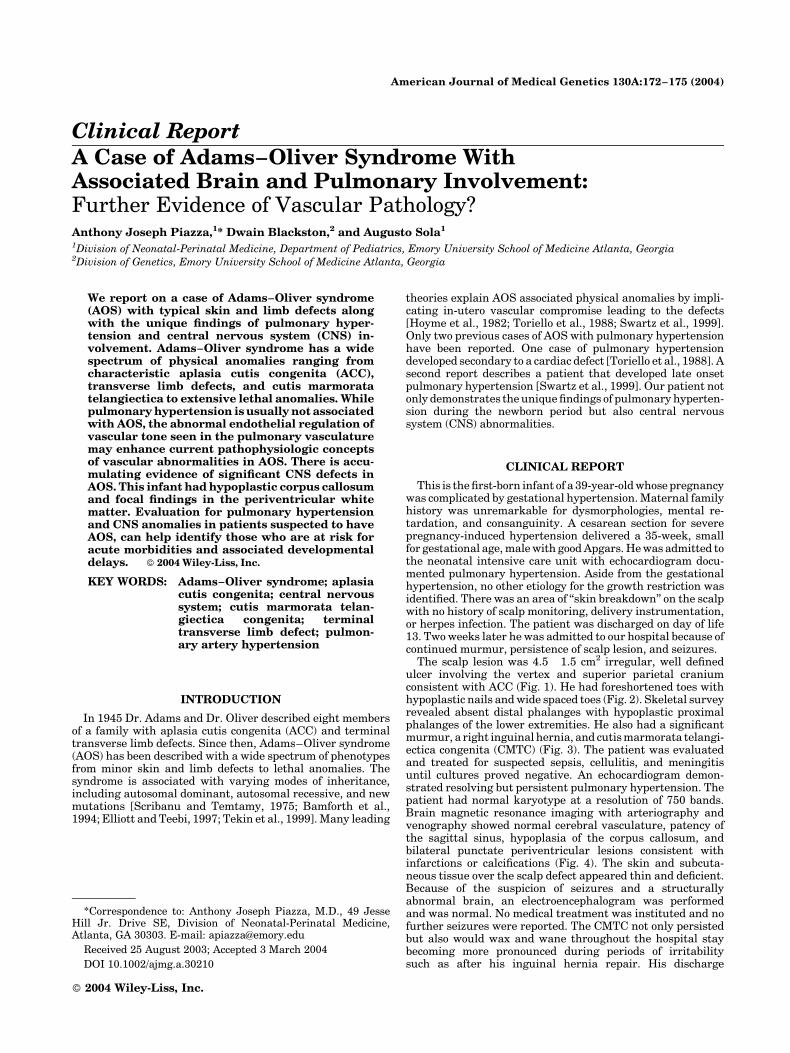
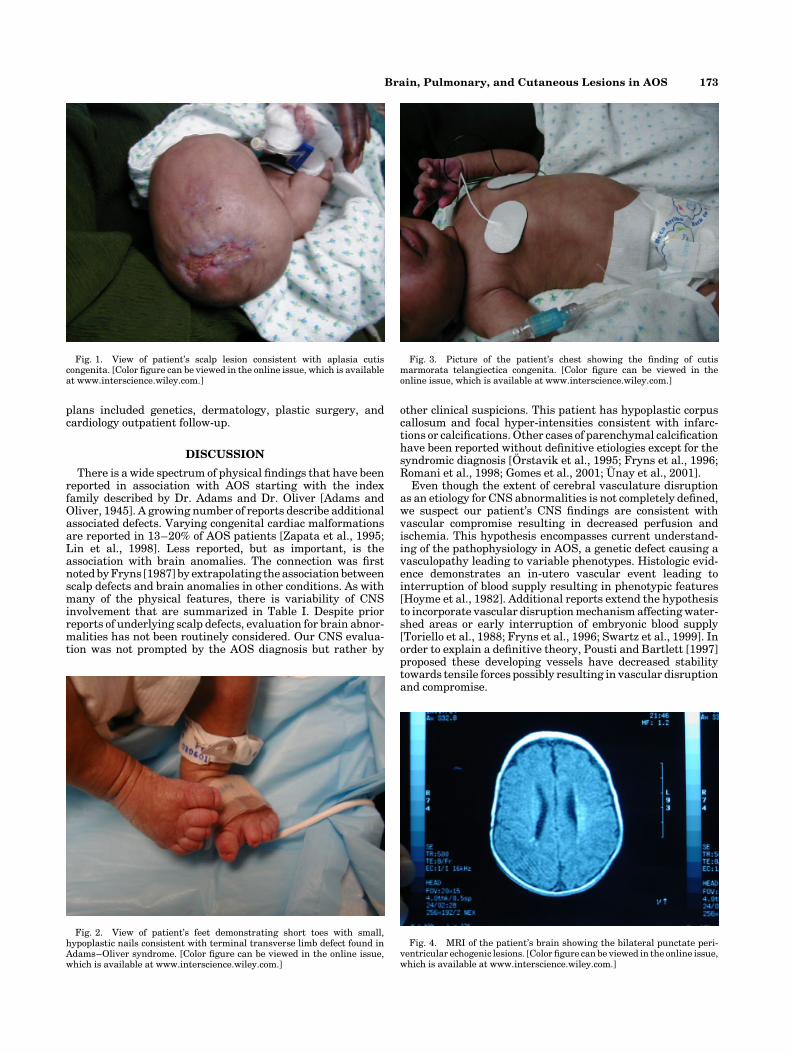
The scalp lesion was 4.5� 1.5 cm2 irregular, well definedulcer involving the vertex and superior parietal craniumconsistent with ACC (Fig. 1). He had foreshortened toes withhypoplastic nails and wide spaced toes (Fig. 2). Skeletal surveyrevealed absent distal phalanges with hypoplastic proximalphalanges of the lower extremities. He also had a significantmurmur, a right inguinal hernia, and cutis marmorata telangi-ectica congenita (CMTC) (Fig. 3). The patient was evaluatedand treated for suspected sepsis, cellulitis, and meningitisuntil cultures proved negative. An echocardiogram demon-strated resolving but persistent pulmonary hypertension. Thepatient had normal karyotype at a resolution of 750 bands.Brain magnetic resonance imaging with arteriography andvenography showed normal cerebral vasculature, patency ofthe sagittal sinus, hypoplasia of the corpus callosum, andbilateral punctate periventricular lesions consistent withinfarctions or calcifications (Fig. 4). The skin and subcuta-neous tissue over the scalp defect appeared thin and deficient.Because of the suspicion of seizures and a structurallyabnormal brain, an electroencephalogram was performedand was normal. No medical treatment was instituted and nofurther seizures were reported. The CMTC not only persistedbut also would wax and wane throughout the hospital staybecoming more pronounced during periods of irritabilitysuch as after his inguinal hernia repair. His discharge
*Correspondence to: Anthony Joseph Piazza, M.D., 49 JesseHill Jr. Drive SE, Division of Neonatal-Perinatal Medicine,Atlanta, GA 30303. E-mail: [email protected]
Received 25 August 2003; Accepted 3 March 2004
DOI 10.1002/ajmg.a.30210
� 2004 Wiley-Liss, Inc.
plans included genetics, dermatology, plastic surgery, andcardiology outpatient follow-up.
DISCUSSION
There is a wide spectrum of physical findings that have beenreported in association with AOS starting with the indexfamily described by Dr. Adams and Dr. Oliver [Adams andOliver, 1945]. A growing number of reports describe additionalassociated defects. Varying congenital cardiac malformationsare reported in 13–20% of AOS patients [Zapata et al., 1995;Lin et al., 1998]. Less reported, but as important, is theassociation with brain anomalies. The connection was firstnoted by Fryns [1987] by extrapolating the association betweenscalp defects and brain anomalies in other conditions. As withmany of the physical features, there is variability of CNSinvolvement that are summarized in Table I. Despite priorreports of underlying scalp defects, evaluation for brain abnor-malities has not been routinely considered. Our CNS evalua-tion was not prompted by the AOS diagnosis but rather by
other clinical suspicions. This patient has hypoplastic corpuscallosum and focal hyper-intensities consistent with infarc-tions or calcifications. Other cases of parenchymal calcificationhave been reported without definitive etiologies except for thesyndromic diagnosis [Orstavik et al., 1995; Fryns et al., 1996;Romani et al., 1998; Gomes et al., 2001; Unay et al., 2001].
Even though the extent of cerebral vasculature disruptionas an etiology for CNS abnormalities is not completely defined,we suspect our patient’s CNS findings are consistent withvascular compromise resulting in decreased perfusion andischemia. This hypothesis encompasses current understand-ing of the pathophysiology in AOS, a genetic defect causing avasculopathy leading to variable phenotypes. Histologic evid-ence demonstrates an in-utero vascular event leading tointerruption of blood supply resulting in phenotypic features[Hoyme et al., 1982]. Additional reports extend the hypothesisto incorporate vascular disruption mechanism affecting water-shed areas or early interruption of embryonic blood supply[Toriello et al., 1988; Fryns et al., 1996; Swartz et al., 1999]. Inorder to explain a definitive theory, Pousti and Bartlett [1997]proposed these developing vessels have decreased stabilitytowards tensile forces possibly resulting in vascular disruptionand compromise.
Fig. 1. View of patient’s scalp lesion consistent with aplasia cutiscongenita. [Color figure can be viewed in the online issue, which is availableat www.interscience.wiley.com.]
Fig. 2. View of patient’s feet demonstrating short toes with small,hypoplastic nails consistent with terminal transverse limb defect found inAdams–Oliver syndrome. [Color figure can be viewed in the online issue,which is available at www.interscience.wiley.com.]
Fig. 3. Picture of the patient’s chest showing the finding of cutismarmorata telangiectica congenita. [Color figure can be viewed in theonline issue, which is available at www.interscience.wiley.com.]
Fig. 4. MRI of the patient’s brain showing the bilateral punctate peri-ventricular echogenic lesions. [Color figure can be viewed in the online issue,which is available at www.interscience.wiley.com.]
Brain, Pulmonary, and Cutaneous Lesions in AOS 173

There are two AOS cases citing pulmonary vasculature in-volvement. Toriello et al. [1988] reports on a patient thatdeveloped pulmonary hypertension secondary to pulmonaryvein stenosis, while Swartz et al. [1999] describes a patientwith double outlet right ventricle and portal hypertension thatdeveloped pulmonary hypertension at 3–4 years of age. InSwartz’s report neither the cardiac defect nor the portal hyper-tension could explain the pulmonary hypertension; however,the portal hypertension was hypothesized to be the result ofendothelial abnormality. A third case of pulmonary hyperten-sion is reported but with an atypical presentation for AOS butalso thought to be consistent with vascular disruption [Al-Sanna’a et al., 2000]. Our patient is unique in that there is nounderlying anomalies that would result in pulmonary hyper-tension at birth or during the newborn period. This raises thequestion whether the pulmonary hypertension is related toAOS associated vasculopathy. The underlying problem in pul-monary hypertension of the newborn is abnormal regulation ofthe pulmonary blood vessel endothelium on vascular tone andreactivity. This pathophysiology can be applied to furtherenhance current concepts of vasculopathy in AOS by invokingabnormal endothelial regulation with subsequent disruption ofblood flow during critical periods of development. The exactmechanism requires further investigation but can explain pul-monary, CNS, and other clinical findings.
Vascular reactivity and disruptive endothelial regulation canbe implicated in other features associated with AOS. It isreasonable to associate pregnancy-induced hypertension andCMTC as vascular abnormalities. Gestational hypertensioncomplicated this pregnancy and resulted in fetal growth-restriction (a common finding in AOS). Although a complicateddisease, pregnancy-induced hypertension is due to an impairedtrophoblastic invasion and a disruptiveendothelial regulationofvascular tone and integrity [Myers and Baker, 2002]. AlthoughCMTC is non-diagnostic, the incidence is reported in 12% ofAOS cases [Farrell et al., 1993]. The pathogenesis of CMTC isalso believed to be a vascular defect [Toriello et al., 1988].
AOS represent an overall heterogenous group of patients.Primarily thought to be an autosomal dominant disease, otherassociated patterns of genetic inheritance and non-geneticinheritance patterns with varying degrees of penetrance andexpression are reported. Despite the many different associatedpatterns of genetic inheritance, the underlying genetic defectseems to express a predisposition for a vasculopathy.
This case demonstrates the need to evaluate and report onCNS defects and to further investigate the pathophysiologyrelated to AOS. Currently, the extent of CNS findings maybeoverlooked or under reported but this case adds to growingevidence of associated CNS abnormalities. A more inclusivehypothesis for AOS would include vascular reactivity andabnormal endothelial regulation as the underlying pathology.This pathophysiology would support previous theories andaccount for the typical clinical features as well as pulmonaryhypertension, CNS abnormalities, pregnancy-induced hyper-tension, and CMTC. We recommend pulmonary hypertensionevaluation and CNS imaging in patients suspected to haveAOS. Timely evaluation would provide interventions foracute problems and identify those at risk for developmentaldelays.
REFERENCES
Adams FH, Oliver CP. 1945. Hereditary deformities in man due to arresteddevelopment. J Hered 36:3.
Al-Sanna’a N, Adatia I, Teebi AS. 2000. Transverse limb defects associatedwith aorto-pulmonary vascular abnormalities: Vascular disruptionsequence or atypical presentation of Adams–Oliver syndrome. Am JMed Genet 94:400–404.
Amor DJ, Leventer RJ, Hayllar S, Bankier A. 2000. Polymicrogyriaassociated with scalp and limb defects: Variant of Adams–Oliversyndrome. Am J Med Genet 93:328–334.
Bamforth JS, Kaurah P, Byrne J, Ferreira P. 1994. Adams Oliver Syndrome:A family with extreme variability in clinical expression. Am J Med Genet49:393–396.
TABLE I. Central Nervous System and Typical Manifestations in Adams–Oliver Syndrome
Authors Central nervous system anomalies Typical major anomalies
Kuster et al. [1988] Encephalocele ACC, terminal transverse limb defectChitayat et al. [1992] Acrania; ventriculomegaly; abnormal cerebral
vasculatureACC, terminal transverse limb defect
Bamforth et al. [1994] Microcephaly ACC, terminal transverse limb defectMicrocephaly ACC, terminal transverse limb defectHydrocephalus; arrhinenephaly ACC, terminal transverse limb defect
Orstavik et al. [1995] Cerebral atrophy; thalamic and periventricularcalcifications; ventricular dilatation
ACC, terminal transverse limb defect
Absent corpus callosum; ventricular dilatation;periventricular leukomalacia
ACC, terminal transverse limb defect
Fryns et al. [1996] Left hemisphere hypoplasia; porencephalic cysts;left mesencephalon, pons and medulla oblongatahypoplasia; focal periventricular and thalamiclesions; left middle cerebral artery hypoplasia
ACC, terminal transverse limb defect
Romani et al. [1998] Periventricular/parenchymal calcium deposits;ventricular dilatation
ACC, terminal transverse limb defect
Mempel et al. [1999] Focal pachygyria and polymicrogyria ACC, CMTC, terminal transverse limb defectSavarirayan et al. [1999] Dysplasia of cerebral cortex ACC, terminal transverse limb defectAmor et al. [2000] Ventriculomegaly; polymicrogyria ACC, terminal transverse limb defect
Ventriculomegaly; polymicrogyria; hypoplastic corpuscallosum
Terminal transverse limb defect
Casken and Kurtoglu [2000] Acrania, microcephaly ACC, terminal transverse limb defectGomes et al. [2001] Hemimegalencephaly; abnormal cerebral veins ACC, terminal transverse limb defect
Encephaloclastic lesion; ventriculomegaly ACC, terminal transverse limb defectUnay et al. [2001] Microcephaly, intracranial calcifications ACC, terminal transverse limb defect
Hypoplastic corpus callosum, bilateral punctateperiventricular lesions
ACC, CMTC terminal transverse limb defect
ACC, aplasia cutis congenita; CMTC, cutis marmorata telangiectica congenita.
174 Piazza et al.

Casken H, Kurtoglu S. 2000. A case of Adams–Oliver syndrome associatedwith acrania, microcephaly, hemiplegia, epilepsy, and mental retarda-tion. Acta Neurologica Belgica 100:252–255.
Chitayat D, Meunier C, Hodgkinson KA, Robb L, Azouz M. 1992. Acrania: Amanifestation of the Adams–Oliver syndrome. Am J Med Genet 44:562–566.
Elliott AM, Teebi AS. 1997. Further examples of autosomal dominanttransmission of nonsyndromic aplasia cutis congenita. Am J Med Genet73:495–496.
Farrell SA, Warda LJ, LaFlair P, Szmonowicz W. 1993. Adams–Oliversyndrome: A case with juvenile chronic myelogenous leukemia andchylothorax. Am J Med Genet 47:1175–1179.
Fryns JP. 1987. Congenital scalp defects with distal limb reduction anoma-lies. J Med Genet 24:493–496.
Fryns JP, Legius E, Demaerel P, van den Berghe H. 1996. Congenital scalpdefect, distal limb reduction anomalies, right spastic hemiplegia andhypoplasia of the left arteria cerebri media: Further evidence thatinterruption of early embryonic blood supply may result in Adams–Oliver (plus) syndrome. Clin Genet 50(6):505–509.
Gomes LB, Castro J, Matos M, Nunes A, Furtado J, Barrueco MC. 2001.Lesions of the central nervous system in Adams–Oliver syndrome. ActaMedica Portuguesa 14(1):89–94.
Hoyme HE, Jones KL, Van Allen MI, Saunders BS, Benirschke K. 1982.Vascular pathogenesis of transverse limb reduction defects. J Pediatrics101(5):839–843.
Kuster W, Lenz W, Kaariainen H, Majewski F. 1988. Congenital scalpdefects with distal limb anomalies (Adams-Oliver syndrome): Report often cases and review of the literature. Am J Med Genet 31:99–115.
Lin AE, Wesgate MN, van der Velde ME, Lacro RV, Holmes LB. 1998.Adams–Oliver syndrome associated with cardiovascular malformation.Clin Dysmorphol 7:235–241.
Mempel M, Abeck D, Lange I, Strom K, Caliebe A, Beham A, Kautza M,Worret WI, Neubauer BA, Ring J, Schroder H, Folster-Holst R. 1999.
The wide spectrum of clinical expression in Adams–Oliver syndrome: Areport of two cases. British J Dermatol 140(6):1157–1160.
Myers JE, Baker PN. 2002. Hypertensive diseases and eclampsia. Curr OpinObstet 14(2):119–125.
Orstavik KH, Stromme P, Spetalen S, Flage T, Westvik J, Vesterhus P,Skjeldal O. 1995. Aplasia cutis congenita associated with limb, eye, andbrain anomalies in sibs: A variant of the Adams–Oliver syndrome? Am JMed Genet 59:92–95.
Pousti TJ, Bartlett RA. 1997. Adams–Oliver syndrome: Genetics and asso-ciated anomalies of cutis aplasia. Plast Reconstr Surg 100:1491–1496.
Romani J, Puig L, Aznar G, Demestre X, Altirriba O, Alomar A. 1998.Adams–Oliver syndrome with unusual central nervous system altera-tions. Pediatr Dermatol 15(1):48–50.
Savarirayan R, Thompson EM, Abbott KJ, Moore MH. 1999. Cerebralcortical dysplasia and digital constriction rings in Adams–Oliversyndrome. Am J Med Genet 86(1):15–19.
Scribanu N, Temtamy SA. 1975. The syndrome of aplasia cutis congenitawith terminal, transverse defects of limbs. J Pediatrics 87:79–82.
Swartz EN, Sanatani S, Sandor GG, Schreiber RA. 1999. Vascularabnormalities in Adams–Oliver syndrome: Cause or effect? Am J MedGenet 82(1):49–52.
Tekin M, Bodurtha J, Ciftci E, Arsan S. 1999. Further family with possibleautosomal recessive inheritance of Adams–Oliver syndrome. Am J MedGenet 86:90–91.
Toriello HV, Graff RG, Florentine MF, Lacina S, Moore WD. 1988. Scalp andlimb defects with cutis marmorata telangiectatica congenita: Adams–Oliver syndrome? Am J Med Genet 29(2):269–276.
Unay B, Sarici SU, Gul D, Akin R, Gokcay E. 2001. Adams–Oliversyndrome: Further evidence for autosomal recessive inheritance. ClinDysmorphol 10:223–225.
Zapata HH, Sletten LJ, Pierpont MEM. 1995. Congenital cardiac malforma-tions in Adams–Oliver syndrome. Clin Genet 47:80–84.
Brain, Pulmonary, and Cutaneous Lesions in AOS 175