Embed Size (px)
Citation preview
CASE REPORT
A case of rapidly progressing primary thyroid angiosarcomain a Japanese man
Nana Rokutanda • Jun Horiguchi • Yukio Koibuchi • Daisuke Takata •
Rin Nagaoka • Ayako Sato • Hideaki Tokiniwa • Sayaka Uchida •
Mio Furuya • Tetsunari Oyama • Izumi Takeyoshi
Received: 28 October 2013 / Accepted: 26 May 2014
� The Japan Society of Clinical Oncology 2014
Abstract Primary thyroid angiosarcoma is a very rare
and aggressive disease, originally reported in patients from
the Swiss Alpine region, but is rare in other parts of the
world. We describe a Japanese case of primary angiosar-
coma of the thyroid in a 64-year-old man, who presented
with a rapidly enlarging painful neck mass. Fine-needle
aspiration biopsy was performed, and the results were
interpreted as malignant. FDG-PET-CT demonstrated a
necrotic lesion on the right side of the neck with high FDG
uptake. The patient underwent a total thyroidectomy.
Pathological findings revealed a proliferation of atypical
cells lined vascular spaces. Immunohistochemistry staining
(IHCS) was positive for factor VIII, and CD31, but not
CD34, and negative for CK 5, CK 7, and CK 20. From
these findings, it was diagnosed as an epithelioid angio-
sarcoma. Two weeks after the operation, bilateral bloody
pleural effusion was observed, and he died 3 months after
the surgery.
Keywords Primary � Angiosarcoma � Thyroid
Introduction
Primary thyroid angiosarcoma is a very rare and aggressive
disease. The incidence of primary thyroid angiosarcoma is
highest in European alpine regions, and it constitutes
2–10 % of all malignant thyroid tumors in Switzerland,
Austria, and northern Italy [1, 2]. In other parts of the
world, it is extremely rare [1–9].
Local recurrence and metastasis are frequent, and
patients usually die within a short period of time after
diagnosis. Early tumor metastasis to regional lymph nodes
and the lungs is frequent. Currently, no optimal treatment
strategy is available for this malignancy [7]. Here, we
present a Japanese case of angiosarcoma of the thyroid
gland that underwent a markedly progressive course as an
undifferentiated thyroid carcinoma.
Case report
A 64-year-old Japanese man with a painful neck mass was
referred to our hospital for evaluation. The patient had
noticed the neck mass 2 months prior. At the first visit, the
patient had no hoarseness. There was no prior history of
neck trauma or irradiation, or a family history of thyroid
disorders. Physical examination revealed a hard, irregular,
and tender painful nodular lesion measuring 5 9 3 cm in
the right thyroid lobe. A few hard, painful lymph nodes
were also palpable in the right neck. Ultrasonography of
the neck revealed a well-circumscribed mass that measured
4.9 9 3.9 cm arising from the right thyroid lobe, as well as
a few swollen lymph nodes. Fine-needle aspiration biopsy
was performed for the thyroid tumor and lymph nodes, and
the results were interpreted as malignant. These cells dis-
played nuclear atypia and prominent nucleoli, absent
N. Rokutanda (&) � J. Horiguchi � Y. Koibuchi � D. Takata �R. Nagaoka � A. Sato � H. Tokiniwa � S. Uchida � I. Takeyoshi
Department of Thoracic and Visceral Organ Surgery, Gunma
University Graduate School of Medicine, 3-39-22 Showa-Machi,
Maebashi, Gunma 371-8511, Japan
e-mail: [email protected]
M. Furuya � T. Oyama
Department of Diagnostic Pathology, and Clinical Department of
Pathology, Gunma University Graduate School of Medicine,
Maebashi, Gunma, Japan
123
Int Canc Conf J
DOI 10.1007/s13691-014-0170-x
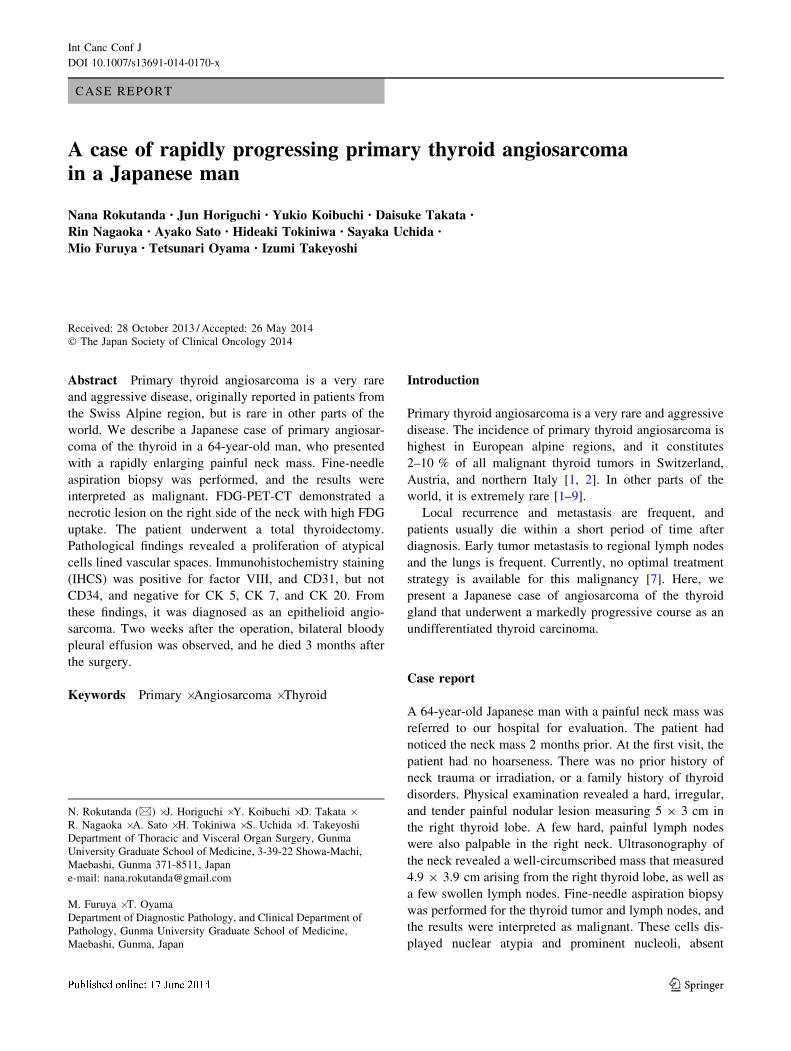
colloid, and poor cellularity (Fig. 1). Immunohistochem-
istry staining of the atypical cells in the aspirate of lymph
node was slightly positive for thyroglobulin, which was
probably of thyroidal origin. Laboratory investigation
showed slight increases in leukocytes (9700/ll), C-reactive
protein (3.8 mg/dl), and liver function (GOT 70 g/dl, GPT
81 mg/dl). Serum thyroid hormone levels were normal, but
thyroglobulin was markedly elevated to 2960 ng/ml (nor-
mal range, 0–35 ng/ml).
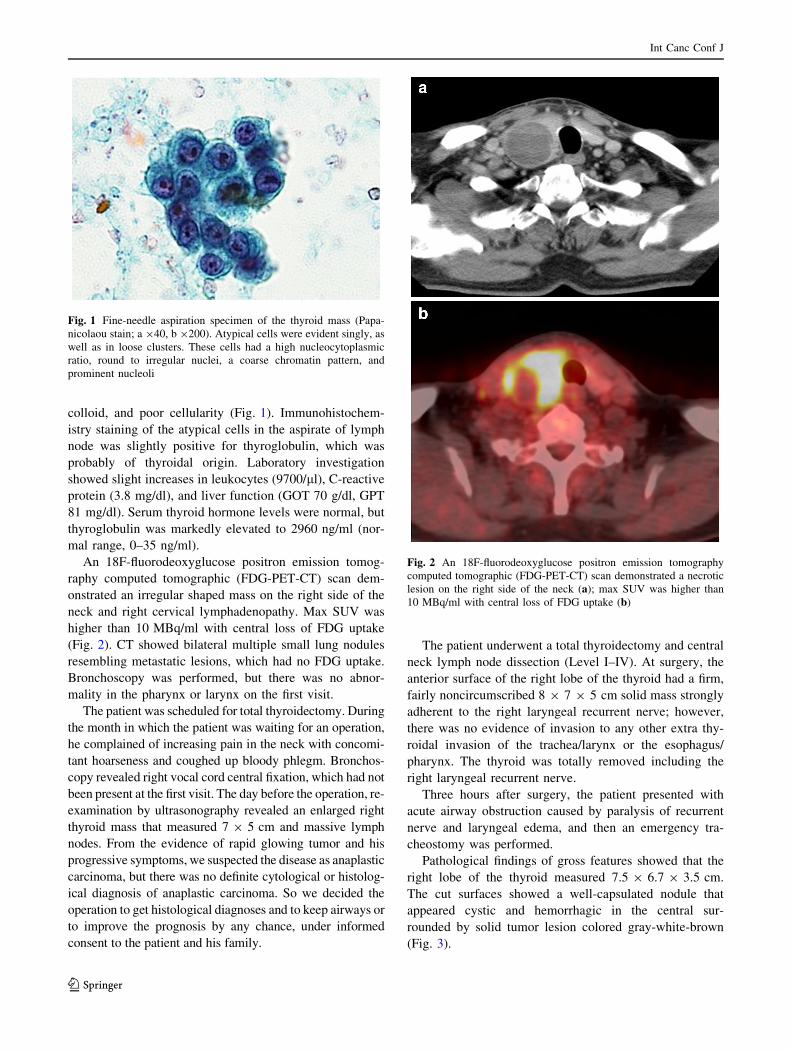
An 18F-fluorodeoxyglucose positron emission tomog-
raphy computed tomographic (FDG-PET-CT) scan dem-
onstrated an irregular shaped mass on the right side of the
neck and right cervical lymphadenopathy. Max SUV was
higher than 10 MBq/ml with central loss of FDG uptake
(Fig. 2). CT showed bilateral multiple small lung nodules
resembling metastatic lesions, which had no FDG uptake.
Bronchoscopy was performed, but there was no abnor-
mality in the pharynx or larynx on the first visit.
The patient was scheduled for total thyroidectomy. During
the month in which the patient was waiting for an operation,
he complained of increasing pain in the neck with concomi-
tant hoarseness and coughed up bloody phlegm. Bronchos-
copy revealed right vocal cord central fixation, which had not
been present at the first visit. The day before the operation, re-
examination by ultrasonography revealed an enlarged right
thyroid mass that measured 7 9 5 cm and massive lymph
nodes. From the evidence of rapid glowing tumor and his
progressive symptoms, we suspected the disease as anaplastic
carcinoma, but there was no definite cytological or histolog-
ical diagnosis of anaplastic carcinoma. So we decided the
operation to get histological diagnoses and to keep airways or
to improve the prognosis by any chance, under informed
consent to the patient and his family.
The patient underwent a total thyroidectomy and central
neck lymph node dissection (Level I–IV). At surgery, the
anterior surface of the right lobe of the thyroid had a firm,
fairly noncircumscribed 8 9 7 9 5 cm solid mass strongly
adherent to the right laryngeal recurrent nerve; however,
there was no evidence of invasion to any other extra thy-
roidal invasion of the trachea/larynx or the esophagus/
pharynx. The thyroid was totally removed including the
right laryngeal recurrent nerve.
Three hours after surgery, the patient presented with
acute airway obstruction caused by paralysis of recurrent
nerve and laryngeal edema, and then an emergency tra-
cheostomy was performed.
Pathological findings of gross features showed that the
right lobe of the thyroid measured 7.5 9 6.7 9 3.5 cm.
The cut surfaces showed a well-capsulated nodule that
appeared cystic and hemorrhagic in the central sur-
rounded by solid tumor lesion colored gray-white-brown
(Fig. 3).
Fig. 1 Fine-needle aspiration specimen of the thyroid mass (Papa-
nicolaou stain; a 940, b 9200). Atypical cells were evident singly, as
well as in loose clusters. These cells had a high nucleocytoplasmic
ratio, round to irregular nuclei, a coarse chromatin pattern, and
prominent nucleoli
Fig. 2 An 18F-fluorodeoxyglucose positron emission tomography
computed tomographic (FDG-PET-CT) scan demonstrated a necrotic
lesion on the right side of the neck (a); max SUV was higher than
10 MBq/ml with central loss of FDG uptake (b)
Int Canc Conf J
123
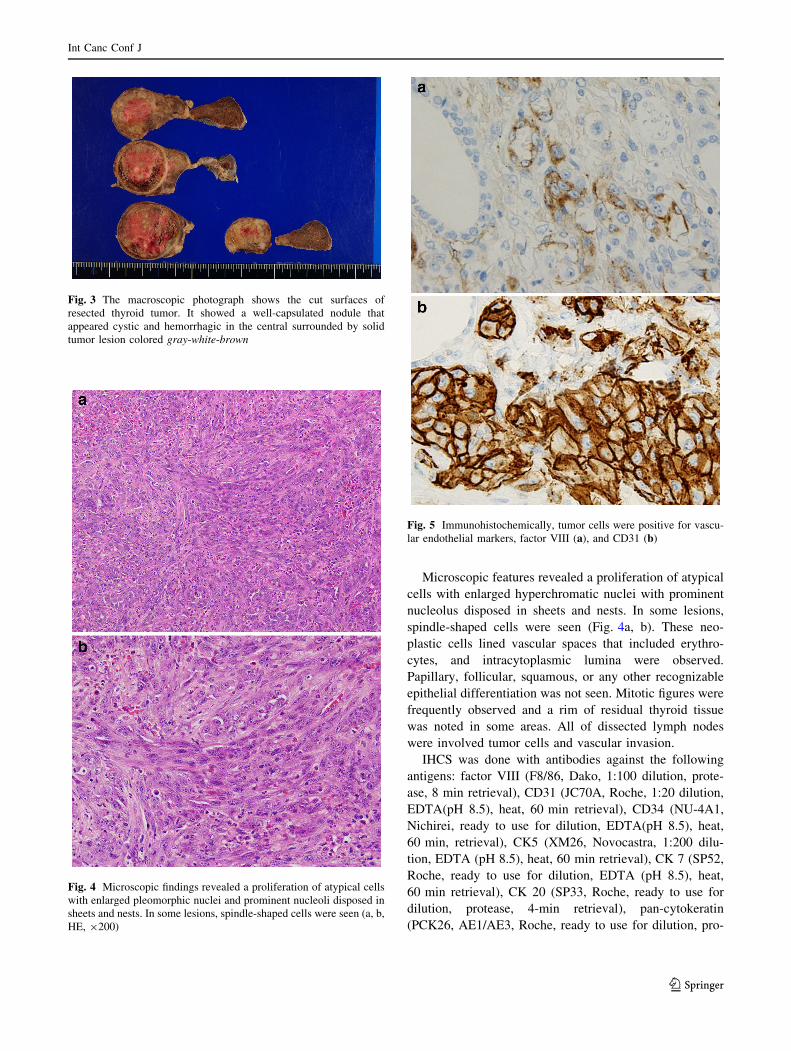
Microscopic features revealed a proliferation of atypical
cells with enlarged hyperchromatic nuclei with prominent
nucleolus disposed in sheets and nests. In some lesions,
spindle-shaped cells were seen (Fig. 4a, b). These neo-
plastic cells lined vascular spaces that included erythro-
cytes, and intracytoplasmic lumina were observed.
Papillary, follicular, squamous, or any other recognizable
epithelial differentiation was not seen. Mitotic figures were
frequently observed and a rim of residual thyroid tissue
was noted in some areas. All of dissected lymph nodes
were involved tumor cells and vascular invasion.
IHCS was done with antibodies against the following
antigens: factor VIII (F8/86, Dako, 1:100 dilution, prote-
ase, 8 min retrieval), CD31 (JC70A, Roche, 1:20 dilution,
EDTA(pH 8.5), heat, 60 min retrieval), CD34 (NU-4A1,
Nichirei, ready to use for dilution, EDTA(pH 8.5), heat,
60 min, retrieval), CK5 (XM26, Novocastra, 1:200 dilu-
tion, EDTA (pH 8.5), heat, 60 min retrieval), CK 7 (SP52,
Roche, ready to use for dilution, EDTA (pH 8.5), heat,
60 min retrieval), CK 20 (SP33, Roche, ready to use for
dilution, protease, 4-min retrieval), pan-cytokeratin
(PCK26, AE1/AE3, Roche, ready to use for dilution, pro-
Fig. 3 The macroscopic photograph shows the cut surfaces of
resected thyroid tumor. It showed a well-capsulated nodule that
appeared cystic and hemorrhagic in the central surrounded by solid
tumor lesion colored gray-white-brown
Fig. 4 Microscopic findings revealed a proliferation of atypical cells
with enlarged pleomorphic nuclei and prominent nucleoli disposed in
sheets and nests. In some lesions, spindle-shaped cells were seen (a, b,
HE, 9200)
Fig. 5 Immunohistochemically, tumor cells were positive for vascu-
lar endothelial markers, factor VIII (a), and CD31 (b)
Int Canc Conf J
123

tease, 4 min retrieval), SMA (1A4, Dako, 1:100 dilution),
S-100 protein (polyclonal, Roche, ready to use for dilu-
tion), c-kit (polyclonal, Dako, 1:50, EDTA (pH 8.5), heat,
60 min retrieval), TTF-1 (SPT24, Nichirei, ready to use for
dilution, EDTA (pH 8.5), heat, 60 min retrieval), Thyro-
globulin (DAK-Tg6, Dako, 1:100 dilution). All of them
were examined using I-VIEW DAB kit. The result of IHCS
of this tissue was intensely positive for vascular endothelial
markers, factor VIII (Fig. 5a), and CD31 (Fig. 5b), but not
CD34. IHCS was negative for CK 5, CK 7, and CK 20, but
partially positive for pan-cytokeratin. IHCS for SMA,
S-100 protein, c-kit, TTF-1, and thyroglobulin was nega-
tive. Based on the microscopic and immunohistochemical
findings, the patient’s neck tumor was diagnosed as an
epithelioid angiosarcoma.
The patient was scheduled for local radiation therapy,
but it was not performed because of an eventful postop-
erative course. Two weeks after the operation, bilateral
bloody pleural effusion was observed, and during the next
2 weeks, the patient required mechanical ventilation. Two
months after the surgery, the patient developed local
recurrence and rapid progress, and then died 3 months after
the surgery.
Discussion
Primary angiosarcoma is a rare tumor of the thyroid gland.
The highest prevalence of primary angiosarcoma is in
Switzerland and the alpine regions; it is rare in other parts
of the world. A search of acknowledged primary epitheli-
oid thyroid angiosarcomas from Asia in the English liter-
ature yielded only seven cases: two from Singapore and
one case each from Malaysia, China, Korea, Iran, and
Turkey [1, 7–12]. This is the first case reported in English
from Japan according to a PubMed search.
Kaur et al. [13] reviewed 47 cases of angiosarcoma of
the thyroid gland, described that the mean age of this
disease is 66.1 years old, and 79.2 % were 60 years or
more years of age. The most common presenting symptom
was rapid increase in a neck mass either with a long-
standing goiter or a new mass. Other common symptoms
are dyspnea, dysphagia, neck pain, weight loss [13]. This
patient complained of a rapid glowing mass and increasing
neck pain and finally hoarseness and severe cough with
bloody phlegm. We imagined that this case would be an
anaplastic carcinoma, but we had never expected a diag-
nosis of angiosarcoma because of its extremely rare
incidence.
There could have been options in treating the cancer had
it been anaplastic carcinoma, like chemotherapy or radia-
tion. However, as there was no definite cytological or
histological diagnosis of anaplastic carcinoma, an
operation was decided on under the informed consent of
the patient and the family, for three reasons: to get histo-
logical diagnoses of this rare case, and to keep the airways
of the patient and to improve the patient’s prognosis even
by a small chance.
Angiosarcoma of the thyroid can rapidly spread to the
lungs, which is the most common site for distant metas-
tasis, lymph nodes, brain, and intestines, and cause severe
bleeding [1, 14–16]. In the present case, non-symptomatic
bilateral small lung metastasis without FDG uptake was
determined preoperatively. After surgery, the lung metas-
tasis immediately worsened and caused bloody pleural
effusion.
Diagnosis of thyroid angiosarcoma can hardly be made
by aspiration cytology, in most cases reported previously
cytology was reported as inconclusive or nonspecific
malignancy or anaplastic/follicular thyroid cancer [13].
Whether thyroid angiosarcomas exist distinctly from
variants of anaplastic thyroid carcinoma with endothelial
differentiation is still controversial [10]. However, the
WHO classification of thyroid tumors, published in 2004,
has added angiosarcoma to the four traditional major tumor
groups [17] and more recent findings support the inde-
pendent existence of thyroid angiosarcomas based on IHCS
criteria, such as expression of endothelial-specific markers
by these tumors [18] and specific electron-microscopic
criteria [19]. In our case, IHCS revealed that the cytoplasm
of a large number of neoplastic cells was strongly positive
for factor VIII and CD31, but negative for several epithe-
lial, lymphocytic, oncofetal, and neuroendocrine markers.
In this case, IHCS of the fine-needle aspiration cytology
was slightly positive for thyroglobulin, but IHCS of the
specimen was negative for thyroglobulin. When non-fol-
licular cells exist near thyroid follicles, false-positive
staining is frequently observed because of antigen perme-
ation. Especially on cytological preparations, the phe-
nomenon more frequently occurs.
The differential diagnosis of this case is anaplastic or
poorly differentiated carcinoma with angiomatoid features.
Pathological findings did not show any evidence of ana-
plastic thyroid carcinoma, or epithelial structure, but the
evidence of a lot of atypical cells lined imitating blood
vessel, and IHCS of CD31 and factor VIII-related antigen,
which were found to be the most consistently vascular
endothelial. And some angiosarcoma showed partially
IHCS positivity for cytokeratin antigen [13]. Taken toge-
ther, these findings support the notion that our patient’s
tumor was indeed an angiosarcoma.
Thyroid angiosarcoma is known to be an aggressive
tumor with poor prognosis. Mortality rate was described up
to 90 % [13]. It is very difficult to assess the true mortality
rate and average survival time from previous reports
because of high variability in follow-up period. Metastatic
Int Canc Conf J
123

disease is associated with poor prognosis and limits the
mean survival time to a few months after diagnosis and
surgical treatment. Good prognosis seems to be related
mainly to the absence of distant metastasis and complete
dissection of the tumor [5]. In the present case, there was
extraglandular tumor invasion and lung metastasis, and the
patient died 3 months after surgery.
There is lack of data to suggest the best treatment for
angiosarcoma of the thyroid. However, studies have been
done to review the treatment options and outcome in cases
of angiosarcoma of the head and neck. Radical excision of
the tumor with adjunctive radiotherapy has been shown to
improve outcome and survival. Chemotherapy was
described as having undefined role in these studies [20–22].
Nowadays, newer treatments under investigation include
drugs targeting VEGF/VEGFR pathway (bevacizumab)
and tyrosine kinase inhibitors with activity against VEGFR
(sunitinib and pazopanib) [23].
In conclusion, we had experienced a very rare and
aggressive primary angiosarcoma of the thyroid. With the
luck of statistical data and guideline for treatment, unfor-
tunately we could not save his life. To provide a more
useful date for the future patients, collating known cases
and studying them are needed to find an effective treatment
for this kind of rare disease.
Conflict of interest Nana Rokutanda and the other co-authors have
no conflict of interest.
References
1. Chan YF, Ma L, Boey JH et al (1986) Angiosarcoma of the
thyroid: an immunohistochemical and ultrastructural study of a
case in a Chinese patient. Cancer 57:2381–2388
2. Ryska A, Ludvıkova M, Szepe P et al (2004) Epithelioid
hemangiosarcoma of the thyroid gland. Report of six cases from a
non-Alpine region. Histopathol 44:40–46
3. Eusebi V, Carcangiu ML, Dina R et al (1990) Keratin-positive
epithelioid angiosarcoma of thyroid. A report of four cases. Am J
Surg Pathol 14:737–747
4. Beer TW (1992) Malignant thyroid haemangioendothelioma in a
nonendemic goitrous region, with immunohistochemical evi-
dence of a vascular origin. Histopathology 20:539–541
5. Maiorana A, Collina G, Cesinaro AM et al (1996) Epithelioid
angiosarcoma of the thyroid. Clinicopathological analysis of
seven cases from non-Alpine areas. Virchows Arch 429:131–137
6. Proces S, Schroeyers P, Delos M et al (1998) Angiosarcoma of
the thyroid and concurrent hyperthyroidism. J Endocrinol In-
vestig 21:67–69
7. Goh SG, Chuah KL, Goh HK et al (2003) Two cases of epithe-
lioid angiosarcoma involving the thyroid and a brief review of
non-Alpine epithelioid angiosarcoma of the thyroid. Arch Pathol
Lab Med 127(2):70–73
8. Isa NM, James DT, Saw TH et al (2009) Primary angiosarcoma
of the thyroid gland with recurrence diagnosed by fine needle
aspiration: a case report. Diagn Cytopathol 37(6):427–432
9. Yilmazlar T, Kirdak T, Adim S et al (2005) A case of heman-
giosarcoma in thyroid with severe anemia due to bone marrow
metastasis. Endocr J 52(1):57–59
10. Yu J, Steiner FA, Muench JP et al (2002) Juxtathyroidal neck soft
tissue angiosarcoma presenting as an undifferentiated thyroid
carcinoma. Thyroid 12(5):427–432
11. Binesh F, Akhavan A, Navabii H et al (2011) Primary angio-
sarcoma of the thyroid gland in an young Iranian woman. BMJ
Case Rep. doi:10.1136/bcr.03.2011.4042
12. Kim NR, Ko YH, Sung CO et al (2003) A case of coexistent
angiosarcoma and follicular carcinoma of the thyroid. J Korean
Med Sci 18:908–913
13. Kaur A, Didolkar MS, Thomas A (2013) Angiosarcoma of the
thyroid: a case report with review of the literature. Endocr Pathol
24(3):156–161
14. Bandorski D, Arps H, Jaspersen D et al (2002) Severe intestinal
bleeding caused by intestinal metastases of primary angiosarcoma
of the thyroid gland. Gastroenterol 40:811–814
15. Rhomberg W, Bohler FK, Eiter H et al (1998) Malignant
hemangioendothelioma of the thyroid gland: new results on
pathogenesis, therapy and prognosis. Wien Klin Wochensch
110:479–484
16. Astl J, Duscova J, Limanova Z et al (2000) Hemangiosarcoma of
the thyroid gland: a case report. Neuroendocrinol Lett
21:213–216
17. De Lellis, RA, Ricardo VL, Philipp UH et al. (2004) Tumours of
endocrine organs. In: WHO classification of tumors. Geneva,
Switzerland: WHO :113–114
18. Ruchti C, Gerber HA, Schaffner T (1984) Factor VIII-related
antigen in malignant hemangioendothelioma of the thyroid:
additional evidence for the endothelial origin of this tumor. Am J
Clin Pathol 82:474–478
19. Carstens PH (1981) The Weibel-Palade body in the diagnosis of
endothelial tumors. Ultrastruct Pathol 2:315–325
20. Lydiatt WM, Shaha AR, Shah JP (1994) Angiosarcoma of the
head and neck. Am J Surg 168(5):451–454
21. McIntosh BC, Narayan D (2005) Head and neck angiosarcomas.
J Craniofac Surg 16(4):699–703
22. Abraham JA, Hornicek FJ, Kaufman AM et al (2007) Treatment
and outcome of 82 patients with angiosarcoma. Ann Surg Oncol
14(6):1953–1967
23. Park MS, Ravi V, Araujo DM (2010) Inhibiting the VEGF–
VEGFR pathway in angiosarcoma, epithelioid hemangioendo-
thelioma, and hemangiopericytoma/solitary fibrous tumor. Curr
Opin Oncol 22(4):351–355
Int Canc Conf J
123





























