Embed Size (px)
Citation preview

A comparative study of death anxiety inhospice and emergency nurses
S.A. Payne BA(Hons ) RGN DipN PhD CPsychol
Director of Research, Health Research Unit, School of Occupational Therapy
and Physiotherapy, University of Southampton
S.J. DeanMedical Student, Department of Psychology, University of Southampton,
Southampton
and C. Kalus BA(Hon) MSc AFBPS
Consultant Clinical Psychologist, The Rowans, Portsmouth, England
Accepted for publication 11 July 1997
PAYNE S.A., DEAN S.J. & KALUS C. (1998) Journal of Advanced Nursing 28(4), 700±706
A comparative study of death anxiety in hospice and emergency nurses
This paper describes a preliminary cross-sectional study which aimed to
compare levels of death anxiety and coping responses in palliative care and
accident and emergency (A & E) nurses. Forty-three nurses (23 from palliative
care and 20 from A & E) were recruited from a district general hospital and
nearby hospice. Both sites had the same mean annual death rate of 150 patients.
Death anxiety was measured by the Death Attitude Pro®le-Revised Question-
naire and coping responses were elicited by a semi-structured interview. As
hypothesized, hospice nurses had lower death anxiety and they were more
likely to recall both good and dif®cult experiences related to patient care. Unlike
the hospice nurses, a subgroup (20%) of A & E nurses reported that they were
unable to discuss problems with colleagues. The study has implications for the
development of institutional support for staff to enable nurses to provide good
quality care for dying patients and bereaved people.
Keywords: hospices, accident and emergency, nurses, death anxiety, coping
INTRODUCTION
All nurses face the dying and death of some of their
patients, and need to provide empathetic care to the
bereaved relatives. This is known to be a source of
occupational stress (Llewellyn & Payne 1995). It presents
not only a professional challenge but may also present
personal challenges. Certain characteristics of the death,
such as traumatic or mutilating injuries, or of the dying
person such as young patients, especially children, are
known to be problematic (Sanders 1993). Yet the quantity
and quality of pre-registration education on death and
dying is very variable (Field & Kitson 1986).
Quali®ed nurses select areas of specialization depending
upon personal preference and employment opportunities.
In acute hospitals, where the focus is on curing disease,
both societal attitudes and those of mainstream medicine
have contributed to health professionals often viewing
death as a failure (Carr & Merriman 1996). Palliative care
aims to offer an alternative or `better' way to die (McNamara
et al. 1995). Palliative care nurses aim to provide holistic
care for the terminally ill, focusing not only on the patient's
physical needs but with a greater emphasis on their social,
psychological and spiritual needs. For the majority of
Correspondence: S.A. Payne, Health Research Unit, School
of Occupational Therapy and Physiotherapy, University of Southampton,
High®eld, Southampton SO17 1BJ, England.
Journal of Advanced Nursing, 1998, 28(4), 700±706 Experience before and throughout the nursing career
700 Ó 1998 Blackwell Science Ltd

people death is only encountered a few times in their lives,
with the death of close friends and relatives. Hospice
nurses, however, are confronted by death and dying on a
daily basis. There is an assumption that nurses selecting
this area of work will feel comfortable with the open
acknowledgement of death and dying.
In comparison, accident and emergency (A & E) nursing
is concerned with providing life saving care of critically
injured or ill patients, although there is an acknowledge-
ment that not all patients survive and that their bereaved
families need support (British Association for Accident
and Emergency Medicine and the Royal College of Nursing
1995). Sudden bereavement is widely recognized as one of
the most traumatic life events but to date there has been
little research on its impact on A & E staff. These nurses
have to deal with many sudden and traumatic deaths and
with distraught relatives. Tye (1993) found that 52% of A
& E nurses felt unprepared for this aspect of their role.
Attitudes to Death
Neimeyer (1994) de®ned death anxiety as that experi-
enced in everyday life rather than in acute situations
where there are immediate threats to life. He suggested
that it has multiple components including: anticipating
one's self dead, fear of the process of dying and fear about
the death of signi®cant others. Most of the previous
research on the construct death anxiety has related to
feelings surrounding the death of the self rather than
objects of professional concern, namely patients (Neim-
eyer 1994). Health professionals are often in the position
of both having to deal with their personal feelings of death
threat and having to cope with death regularly in their
professional lives. Nichols (1984) has argued that doctors
and nurses cope with the emotional burden of their work
by distancing themselves from patients and concentrating
on the biomedical aspects of disease. While this might be
functional, it runs counter to current trends in nurse
education which emphasizes the psycho-social aspects of
care. A review of the literature by Neimeyer (1994)
indicates that health professionals with high levels of
death anxiety are more likely to use `avoiding' coping
strategies.
Neimeyer (1994) devised a multidimensional question-
naire to measure personal attitudes towards death. It
includes: fear of death, death avoidance, neutral accep-
tance (a state where death is neither feared or welcomed,
simply accepted), approach acceptance (a belief in a
happy afterlife), and escape acceptance which describes
death as a welcome alternative to a life full of pain and
suffering. Individuals may exist in any of the three states
of death acceptance. Alternatively individuals may hold a
strong fear of death or simply avoid thinking about it
altogether. Neimeyer suggests the personal attitudes we
hold about death strongly in¯uence how we live our lives.
Individuals who exhibit a high neutral acceptance or
approach acceptance can live happy, ful®lled lives. Those
with a strong fear of death may be unable to live life to the
full, particularly ®nding dif®culty with close relationships
as they may fear the death of those they love.
Recent research has suggested that hospice nurses have
low death anxiety and exhibit a greater comfort in caring
for the terminally ill, in contrast to hospital nurses who
exhibited high death anxiety and were reluctant to spend
time with dying patients (Carr & Merriman 1996). The
purpose of the study was to compare levels of death
anxiety between A & E nurses and palliative care nurses,
and to relate these to self-reported coping responses. It is
hypothesized that a nurse's skill and con®dence in pro-
viding good quality care to dying and bereaved people,
relates to not only his/her level of experience and training
but to personal attributes such as degree of death anxiety.
METHOD
Design
The study employed a cross-sectional design and was
conducted in the A & E Department of a large district
general hospital and at a nearby hospice in the south of
England. Within each unit the mean annual death rate was
150 deaths (» 3 per week). A questionnaire, followed by a
short structured interview, was used to obtain data from
nurses.
Participants
Sixty nurses from A & E (n � 30) and from the hospice
(n � 30) were invited to participate in the study by letter.
Measures
The Death Attitude Pro®le-Revised (DAP-R) (Wong et al.
1994a) is a 32-item standardized measure of attitudes
towards death comprising ®ve sub-scales of 6 or 7 items
each, assessing: fear of death, death avoidance, neutral
acceptance, approach acceptance and escape acceptance.
Participants rated each question on a 7-point scale, with
responses ranging from `strongly disagree' to `strongly
agree'. The scales demonstrate good reliability and valid-
ity, and there are established gender- and age-related
norms (Wong et al. 1994a).
A second questionnaire was devised for the study,
asking why nurses chose to work in that speciality, the
years spent in that speciality and to list any post-basic
quali®cations. A short semi-structured interview was
developed to elicit information about individual strategies
for coping with deaths in the clinical situation. There
were six questions:
� Could you tell me about a patient that you cared for
particularly well?
Experience before and throughout the nursing career Death anxiety in nurses
Ó 1998 Blackwell Science Ltd, Journal of Advanced Nursing, 28(4), 700±706 701

� In contrast could you tell me about a patient whose care
you found particularly dif®cult?
� If you have had a dif®cult day do you ®nd yourself
thinking about it when you go home?
� Is there someone you can talk to at home?
� What about at work?
� Do you feel that support is available if you need it?
Procedure
The collaboration of clinical managers was obtained at
each site. The DAP-R questionnaire was administered
individually to the nurses in an undisturbed private area
within each setting. They were left alone for 10 minutes to
complete the questionnaire. This was followed by the
short semi-structured interview which was audio-tape
recorded with participant's consent. All interviews were
performed by the same interviewer. Hospital Ethical
Committee permission was obtained. Con®dentiality and
the right to withdraw from the study at any time was
assured. Due to the sensitive nature of the research topic,
it was arranged that any participants who appeared to be
distressed would be referred to a clinical psychologist for
con®dential support.
Analysis
Data from the questionnaires were entered onto a spread-
sheet using the Statistical Package for Social Scientists
(SPSS). Responses to the 32 questions were coded from `1-
strongly agree' to `7 - strongly disagree'. Responses to the
questions were found to be normally distributed so data
were analysed using Student's t-tests. The data from the
DAP-R and content analyses were compared between the
hospice and A & E nurses to determine differences in
death anxiety and coping. Comparisons between the data
were undertaken to identify features of a supportive
environment.
The interviewer conducted a content analysis. One
interview was transcribed verbatim and this was used to
identify the type of responses made. Interview data were
categorized after careful and repeated examination of the
audio-tapes.
RESULTS
Characteristics of respondents
In total 43 nurses agreed to participate, 20 from A & E and
23 from palliative care, which is a response rate of 71á6%.
The A & E nurses had a mean age of 33 years (range 25±
50 years) and hospice nurses had a mean age of 37 years
(range 25±52 years), which was not statistically different
(t-test Ð 1á48, d.f. 38, P < 0á14). The mean number of years
spent in each speciality was: 4 years (range 1±17 years) for
A & E nurses; 3 years (range 1±10 years) for hospice
nurses. On average A & E nurses had two post-basic
quali®cations while hospice nurses had three. Nurses'
reasons for choice of speciality are shown in Table 1.
Differences between hospice and A & E nurseson death anxiety
From the previous literature the researchers hypothesized
that hospice nurses would feel more comfortable with
death than A & E nurses. This has been supported by the
data in relation to responses to 8 items from the DAP-R,
which are shown in Table 2, but in all other items (24) the
groups were not statistically signi®cantly different.
On the sub-scale of `death avoidance', three items (3, 12
and 19, shown in Table 2) signi®cantly discriminated
Table 1 Nurses' reasons for choice of speciality
Accident and Emergency (n = 20) Hospice (n = 23)
Rank Comments Responses Rank Comments Responses
1. Variety of patients 13 1. Dissatisfaction with care in hospital 7
2. Variety of procedures 10 2. Rewarding 7
3. Adrenaline/excitement/
experience of the
emergency situation
6 3. To have time to give
all aspects of care
6
4. Job satisfaction/enjoyment 3 4. Improve quality of life remaining 5
5. Lack of routine 2 5. Something I always wanted to do 5
6. Challenging 2 6. Work closely with properly 3
7. Busy environment 1 7. To ensure digni®ed death 3
8. Patients grateful for effort 1 8. Find subject of death fascinating 3
9. Like helping people 1 9. Personal experience of
terminal illness
2
10. More time to spend with
patients than on the wards
1 10. To be able to follow through
post-death with families
2
S.A. Payne et al.
702 Ó 1998 Blackwell Science Ltd, Journal of Advanced Nursing, 28(4), 700±706
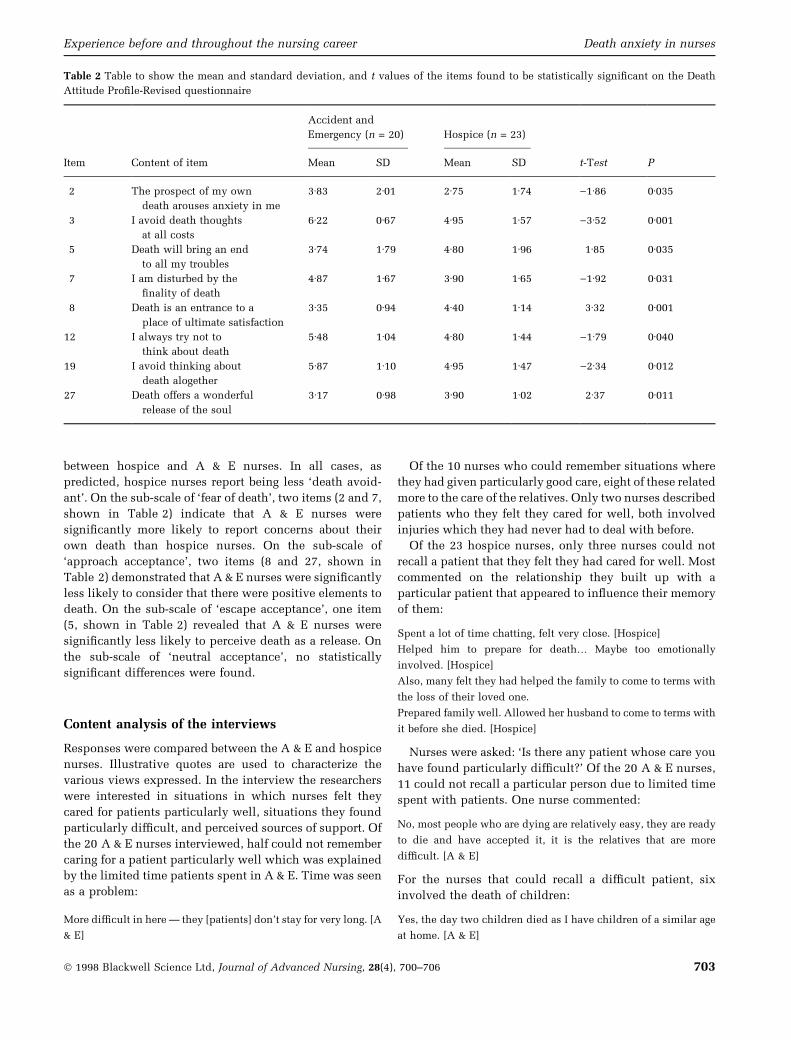
between hospice and A & E nurses. In all cases, as
predicted, hospice nurses report being less `death avoid-
ant'. On the sub-scale of `fear of death', two items (2 and 7,
shown in Table 2) indicate that A & E nurses were
signi®cantly more likely to report concerns about their
own death than hospice nurses. On the sub-scale of
`approach acceptance', two items (8 and 27, shown in
Table 2) demonstrated that A & E nurses were signi®cantly
less likely to consider that there were positive elements to
death. On the sub-scale of `escape acceptance', one item
(5, shown in Table 2) revealed that A & E nurses were
signi®cantly less likely to perceive death as a release. On
the sub-scale of `neutral acceptance', no statistically
signi®cant differences were found.
Content analysis of the interviews
Responses were compared between the A & E and hospice
nurses. Illustrative quotes are used to characterize the
various views expressed. In the interview the researchers
were interested in situations in which nurses felt they
cared for patients particularly well, situations they found
particularly dif®cult, and perceived sources of support. Of
the 20 A & E nurses interviewed, half could not remember
caring for a patient particularly well which was explained
by the limited time patients spent in A & E. Time was seen
as a problem:
More dif®cult in here Ð they [patients] don't stay for very long. [A
& E]
Of the 10 nurses who could remember situations where
they had given particularly good care, eight of these related
more to the care of the relatives. Only two nurses described
patients who they felt they cared for well, both involved
injuries which they had never had to deal with before.
Of the 23 hospice nurses, only three nurses could not
recall a patient that they felt they had cared for well. Most
commented on the relationship they built up with a
particular patient that appeared to in¯uence their memory
of them:
Spent a lot of time chatting, felt very close. [Hospice]
Helped him to prepare for death¼ Maybe too emotionally
involved. [Hospice]
Also, many felt they had helped the family to come to terms with
the loss of their loved one.
Prepared family well. Allowed her husband to come to terms with
it before she died. [Hospice]
Nurses were asked: `Is there any patient whose care you
have found particularly dif®cult?' Of the 20 A & E nurses,
11 could not recall a particular person due to limited time
spent with patients. One nurse commented:
No, most people who are dying are relatively easy, they are ready
to die and have accepted it, it is the relatives that are more
dif®cult. [A & E]
For the nurses that could recall a dif®cult patient, six
involved the death of children:
Yes, the day two children died as I have children of a similar age
at home. [A & E]
Table 2 Table to show the mean and standard deviation, and t values of the items found to be statistically signi®cant on the Death
Attitude Pro®le-Revised questionnaire
Accident and
Emergency (n = 20) Hospice (n = 23)
Item Content of item Mean SD Mean SD t-Test P
2 The prospect of my own
death arouses anxiety in me
3á83 2á01 2á75 1á74 )1á86 0á035
3 I avoid death thoughts
at all costs
6á22 0á67 4á95 1á57 )3á52 0á001
5 Death will bring an end
to all my troubles
3á74 1á79 4á80 1á96 1á85 0á035
7 I am disturbed by the
®nality of death
4á87 1á67 3á90 1á65 )1á92 0á031
8 Death is an entrance to a
place of ultimate satisfaction
3á35 0á94 4á40 1á14 3á32 0á001
12 I always try not to
think about death
5á48 1á04 4á80 1á44 )1á79 0á040
19 I avoid thinking about
death alogether
5á87 1á10 4á95 1á47 )2á34 0á012
27 Death offers a wonderful
release of the soul
3á17 0á98 3á90 1á02 2á37 0á011
Experience before and throughout the nursing career Death anxiety in nurses
Ó 1998 Blackwell Science Ltd, Journal of Advanced Nursing, 28(4), 700±706 703
Two nurses could remember patients because they
revived personal memories:
Yes, a patient with leukaemia as during that time my father was
dying from leukaemia. [A & E]
Yes, a patient with a brain tumour as I had a relative die of a brain
tumour, so I thought about that patient more. (A & E)
Issues surrounding the resuscitation of patients ap-
peared to cause stress for A & E nurses.
The 2-year-old drowning, we tried for 3 hours to resuscitate her
and the stress was increased by the mother being there. Nobody
agreed to it. [A & E]
One nurse commented that not knowing the outcome
was stressful:
No feedback from ITU so don't know outcome and therefore
worrying as don't know how they coped. [A & E]
Of the 23 hospice nurses, only two could not recall a
patient whose care they had found dif®cult. For one nurse
the particular patient who had stuck in her mind was a
patient she had witnessed die an unsatisfactory death in
hospital many years before. Five nurses could recall
patients whose symptoms were uncontrolled:
Lady with particularly dif®cult pain. Sought always for you to
make things better. [Hospice]
One nurse found a patient with two young children
dif®cult:
Very close to home. [Hospice]
Two nurses found the illness itself dif®cult to cope
with:
His physical state, something I had not experienced before, his
eyes and tongue were protruding. [Hospice]
Yes, because of illness felt out of my depth. [Hospice]
For other nurses it was the relatives that were a source
of stress:
Lot of trouble with will¼ family more concerned with will than
supporting patient. [Hospice]
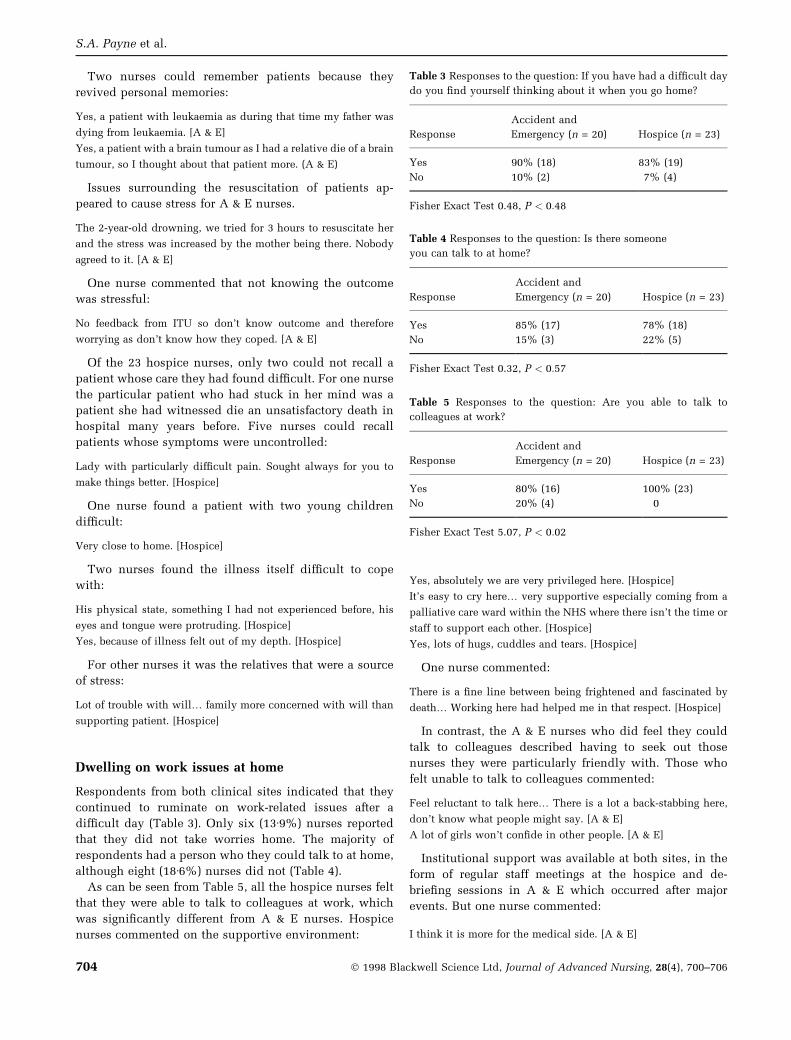
Dwelling on work issues at home
Respondents from both clinical sites indicated that they
continued to ruminate on work-related issues after a
dif®cult day (Table 3). Only six (13á9%) nurses reported
that they did not take worries home. The majority of
respondents had a person who they could talk to at home,
although eight (18á6%) nurses did not (Table 4).
As can be seen from Table 5, all the hospice nurses felt
that they were able to talk to colleagues at work, which
was signi®cantly different from A & E nurses. Hospice
nurses commented on the supportive environment:
Yes, absolutely we are very privileged here. [Hospice]
It's easy to cry here¼ very supportive especially coming from a
palliative care ward within the NHS where there isn't the time or
staff to support each other. [Hospice]
Yes, lots of hugs, cuddles and tears. [Hospice]
One nurse commented:
There is a ®ne line between being frightened and fascinated by
death¼ Working here had helped me in that respect. [Hospice]
In contrast, the A & E nurses who did feel they could
talk to colleagues described having to seek out those
nurses they were particularly friendly with. Those who
felt unable to talk to colleagues commented:
Feel reluctant to talk here¼ There is a lot a back-stabbing here,
don't know what people might say. [A & E]
A lot of girls won't con®de in other people. [A & E]
Institutional support was available at both sites, in the
form of regular staff meetings at the hospice and de-
brie®ng sessions in A & E which occurred after major
events. But one nurse commented:
I think it is more for the medical side. [A & E]
Table 3 Responses to the question: If you have had a dif®cult day
do you ®nd yourself thinking about it when you go home?
Response
Accident and
Emergency (n = 20) Hospice (n = 23)
Yes 90% (18) 83% (19)
No 10% (2) 7% (4)
Fisher Exact Test 0.48, P < 0:48
Table 4 Responses to the question: Is there someone
you can talk to at home?
Response
Accident and
Emergency (n = 20) Hospice (n = 23)
Yes 85% (17) 78% (18)
No 15% (3) 22% (5)
Fisher Exact Test 0.32, P < 0:57
Table 5 Responses to the question: Are you able to talk to
colleagues at work?
Response
Accident and
Emergency (n = 20) Hospice (n = 23)
Yes 80% (16) 100% (23)
No 20% (4) 0
Fisher Exact Test 5.07, P < 0:02
S.A. Payne et al.
704 Ó 1998 Blackwell Science Ltd, Journal of Advanced Nursing, 28(4), 700±706

DISCUSSION
This preliminary study, conducted at two sites, which
have the same mean annual death rate, has demonstrated
that on a self-report measure of death anxiety nurses have
fairly similar responses. However, in a quarter of the
responses there were statistically signi®cant differences.
As anticipated, A & E nurses are more likely to avoid
thinking about death than hospice nurses. They also
showed a greater fear of death and less acceptance than
hospice nurses. These results support those of Carr &
Merriman (1996) who found that hospice nurses had low
death anxiety compared to hospital nurses who showed
high death anxiety and a reluctance to spend time with
dying patients.
There are a number of reasons to be cautious in
interpreting the results. Although the study sites shared
the same mean death rate, there was obviously consider-
able variation in individual exposure to death. Future
studies should investigate this as the data from patients
indicated differences in perceived distress from witness-
ing deaths (Payne et al. 1996). The sample size was small
with a response rate of 71% which was due to the research
team's limited resources and time. As this was a cross-
sectional study, it is not possible to draw inferences about
causality. For example, were the differences found due to
intrinsic features of the nurses which led them to make
different career choices, or due to structural features of the
work environment which differ in the acknowledgement
and containment of staff distress? Future research could
usefully explore these issues.
This study relied on self-report measures and it is
important to remember that there are potential differences
between perceived methods of coping and actual behav-
iours. Nurses may be unwilling to report less socially
acceptable coping responses such as drug taking and
taking `sick' days off.
Folta (1965) suggested that people with a high death
anxiety are more likely to work within the health profes-
sion. While this may be true for A & E nurses who
exhibited high death anxiety, this does not follow for the
hospice nurses. When questioned about why they chose to
work in that particular speciality the hospice nurses gave
reasons such as `Find subject of death fascinating' and
`something I always wanted to do' as well as `personal
experience of terminal illness'. These responses do not
suggest an anxiety about death, instead they indicate a
comfort with dealing in death. In contrast when A & E
nurses were questioned about why they chose to work in
that speciality they gave reasons such as `busy, excite-
ment, lack of routine' and `variety of patients/procedures',
with no reference to wanting to work with dying patients.
It may be that it is people with a low death anxiety and
high approach acceptance of death who feel able to work
closely with dying patients, but for A & E nurses who do
not choose to work with the dying they may be faced with
death as an unfortunate consequence of the job.
The researchers suggest there is evidence from the
interview data that nurses varied on their ability and/or
willingness to re¯ect on the care provided. The pace of
nursing care is likely to be different between the two
specialities but all nurses are now encouraged to be
re¯ective practitioners. The description of distressing
features such as child deaths and traumatic deaths were
similar to those reported in previous research (Payne et al.
1996). Areas such as the death of young people and
problems during resuscitation appear to be stressful for
the A & E nurses, yet there appeared to be limited
opportunity to discuss these issues. The A & E Department
were aware of the training needs in bereavement of their
staff which, following the study, have been provided by
the researchers.
In conclusion, this study suggests that hospice nurses
appeared to have low death anxiety despite spending
almost every day with dying patients. The evidence shows
there is a need for an easily accessible and con®dential
support network within A & E. As well as a support
system, education in areas such as bereavement and
communication skills could be bene®cial since many of
the A & E nurses reported that some of their most dif®cult
times were spent with bereaved relatives. The experience
of palliative care health professionals in developing be-
reavement services and support systems for staff could
provide guidance in other health care settings.
Acknowledgements
The researchers would like to thank the nurses who took
part in the study. The research was funded by the Nuf®eld
Foundation.
References
Carr M. & Merriman M. (1996) Comparison of death attitudes
among hospice workers and health care professionals in other
settings. Omega 32(4), 287±301.
Field D. & Kitson C. (1986) Formal teaching about death and dying
in UK nursing schools. Nurse Education Today 6, 270±276.
Folta D. (1965) The perception of death. Nursing Research 14,
232.
Llewellyn S. & Payne S. (1995) Caring: the costs to nurses and
families. In Health Psychology: Processes and Application 2nd
edn (Broome A. & Llewellyn S.), Chapman & Hall, London, pp.
109±22.
McNamara B., Waddell C. & Colvin M. (1995) Threats to the good
death: the cultural context of stress and coping among hospice
nurses. Sociology of Health and Illness 17(2), 222±244.
Neimeyer R.A. (1994) Death Anxiety Handbook. Taylor and
Francis, Washington.
Nichols K.A. (1984) Psychological Care in Physical Illness. Croom
Helm, London.
Experience before and throughout the nursing career Death anxiety in nurses
Ó 1998 Blackwell Science Ltd, Journal of Advanced Nursing, 28(4), 700±706 705

Payne S., Hillier R., Langley-Evans A. & Roberts T. (1996) Impact
of witnessing death on hospice patients. Social Science and
Medicine 43(12), 1785±1794.
Payne S., Langley-Evans A. & Hillier R. (1996) Perceptions of a
`good' death: a comparative study of the views of hospice
patients and staff. Palliative Medicine 10, 307±321.
British Association for Accident and Emergency Medicine and
Royal College of Nursing (1995) Report of the Working Group.
Bereavement Care in A & E Departments. RCN, London.
Sanders C.M. (1993) Risk factors in bereavement outcome. In
Handbook of Bereavement (Stroebe M., Stroebe W. & Hansson
R. eds), Cambridge University Press, Cambridge, pp. 255±70.
Tye C. (1993) Sudden bereavement in Accident and Emergency:
the development and evaluation of a short educational course
for quali®ed nurses. Accident and Emergency Nursing 4, 88±93.
Wong P., Reker G. & Gesser G. (1994) Death Attitude Pro®le-
Revised. In Death Anxiety Handbook (Neimeyer R.A. ed.),
Taylor & Francis, Washington, pp. 121±48.
S.A. Payne et al.
706 Ó 1998 Blackwell Science Ltd, Journal of Advanced Nursing, 28(4), 700±706