Embed Size (px)
Citation preview
I 046 BRIT. J. SURG., 1966, Vol. 53, No. 12, DECEMBER
A COMPARISON OF THE RESULTS OF VAGOTOMY AND PYLOROPLASTY WITH VAGOTOMY
AND GASTRO-ENTEROSTOMY FOR CHRONIC DUODENAL ULCER BY B. R. HOPKINSON*
QUEEN ELIZABETH HOSPITAL, BIRMINGHAM
IN 1958 Burge and Pick reviewed 301 cases of vagotomy and gastro-enterostomy 8 years after operation. The results showed this procedure to be as good as partial gastrectomy for curing duodenal ulcers, with the advantages of a lower operative mortality and fewer late metabolic disturbances. Holt and Lythgoe (1965) compared the results of vagotomy and gastro-enterostomy with vagotomy and anterior pylorectomy, showing that in their hands vagotomy and anterior pylorectomy is the best operation available for chronic duodenal ulcer. This present series compares the symptomatic and meta- bolic findings after vagotomy with gastro-enterostomy and vagotomy with pyloroplasty.
At the Hallam Hospital, West Bromwich, between January, 1959, and January, 1965, 135 elective
discharge from hospital. One patient was a 61-year-old man who had had a vagotomy and gastro-enterostomy in 1959. Two years later he had had a negative laparo- tomy for suspected recurrent ulcer. He died of an unknown cause 4 years postoperatively. The other patient was a 49-year-old man who had had an anasto- motic ulcer which perforated 3 years after an appar- ently successful vagotomy and gastro-enterostomy in 1960. He was symptomless before and after the perforation and died 4 years postoperatively of carcinoma of the bronchus.
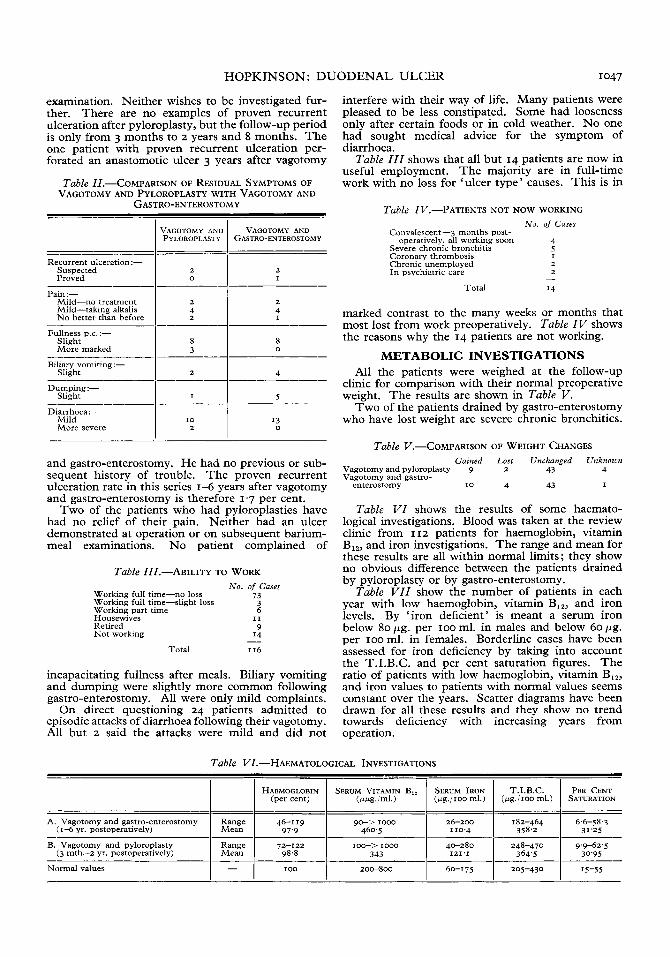
SYMPTOMATIC RESULTS The patients' symptoms were assessed using the
grading suggested by Visick (1948). Table Z shows that Grade I patients form the largest group; these
Table ~.-SYMPTOMATIC RESULTS IN 116 CASES OF VAGOTOMY AND DRAINAGE
PYLOROPLASTY GASTRO-ENTEROSTOMY REMARKS
97'4 per cent satisfactory
I 2.6 per cent unsatisfactory
VISICK'S GRADING
I. No symptoms
11. Mild symptoms, easily controlled
111s. Mild symptoms, not controlled, but satisfactory
IIIU. As IIIS, but unsatisfactory
IV. Not improved
I 58 I 58 I - Total
vagotomies were performed for chronic duodenal ulcer. They were drained by gastro-enterostomy in 73 cases and pyloroplasty in 62 cases. The main indication for surgery has been the clinical assess- ment, supported where possible by a barium meal demonstrating a duodenal ulcer. Few gastric acid studies were done before or after vagotomy. The technique used was total subdiaphragmatic vagotomy with drainage of the stomach by retrocolic short-loop isoperistaltic gastro-enterostomy or by a single-layer closure pyloroplasty.
All the patients were invited to attend for review between 24 Feb. and 25 March, 1965. One hundred and sixteen of them came and I I Z gave blood for haematological investigation. Three patients are known to have died and 2 have left the country, leaving 14 patients untraced.
There was only I death during the postoperative period; a 78-year-old lady dying from a presumed coronary thrombosis on the eighth day.
Both of the patients who died some years after vagotomy had gastric troubles following their initial
~~~
* Present address: Buswell Research Fellow, E. J. Meyer, Memorial Hospital, 462 Grider St., Buffalo, N. Y. 14226, U.S.A.
have no symptoms at all. Grade I1 patients form the next largest group; they have occasional symptoms such as a little fullness after meals or mild dumping. The one Grade IIIU patient had a vagotomy and gastro-enterostomy in 1962 for pyloric stenosis. He still has some residual epigastric pain, but declined further investigations. The two Grade IV patients had no ulcer demonstrated at operation or on barium: meal examination since. They are both errors of selection. These figures show that a few more patients are symptom-free after pyloroplasty than gastro-enterostomy. Of the patients 97.4 per cent are classed as having satisfactory results.
RECURRENT ULCERATION AND RESIDUAL SYMPTOMS
Table ZZ compares the residual symptoms of those patients on whom gastro-enterotomy or pyloroplasty was performed. Recurrent ulceration is suspected in 2 patients after pyloroplasty, but barium meals have not confirmed this. Both patients refuse further investigation.
Two patients are suspected of having recurrent ulceration after gastro-enterostomy ; one had a barium-meal examination which failed to show an ulcer and the other failed to attend for radiological
HOPKINSON: DUODENAL ULCER I047
Range Mean
examination. Neither wishes to be investigated fur- ther. There are no examples of proven recurrent ulceration after pyloroplasty, but the follow-up period is only from 3 months to 2 years and 8 months. The one patient with proven recurrent ulceration per- forated an anastomotic ulcer 3 years after vagotomy
Table ZZ.-COMPARISON OF RESIDUAL SYMPTOMS OF
GASTRO-ENTEROSTOMY VAGOTOMY AND PYLOROPLASTY WITH VAGOTOMY AND
~~~ ~
HAEMOGLOBIN SERUM VITAMIN B,, SERUM IRON T.I.B.C. PER CENT (per cent) (wg./ml.) (ug./ioo ml.) (ug./Ioo ml.) SATURATION
46-119 90-> 1000 26-200 182-464 6.6-58.3 97.9 460.5 110.4 358.2 31'25
VAGOTOMY AND VAGOTOMY AND PYLOROPLASTY GASTRO-ENTEROSTOMY
I Recurrent ulceration :-
Suspected Proved - I-- l-
Pain:- Mild-no treatment Mild-taking alkalis No better than before
2 4 2
2 4 I
Fullness p.c. :-
More Slight marked I : I 4 Slight _ _ _ _ _ _ ~ - - ! : Biliary vomiting:-
5 Dumping :-
Slight
Diarrhoea :- I I: Mild More severe
13 0
and gastro-enterostomy. He had no previous or sub- sequent history of trouble. The proven recurrent ulceration rate in this series 1-6 years after vagotomy and gastro-enterostomy is therefore 1'7 per cent.
Two of the patients who had pyloroplasties have had no relief of their pain. Neither had an ulcer demonstrated at operation or on subsequent barium- meal examinations. No patient complained of
Table ZZZ.--ABILITY TO WORK
Working full time-no loss Working full time-slight loss Working part time Housewives Retired Not working
No. of Cases 73
3 6
9 I4
I1
- Total I 16
incapacitating fullness after meals. Biliary vomiting and dumping were slightly more common following gastro-enterostomy. All were only mild complaints.
On direct questioning 24 patients admitted to episodic attacks of diarrhoea following their vagotomy. All but z said the attacks were mild and did not
interfere with their way of life. Many patients were pleased to be less constipated. Some had looseness only after certain foods or in cold weather. No one had sought medical advice for the symptom of diarrhoea.
Table ZZZ shows that all but 14 patients are now in useful employment. The majority are in full-time work with no loss for 'ulcer type' causes. This is in
Table ZV.-pATIENTS NOT NOW WORKING No. of Cases
Convalescent-3 months post-
Severe chronic bronchitis 5 Coronary thrombosis I Chronic unemployed 2 In psychiatric care
Total I4
operatively. all working soon 4
2 -
marked contrast to the many weeks or months that most lost from work preoperatively. Table ZV shows the reasons why the 14 patients are not working.
METABOLIC INVESTIGATIONS All the patients were weighed at the follow-up
clinic for comparison with their normal preoperative weight. The results are shown in Table V.
Two of the patients drained by gastro-enterostomy who have lost weight are severe chronic bronchitics.
Table V.-COMPARISON OF WEIGHT CHANGES Gained LOSI Unchanged Unknown
Vagotomy and pyloroplasty 9 2 43 4 Vagotomy and gastro-
enterostomy I0 4 43 I
Table VZ shows the results of some haemato- logical investigations. Blood was taken at the review clinic from I 12 patients for haemoglobin, vitamin B,,, and iron investigations. The range and mean for these results are all within normal limits; they show no obvious difference between the patients drained by pyloroplasty or by gastro-enterostomy.
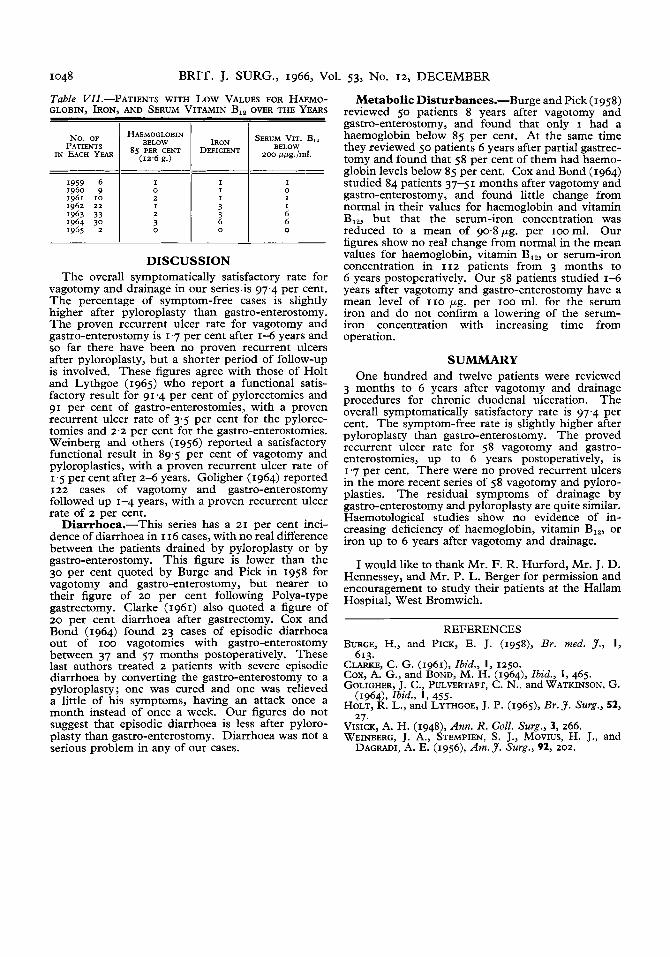
Table VIZ show the number of patients in each year with low haemoglobin, vitamin B,,, and iron levels. By 'iron deficient' is meant a serum iron below 80 pg. per IOO ml. in males and below 60 pg. per IOO ml. in females. Borderline cases have been assessed for iron deficiency by taking into account the T.I.B.C. and per cent saturation figures. The ratio of patients with low haemoglobin, vitamin B,,, and iron values to patients with normal values seems constant over the years. Scatter diagrams have been drawn for all these results and they show no trend towards deficiency with increasing years from operation.
Table VZ.-HAEMATOLOGICAL INVESTIGATIONS
A. Vagotomy and gastro-enterostomy (1-6 yr. postoperatively)
72-122 I 4-280 I 248-470 1 9.9-62.5 (3 rnth.-z yr. postoperatively) 343 121'1 364.5 30.95
B. Vagotomy and pyloroplasty
Normal values 1 - I 100 1 200-800 I 60-175 I 205-430 I 15-55
1048 BRIT. J. SURG., 1966, Vol. 53, No. 12, DECEMBER
IRON DEFICIENT
Table PATIENTS WITH Low VALUES FOR HAEMO- GLOBIN, IRON, AND SERUM VITAMIN B,, OVER THE YEARS
SERUM VIT. B,,
200 wpg./mI. BELOW
No. OF PATIENTS
IN EACH YEAR
HAEMOGLOBIN
( 1 2 . 6 9.)
BELOW 8s PER CENT
I 0 2 I 2
0 3
DISCUSSION The overall symptomatically satisfactory rate for
vagotomy and drainage in our series is 97.4 per cent. The percentage of symptom-free cases is slightly higher after pyloroplasty than gastro-enterostomy. The proven recurrent ulcer rate for vagotomy and gastro-enterostomy is 1'7 per cent after 1-6 years and so far there have been no proven recurrent ulcers after pyloroplasty, but a shorter period of follow-up is involved. These figures agree with those of Holt and Lythgoe (1965) who report a functional satis- factory result for 91.4 per cent of pylorectomies and 91 per cent of gastro-enterostomies, with a proven recurrent ulcer rate of 3.5 per cent for the pylorec- tomies and 2.2 per cent for the gastro-enterostomies. Weinberg and others (1956) reported a satisfactory functional result in 89.5 per cent of vagotomy and pyloroplasties, with a proven recurrent ulcer rate of 1.5 per cent after 2-6 years. Goligher (1964) reported 122 cases of vagotomy and gastro-enterostomy followed up 1-4 years, with a proven recurrent ulcer rate of 2 per cent.
Diarrhoea.-This series has a 21 per cent inci- dence of diarrhoea in I 16 cases, with no real difference between the patients drained by pyloroplasty or by gastro-enterostomy. This figure is lower than the 30 per cent quoted by Burge and Pick in 1958 for vagotomy and gastro-enterostomy, but nearer to their figure of 20 per cent following Polya-type gastrectomy. Clarke (1961) also quoted a figure of 20 per cent diarrhoea after gastrectomy. Cox and Bond (1964) found 23 cases of episodic diarrhoea out of IOO vagotomies with gastro-enterostomy between 37 and 57 months postoperatively. These last authors treated 2 patients with severe episodic diarrhoea by converting the gastro-enterostomy to a pyloroplasty; one was cured and one was relieved a little of his symptoms, having an attack once a month instead of once a week. Our figures do not suggest that episodic diarrhoea is less after pyloro- plasty than gastro-enterostomy. Diarrhoea was not a serious problem in any of our cases.
Metabolic Disturbances-Burge and Pick (1958) reviewed 50 patients 8 years after vagotomy and gastro-enterostomy, and found that only I had a haemoglobin below 85 per cent. At the same time they reviewed 50 patients 6 years after partial gastrec- tomy and found that 58 per cent of them had haemo- globin levels below 85 per cent. Cox and Bond (1964) studied 84 patients 37-51 months after vagotomy and gastro-enterostomy, and found little change from normal in their values for haemoglobin and vitamin B,,, but that the serum-iron concentration was reduced to a mean of 90.8pg. per ~ o o m l . Our figures show no real change from normal in the mean values for haemoglobin, vitamin B,,, or serum-iron concentration in 112 patients from 3 months to 6 years postoperatively. Our 58 patients studied 1-6 years after vagotomy and gastro-enterostomy have a mean level of I I O pg. per IOO ml. for the serum iron and do not confirm a lowering of the serum- iron concentration with increasing time from operation.
SUMMARY One hundred and twelve patients were reviewed
3 months to 6 years after vagotomy and drainage procedures for chronic duodenal ulceration. The overall symptomatically satisfactory rate is 97.4 per cent. The symptom-free rate is slightly higher after pyloroplasty than gastro-enterostomy. The proved recurrent ulcer rate for 58 vagotomy and gastro- enterostomies, up to 6 years postoperatively, is 1.7 per cent. There were no proved recurrent ulcers in the more recent series of 58 vagotomy and pyloro- plasties. The residual symptoms of drainage by gastro-enterostomy and pyloroplasty are quite similar. Haemotological studies show no evidence of in- creasing deficiency of haemoglobin, vitamin B,,, or iron up to 6 years after vagotomy and drainage.
I would like to thank Mr. F. R. Hurford, Mr. J. D. Hennessey, and Mr. P. L. Berger for permission and encouragement to study their patients at the Hallam Hospital, West Bromwich.
REFERENCES BURGE, H., and PICK, E. J. (1999, Br. med. J . , I,
CLARKE, C. G. (1961), Zbid., I, 1250. Cox, A. G., and BOND, M. H. (1964), Zbid., I , 465. GOLIGHER, J. C., PULVERTAFT, C. N., and WATKINSON, G.
(1964)~ Zbid., 1, 455. HOLT, R. L., and LYTHGOE, J. P. (1965), Br.J. Surg., 52,
27. VISICK, A. H. (1948), Ann. R. Coll. Surg., 3, 266. WEINBERG, J. A., STEMPIEN, S. J., MOVIUS, H. J., and
DAGRADI, A. E. (1956), Arn.J. Surg., 92, 202.
613.






![Review Article Enterostomy Closure after Acute Abdomen in Neonate … · 2019. 4. 4. · complications such as cholestasis, liver failure, and central catheter infection [27]. Refeeding](https://img.pdfslide.net/doc/110x75/60348540bcf2ac0dd319b18e/review-article-enterostomy-closure-after-acute-abdomen-in-neonate-2019-4-4.jpg)






















