Embed Size (px)
Citation preview
Journal of Surgical Research 159, 468–473 (2010)doi:10.1016/j.jss.2009.04.020
ASSOCIATION FOR ACADEMIC SURGERY
A Different View of Lactate in Trauma Patients: Protecting the Injured Brain
Elizabeth L. Cureton, M.D.,* Rita O. Kwan, M.D., M.P.H.,* Kristopher C. Dozier, M.D.,* Javid Sadjadi, M.D.,*Jay D. Pal, M.D., Ph.D.,† and Gregory P. Victorino, M.D.*,1
*Department of Surgery, University of California San Francisco-East Bay, Alameda County Medical Center, Oakland, California;and †Department of Surgery, Duke University, Durham, North Carolina
Submitted for publication January 9, 2009
Background. The relationship between lactate andhead injury is controversial. We sought to determinethe relationship between initial serum lactate, sever-ity of head injury, and outcome. We hypothesizedthat lactate is elevated in head injured patients, andthat initial serum lactate increases as the severity ofhead injury increases. Furthermore, lactate may beneuroprotective and improve neurologic outcomes.
Materials and Methods. We identified normotensiveadult patients over a 6-y period at our university-basedurban trauma center with isolated blunt head injury.We performed univariate and multivariate analysisto examine the relationship between lactate and Glas-gow coma scale (GCS). The correlation of admissionlactate with survival and neurologic function wasalso examined.
Results. There were 555 patients who met study cri-teria. While controlling for injury severity score andage, increased lactate was associated with more severehead injury (P < 0.0001). The admission lactate was2.2 ± 0.07, 3.7 ± 0.7, and 4.7 ± 0.8 mmol/L in patientswith mild, moderate, and severe head injury respec-tively (P < 0.01). Patients with moderate or severehead injury and an admission lactate > 5 were morelikely to have a normal mental status on discharge(P < 0.0001).
Conclusions. In normotensive isolated head injuredpatients, there was an increase in serum lactate ashead injuries became more severe. Since lactate isa readily available fuel source of the injured brain,this may be a mechanism by which brain function ispreserved in trauma patients. Elevations in lactatedue to anaerobic metabolism in trauma patients may
1 To whom correspondence and reprint requests should be ad-dressed at Department of Surgery, University of California San Fran-cisco-East Bay, Alameda County Medical Center, UCSF-East Bay,1411 East 31st Street, Oakland, CA 94602. E-mail: [email protected].
0022-4804/09 $36.00� 2010 Elsevier Inc. All rights reserved.
468
have beneficial effects by protecting the brain duringinjury. � 2010 Elsevier Inc. All rights reserved.
Key Words: lactate; head injury.
INTRODUCTION
Lactate has traditionally been thought of as a meta-bolic waste product indicative of a potentially poor out-come. It is released during anaerobic metabolism and istherefore a marker of hypoperfusion and shock. In addi-tion to ischemia and hypoxia, lactate may be elevateddue to other etiologies, including circumstances thatmay either increase lactate production (such as whiteblood cells or certain medications) or decrease its clear-ance (such as liver or kidney failure) [1]. Lactate’s in-ability to correlate with other indicators of injuryseverity and to predict poor clinical outcome has alsobeen reported [2]. Furthermore, since neurons exposedto lactate concentrations of 20 mmol/L for 6 h at normalpH are not damaged [3], it is unclear whether lactateitself is dangerous to cells. It may be the acidosis, result-ing from proton release from the hydrolysis of adeno-sine triphosphate (ATP) in cells with overwhelmedbuffering capacity, which causes toxicity [4]. Lactate,therefore, may not be as detrimental as it has been con-ventionally thought to be.
The relationship between lactate levels and head in-jury is controversial. Like other tissues, lactate can be re-leased from the injured brain as a result of ischemia,hypoxia, and resulting anaerobic respiration. Lactatelevels increase in the blood and cerebrospinal fluid aftersevere head injury. Blood levels normalize in24 to 36 h af-ter acute head injury, but cerebrospinal fluid levels mayremain high [5]. Interestingly, lactate levels that remainelevated in cerebrospinal fluid as blood levels have nor-malized, are associated with death and poor outcomes [6].

CURETON ET AL.: LACTATE AND HEAD INJURY 469
Because of these controversies, we wondered aboutthe correlation of admission venous serum lactatelevels to head injury severity. Furthermore, we askedif this circulating systemic lactate would relate to out-come after head injury. We hypothesized that admis-sion lactate would be higher in patients with moresevere head injury, and that given a certain severityof head injury, elevated lactate may be neuroprotective.
MATERIALS AND METHODS
Institutional review board approval was obtained for this study. Aretrospective analysis was performed of adult trauma patients atour university-based urban trauma center between January 1, 1998and September 30, 2003. The study was limited to patients with clin-ically isolated blunt head injury. We only included patients who werenormotensive on arrival to the trauma bay and throughout their stayin the emergency room, to remove the confounding factor of increasesin lactate due to blood loss. We excluded patients with known pre-existing medical conditions that could affect lactate levels, includingrenal or hepatic insufficiency and diabetes. Therefore, any patientwith a diagnosis of renal or hepatic insufficiency or diabetes listedby ICD-9 code, either pre-existing or during the hospital stay, was ex-cluded. We did not review individual blood sugar levels for exclusionof diabetic patients for this study. Venous lactate values were drawnroutinely upon admission on patients arriving in the trauma bay.
We performed univariate and multivariate analyses to examine therelationship between admission lactate and admission Glasgow comascale (GCS), while controlling for injury severity score (ISS) and age.Mild head injury was defined as GCS 13–15, moderate head injurywas defined as GCS 9–12, and severe injury was defined as GCS3–8. Patients with mild head injury all had loss of consciousness.The GCS for intubated patients was determined by the GCS just priorto intubation. We defined neuroprotective as having an improved out-come in terms of neurological status (GCS) at the time of dischargefrom our hospital.
We also examined the outcomes of patients at hospital dischargebased on the records of our trauma registry and patient chartswhen available. Patients were categorized as either dead, normal(GCS of 15), or abnormal (GCS < 15) at the time of discharge fromour facility (including discharge to home or to another facility).Fisher’s exact test and the Mann-Whitney test were used for categor-ical variables, and the Student’s t-test, Mann-Whitney test, and Anal-ysis of Variance were used to study continuous variables asappropriate. Logistic regression was also performed. The softwareused was Stat View Version 5.0.1 (1992–1998, Cary, NC).
RESULTS
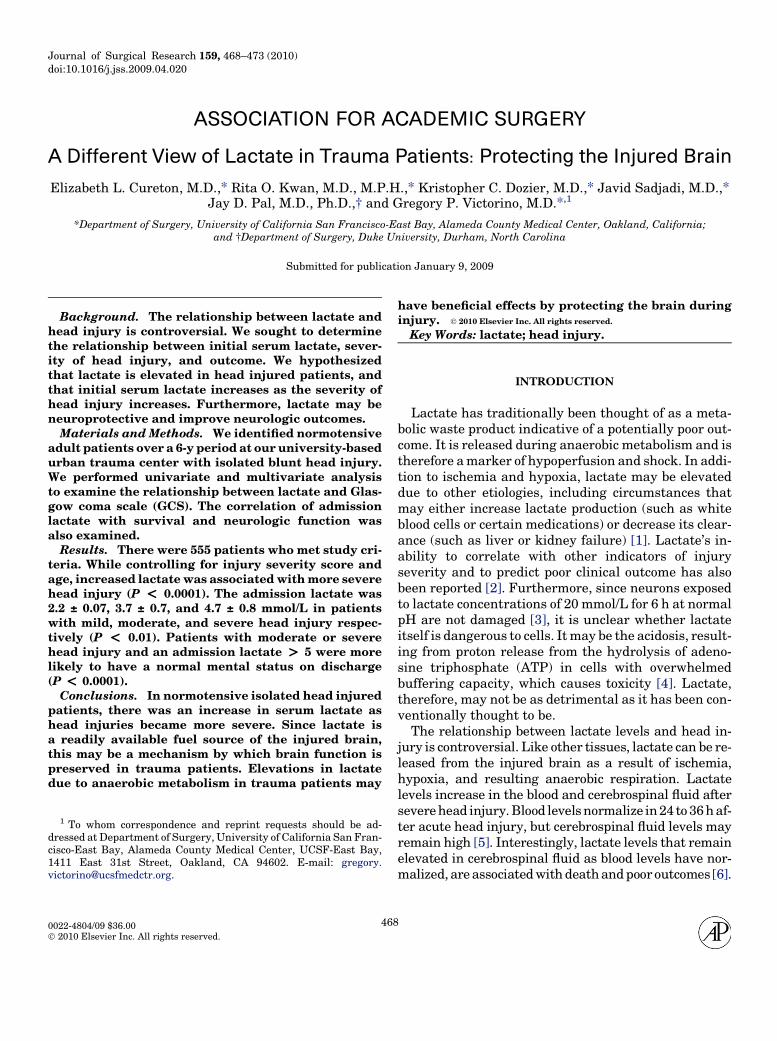
A total of 555 isolated head injury patients were in-cluded in the analysis. Four hundred seventy-one pa-tients had mild head injury (GCS 13–15), 34 patientshad moderate head injury (GCS 9–12), and 46 patientshad severe head injury (GCS 3–8). Specific head in-juries ranged in all severity categories from subduraland subarachnoid hemorrhage, to skull fractures, tolarge numbers of ‘unspecified’ head or intracranial in-juries. Concussions predominated in the mild head in-jury group. All patients had isolated head injury withabbreviated injury score recorded for head injury; nopatients were included who had injuries in any othercategories aside from skin abrasions with an AIS of 1.
Characteristics of patients with mild, moderate, and se-vere head injury as well as survivors versus non-survivors can be seen in Table 1.
To answer the question if lactate was related to sever-ity of head injury, we analyzed the mean lactate in pa-tients with mild, moderate, and severe head injury. Themean lactate increased with increasing severity of headinjury: patients with mild head injury had a mean ad-mission lactate of 2.2 6 0.07 mmol/L, while patientswith moderate and severe head injury had mean admis-sion lactates of 3.7 6 0.7 and 4.7 6 0.8 mmol/L, respec-tively (Fig. 1). Lactate was elevated (>2 mmol/L) in 44%of patients with mild head injury, 62% of patients withmoderate head injury, and 82% of patients with severehead injury (P < 0.04). While controlling for ISS andage, logistic regression showed that severity of head in-jury, as measured by GCS, was an independent risk fac-tor for elevated lactate (P < 0.0001). However, elevatedlactate did not correlate with elevated ISS and viceversa: the mean lactate was 2.9 mmol/L in patientswith an ISS � 15 and 2.5 mmoL/L (P ¼ 0.3) in patientswith an ISS > 15. The mean ISS was 5 in both patientgroups with lactate � 5 and > 5 (P ¼ 0.1). Similarly,analysis by AIS showed a lack of correlation with lac-tate: the mean AIS in patients with lactate � 5 was2.3 6 0.03, and the mean lactate in patients with lactate> 5 was 2.4 6 0.1 (P ¼ 0.2).
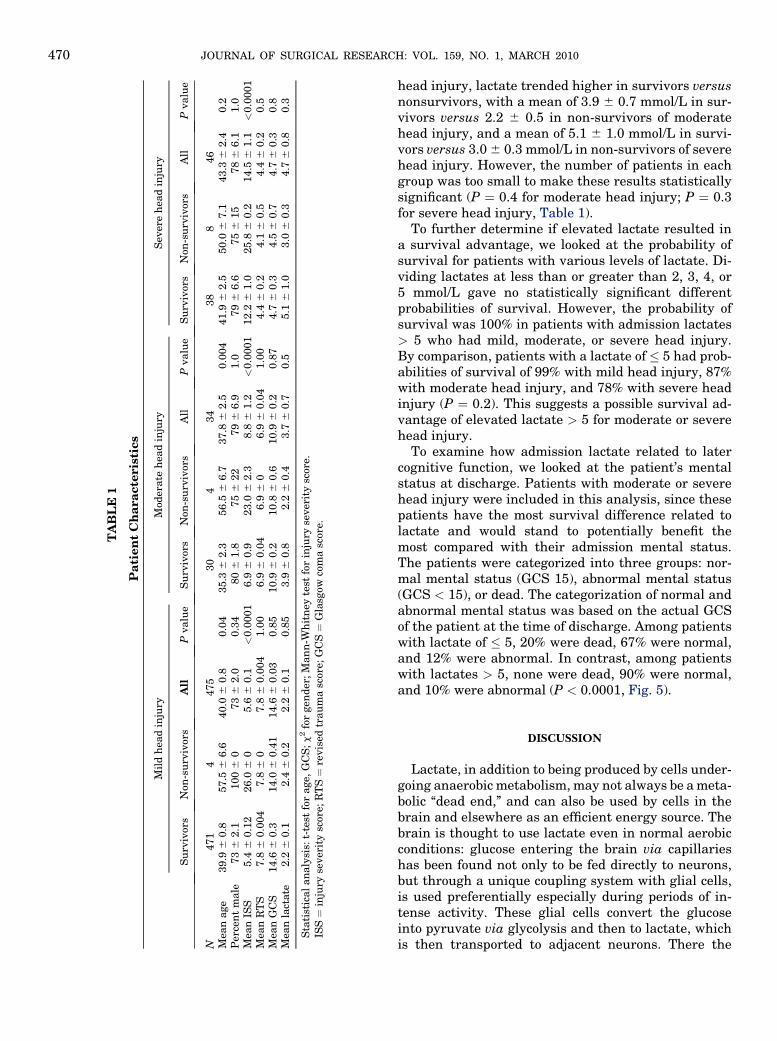
To investigate whether the elevated lactates could beexplained by alcohol or seizures, we looked at the rela-tionship between elevated lactate, blood alcohol concen-tration, and seizures. The mean alcohol concentrationin patients with lactates � 5 is 0.18% versus 0.47% inpatients with lactates > 5 (P ¼ 0.4). The mean lactatein patients with alcohol concentrations � 0.08 is 3.2 6
0.4 mmol/L versus 2.7 6 0.1 mmol/L in patients with al-cohol concentrations> 0.08 (P¼ 0.08) (Fig. 2). Althoughseizures were more common in patients with lactates> 5 in mild head injury (28% versus 3% in patientswith lactates� 5, P< 0.0001), there was no statisticallysignificant difference between the incidence of seizuresin moderate head injury (0% with lactates > 5 versus3% with lactates � 5, P ¼ 1.0), or in severe head injury(25% with lactates > 5 versus 5% with lactates � 5,P ¼ 0.1) (Fig. 3).
We then looked at the outcomes of the patients as re-lated to admission lactates. Elevated lactates by theconventional >2 mmol/L were observed more com-monly in non-survivors than survivors (75% versus48%, P ¼ 0.03). However, among patients with all de-grees of head injury, the admission lactates of survivorswere clustered around a smaller range of lower valuescompared with non-survivors (Fig. 4). The mean lac-tates of patients with mild head injury who survivedwere 2.2 6 0.07 mmol/L versus 2.4 6 0.2 in patientswho died (P ¼ 0.9). However, in moderate or severe
TA
BL
E1
Pa
tien
tC
ha
ra
cte
ris
tics
Mil
dh
ead
inju
ryM
oder
ate
hea
din
jury
Sev
ere
hea
din
jury
Su
rviv
ors
Non
-su
rviv
ors
All
Pvalu
eS
urv
ivor
sN
on-s
urv
ivor
sA
llP
valu
eS
urv
ivor
sN
on-s
urv
ivor
sA
llP
valu
e
N471
4475
30
434
38
846
Mea
nage
39.9
60.8
57.5
66.6
40.0
60.8
0.0
435.3
62.3
56.5
66.7
37.8
62.5
0.0
04
41.9
62.5
50.0
67.1
43.3
62.4
0.2
Per
cen
tm
ale
73
62.1
100
60
73
62.0
0.3
480
61.8
75
622
79
66.9
1.0
79
66.6
75
615
78
66.1
1.0
Mea
nIS
S5.4
60.1
226.0
60
5.6
60.1
<0.0
001
6.9
60.9
23.0
62.3
8.8
61.2
<0.0
001
12.2
61.0
25.8
60.2
14.5
61.1
<0.0
001
Mea
nR
TS
7.8
60.0
04
7.8
60
7.8
60.0
04
1.0
06.9
60.0
46.9
60
6.9
60.0
41.0
04.4
60.2
4.1
60.5
4.4
60.2
0.5
Mea
nG
CS
14.6
60.3
14.0
60.4
114.6
60.0
30.8
510.9
60.2
10.8
60.6
10.9
60. 2
0.8
74.7
60.3
4.5
60.7
4.7
60.3
0.8
Mea
nla
ctate
2.2
60.1
2.4
60.2
2.2
60.1
0.8
53.9
60.8
2.2
60.4
3.7
60.7
0.5
5.1
61.0
3.0
60.3
4.7
60.8
0.3
Sta
tist
ical
an
aly
sis:
t-te
stfo
rage,
GC
S;
c2
for
gen
der
;M
an
n-W
hit
ney
test
for
inju
ryse
ver
ity
scor
e.IS
S¼
inju
ryse
ver
ity
scor
e;R
TS¼
revis
edtr
au
ma
scor
e;G
CS¼
Gla
sgow
com
asc
ore.
JOURNAL OF SURGICAL RESEARCH: VOL. 159, NO. 1, MARCH 2010470
head injury, lactate trended higher in survivors versusnonsurvivors, with a mean of 3.9 6 0.7 mmol/L in sur-vivors versus 2.2 6 0.5 in non-survivors of moderatehead injury, and a mean of 5.1 6 1.0 mmol/L in survi-vors versus 3.0 6 0.3 mmol/L in non-survivors of severehead injury. However, the number of patients in eachgroup was too small to make these results statisticallysignificant (P ¼ 0.4 for moderate head injury; P ¼ 0.3for severe head injury, Table 1).
To further determine if elevated lactate resulted ina survival advantage, we looked at the probability ofsurvival for patients with various levels of lactate. Di-viding lactates at less than or greater than 2, 3, 4, or5 mmol/L gave no statistically significant differentprobabilities of survival. However, the probability ofsurvival was 100% in patients with admission lactates> 5 who had mild, moderate, or severe head injury.By comparison, patients with a lactate of � 5 had prob-abilities of survival of 99% with mild head injury, 87%with moderate head injury, and 78% with severe headinjury (P ¼ 0.2). This suggests a possible survival ad-vantage of elevated lactate > 5 for moderate or severehead injury.
To examine how admission lactate related to latercognitive function, we looked at the patient’s mentalstatus at discharge. Patients with moderate or severehead injury were included in this analysis, since thesepatients have the most survival difference related tolactate and would stand to potentially benefit themost compared with their admission mental status.The patients were categorized into three groups: nor-mal mental status (GCS 15), abnormal mental status(GCS < 15), or dead. The categorization of normal andabnormal mental status was based on the actual GCSof the patient at the time of discharge. Among patientswith lactate of � 5, 20% were dead, 67% were normal,and 12% were abnormal. In contrast, among patientswith lactates > 5, none were dead, 90% were normal,and 10% were abnormal (P < 0.0001, Fig. 5).
DISCUSSION
Lactate, in addition to being produced by cells under-going anaerobic metabolism, may not always be a meta-bolic ‘‘dead end,’’ and can also be used by cells in thebrain and elsewhere as an efficient energy source. Thebrain is thought to use lactate even in normal aerobicconditions: glucose entering the brain via capillarieshas been found not only to be fed directly to neurons,but through a unique coupling system with glial cells,is used preferentially especially during periods of in-tense activity. These glial cells convert the glucoseinto pyruvate via glycolysis and then to lactate, whichis then transported to adjacent neurons. There the
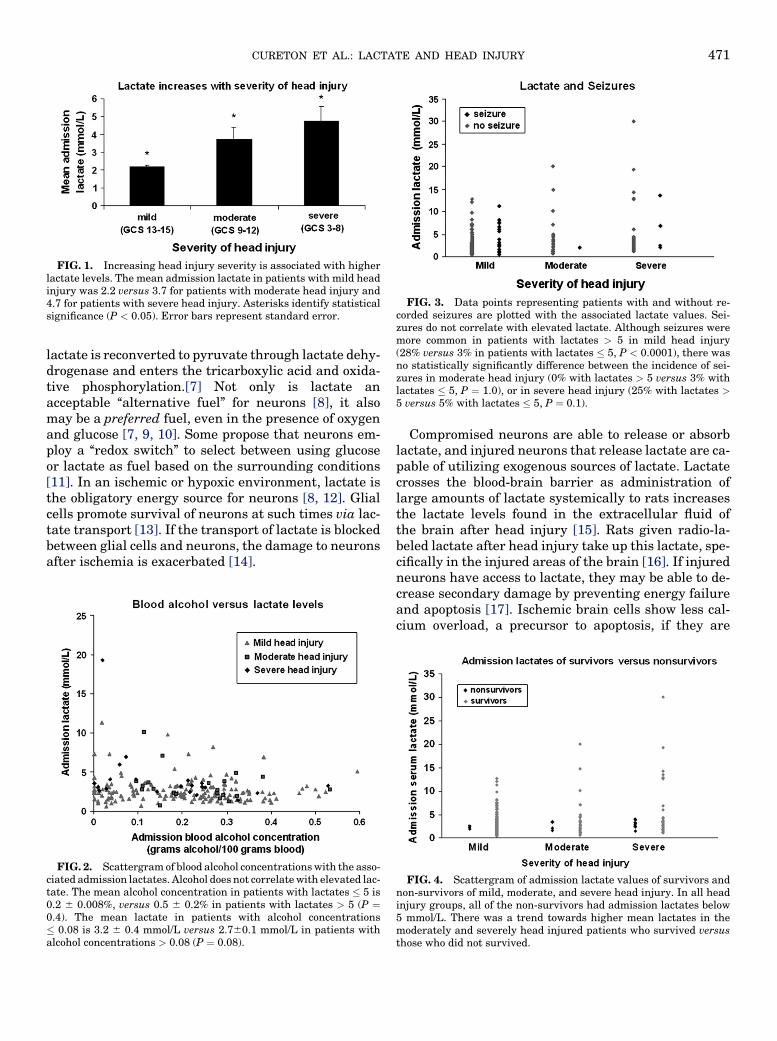
FIG. 3. Data points representing patients with and without re-corded seizures are plotted with the associated lactate values. Sei-zures do not correlate with elevated lactate. Although seizures weremore common in patients with lactates > 5 in mild head injury(28% versus 3% in patients with lactates � 5, P < 0.0001), there wasno statistically significantly difference between the incidence of sei-zures in moderate head injury (0% with lactates > 5 versus 3% withlactates � 5, P ¼ 1.0), or in severe head injury (25% with lactates >5 versus 5% with lactates � 5, P ¼ 0.1).
FIG. 1. Increasing head injury severity is associated with higherlactate levels. The mean admission lactate in patients with mild headinjury was 2.2 versus 3.7 for patients with moderate head injury and4.7 for patients with severe head injury. Asterisks identify statisticalsignificance (P < 0.05). Error bars represent standard error.
CURETON ET AL.: LACTATE AND HEAD INJURY 471
lactate is reconverted to pyruvate through lactate dehy-drogenase and enters the tricarboxylic acid and oxida-tive phosphorylation.[7] Not only is lactate anacceptable ‘‘alternative fuel’’ for neurons [8], it alsomay be a preferred fuel, even in the presence of oxygenand glucose [7, 9, 10]. Some propose that neurons em-ploy a ‘‘redox switch’’ to select between using glucoseor lactate as fuel based on the surrounding conditions[11]. In an ischemic or hypoxic environment, lactate isthe obligatory energy source for neurons [8, 12]. Glialcells promote survival of neurons at such times via lac-tate transport [13]. If the transport of lactate is blockedbetween glial cells and neurons, the damage to neuronsafter ischemia is exacerbated [14].
FIG. 2. Scattergram of blood alcohol concentrations with the asso-ciated admission lactates. Alcohol does not correlate with elevated lac-tate. The mean alcohol concentration in patients with lactates � 5 is0.2 6 0.008%, versus 0.5 6 0.2% in patients with lactates > 5 (P ¼0.4). The mean lactate in patients with alcohol concentrations� 0.08 is 3.2 6 0.4 mmol/L versus 2.760.1 mmol/L in patients withalcohol concentrations > 0.08 (P ¼ 0.08).
Compromised neurons are able to release or absorblactate, and injured neurons that release lactate are ca-pable of utilizing exogenous sources of lactate. Lactatecrosses the blood-brain barrier as administration oflarge amounts of lactate systemically to rats increasesthe lactate levels found in the extracellular fluid ofthe brain after head injury [15]. Rats given radio-la-beled lactate after head injury take up this lactate, spe-cifically in the injured areas of the brain [16]. If injuredneurons have access to lactate, they may be able to de-crease secondary damage by preventing energy failureand apoptosis [17]. Ischemic brain cells show less cal-cium overload, a precursor to apoptosis, if they are
FIG. 4. Scattergram of admission lactate values of survivors andnon-survivors of mild, moderate, and severe head injury. In all headinjury groups, all of the non-survivors had admission lactates below5 mmol/L. There was a trend towards higher mean lactates in themoderately and severely head injured patients who survived versusthose who did not survived.
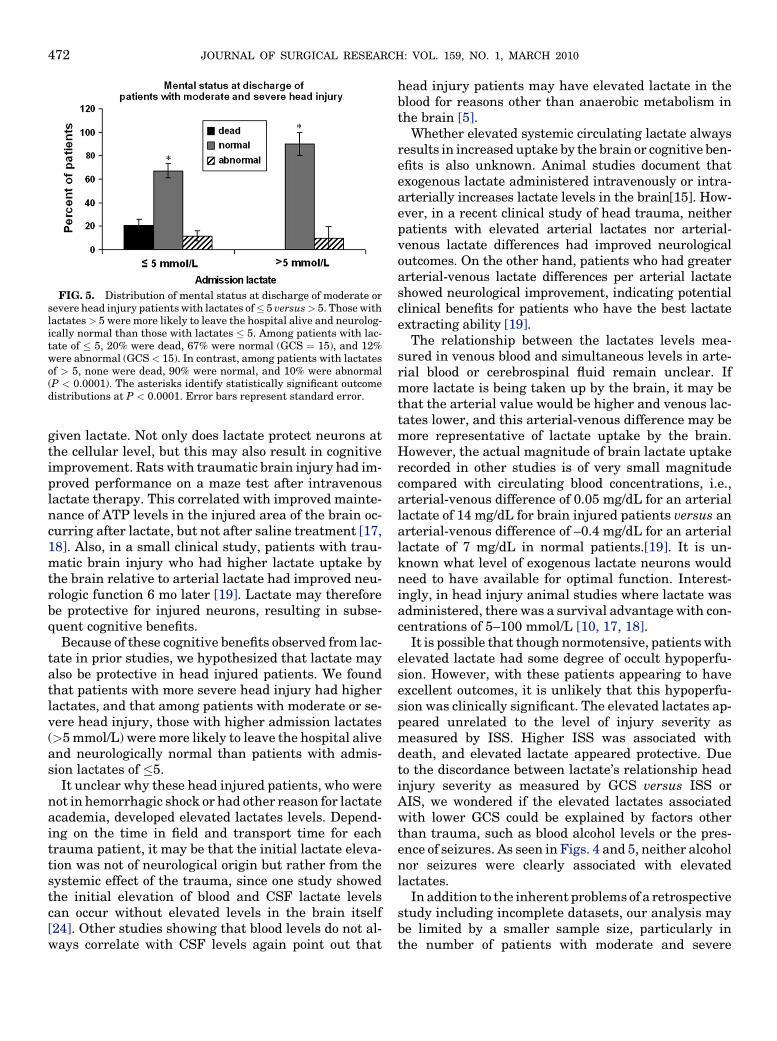
FIG. 5. Distribution of mental status at discharge of moderate orsevere head injury patients with lactates of� 5 versus> 5. Those withlactates> 5 were more likely to leave the hospital alive and neurolog-ically normal than those with lactates � 5. Among patients with lac-tate of � 5, 20% were dead, 67% were normal (GCS ¼ 15), and 12%were abnormal (GCS < 15). In contrast, among patients with lactatesof > 5, none were dead, 90% were normal, and 10% were abnormal(P < 0.0001). The asterisks identify statistically significant outcomedistributions at P < 0.0001. Error bars represent standard error.
JOURNAL OF SURGICAL RESEARCH: VOL. 159, NO. 1, MARCH 2010472
given lactate. Not only does lactate protect neurons atthe cellular level, but this may also result in cognitiveimprovement. Rats with traumatic brain injury had im-proved performance on a maze test after intravenouslactate therapy. This correlated with improved mainte-nance of ATP levels in the injured area of the brain oc-curring after lactate, but not after saline treatment [17,18]. Also, in a small clinical study, patients with trau-matic brain injury who had higher lactate uptake bythe brain relative to arterial lactate had improved neu-rologic function 6 mo later [19]. Lactate may thereforebe protective for injured neurons, resulting in subse-quent cognitive benefits.
Because of these cognitive benefits observed from lac-tate in prior studies, we hypothesized that lactate mayalso be protective in head injured patients. We foundthat patients with more severe head injury had higherlactates, and that among patients with moderate or se-vere head injury, those with higher admission lactates(>5 mmol/L) were more likely to leave the hospital aliveand neurologically normal than patients with admis-sion lactates of �5.
It unclear why these head injured patients, who werenot in hemorrhagic shock or had other reason for lactateacademia, developed elevated lactates levels. Depend-ing on the time in field and transport time for eachtrauma patient, it may be that the initial lactate eleva-tion was not of neurological origin but rather from thesystemic effect of the trauma, since one study showedthe initial elevation of blood and CSF lactate levelscan occur without elevated levels in the brain itself[24]. Other studies showing that blood levels do not al-ways correlate with CSF levels again point out that
head injury patients may have elevated lactate in theblood for reasons other than anaerobic metabolism inthe brain [5].
Whether elevated systemic circulating lactate alwaysresults in increased uptake by the brain or cognitive ben-efits is also unknown. Animal studies document thatexogenous lactate administered intravenously or intra-arterially increases lactate levels in the brain[15]. How-ever, in a recent clinical study of head trauma, neitherpatients with elevated arterial lactates nor arterial-venous lactate differences had improved neurologicaloutcomes. On the other hand, patients who had greaterarterial-venous lactate differences per arterial lactateshowed neurological improvement, indicating potentialclinical benefits for patients who have the best lactateextracting ability [19].
The relationship between the lactates levels mea-sured in venous blood and simultaneous levels in arte-rial blood or cerebrospinal fluid remain unclear. Ifmore lactate is being taken up by the brain, it may bethat the arterial value would be higher and venous lac-tates lower, and this arterial-venous difference may bemore representative of lactate uptake by the brain.However, the actual magnitude of brain lactate uptakerecorded in other studies is of very small magnitudecompared with circulating blood concentrations, i.e.,arterial-venous difference of 0.05 mg/dL for an arteriallactate of 14 mg/dL for brain injured patients versus anarterial-venous difference of –0.4 mg/dL for an arteriallactate of 7 mg/dL in normal patients.[19]. It is un-known what level of exogenous lactate neurons wouldneed to have available for optimal function. Interest-ingly, in head injury animal studies where lactate wasadministered, there was a survival advantage with con-centrations of 5–100 mmol/L [10, 17, 18].
It is possible that though normotensive, patients withelevated lactate had some degree of occult hypoperfu-sion. However, with these patients appearing to haveexcellent outcomes, it is unlikely that this hypoperfu-sion was clinically significant. The elevated lactates ap-peared unrelated to the level of injury severity asmeasured by ISS. Higher ISS was associated withdeath, and elevated lactate appeared protective. Dueto the discordance between lactate’s relationship headinjury severity as measured by GCS versus ISS orAIS, we wondered if the elevated lactates associatedwith lower GCS could be explained by factors otherthan trauma, such as blood alcohol levels or the pres-ence of seizures. As seen in Figs. 4 and 5, neither alcoholnor seizures were clearly associated with elevatedlactates.
In addition to the inherent problems of a retrospectivestudy including incomplete datasets, our analysis maybe limited by a smaller sample size, particularly inthe number of patients with moderate and severe

CURETON ET AL.: LACTATE AND HEAD INJURY 473
head injury. Additionally, there may be a selection biasin that only 70% of all trauma patients during the studyperiod had lactates drawn. However, this selection biasis probably minimal since the ISS and GCS of patientswho had lactates drawn versus those who did not wassimilar (ISS: 9.6 6 0.1 versus 9.1 6 0.2, GCS: 14.1 6
0.03 versus 13.6 6 0.05, respectively). Finally, the pa-tients’ long term neurological status after dischargewas not available, and we based neurologic outcomeson discharge GCS. Because neurological function at dis-charge predicts neurological function at 6 mo [20] and 1y[21], and since patients can show small cognitive im-provements over time [22, 23], it is reasonable to as-sume that the long term neurological function was atleast as good as it was at discharge for most patients.We were not able to assess fine differences in cognitivefunction, and though these are important for functionaloutcome, they are not likely to affect the gross differ-ences in GCS.
Whatever the cause of the elevated lactates, we foundthat lactate is elevated with more severe head injury,and this elevation in lactate is associated with im-proved neurologic outcomes. Although the small num-bers of moderate and severe head injured patientsand patients who died prevent us from concludingthat lactate is clearly correlated with improved out-comes, the data emphasize that in contrast to conven-tional thought, an elevated lactate by itself does notnecessarily mean a poor prognosis in injured patients.In head injured patients, a value of 5 mmol/L ratherthan the traditional 2 mmol/L may provide more clini-cal information, as none of the patients with lactates> 5 mmol/L died. Neurons can both release and use lac-tate, and it is clear that lactate from both exogenoussources and lactate released from ischemic brain tissueenhance the lactate released by neighboring glial cellsto protect injured neurons. Lactate, although a poten-tial diagnostic or prognostic tool in head injury, maytherefore be more useful therapeutically to protect theinjured brain.
REFERENCES
1. Cohen R, Woods H. Clinical and biochemical aspects of lactic ac-idosis. Oxford: Blackwell, 1976.
2. Pal JD, Victorino GP, Twomey P, et al. Admission serum lactatelevels do not predict mortality in the acutely injured patient.J Trauma 2006;60:583.
3. Nedergaard M, Goldman S. Carrier-mediated transport of lacticacid in cultured neurons and astrocytes. Am J Physiol 1993;265:R282.
4. Lin B, Busto R, Globus M, et al. Brain temperature modulationsduring global ischemia fail to influence extracellular lactatelevels in rats. Stroke 1995;26:1634.
5. De Salles A, Muizelaar J, Young H. Hyperglycemia, cerebrospi-nal fluid lactic acidosis, and cerebral blood flow in severely head-injured patients. Neurosurgery 1987;21:45.
6. De Salles A, Kontos H, Becker D, et al. Prognostic significance ofventricular CSF lactic acidosis in severe head injury. J Neuro-surg 1986;65:615.
7. Tsacopoulos M, Magistretti PJ. Metabolic coupling between gliaand neurons. J Neurosci 1996;16:877.
8. Schurr A, West CA, Rigor BM. Lactate-supported synaptic func-tion in the rat hippocampal slice preparation. Science 1988;240:1326.
9. Levasseur JE, Alessandri B, Reinert M, et al. Lactate, not glu-cose, up-regulates mitochondrial oxygen consumption both insham and lateral fluid percussed rat brains. Neurosurgery2006;59:1122.
10. Larrabee MG. Lactate metabolism and its effects on glucose me-tabolism in an excised neural tissue. J Neurochem 1995;64:1734.
11. Cerdan S, Rodrigues TB, Sierra A, et al. The redox switch/redoxcoupling hypothesis. Neurochemistry international 2006;48:523.
12. Schurr A, Rigor BM. Brain anaerobic lactate production: A sui-cide note or a survival kit? Developmental neuroscience 1998;20:348.
13. Schurr A, Payne RS, Miller JJ, et al. Glia are the main source oflactate utilized by neurons for recovery of function posthypoxia.Brain Res 1997;774:221.
14. Schurr A, Payne RS, Miller JJ, et al. Blockade of lactate trans-port exacerbates delayed neuronal damage in a rat model of ce-rebral ischemia. Brain Res 2001;895:268.
15. Chen T, Qian YZ, Di X, et al. Lactate/glucose dynamics after ratfluid percussion brain injury. J Neurotrauma 2000;17:135.
16. Chen T, Qian YZ, Rice A, et al. Brain lactate uptake increases atthe site of impact after traumatic brain injury. Brain Res 2000;861:281.
17. Rice AC, Zsoldos R, Chen T, et al. Lactate administration atten-uates cognitive deficits following traumatic brain injury. BrainRes 2002;928:156.
18. Holloway R, Zhou Z, Harvey HB, et al. Effect of lactate therapyupon cognitive deficits after traumatic brain injury in the rat.Acta Neurochir (Wien) 2007;149:919. discussion 927.
19. Glenn TC, Kelly DF, Boscardin WJ, et al. Energy dysfunction asa predictor of outcome after moderate or severe head injury: In-dices of oxygen, glucose, and lactate metabolism. J Cereb BloodFlow Metab 2003;23:1239.
20. Perel P, Edwards P, Shakur H, et al. Use of the Oxford HandicapScale at hospital discharge to predict Glasgow Outcome Scale at6 months in patients with traumatic brain injury. BMC Med ResMethodol 2008;8:72.
21. Hanks R, Millis S, Ricker J, et al. The predictive validity of a briefinpatient neuropsychological battery for persons with traumaticbrain injury. Arch Phys Med Rehab 2008;89:950.
22. Corral L, Ventura J, Herrero J, et al. Improvement in GOS andGOSE scores 6 and 12 months after severe traumatic brain in-jury. Brain Inj 2007;21:1225.
23. Millis S, Rosenthal M, Novack T, et al. Long-term neuropsycho-logical outcome after traumatic brain injury. J Head TraumaRehab 2001;16:343.
24. Inao S, Marmarou A, Clarke G, et al. Production and clearance oflactate from brain tissue, cerebrospinal fluid, and serum follow-ing experimental brain injury. J Neurosurg 1988;69:736.