Embed Size (px)
Citation preview

CASE REPORT
A frightening bronchial foreign body
P. Pace-Asciak *, E. Chang, J.P. Ludemann
The Division of Otolaryngology, British Columbia’s Children’s Hospital, The Universityof British Columbia, 4480 Oak street, Vancouver, British Columbia, Canada V6H-3V4
Received 3 March 2008; accepted 18 June 2008Available online 5 September 2008
International Journal of Pediatric Otorhinolaryngology Extra (2009) 4, 59—61
www.elsevier.com/locate/ijporl
KEYWORDSBronchial foreign body;Pediatrics;Metal button backing
Summary We report our experience, not previously reported in the literature,with ayoung male Jehovah Witness who aspirated a metal button backing into his rightbronchus intermedius. While in the operating room, a size 5, 30 cm Storz rigidventilating bronchoscope with a 0 degrees rod lens telescope was passed throughthe larynx to visualize the bronchus intermedius. Then, using the ‘‘duckbill’’ telescopicalligator forceps, the sharp edges of the foreign body were grasped and removed. Thepatient recoveredwell andwasdischargedhomehours afterwithout any complications.# 2008 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Bronchial foreign bodies are common in children [1].Sharp bronchial foreign bodies however are rela-tively uncommon, especially in young children [2].Fortunately, multi-pointed bronchial foreign bodiesare rare, since the potential morbidity increaseswhen several sharp points are present. Such foreignbodies increase the need to resort to thoracotomyand bronchotomy for safe removal.
We report our experience, not previouslyreported in the literature, with a young male Jeho-vah Witness who aspirated a metal button backinginto his bronchus intermedius.
2. Case report
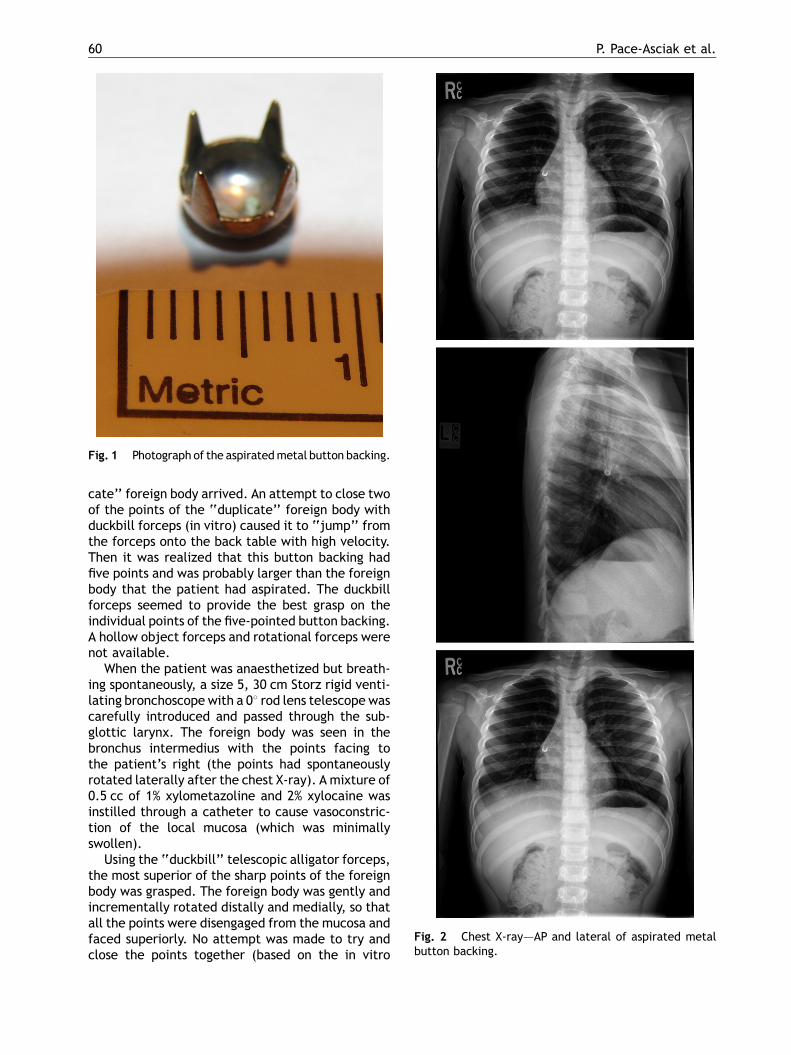
A 5-year-old male Jehovah’s Witness, while playingunsupervised in a sewing room, aspirated a metal
* Corresponding author.E-mail addresses: [email protected] (P. Pace-Asciak),
[email protected] (J.P. Ludemann).
1871-4048/$ — see front matter # 2008 Elsevier Ireland Ltd. All rigdoi:10.1016/j.pedex.2008.06.007
button backing (with four sharp triangular points)(Fig. 1). Concerned by his coughing fit, his motherbrought him to their local Emergency Department. Achest X-ray demonstrated the metal button backingin the bronchus intermedius, with the sharp pointsfacing superiorly (Fig. 2). The patient was trans-ferred to B.C. Children’s Hospital in stable condi-tion, with no respiratory distress. His tetanus shotswere up-to-date. The patient was consented forrigid bronchoscopy with removal of the foreign body.We explained that if attempted removal of theforeign body resulted in bronchial rupture, thatthoracotomy and possibly blood transfusion mightbe required in rapid sequence in order to save thepatient’s life. A thoracic surgeon was consulted andcell-saving and cardiac bypass equipment and an ICUbed were made available.
Upon our request, the patient’s mother asked herfriendtobringusaduplicate foreignbody, sowecoulddetermine, by preoperative in vitro testing, whichforceps and removal technique would work best.
The patient was brought to the operative roomand administered anesthesia by the anesthesiolo-gist. During induction of anesthesia, the ‘‘dupli-
hts reserved.
60 P. Pace-Asciak et al.
Fig. 1 Photograph of the aspiratedmetal button backing.
Fig. 2 Chest X-ray–—AP and lateral of aspirated metalbutton backing.
cate’’ foreign body arrived. An attempt to close twoof the points of the ‘‘duplicate’’ foreign body withduckbill forceps (in vitro) caused it to ‘‘jump’’ fromthe forceps onto the back table with high velocity.Then it was realized that this button backing hadfive points and was probably larger than the foreignbody that the patient had aspirated. The duckbillforceps seemed to provide the best grasp on theindividual points of the five-pointed button backing.A hollow object forceps and rotational forceps werenot available.
When the patient was anaesthetized but breath-ing spontaneously, a size 5, 30 cm Storz rigid venti-lating bronchoscope with a 08 rod lens telescope wascarefully introduced and passed through the sub-glottic larynx. The foreign body was seen in thebronchus intermedius with the points facing tothe patient’s right (the points had spontaneouslyrotated laterally after the chest X-ray). A mixture of0.5 cc of 1% xylometazoline and 2% xylocaine wasinstilled through a catheter to cause vasoconstric-tion of the local mucosa (which was minimallyswollen).
Using the ‘‘duckbill’’ telescopic alligator forceps,the most superior of the sharp points of the foreignbody was grasped. The foreign body was gently andincrementally rotated distally and medially, so thatall the points were disengaged from the mucosa andfaced superiorly. No attempt was made to try andclose the points together (based on the in vitro

A frightening bronchial foreign body 61
experience). Instead, the bronchoscope was advan-ced to ensheath all four points (while one point washeld with the forceps), then the foreign body wasremoved while the bronchoscope remained in thetrachea.
A regular telescope and a flexible suction were re-inserted through the bronchoscope. Traces of bloodwere aspirated from a shallow linear mucosal lacera-tion on the right side of the bronchus intermedius.There was no evidence of bronchial rupture. Thepatient was given decadron (to prevent subglotticedema) and ampicillin (to prevent bronchitis). Post-operatively, the patient did very well and was dis-charged home within a few hours. He had a fullrecovery, and agreed not to place non-food itemsinhismouth.Moreover, hismother agreed tokeephermetallic sewing paraphernalia under lock and key.
3. Discussion
Chevalier Jackson developed the standard techni-ques for rigid bronchoscope removal of pins, basedon his belief, ‘‘advancing points perforate; retreat-ing points do not’’ [5]. In order to spare his patientsthoractomy, Jackson developed pin-bending forcepsand long, thin costophrenic bronchoscopes designedto retrieve foreign bodies lodged within subsege-mental bronchi.
Ideally, a true duplicate of the foreign bodyshould be tested before the patient enters theoperating room. We realized that the ‘‘duplicate’’foreign body that we had received was not an exactduplicate after we discovered, in vitro, that thepoints of a button backing could not be benttogether with our strongest bronchial forceps.
Positive action forceps are useful for most remov-ing pediatric foreign bodies since they offer a widerange of blades to extract various types of objects.The blade types include forward-grasping, rotationand globular object [3]. We used a large, duck-billedforward-grasping forceps since it offered the mostpowerful grip on the pointed metal edges of thebutton backing. A hollow forceps might have beenpreferable if it had been available and if the pointsof the foreign body had still been facing superiorlyand could not be forward-grasped because of muco-sal edema. We were surprised that the object hadspontaneously turned 908 before bronchoscopy. Theminimal mucosa edema, plus topical treatment with
Available online at www
xylometazoline, allowed rotation of the foreignbody back to its initial orientation without signifi-cant trauma. Thus we were able to avoid thoract-omy and possible blood transfusion in this JehovahWitness child.
Since 1998, at B.C. Children’s Hospital, ten othersharp bronchial foreign bodies have been removed,including several pins and thumbtacks and one blow-dart (but no Arabian scarf-pins) [2]. The most diffi-cult bronchial foreign body removal at our hospitalwas a 5 cm glass mercury thermometer fragment inthe distal left main stem bronchus in a 6-year-oldgirl [4]. This foreign body was eventually removedwith the use of an inflated Fogarty catheter withoutcomplications, after multiple failed attempts toremove the foreign body with various forceps.
4. Conclusion
Aspiration of sharp metallic objects remains a chal-lenge to otolaryngologists. Treatment of patientswith foreign bodies of multiple sharp points must beindividualized based on the characteristics of theforeign body, the condition of the surrounding bron-chial mucosa, and the equipment and surgicalexpertise available. In vitro preoperative testing,when possible, is paramount. The need for emer-gent or urgent thoracotomy, bronchotomy andrepair and/or blood transfusion are very real possi-bilities that must be considered before any attemptsat removing a bronchial foreign body with multiplesharp points.
References
[1] C. Jackson, C.L. Jackson, Pins at the periphery of the lung,Archives of Otolaryngology 15 (1932) 860—882.
[2] J.P. Ludemann, K.H. Riding, Choking on pins, needles, and ablowdart: aspiration of sharp, metallic foreign bodies sec-ondary to careless behavior in 7 adolescents, InternationalJournal of Pediatric Otorhinolaryngology 71 (2007) 307—310.
[3] J.P. Ludemann, C.A. Hughes, L.D. Holinger, Management offoreign bodies of the airway, in: T.W. Shields (Ed.), GeneralThoracic Surgery, Fifth edition, Lippincott Williams &Wilkins,Philadelphia, 2000 , pp. 853—862 (Chapter 73).
[4] J.P. Moxham, P.K. Lee, Broken glass mercury thermometer: adifficult airway foreign body, Otolaryngology-Head and NeckSurgery 127 (2002) 339—341.
[5] C. Jackson, Peroral Endoscopy and Laryngeal Surgery, Lar-yngoscope Company, St. Louis, 1914.
.sciencedirect.com