Embed Size (px)
Citation preview
Clinical Genetics 1988: 34: 299-305
A new type of muscular dystrophy in two brothers: analysis by use of DNA probes
suggests autosomal recessive inheritance
PONMANI GOONEWARDENA~, KARL-HENRIK GUSTAVSON’, INGRID GAMSTORP’, NILS-RUNE LUNDSTR6M4 AND ULF PEl%RSSONJ
IeJDepartment of Medical Genetics, BMC, University of Uppsala, Departments of ’Clinical Genetics and ’Pediatrics, University Hospital, Uppsala and ‘Department of Pediatrics, University Hospital,
Lund, Sweden
X-chromosome-specific DNA probes were used to study a new type of muscular dystrophy (MD) presented by two boys in a family in which there was no previous history of neuromuscu- lar disease. Clinical investigations showed evidence of myogenic myopathyia, but its exact nature could not be established. The results of the DNA analysis exclude DMD, BMD and EMD. We suggest a probable autosomal recessive inheritance for the MD seen in this family.
Received 22 February, revised 16 May, accepted for publication 21 July 1988
Key wordr: flanking DNA probes; linkage studies; new type of muscular dystrophy.
The most common of the muscular dys- trophies (MD) is the severe X-linked Duch- enne type. The onset of symptoms usually occurs between 3 and 5 years of age. Pro- gress is rapid so that few can walk after the age of 12 years and most of the patients die before 20 years of age. The Becker type X- linked MD, which has a later onset and slower progression, has very similar clinical features (Emery 1987). The Duchenne (DMD) and Becker (BMD) muscular dys- trophies are probably caused by allelic mu- tations localized at the band Xp21, accord- ing to linkage studies with DNA markers (Brown et al. 1985, Fadda et al. 1985). A third X-linked MD is the very rare Emery- Dreifuss type, characterized by early con- tractures and cardiomyopathy, and with the
gene localized to Xq27-28 (Thomas et al. 1986, Boswinkel et al. 1985).
There is also a childhood MD with a clinical picture like DMD, and autosomal recessive inheritance (Somer et al. 1985).
Genetic risk estimates for the different types of MD are in accordance with their mode of inheritance.
We report here on a family with two young brothers affected with MD. Clinical findings suggested ambiguity between the autosomal and X-linked types of muscular dystrophies.
Case Reports
Case I Boy J. 111-3, born in 1972, first child of

300 G O O N E W A R D E N A E T A L .
healthy unrelated parents. A younger brother (Case 2) has the same disorder as J. No other case of neuromuscular disorder is known in the family. J. was born after a normal pregnancy in a normal delivery. He had a congenital stridor and some feeding difficulties during his first half-year, but was otherwise healthy and developed normally. He could sit unsupported at the age of 8 months and walk at the age of 14 months. When he was 2 years old his parents noted that his gait was waddling, that he did not run and that he appeared to tire easily when walking. When he came to his first specialist examination at the age of 54 years, his con- dition had remained stationary or possibly deteriorated slightly. At the age of 53 years J. could walk but not run; he could climb stairs with difficulty without the use of his hands; when getting up from sitting on the floor he had to climb with his hands on his knees and thighs, but could do so without using any material aid. Muscular weakness and hypotonia were most pronounced in the pelvic girdle and evident also in the shoulder girdle. There was no selective atro- phy of girdle muscles, which is typical in DMD. Peripheral muscles were also slightly weak, but weakness was much milder thcre. Muscles innervated by cranial nerves were entirely spared. There was no muscular hy- pertrophy. Fine motor movements, speech and general development were normal or rather advanced for his age.
Serum creatine activity was slightly in- creased (6.7 pkat/l; upper limit of normal 2.8). Neurophysiological examinations showed normal conduction velocity of peri- pheral nerves and evidence of myogenic myopathy. Histological examination of a muscular biopsy specimen (including .histo- chemistry and electron microscopy) reveal- ed evidence of myogenic myopathy, but its exact nature could not be established.
Cardiac involvement of his muscular dis- order was discovered because a routine elec-
trocardiogram was taken at 5 years of age. He has not had any arrhythmia or other cardiac symptoms. The physical examin- ation of the heart was normal. The electro- cardiogram was abnormal with broad Q- waves and flat T-waves in lead aVL, I and VM. The Q-T interval was within normal limits. At echocardiography a normal-sized left ventricle was normal: based on systolic time intervals and shortening fraction of the left ventricular dimension. The lower part of the interventricular septum seemed to have a slightly reduced movement. Doppler- echocardiography showed no valvular dys- function. The cardiac findings have not changed during the last 4 years.
J. has received physical therapy and been followed. His condition has improved slightly. At the latest examination in 1986 at the age of 14, he could, with some diffi- culty, get up from sitting on the floor with- out using his hands; he could run, though slowly and waddling, and he could climb up on a 25-cm-high chair without using his hands. Compared with earlier investigations his muscle strength had improved some- what, whereas atrophy was easier to see and now particularly involved the thigh muscles, the pectoral muscle and the middle part of the trapezius. Muscles innervated by cranial nerves remained uninvolved. No muscular hypertrophy was seen. According to the pa- rents’ reports, the clinical picture has since remained the same.
Case 2 M., 111-4, born in 1976, J.’s brother. When M. was about 2 years old, his parents noted that he had difficulties in running of exactly the same type as his brother. M. was first examined at 4 years of age. He had atrophy and weakness of pelvic and shoulder girdle muscles without selective atrophy of specific muscle groups. Muscles innervated by cran- ial nerves were uninvolved. No muscular

N E W T Y P E O F M U S C U L A R D Y S T R O P H Y 30 1
hypertrophy was noted. M. showed signs of cardiom yopath y.
Serum creatine kinase activity was slight- ly increased (3.15 pkatll; normal upper limit 2.8). Neurophysiological and histological findings were the same as in his brother (Case 1). M. has received physical therapy. His situation has remained essentially un- changed. His latest examination was in 1986 at the age of 10 years. He could then walk but not run; he could barely walk on his toes but not on his heels; he could neither get up from sitting on the floor nor climb up on a 25-cm-high chair, without helping himself with his hands. A selective atrophy of the pectoral and middle trapezius muscles was now seen, the muscles innervated by the cranial nerves remained uninvolved, and no muscular hypertrophy was seen.
The cardiac involvement was discovered because a routine electrocardiogram was taken at 4 years of age. He has not had any arrhythmia or other cardiac symptoms.
Physical examination revealed a short systolic ejection murmur, best heard over the second left intercostal space. Blood pressure and peripheral pulses were normal. The electrocardiogram showed deep, broad Q-waves and flat to biphasic T-waves in lead aVL and VCS. The Q-T interval was within normal limits. The echocardiogram showed a normal-sized left ventricle with a moderately increased wall thickness of the posterior wall as well as the interventricular septum. In the upper part of the interven- tricular septum there was a short localized bulge causing a slight narrowing of the left ventricular outflow tract. The systolic func- tion of the left ventricle was normal, judged by systolic time intervals and shortening fraction of the left ventricular dimension. Doppler echocardiography showed a nor- mal flow signal in the left ventricular out- flow tract and the ascending aorta. There were no signs of AV-valve regurgitation. The cardiac findings have not changed dur-
ing the last 4 years. Fine motor movements, speech and general development were normal.
M. appears slightly more severely affected than his brother J., Case 1; otherwise, the disease seems identical. The clinical features of the affected brothers did not fit with the X-linked Duchenne, Becker or Emery- Dreifuss MD, nor with any of the slowly progressive autosomal recessive dys- trophies.
J. and M. have two younger sisters (a pair of dizygotic twins) and two younger brothers; all four are healthy and develop- ing normally. The parents and siblings had -normal serum creatine kinase activities.
Material and Methods for DNA Analysis
Chromosome Studies Cytogenetic analyses were performed on cultured blood cells from the two affected boys by standard G-banding techniques.
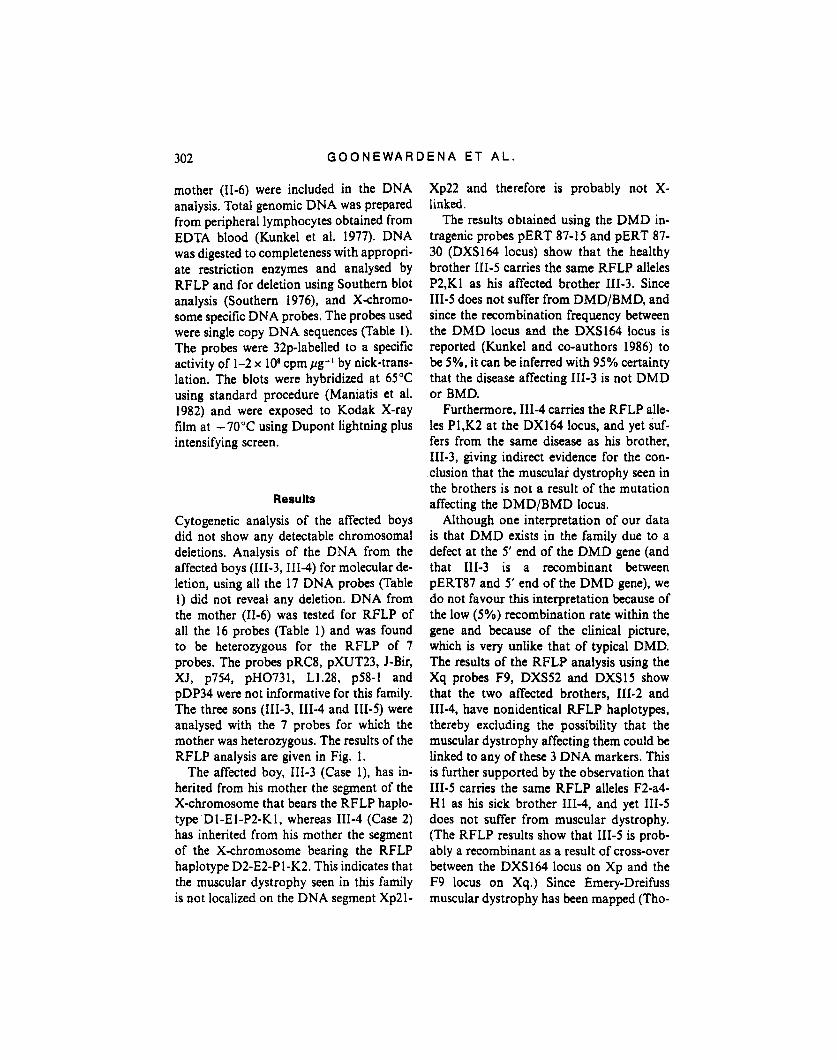
DNA Analysis The pedigree of the family is shown in Fig. 1. The affected boys (111-3, 111-4), one of the healthy brothers (111-5) and their
I 'Djo 30-T-P-P
0 Female c] Mali
Muscular dystrophy
Fig. 1. Pedigree of the family and RFLP data. The symbols used to present the RFLP results are given in Table 1.
302 G O O N E W A R D E N A E T A L .
mother (11-6) were included in the DNA analysis. Total genomic DNA was prepared from peripheral lymphocytes obtained from EDTA blood (Kunkel et al. 1977). DNA was digested to completeness with appropri- ate restriction enzymes and analysed by RFLP and for deletion using Southern blot analysis (Southern 1976), and Xthromo- some specific DNA probes. The probes used were single copy DNA sequences (Table 1). The probes were 32p-labelled to a specific activity of 1-2 x lo8 cpm pg-1 by nick-trans- lation. The blots were hybridized at 65°C using standard procedure (Maniatis et al. 1982) and were exposed to Kodak X-ray film at -70°C using Dupont lightning plus intensifying screen.
Results
Cytogenetic analysis of the affected boys did not show any detectable chromosomal deletions. Analysis of the DNA from the affected boys (111-3,III-4) for molecular de- letion, using all the 17 DNA probes (Table 1) did not reveal any deletion. DNA from the mother (11-6) was tested for RFLP of all the 16 probes (Table 1) and was found to be heterozygous for the RFLP of 7 probes. The probes pRC8, pXUT23, J-Bir, XI, p754, pH0731, L1.28, p58-1 and pDP34 were not informative for this family. The three sons (1113, 111-4 and 111-5) were analysed with the 7 probes for which the mother was heterozygous. The results of the RFLP analysis are given in Fig. 1.
The affected boy, 111-3 (Case l), has in- herited from his mother the segment of the X-chromosome that bears the RFLP haplo- type Dl-El-P2-K1, whereas 111-4 (Case 2) has inherited from his mother the segment of the X-chromosome bearing the RFLP haplotype D2-E2-P 1X2. This indicates that the muscular dystrophy seen in this family is not localized on the DNA segment Xp21-
Xp22 and therefore is probably not X- linked.
The results obtained using the DMD in- tragenic probes PERT 87-15 and PERT 87- 30 (DXS164 locus) show that the healthy brother 111-5 carries the same RFLP alleles P2,Kl as his affected brother 111-3. Since 111-5 does not suffer from DMD/BMD, and since the recombination frequency between the DMD locus and the DXS164 locus is reported (Kunkel and co-authors 1986) to be 5%, it can be inferred with 95% certainty that the disease affecting I113 is not DMD or BMD.
Furthermore, I114 carries the RFLP alle- les P1,K2 at the DX164 locus, and yet suf- fers from the same disease as his brother, 111-3, giving indirect evidence for the con- clusion that the muscular dystrophy seen in the brothers is not a result of the mutation affecting the DMD/BMD locus.
Although one interpretation of our data is that DMD exists in the family due to a defect at the 5’ end of the DMD gene (and that 111-3 is a recombinant between pERT87 and 5’ end of the DMD gene), we do not favour this interpretation because of the low (5%) recombination rate within the gene and because of the clinical picture, which is very unlike that of typical DMD. The results of the RFLP analysis using the Xq probes F9, DXS52 and DXS15 show that the two affected brothers, 111-2 and 111-4, have nonidentical RFLP haplotypes, thereby excluding the possibility that the muscular dystrophy affecting them could be linked to any of these 3 DNA markers. This is further supported by the observation that 111-5 carries the same RFLP alleles F2-a4- HI as his sick brother 111-4, and yet 111-5 does not suffer from muscular dystrophy. (The RFLP results show that 111-5 is prob- ably a recombinant as a result of cross-over between the DXS164 locus on Xp and the F9 locus on Xq.) Since Emery-Dreifuss muscular dystrophy has been mapped (Tho-
NEW T Y P E O F M U S C U L A R D Y S T R O P H Y 303
Table 1
X chromosome specific probes used in this study
Probe RFLP
HGM Symbol Xpter Name Location Reference Enzyme Symbol
DXS9 RC8 P22 Murray et al. (1982) Taq 1
DXS43 P D ~ p22.1-pZ Aldridge et al. (1984) Pvul l D1, D2 DXS28 c 7 p21.3 Bakker et al. (1985) EcoRV El, E2 DXS164 pERT87-15 P21 Kunkel et at. (1985) Taql K1. K2 DXS164 pERT87-30 P21 Kunkel et at. (1985) Bglll P1, P2 DXS206 XJ1.l P21 Ray et al. (1985) Taq 1 DXS206 XJ1.2 P21 Ray et at. (1985) BCll DXS206 XJ2.3 P21 Ray et al. (1985) Taql DXS84 P754 P21 Bakker et al. (1985) PStl OTC pH0731 p21.1 Rozen et al. (1985) Mspl DXS7 L1.28 p11.3 Bakker eta]. (1985) Taq 1
p l l cen . Aldridge et al. (1984) Mspl Page et al. (1964) Taql
DXS14 p-1 DXYS1 pDP34 qi3-qzi . i F9 pCVlll q27 Camerino et al. (1984) Taql F1, F2 DXS52 Stl4-1 q28 Oberle et al. (1985) Taql a, 1-8 DXS15 DX13 q28 Drayna et al. (1984) Bg l l l H1, H2
DXS16 pXUT23 P Z Bakker et al. (1985) Bg l l l
~~ ~
* Probes were not informative for this family: 1 the allele with major frequency of occurrence; 2 the allele with minor frequency of occurrence.
mas et al. 1986) to Xq27-q28, we can ex- clude the possibility that the muscular dys- trophy seen in this family is of the X-linked Emery-Dreifuss type.
Discussion
The clinical features in the two affected brothers in the present family do not fit with the X-linked Duchenne, Becker or Emery- Dreifuss MD, nor with any of the reported slowly progressive autosomal recessive dys- trophies (Emery 1987, Barditser 1982). Be- cause of the ambiguity in clinical diagnosis, it was not possible to assign the MD seen in this family to the autosomal recessive or X-linked type, and hence it was not possible to provide genetic counselling to the family.
The DNA probes did not detect any de- letion in the X-chromosornes of the affected boys. The use of DNA probes as linkage markers, however, excluded with high prob- ability X-linked inheritance, and led to the conclusion that the MD in the present fam-
ily probably is autosomal recessively in- herited: DMD and BMD map to the Xp21 (Brown et al. 1985, Fadda et al. 1985, Bos- winkel et al. 1985), and the absence oflinkage of the MD to DNA probes from this region of the X-chromosome is used to exclude that the disease is either DMD or BMD.
Although analysis using entire cDNA for DMD would have been useful to exclude more reliably the diagnosis of DMD/BMD in this family, our data with pERT87 probes along with the clinical features strongly fa- vour the exclusion of DMD/BMD. Simi- larly, since the Emery-Dreifuss MD has been mapped to the distal Xq (Thomas et al. 1986, Boswinkel et al. 1985), the absence of linkage of the disease to the DNA probes DXS52 and DXS15 from this region of the X-chromosome is taken as suggesting that the disease is not the Emery-Dreifuss MD. We propose that the MD seen in this family could be of a type that has not been delin- eated before, and with a probable autoso- ma1 recessive inheritance.
304 G O O N E W A R D E N A E T A L .
Acknowledgements
The generous gift of DNA probes from Drs G. Brownlee, K. E. Davies, W. A. Fenton, L. M. Kunkel, S. Latt, J. L. Mandel, D. Page, P. L. Pearson, H. F. Willard and R. Worton is gratefully acknowledged.
This study was supported by grants from the Swedish Medical Research Council (to U. P. and K.-H. G.), the Linnka and Josef Carlsson Foundation and the Norrbacka Eugenia Foundation (to. I.G. and K.H.G.). The Bank of Sweden Tercentenary Foun- dation to U.P., the Marcus Borgstrom Foundation to U.P. and P.G. and the Royal Physiographic Society in Lund to P.G.
References
Aldridge, J., M. L. Kunkel, G. Bruns. U. Tantra- vahi, M. Lalande, T. Brewster, E. Moreau, M. Wilson, W. Bromley, T. Roderick & S. A. Latt (1984). A strategy to reveal high-frequency RFLPs along the human X chromosome. Am. J. Hum. Genet. 36, 546-564.
Bakker, E., M. H. Hofker. N. Goor, J. L. Mandel, K. Wrogemann, K. Davies, L. M. Kunkel, H. F. Willard, W. A. Fenton, L. Sandkuyl, D. Ma- joor-Krakauer, A. J. V. Essen, M. G. J. Jakoda, E. S. Sachs, G. J. B. van Ommen & P. L. Pearson (1985). Prenatal diagnosis and camer detection of Duchenne muscular dystrophy with closely linked RFLPs. Lancet i: 655-658.
Baraitser, M. (1982). The Genetics of Neurological Disorders. 2nd Edit. Oxford, Oxford University Press.
Boswinkel, E., A. Walker, S. Hodgson, F. Benham, M. Bobrow, K. Davies, V. Dubow- itz & C. Grenata (1985). Linkage analysis using eight DNA polymorphisms along the length of the X chromosome locates the gene for Emery- Dreifuss muscular dystrophy to distal Xq. Cy- togenet. Cell Genet. 40, 586.
Brown, C. S., N. S. T. Thomas, M. Sarfarazi, K. E. Davies, L. M. Kunkel, P. L. Pearson, H. M. Kingston, D. J. Shaw & P. S. Harper (1985). Genetic linkage relationships of seven DNA probes with Duchenne and Becker muscular dystrophy. Hum. Genet, 71, 62-74.
Camerino, G., K. Gneschik, M. Jaye, H. de le Salle, P. Tolstoshev, J. Lecocq. R. Heilig & J.- L. Mandel(1984). Regional localisation on the
human X chromosome and polymorphism of the coagulation factor IX gene. Proc. Natl. Acad. Sci. USA 81, 498-502.
Drayna, D., K. Davies, D. Hartley, J.-L. Mandel, G. Camerino, R. Williamson & R. White (1984). Genetic mapping of the human X chro- mosome by using RFLPs. Proc. Natl. Acad. Sci. USA 81. 28362839.
Emery, A. E . H. (1987). Duchenne Muscular Dys- trophy. Oxford, Oxford Monographs on Medi- cal Genetics, No. 15.
Fadda, S., M. Mochi, L. Roncuzzi, S. Sangiorgi, D. Sbarra, M. Zatr & G. Romeo (1985). De- finiltive localization of Becker muscular dys- trophy in Xp by linkage to a cluster of DNA polymorphisms (DXS43 and DXS9). H m . Genet. 71, 33-36.
Kingston, H. M., M. Sarfarazi, N. Thomas & P. S. Harper (1984). Localization of the Becker muscular dystrophy gene on the short arm of the X chromosome by linkage to cloned DNA sequences. Hum. Genet. 67, 6-17.
Kunkel. L. M., K. D. Smith, S. H. Boyer, D. S. Borgnonhar. S. S. Wachtel, 0. J. Miller, W. R. Berg, H. W. Jones Jr & J. H. Rany (1977). Analysis of human Y-specific reiterated DNA in chromosome variants. Proc. Natl. Acad. Sci. USA 74, 1245-1249.
Kunkel, L. M., A. P. Monaco, W. Middlesworth, H. D. Ochs & S. A. Latt (1985). Specific clon- ing of DNA fragments absent from the DNA of a male patient with an X chromosome de- letion. Proc. Natl. Acad. Sci. USA 82, 4778-4782.
Kunkel, L. M. and co-authors (1986). Analysis of deletions in DNA from patients with Becker and Duchenne muscular dystrophy. Nature 322, 73-77.
Maniatis, I., E. F. Fritsch & J. Svmbrook (1982). Molecular Cloning - A Laboratory Manual. Cold Spring Harbor Laboratory, Cold Spring Harbor, N.Y.
Monaco, A. P., C. J. Bertelson, C. Colletti- Feener & L. M. Kunkel (1987). Localisation and cloning of Xp21 deletion break points in- volved in muscular dystrophy. Hum. Genet. 75,
Murray, J. M., K.-E. Davies, P. S. Harper, L. Meredith, C. P. Mueller & R. Williams (1982). Linkage relationship of a cloned DNA se- quence on the short arm of the Xchromosome to Duchenne muscular dystrophy. Nature 300, 69-7 1.
Oberle, I., D. Drayana, G. Camerino, R. White & J.-L. Mandel (1985). The telomeric region of the human X chromosome long arm: presence
221-227.

N E W T Y P E O F M U S C U L A R D Y S T R O P H Y 305
of a highly polymorphic DNA marker and analysis of recombination frequency. Proc. Natl. Acad. Sci. USA 82, 2824-2828.
Page, D. C., M. E. Harper, J. Love & D. Botstein (1984). Occurrence of a transposition from the X-chromosome long arm to the Y-chromo- some short arm during human evolution. Na- ture 311, 119-123.
Ray, P., B. Belfall, C. Duff, C. Logan, V. Kean, M. W. Thompson, J. E. Sylvester, J. C. Gorski, R. D. Schimkel & R. G. Worton (1985). Clon- ing of the breakpoint of an X.21 translocation associated with Duchenne muscular dystrophy. Nature 318, 672-675.
Roten, R., J. Fox, A. W. Fenton, A. L. Hor- wich & L. E. Rosenberg (1985). Gene deletion and restriction fragment length polymorphism at the human ornithine transcarbamyIase lo- cus. Nature 313, 8 15-8 17.
Somer, H., A. Voutilainen, S. Knuutila, S. Kaiti-
la, J. Rapola & H. Leinonen (1985). Duchenne- like muscular dystrophy in two sisters with nor- mal karyotypes: evidence for autosomal recess- ive inheritance. Clin. Genet. 28, 151-156.
Southern, E. M. (1976). Detection of specific se- quences among DNA fragments separated by gel electrophoresis. J. Mol. Biol. 98, 503-517.
Thomas, N. S. T., H. Williams, L. J. Elsas, L. C. Hopkins, M. Sarfarazi & P. S. Harper (1986). Localization of the gene for Emery-Dreifuss muscular dystrophy to the distal long arm of the X chromosome. J. Med. Genet. 28, 151-156.
Addres's: Professor Karl-Henrik Gustavson Department of Clinical Genetics University Hospital S- 751 85 Uppsala Sweden













![Autosomal recessive ichthyosis with limb reduction defect ... · including autosomal dominant, autosomal recessive and X-linked inheritance [1,2]. Associated cutaneous and extracutaneous](https://img.pdfslide.net/doc/110x75/5ec8c9b91adfdf12ab3e663c/autosomal-recessive-ichthyosis-with-limb-reduction-defect-including-autosomal.jpg)















