Embed Size (px)
Citation preview

840
CHEST Special Features
Special Features
A practical diagnostic algorithm for approaching the solitary pulmonary nodule (SPN), stratifying clin-
ical risk factors in a standardized manner and blending this information with radiologic clues, would point the physician toward a benign or malignant cause. 1-7 Such an approach would be expected to spare patients with benign causes the morbidity and cost associated with invasive tissue sampling and, at the same time, guide the physician toward recommending invasive tests for the nodules likely to be malignant.
Calculation of Pretest Probability
The clinical and radiologic features described in Part 1 (see page 825) 8 can individually provide clues
as to whether a given SPN is benign or malignant. 9-16 However, assimilating all these factors and assign-ing the “weight” of probability of malignancy to each factor, and coming up with the approximate probabil-ity of malignancy, is an onerous task. Let us take, for example, a 65-year-old patient with a 20-pack-year smoking history who is found to have a 3-cm noncal-cifi ed SPN with lobulated borders in the right upper lobe ( Fig 1 ). The physician is faced with the task of calculating the probability of malignancy in this nodule. If the probability is low, the physician is likely to rec-ommend follow-up of this SPN with serial CT scans. On the other hand, if the probability of malignancy is moderate or high, the patient should be referred for further testing or tissue sampling. How consistent are physicians in stratifying the malignant potential of a SPN? In the instance cited, the range of pretest prob-ability was calculated by showing the same image on the same computer screen to 44 physicians (internists and pulmonologists in academic and private practice
In this second part of a two-part series, we describe an algorithmic approach to the diagnosis of the solitary pulmonary nodule (SPN). An essential aspect of the evaluation of SPN is determining the pretest probability of malignancy, taking into account the signifi cant medical history and social habits of the individual patient, as well as morphologic characteristics of the nodule. Because pretest probability plays an important role in determining the next step in the evaluation, we describe various methods the physician may use to make this determination. Subsequently, we outline a simple yet comprehensive algorithm for diagnosing a SPN, with distinct pathways for the solid and subsolid SPN. CHEST 2013; 143(3):840–846
Abbreviations: GGN 5 ground glass nodule; FDG 5 18 F-2-deoxy-2-fl uoro- d -glucose; SPN 5 solitary pulmonary nodule
A Practical Algorithmic Approach to the Diagnosis and Management of Solitary Pulmonary Nodules Part 2: Pretest Probability and Algorithm
Vishal K. Patel , MBBS ; Sagar K. Naik , MBBS ; David P. Naidich , MD , FCCP ; William D. Travis , MD , FCCP ; Jeremy A. Weingarten , MD , FCCP ; Richard Lazzaro , MD ; David D. Gutterman , MD , FCCP ; Catherine Wentowski , MD ; Horiana B. Grosu , MD ; and Suhail Raoof , MBBS , FCCP
Manuscript received June 12, 2012; revision accepted November 1, 2012. Affi liations: From the New York Methodist Hospital (Drs Patel, Naik, Weingarten, Lazzaro, Wentowski, Grosu, and Raoof), Brooklyn, NY; New York University Langone Medical Center (Dr Naidich), New York, NY; Memorial Sloan-Kettering Cancer Center (Dr Travis), New York, NY; and Medical College of Wisconsin (Dr Gutterman), Milwaukee, WI . Correspondence to: Suhail Raoof, MBBS, FCCP, New York Methodist Hospital, Department of Pulmonary and Critical Care, 506 Sixth St, Brooklyn, NY 11215; e-mail: [email protected]
© 2013 American College of Chest Physicians . Reproduction of this article is prohibited without written permission from the American College of Chest Physicians. See online for more details. DOI: 10.1378/chest.12-1487
Downloaded From: http://journal.publications.chestnet.org/ by a Thomas Jefferson University User on 05/24/2013
journal.publications.chestnet.org CHEST / 143 / 3 / MARCH 2013 841
calculator takes into account the likelihood ratios from a list of clinical and radiologic factors ( Table 1 ) and generates a percentage probability of malignancy. Based on this calculator, the pretest probability of malig nancy in the lesion described in the previous paragraph is 95%. Interestingly, only 66% of the respon-dents in our survey correctly identifi ed the pretest probability of malignancy as � 60%.
Swensen et al 26 employed multivariate regression analysis in an attempt to account for the correlation and interaction among various clinical and radiologic risk factors. They derived their model from a cohort of 419 patients with SPNs detected on chest radio-graph and identifi ed risk factors as delineated in Table 1 . This prediction model is described by the following equation:
x xProbability of malignancy e 1 e
x 6.8272 0.0391 age 0.7917 smoke
1.3388 cancer 0.1274 diameter
1.0407 spiculation 0.7838 location
where e 5 the natural logarithm, age is the patient’s age in years, smoke 5 1 if the patient is a current or former smoker (otherwise, smoke 5 0), diameter is the diameter of the nodule in millimeters, spiculation 5 1 if the edge of the nodule has spicules (otherwise, spiculation 5 0), and location 5 1 if the nodule is located in an upper lobe (otherwise, location 5 0). The model
in a community hospital in New York). The range was found to be 2% to 95% (unpublished data). Although experienced physicians routinely make these judg-ments by gestalt in day-to-day practice, standardized methods have been developed to calculate the prob-ability of the malignancy of a SPN. 17
Bayesian analysis is one such approach. Likelihood ratios for malignancy are assigned to each clinical and radiologic feature by dividing the probability of fi nd-ing a particular feature in patients with malignant nodules by the probability of fi nding the same feature in patients with benign nodules. The odds of malig-nancy can then be calculated by multiplying the like-lihood ratios for each individual clinical and radiologic feature by the prior odds of malignancy. Probability of malignancy can then be calculated easily from the odds. A number of authors developed this approach during the 1970s and 1980s, 18-23 but Gurney et al 24,25 provided the most rigorous test. They derived likeli-hood ratios from a database of 3,858 patients and then validated the model by comparing it with sub-jective clinical assessments. Following a review of the literature current at that time, they calculated likeli-hood ratios for age, smoking history, history of previous malignancy, hemoptysis, size of the SPN, location, edge characteristics, calcifi cation, growth rate, and cavity wall thickness. Needless to say, these calculations were only as accurate as the studies that were used to glean the data. Subsequently, a total of 66 patients with SPNs were evaluated for the probability of malignancy by four radiologists with an average experience of 16 years, yielding an accuracy of 62.5% and an error rate of 37%. When the previously determined Bayes-ian analysis was employed by a separate set of radiol-ogists with far less experience, the accuracy and error rates were much better, at 77.5% and 15.5% respec-tively, with fewer false-negative results.
A convenient and reliable way of performing this assessment is by using a calculator available online at www.chestx-ray.com under the tab “Practice.” This
Figure 1. Pulmonary varix.
Table 1— Calculation of Probability of Malignancy
Source/ReferenceFactors Taken Into Consideration to
Determine the Probability of Malignancy
www.chestx-ray.com 1. Age2. Smoking (ever vs never and pack-y)3. Hemoptysis4. History of prior malignancy5. Nodule diameter6. Location7. Edge characteristics8. Growth rate9. Cavity wall thickness10. Calcifi cation11. Contrast enhancement on CT scan . 15 HU12. PET scan
Swensen et al 26 1. Age2. Smoking history (ever vs never)3. History of previous malignancy . 5 y ago4. Presence of spiculation5. Upper lobe location
Gould et al 27 1. Age2. Smoking history (ever vs never)3. Nodule diameter4. Time since quitting smoking
HU 5 Hounsfi eld unit.
Downloaded From: http://journal.publications.chestnet.org/ by a Thomas Jefferson University User on 05/24/2013

842 Special Features
therefore have to carefully consider the prevalence of malignancy in their practice setting when choosing between the two models. A comparison of these two models in a sample of 151 patients with SPNs 7 to 30 mm in size demonstrated no statistically signifi -cant difference in the receiver-operating characteris-tic curves, suggesting that both models were suffi ciently accurate to guide clinical decision making in patients with SPNs. 17
Regardless of the model used, an assessment must then be made as to whether the calculated pretest probability of malignancy is suffi cient to guide clin-ical decision-making (the “observe vs excise” dilemma presented in the previous example), or whether fur-ther imaging studies are needed to give a clearer pic-ture as to the probability of malignancy. These imaging studies are discussed in the following sections.
Practical Algorithmic Approach to the SPN
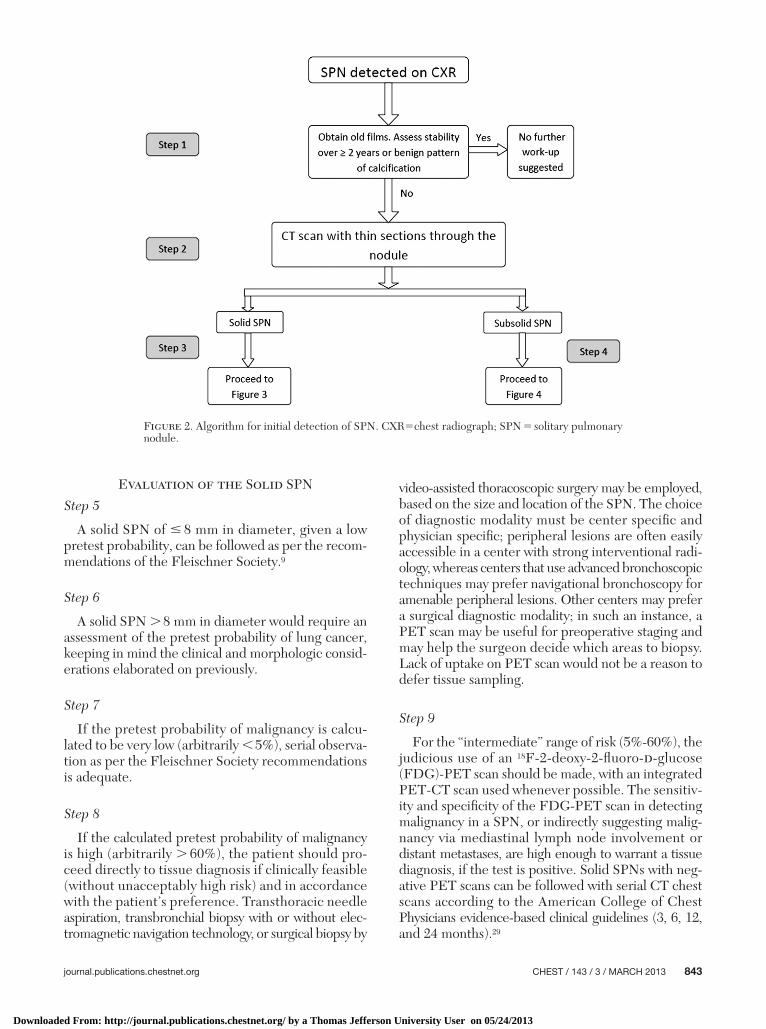
To consolidate the preceding discussion into a log-ical sequence of steps, we propose a practical algo-rithm for approaching a SPN ( Fig 2 ) detected on chest roentgenogram or CT chest scan.
Step 1
The fi rst step in the evaluation of a SPN detected on chest roentgenogram is to review a previous chest roentgenogram or CT scan to assess the growth rate. A volume doubling time � 2 years or a benign pattern of calcifi cation suggests the SPN is benign and requires no further workup. However, one should be cognizant that a malignant subsolid nodule may have a doubling time � 2 years, as mentioned earlier.
Step 2
The second step is to decide whether the SPN is solid or subsolid. A CT chest scan with thin sections through the nodule is strongly recommended for precise char-acterization of the lesions. Consideration should be given to the use of low-dose techniques for this pur-pose as well as for all subsequent follow-up CT exam-inations when needed.
Step 3
Evaluation of solid nodules is discussed in algo-rithm 2. See Figure 3 for details.
Step 4
Subsolid nodules are an exception to the volume doubling rule, and are discussed separately in algo-rithm 3. See Figure 4 for details.
was then validated on separate groups of patients show-ing excellent calibration of the prediction model. 26,28 Additionally, the area under the curve of the pre-diction model was not statistically different from PET scan results. These scan results, when added to the predicted probability calculated by the model, improved the area under the curve by 13.6% (95% CI, 6-21; P 5 .0003). Although this “Mayo Clinic model” yielded an excellent receiver-operating characteristic curve (0.8328 � 0.0226), it had several important lim-itations: (1) Patients who had been given a diagnosis of any cancer, including lung cancer, in the past 5 years were excluded (as discussed previously, a history of malignancy confers a signifi cant risk of a new SPN being malignant, whether metastatic or a new lung primary, and excluding these patients from the calcu-lation would therefore potentially underestimate the probability of malignancy); (2) the model was devel-oped in a cohort of patients with lung nodules who were originally managed more than 20 years previ-ously at a single tertiary care center in the midwestern United States, thereby limiting the model’s general-izability; and (3) the prevalence of malignancy was relatively low (23%), and in 12% of patients a fi nal diag-nosis was not determined.
To address these limitations, Gould et al 27 studied a geographically diverse sample of 375 veterans with a high prevalence of malignant SPNs (54%). This study again identified independent predictors of malignancy by using multivariate regression analysis ( Table 1 ). Interestingly, upper lobe location was not found to be an independent predictor of malignancy. Notable limitations to this “VA model” are as follows: (1) SPN , 7 mm in diameter were excluded from the study; (2) the study sample consisted primarily of older white men, thereby limiting the generalizability of the model to female patients and patients of other ethnicities; (3) information about nodule morphology on CT chest scans was not taken into account (instead of defi nitive nodule morphology characteristics, radi-ologists were asked to rate each SPN on a fi ve-point scale between “defi nitely benign” and “defi nitely malig-nant” based on chest roentgenogram morphology; this characterization was taken as a surrogate marker for spiculation. A “defi nitely malignant” nodule mor-phology on chest roentgenogram did not attain sta-tistical signifi cance as an independent predictor for malignancy, possibly because of the limited resolution of the chest roentgenogram images. A spiculated nod-ule should, thus, be considered “high probability” for malignancy even if the pretest probability calculated by the “VA model” suggests otherwise); and (4) the model may not be well calibrated for use in popula-tions in which the prevalence of malignancy is much lower or higher than in this study. Physicians would
Downloaded From: http://journal.publications.chestnet.org/ by a Thomas Jefferson University User on 05/24/2013
journal.publications.chestnet.org CHEST / 143 / 3 / MARCH 2013 843
video-assisted thoracoscopic surgery may be employed, based on the size and location of the SPN. The choice of diagnostic modality must be center specifi c and physician specifi c; peripheral lesions are often easily accessible in a center with strong interventional radi-ology, whereas centers that use advanced bronchoscopic techniques may prefer navigational bronchos copy for amenable peripheral lesions. Other centers may prefer a surgical diagnostic modality; in such an instance, a PET scan may be useful for preoperative staging and may help the surgeon decide which areas to biopsy. Lack of uptake on PET scan would not be a reason to defer tissue sampling.
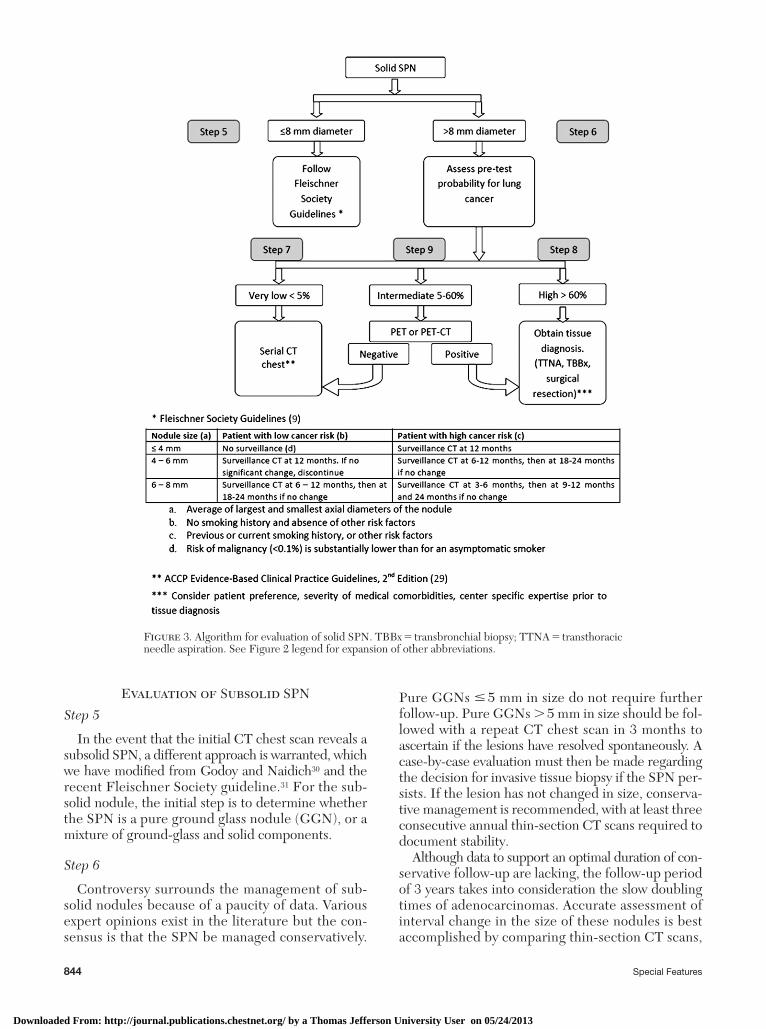
Step 9
For the “intermediate” range of risk (5%-60%), the judicious use of an 18 F-2-deoxy-2-fl uoro- d -glucose (FDG)-PET scan should be made, with an integrated PET-CT scan used whenever possible. The sensitiv-ity and specifi city of the FDG-PET scan in detecting malignancy in a SPN, or indirectly suggesting malig-nancy via mediastinal lymph node involvement or distant metastases, are high enough to warrant a tissue diagnosis, if the test is positive. Solid SPNs with neg-ative PET scans can be followed with serial CT chest scans according to the American College of Chest Physicians evidence-based clinical guidelines (3, 6, 12, and 24 months). 29
Evaluation of the Solid SPN
Step 5
A solid SPN of � 8 mm in diameter, given a low pretest probability, can be followed as per the recom-mendations of the Fleischner Society. 9
Step 6
A solid SPN . 8 mm in diameter would require an assessment of the pretest probability of lung cancer, keeping in mind the clinical and morphologic consid-erations elaborated on previously.
Step 7
If the pretest probability of malignancy is calcu-lated to be very low (arbitrarily , 5%), serial observa-tion as per the Fleischner Society recommendations is adequate.
Step 8
If the calculated pretest probability of malignancy is high (arbitrarily . 60%), the patient should pro-ceed directly to tissue diagnosis if clinically feasible (without unacceptably high risk) and in accordance with the patient’s preference. Transthoracic needle aspiration, transbronchial biopsy with or without elec-tromagnetic navigation technology, or surgical biopsy by
Figure 2. Algorithm for initial detection of SPN. CXR 5 chest radiograph; SPN 5 solitary pulmonary nodule.
Downloaded From: http://journal.publications.chestnet.org/ by a Thomas Jefferson University User on 05/24/2013
844 Special Features
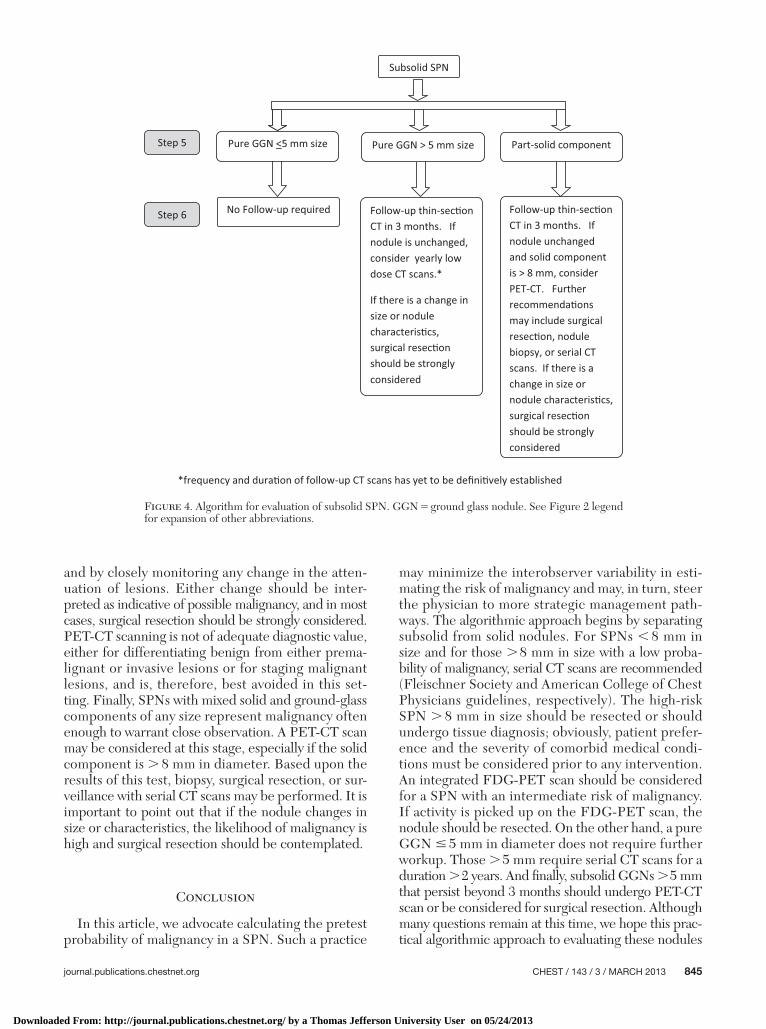
Pure GGNs � 5 mm in size do not require further follow-up. Pure GGNs . 5 mm in size should be fol-lowed with a repeat CT chest scan in 3 months to ascertain if the lesions have resolved spontaneously. A case-by-case evaluation must then be made regarding the decision for invasive tissue biopsy if the SPN per-sists. If the lesion has not changed in size, conserva-tive management is recommended, with at least three consecutive annual thin-section CT scans required to document stability.
Although data to support an optimal duration of con-servative follow-up are lacking, the follow-up period of 3 years takes into consideration the slow doubling times of adenocarcinomas. Accurate assessment of inter val change in the size of these nodules is best accomplished by comparing thin-section CT scans,
Evaluation of Subsolid SPN
Step 5
In the event that the initial CT chest scan reveals a subsolid SPN, a different approach is warranted, which we have modifi ed from Godoy and Naidich 30 and the recent Fleischner Society guideline. 31 For the sub-solid nodule, the initial step is to determine whether the SPN is a pure ground glass nodule (GGN), or a mixture of ground-glass and solid components.
Step 6
Controversy surrounds the management of sub-solid nodules because of a paucity of data. Various expert opin ions exist in the literature but the con-sensus is that the SPN be managed conservatively.
Figure 3. Algorithm for evaluation of solid SPN. TBBx 5 transbronchial biopsy; TTNA 5 transthoracic needle aspiration. See Figure 2 legend for expansion of other abbreviations.
Downloaded From: http://journal.publications.chestnet.org/ by a Thomas Jefferson University User on 05/24/2013
journal.publications.chestnet.org CHEST / 143 / 3 / MARCH 2013 845
may minimize the interobserver variability in esti-mating the risk of malignancy and may, in turn, steer the physician to more strategic management path-ways. The algorithmic approach begins by separating subsolid from solid nodules. For SPNs , 8 mm in size and for those . 8 mm in size with a low proba-bility of malignancy, serial CT scans are recommended (Fleischner Society and American College of Chest Physicians guidelines, respectively). The high-risk SPN . 8 mm in size should be resected or should undergo tissue diagnosis; obviously, patient prefer-ence and the sever ity of comorbid medical condi-tions must be considered prior to any intervention. An integrated FDG-PET scan should be considered for a SPN with an intermediate risk of malignancy. If activ ity is picked up on the FDG-PET scan, the nodule should be resected. On the other hand, a pure GGN � 5 mm in diameter does not require further workup. Those . 5 mm require serial CT scans for a duration . 2 years. And fi nally, subsolid GGNs . 5 mm that persist beyond 3 months should undergo PET-CT scan or be considered for surgical resection. Although many questions remain at this time, we hope this prac-tical algorithmic approach to evaluating these nodules
and by closely monitoring any change in the atten-uation of lesions. Either change should be inter-preted as indicative of possible malignancy, and in most cases, surgical resection should be strongly considered. PET-CT scanning is not of adequate diagnostic value, either for differentiating benign from either prema-lignant or invasive lesions or for staging malignant lesions, and is, therefore, best avoided in this set-ting. Finally, SPNs with mixed solid and ground-glass components of any size represent malignancy often enough to warrant close observation. A PET-CT scan may be considered at this stage, especially if the solid component is . 8 mm in diameter. Based upon the results of this test, biopsy, surgical resection, or sur-veillance with serial CT scans may be performed. It is important to point out that if the nodule changes in size or characteristics, the likelihood of malignancy is high and surgical resection should be contemplated.
Conclusion
In this article, we advocate calculating the pretest probability of malignancy in a SPN. Such a practice
Figure 4. Algorithm for evaluation of subsolid SPN. GGN 5 ground glass nodule. See Figure 2 legend for expansion of other abbreviations.
Downloaded From: http://journal.publications.chestnet.org/ by a Thomas Jefferson University User on 05/24/2013

846 Special Features
can help physicians navigate toward a defi nitive diagno-sis in a timely, reliable, and resource-conscious fashion.
Acknowledgments Financial/nonfi nancial disclosures: The authors have reported to CHEST that no potential confl icts of interest exist with any companies/organizations whose products or services may be dis-cussed in this article . Other contributions: The authors thanks Patrice Balistreri, adminstrative assistant, for her invaluable clerical assistance.
References 1 . Nathan MH , Collins VP , Adams RA . Differentiation of benign
and malignant pulmonary nodules by growth rate . Radiology . 1962 ; 79 : 221 - 232 .
2 . Garland LH , Coulson W , Wollin E . The rate of growth and apparent duration of untreated primary bronchial carcinoma . Cancer . 1963 ; 16 : 694 - 707 .
3 . Steele JD , Buell P . Asymptomatic solitary pulmonary nod-ules. Host survival, tumor size, and growth rate . J Thorac Cardiovasc Surg . 1973 ; 65 ( 1 ): 140 - 151 .
4 . Weiss W . Tumor doubling time and survival of men with bronchogenic carcinoma . Chest . 1974 ; 65 ( 1 ): 3 - 8 .
5 . Friberg S , Mattson S . On the growth rates of human malig-nant tumors: implications for medical decision making . J Surg Oncol . 1997 ; 65 ( 4 ): 284 - 297 .
6 . Bach PB , Silvestri GA , Hanger M . Screening for lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition). Chest. 2007 ;132(suppl 3):69S-77S.
7 . Soubani AO . The evaluation and management of the solitary pulmonary nodule . Postgrad Med J . 2008 ; 84 ( 995 ): 459 - 466 .
8 . Patel VK , Naik SK , Naidich DP , et al . A practical algorithm approach to the diagnosis and management of solitary pul-monary nodules: part 1: radiologic characteristics and imaging modalities . Chest . 2013 ; 143 ( 3 ): 825 - 839 .
9 . MacMahon H , Austin JH , Gamsu G , et al ; Fleischner Society . Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society . Radiology . 2005 ; 237 ( 2 ): 395 - 400 .
10 . Swensen SJ , Viggiano RW , Midthun DE , et al . Lung nodule enhancement at CT: multicenter study . Radiology . 2000 ; 214 ( 1 ): 73 - 80 .
11 . Furuya K , Murayama S , Soeda H , et al . New classifi cation of small pulmonary nodules by margin characteristics on high-resolution CT . Acta Radiol . 1999 ; 40 ( 5 ): 496 - 504 .
12 . Seemann MD , Seemann O , Luboldt W , et al . Differentiation of malignant from benign solitary pulmonary lesions using chest radiography, spiral CT and HRCT . Lung Cancer . 2000 ; 29 ( 2 ): 105 - 124 .
13 . Zwirewich CV , Vedal S , Miller RR , Müller NL . Solitary pul-monary nodule: high-resolution CT and radiologic-pathologic correlation . Radiology . 1991 ; 179 ( 2 ): 469 - 476 .
14 . Siegelman SS , Zerhouni EA , Leo FP , Khouri NF , Stitik FP . CT of the solitary pulmonary nodule . AJR Am J Roentgenol . 1980 ; 135 ( 1 ): 1 - 13 .
15 . Huston J III , Muhm JR . Solitary pulmonary opacities: plain tomography . Radiology . 1987 ; 163 ( 2 ): 481 - 485 .
16 . Ikehara M , Saito H , Kondo T , et al . Comparison of thin-section CT and pathological fi ndings in small solid-density type pul-monary adenocarcinoma: prognostic factors from CT fi ndings . Eur J Radiol . 2012 ; 81 ( 1 ): 189 - 194 .
17 . Schultz EM , Sanders GD , Trotter PR , et al . Validation of two models to estimate the probability of malignancy in patients with solitary pulmonary nodules . Thorax . 2008 ; 63 ( 4 ): 335 - 341 .
18 . Templeton AW , Jansen C , Lehr JL , Hufft R . Solitary pul-monary lesions. Computer-aided differential diagnosis and evaluation of mathematical methods . Radiology . 1967 ; 89 ( 4 ): 605 - 613 .
19 . Wojtowicz J , Grala B , Pietraszkiewicz , L . A trial of differential diagnosis of solitary pulmonary foci on the basis of Bayes’s equation with the use of electronic digital cornputers . Pol Rev Radiol NucI Med . 1970 ; 34 : 684 - 691 .
20 . Alperovitch A , Lellouch J . Value of computer diagnosis of a single thoracic X-ray circular opacity . Biomedicine . 1974 ; 20 ( 1 ): 54 - 60 .
21 . Rotte KH , Meiske W . Results of computer-aided diagnosis of peripheral bronchial carcinoma . Radiology . 1977 ; 125 ( 3 ): 583 - 586 .
22 . Edwards FH , Schaefer PS , Callahan S , Graeber GM , Albus RA . Bayesian statistical theory in the preoperative diagnosis of pulmonary lesions . Chest . 1987 ; 92 ( 5 ): 888 - 891 .
23 . Edwards FH , Schaefer PS , Cohen AJ , et al . Use of artifi cial intelligence for the preoperative diagnosis of pulmonary lesions . Ann Thorac Surg . 1989 ; 48 ( 4 ): 556 - 559 .
24 . Gurney JW . Determining the likelihood of malignancy in soli-tary pulmonary nodules with Bayesian analysis. Part I. Theory . Radiology . 1993 ; 186 ( 2 ): 405 - 413 .
25 . Gurney JW , Lyddon DM , McKay JA . Determining the like-lihood of malignancy in solitary pulmonary nodules with Bayesian analysis. Part II. Application . Radiology . 1993 ; 186 ( 2 ): 415 - 422 .
26 . Swensen SJ , Silverstein MD , Ilstrup DM , Schleck CD , Edell ES . The probability of malignancy in solitary pulmonary nod-ules. Application to small radiologically indeterminate nod-ules . Arch Intern Med . 1997 ; 157 ( 8 ): 849 - 855 .
27 . Gould MK , Ananth L , Barnett PG ; Veterans Affairs SNAP Cooperative Study Group . A clinical model to estimate the pretest probability of lung cancer in patients with solitary pul-monary nodules . Chest . 2007 ; 131 ( 2 ): 383 - 388 .
28 . Herder GJ , van Tinteren H , Golding RP , et al . Clinical pre-diction model to characterize pulmonary nodules: validation and added value of 18F-fl uorodeoxyglucose positron emission tomography . Chest . 2005 ; 128 ( 4 ): 2490 - 2496 .
29 . Gould MK , Fletcher J , Iannettoni MD , et al ; American College of Chest Physicians . Evaluation of patients with pul-monary nodules: when is it lung cancer? ACCP evidence-based clinical practice guidelines (2nd edition). Chest. 2007 ;132(suppl 3):108S-130S.
30 . Godoy MC , Naidich DP . Subsolid pulmonary nodules and the spectrum of peripheral adenocarcinomas of the lung: rec-ommended interim guidelines for assessment and management . Radiology . 2009 ; 253 ( 3 ): 606 - 622 .
31 . Naidich DP , Bankier AA , Macmahon H , et al . Recommenda-tions for the management of subsolid pulmonary nodules detected at CT: a statement from the Fleischner Society . Radiology. 2013 ; 266 ( 1 ): 304 - 317 .
Downloaded From: http://journal.publications.chestnet.org/ by a Thomas Jefferson University User on 05/24/2013





























