Embed Size (px)
Citation preview
RARE OR 0BSCUR.E CASES 517
From the evidence of the skiagrains and the splash, there can be no doubt that there was a collection of air and fluid inside the skull in the right frontal region. The air must have entered the cranial cavity through a fracture involving the right frontal sinus. One cannot be certain whether the air was internal or external to the dura mater. On the one hand, the sharp definition of the shadow a t the middle line in the antero-posterior negative suggests a limitation hy the falx cerebri ; on the othcr. the tough dura mater was not likely to be torn by the fracture involving so little displacement of the bone. In my opinion the air was probably extradural. It is possible that frequent shaking of his head to elicit the splash hastened absorption of the air.
By the cnd of March his head symptoms had much improved, and he returned to work on April 3, but had to leave work again on April 19 with left lobar pneumonia, which disabled him until June 10.
A REMARKABLE EXAMPLE OF THE TENDENCY TO RECURRENT PEPTIC ULCERATION
FOLLOWING GASTRO-ENTEROSTOMY FOR DUODENAL ULCER. BP TIIE LATE WALTER THOMPSON,
AND ill. J. STEWART. H O N . SURGEON TO THE LLEDS GENERAL INIIRMAHY ;
PROFERbOR OF PAlHOLOCY IEr TlfE UNIVLRSITY OF LECDS,
SIX JOHN BLAND-SUTTON, in his Hunterian Oration on jejunal ulcer (1916), speaks in his inimitable way of ‘new ulcers for old’, but even he could hardly have imagined a case in which a surgical magician would be able repeatedly to effect such an exchange over a number of years in one and the same individual. The case which we now report is possibly unique in this respect ; a t least wc have failed to find a parallel, or even a comparable example, in the literature.
The patient was subjected, during a period of sixteen years, to no fewer than five separate and distinct operations upon his stomach-four gastro- cnterostomies and a partial gastrectomy-the last of which he survived for two years more, finally dying of chronic interstitial nephritis and arteriosclerosis. The tendency throughout was for the original ulcer to heal and a fresh ulcer to develop in relation to the new stoma, and even a t autopsy two new ulcers wcrc present in the small remaining portion of the stomach. All the operations mere carried out in the Leeds General Infirmary, as was the post-mortem.
FIRST HOSPITAL PEnIon.--The patient, when he first came under observa- tion in 1005, was a single man of 36, born of healthy stock and a solderer by trade. He was a hard-working man and a moderate beer-drinker, and he lived in healthy and comfortable surroundings. He had suffered For many years from dyspeptic symptoms, with long intervals of freedom, but was otherwise healthy. A duodenal ulcer was found a t operation, and posterior gastro-enterostomy performed (Fig. 377, 1).
SECOND HOSPITAL PEnIoD.-Nine years later, on .June 1, 1914, he was again admitted to hospital. He stated that he had remained well for fire years
518 THE BRITISH JOURNAL OF SURGERY
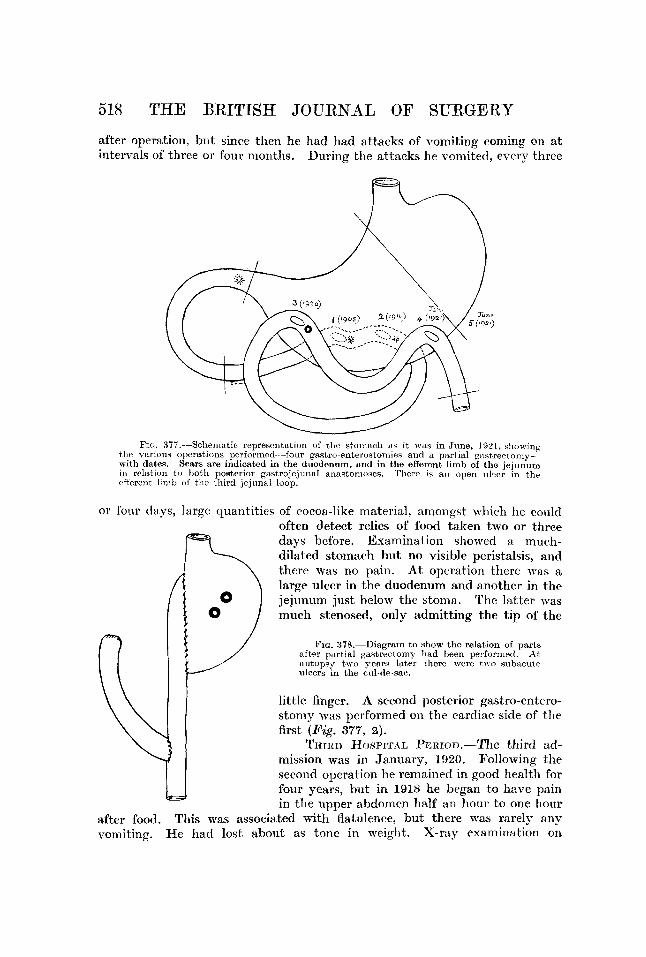
after operation, but since then he had had att,acks of vomiting conling on at intervals of three or four months. Dining the attacks he vomited, every three
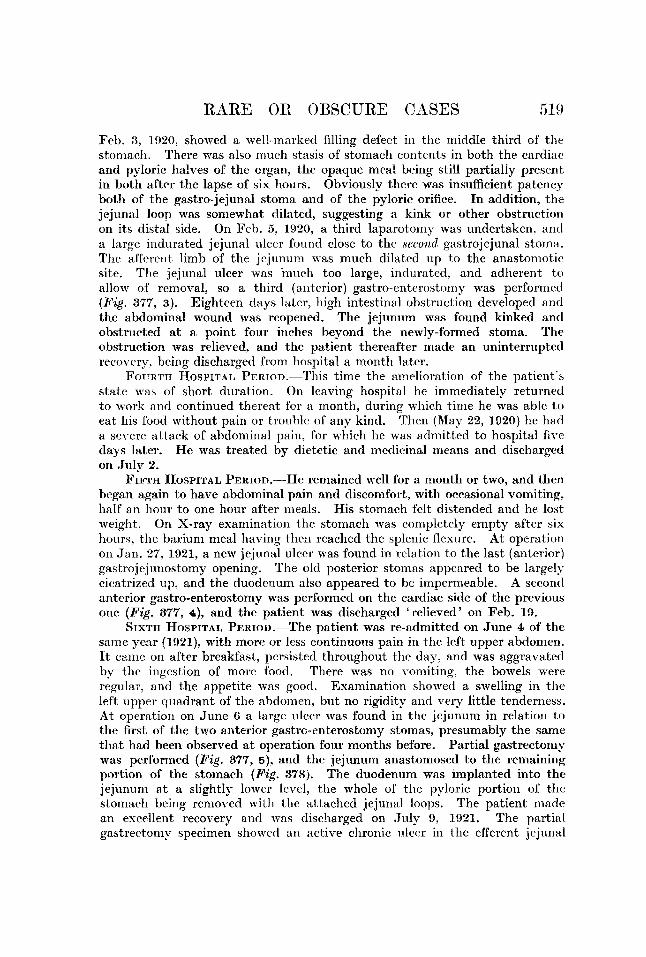
FIG. 37i.--Scliernatic representation of the st,oinacIi a s i t was in June, 1921, showiiig the vnrioiia operations perforrnccl-~-foiir ~~stro-onterostoinins and a partial gastrertonly- with dates. Sears are indicntcd in the diiodeniim, and in the efferent. limb of the jejunum in rolation to both posterior gastrojrjiinal nnantomoscs. There is a n open ulwr i n the rffcrent l i i i i h o f the third jejnnal loop.
or four days, large quantitics of cocoa-like material, amongst whichh he coLlld often detect relics of food taken two or three days before. Examination showed a much- dilated stomach hut no visible peristalsis, and therc was no pain. At operation therc was a large ulcer in the duodenum and anqther in the jejunum just below the stoma. Thc latter was much stenosed, only admitting the tip of the
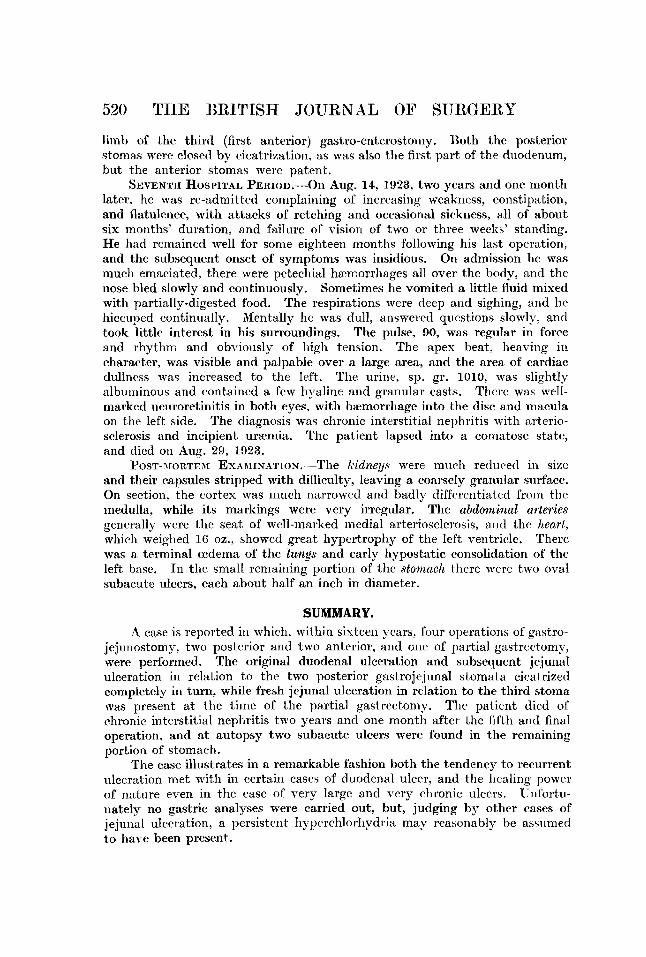
FIG. 378.-Diagraln to qhow the relation of parts nftor part it11 gaytrectorny had been perforrned A t aiitopsy tMo ymrs later there were tiro subnciite ulcers in the rid-clr-sac,.
little Singcr. A second posterior gastro-entero- stomy W ~ S performed on the cardiac side of the first (Pig. 377, 9).
TirrItn $€OSPITAL Psnrori.--Tlie third ad- mission was in January, 1'320. Following the second operation he remained in good health for Sour years, but in 191s he began to have pain in the upper abdomcn half an hour to one hour
Tllis was associated with flatulence, but there was rarely any X-ray exanhat ion on
after food. vorniting. He 2lad lost about as tone in weight.
RARE OR OBSCURE CASES 519
Feb. 3, 1920, showed a well-marked filling defect in tlie middle third of the stomach. There was also imuch stasis of stomach contents in both the cardiac and pploric halves of the organ, the opaque meal being still partially present in both after the lapse of six hours. Obviously there was insufficient patency both of the gastro-jejunal stoma and of the pploric orifice. In addition, the jejunal loop was somewhat dilated, suggesting a kink or other obstruction on its distal side. On Feh. 3 , 1920, a third laparotomy was undertaken, and a large indurated jcjunal ulcer found close to the second gastrojejunal stoma. The afferent limb of the jejunum was much dilated u p to thc anastomotir site. The jejunal ulcer was inuch too large, indurated, and adherent to allow of removal, so a third (anterior) gastro-enterostomy was performed (Fig. 377, 3). Eighteen days later, high intestinal obstruction developed and the abdominal wound was reopened. The jejunum was found kinked and obstructed a t a point four inches heyond the newly-formed stoma. The obstruction was relieved, and the patient thereafter made an uninterrupted recovery, being discharged from hospital a month later.
Fouit.rII HOSPITAL P e ~ ~ o ~ . - - T h i s time the amelioration of the patient's state was of short duration. On leaving hospital he immediately returned to work and continued thereat for a month, during which time he was able to eat his food without pain or trouble of any kind. Then (Map 22, 1020) he had a seT-ere attack of ahdominal pain, for which he was admitted to hospital five days later. He was treated by dietetic and medicinal means and discharged on Jiily 2.
FIFTH HOSPITAL YmtIon.--He remained well for a month or two, and then began again to have abdominal pain and discomfort, with occasional vomiting. half an hour to one hour after meals. His stomach felt distended and he lost weight. On X-ray examination the stomach was completely empty after six hours, the barium meal having then reached the splenic flexure. At operation on .Jan. 27, 1921, a new jejunal ulcer was found in relation to the last (anterior) gastrojejunostomy opening. The old posterior stomas appeared to be largely cicatrized up, and the duodenum also appeared to be impermeable. A secoiitl anterior gastro-enterostomp was performed on the cardiac side of the previous one (Fig. 377. 4), and the patient was discharged 'relieved' on Feb. 19.
SIXTIT HOSPITAL Pmron.-The patient was re-admitted on Jiine 4 of the same year (1921), with more or less continuous pain in the left upper abdomen. It came on after breakfast, persisted throughout the day, and was aggravated by the ingestion of morc food. There was no vomiting, the bowels were regular, and the appetite was good. Examination showed a swelling in tlie left upper quadrant of the abdomen, but no rigidity and very little tcnderness. A t operation on June 6 a large irlcer was found in the jejunum in relation to the first of the two anterior gastrc-enterostomy stomas, presumably the same that had been observed at operation four months before. Partial gastrectoniv was performed (Fig. 377, 5), and the jejunum anastomosed to the remaining portion of the stomach (Fig. 378). Tine duodenum was implanted into the jejunum a t a slightly lower level, the whole of the pyloric portion of the stomach being rcmoved witli the attached jejunal loops. The patient madr an excellent recovery and was discharged on July 9, 1921. The partial gastrectonip specimen showed an active chronic illeer in the efferent jejunal
520 THE BRITISH JOURNAL OF SURGERY
limb of the third (first anterior) gastro-enterostoniy. Both the posterior stomas were closed by cicatrization, as was also the first part of the duodenum, but the anterior stomas were patent.
SEVENTII HOSPITAL PERIOD.--O~~ Aug. 14, 1923, two years and one month later, he was re-admitted complaining of increasing weakness, constipation, and flatulence, with attacks of retching and occasional sickness, all of about six months' duration, and failure of vision of two or three weeks' standing. He had remained well for some eighteen months following his last operation. and the subsequcnt onset of symptoms was insidious. On admission he was much emaciated, there were petechial hzcmorrhagrs all over thc body, and the nose bled slowly and continuously. Sometimes he vomited a little fluid mixed with partially-digested food. The respirations were deep and sighing, and he hiccuped continually. Mentally he was dull, answered questions slowly, and took little intercst in his surroundings. The pulse, 90, was regular in force and rhythm and obviously of high tcn4on. The apex beat, heaving in charactcr, was visible and palpable over a large area, and the area of cardiac dullncss was increased to the left. The urine, sp. gr. 1010, was slightly albuminous and contained a few hpaline and granular casts. There was well- marked neuroretinitis in both eyes, with hxmorrhagc into the disc and macula on the left side. The diagnosis was chronic interstitial nephritis with arterio- sclerosis and incipient uramia. The patient lapsed into a coniatose state, and died on h u g . 29, 1033.
POST-JIORTEM EXARIINATION.-The lt-idnegs were much reduced in sizc and their capsules stripped with difliculty, leaving a coarscly granular surface. On section, the cortex was much narrowed and badly differentiated from the medulla, while its markings were very irregular. The abdominal arteries gencrally were the seat of well-marked niedial arteriosclrrosis, and the heart, which weighed 16 oz. , showed great hypertrophy of the lcft ventriclc. There was a terminal mdcma of the lungs and early hypostatic consolidation of the lcft bast,. In the small remaining portion of the stomach therc were two oval subacutc ulcers, each about half an inch in diameter.
SUMMARY. A rase is reported in which, within sixteen ycar5, four operations of' gastro-
jejnnostomp, two posterior and two anterior, and one of partial gastrectomy, were performed. The original duodenal ulceration and subsequent jejunal ulceration in relation to the two posterior gastrojejunal stomata cicatrized completely in turn, while fresh jejunal ulceration in relation to the third stoma was present a t the timc of the partial gastrectomy. Thr patient died of chronic interstitial nephritis two years and one month after the fifth and final operation, and at autopsy two subacute ulcers were found in the remaining portion of stomach.
The case illustrates in a remarkable fashion both the tendency to recurrent ulceration met with in certain cases of duodenal ulcer, and the liealing powcr of nature even in the case of very large and very chronic ulcers. Tlnfortu- natelp no gastric analyses were carried out, but, judging by other cases of jejunal ulceration, a persistent hypcrchlorh~dria map reawnably be assumed to have been present.