Embed Size (px)
Citation preview
Arch. Geronwl. Geriatr., 5 (1986) 33-39 33 Elsevier
AGG 00134
A survey of elderly patients admitted to hospital for social reasons
Christina R. Victor and Norman J. Vetter Research Team for The Care of the Elderly. University of Wales College of Medicine.
St. Davids Hospital, Cardiff, UK
(Received 9 September 1985; revised version received 18 November 1985, accepted 20 November 1985)
Summary
A random 4~ sample of the over 65's discharged from general hospitals throughout Wales was selected from Welsh Office HAA returns. Included within the group were 101 patients admitted for social reasons (ICD code V600 to V6055). Such patients were predominantly very elderly, female and extremely disabled. Typically such patients lived with, and were being cared for, by relatives. The majority of admissions were booked or planned to provide relief to these carets. Geographical variations in the use of such care was demonstrated. Use of domiciliary medical services by these patients was extremely high in contrast to their use of domiciliary social services. Mortality and re-admission rates at 3 months and 12 months after the initial discharge were very high and hospital treatment had little influence upon patients" disability. However, the short mean length of stay suggests that such patients do not "block beds'.
elderly: social admission
Introduction
It is recognised that some elderly people are admitted to hospital for social rather than medical reasons. Four per cent of patients in a recent survey of the elderly after discharge from hospital had been admitted to hospital primarily for social reasons. Very little is known about the characteristics of such patients; how long they stay in hospital; how they fare after discharge and what use they make of community services. This paper describes the characteristics of a sample of such patients derived from a wider observational study of the elderly after discharge from hospital (Victor, 1984). Patients admitted for social reasons are compared with a random sample of all elderly discharged from hospital.
Correspondence should be addressed to: Dr. Christina R. Victor, Department of Community Health, The University of Nottingham, Queen's Medical Centre, Clifton Blvd., Nottingham, NG7 2UH. UK.
0167-4943/86/$03.50 ~ 1986 Elsevier Science Publishers B.V. (Biomedical Division)
34
Method
A random 4~ sample of the over 65's discharged from general hospitals throughout Wales was selected from Welsh Office HAA returns. The survey was undertaken in seven of the eight Health Authorities current in Wales at the time of the research. Powys was excluded as it lacked a large district general hospital. This sample of 2 711 subjects included 101 patients who were, according to the diagnostic information given on the HAA form, admitted for social reasons (ICD code V600 to V6055). The sample was collected monthly for one complete calendar year, 1981, to exclude the influence of seasonal variations in admission patterns. Only patients with a minimum of 48 hours in hospital were eligible for inclusion in the study.
Three and 12 months after discharge from hospital, patients were sent a postal questionnaire which requested information about patients' use of services, re-admis- sion to hospital, as well as standard demographic details. Disability was recorded using a well validated index described by Townsend (1979) in which subjects are asked to describe if they require assistance to perform nine tasks considered a normal part of independent life in the community such as shopping or heavy housework. Subjects scored 0 if they could perform the task, 1 if they need help and 2 if unable to perform the task at all. Thus the score ranges from 0 to 18. A score of 0 was classified as not disabled; 1-5 as mildly disabled; 6-11 as moderately disabled; 12-14 as severely disabled, and 14 and over as very severely disabled. Problems with incontinence, sight and hearing were also recorded. Subjects were also asked to provide morbidity data for the month prior to admission.
R ~ d ~
Response
Of the 101 patients discharged with a mean diagnosis of social admission recorded on the HAA form a questionnaire was returned, at 3 months, by 64 (63~) subjects, compared with 71~ of the total sample. One patient refused to participate. At 12 months a questionnaire was returned by 55 (86~) social admission patients and by 77~$ of the total sample.
Patient characteristics
Demographic characteristics The majority of social admission patients, 72~, were females; 15~ lived alone
whilst the majority rived with their children or other relatives (61~$); 23~$ lived with their spouse. No patients were resident in institutions prior to admission. The majority of subjects admitted for social reasons, 505, were aged over 80 years and only 9~$ were aged between 65-69 years. This contrasts with a random sample of over 65's admitted to hospital where 31~ lived alone, 40~$ lived with a spouse and 29~ lived with their children or other relatives. Twenty four per cent of the entire
35
sample were aged between 65-69 years and a further 25% were aged over 80 years. There were no social class differences in the composition of the two groups.
The fraction of patients admitted for social reasons increased with age from 3% of admissions for those aged 65-69 to 12% of admissions of those aged 85 years and over.
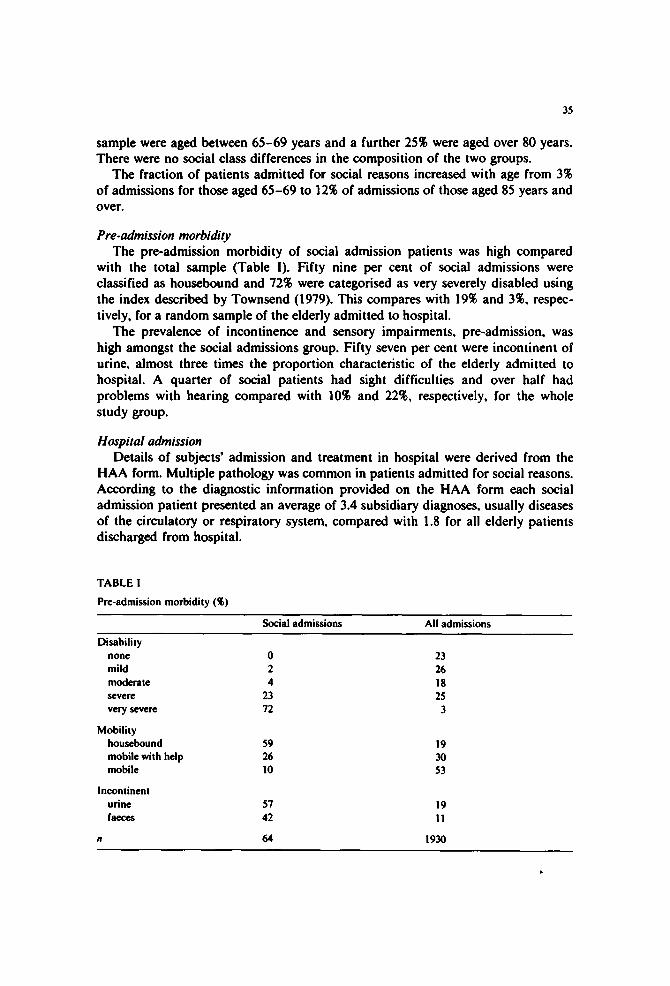
Pre-admission morbidity The pre-admission morbidity of social admission patients was high compared
with the total sample (Table I). Fifty nine per cent of social admissions were classified as housebound and 72% were categorised as very severely disabled using the index described by Townsend (1979). This compares with 19% and 3%, respec- tively, for a random sample of the elderly admitted to hospital.
The prevalence of incontinence and sensory impairments, pre-admission, was high amongst the social admissions group. Fifty seven per cent were incontinent of urine, almost three times the proportion characteristic of the elderly admitted to hospital. A quarter of social patients had sight difficulties and over half had problems with hearing compared with 10% and 22%, respectively, for the whole study group.
Hospital admission Details of subjects' admission and treatment in hospital were derived from the
HAA form. Multiple pathology was common in patients admitted for social reasons. According to the diagnostic information provided on the HAA form each social admission patient presented an average of 3.4 subsidiary diagnoses, usually diseases of the circulatory or respiratory system, compared with 1.8 for all elderly patients discharged from hospital.
TABLE I
Pre-admission morbidity {%)
Social admissions All admissions
Disability none mild moderate s e v e r e
very severe
Mobility housebound mobile with help mobile
Incontinent urine faeces
0 23 2 26 4 18
23 25 72 3
59 19 26 30 10 53
57 19 42 11
64 1930
36
The majority of patients admitted for social reasons were booked or planned admission, 6070, compared with 147o for the whole group. Six per cent of social patients compared with 2470 of all admissions were admitted from the waiting list. Inter-hospital transfers accounted for 870 of all admissions and 570 of social admissions. The remaining admissions, 2970 of the social group and 5570 of the total sample, were classified as emergencies. All patients admitted to hospital for social reasons were treated in the medical specialty of geriatrics.
Substantial inter-county variations in the fraction of patients admitted for social reasons were observed. Overall 470 of admissions were so classified. Below average admission rates were generally characteristic of the more rural northern and western counties of Wales such as CIwyd, Dyfed and West Glamorgan. In contrast above average admission rates were typical of the three counties of industrial South Wales; Mid Glamorgan, South Glamorgan and Gwent. South Glamorgan had the highest admission rate with 1270 of all admissions of elderly being defined as for social reasons.
Process measures
Length of stay in hospital it is sometimes suggested that patients admitted for 'social' reasons block beds
for extensive periods of time. In this study mean length of stay in hospital was 8 days for social admission patients and 12 days for the sample as a whole. Eighty per cent of social admission subjects were in hospital for 2 weeks or less, compared with 5770 of the whole group.
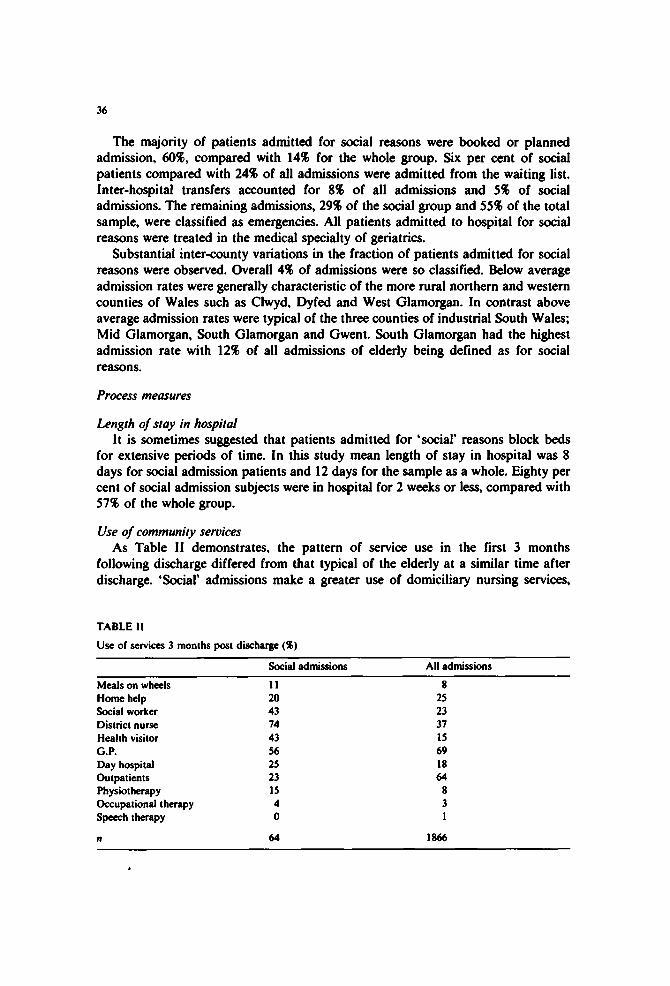
Use of community services As Table II demonstrates, the pattern of service use in the first 3 months
following discharge differed from that typical of the elderly at a similar time after discharge. 'Social' admissions make a greater use of domiciliary nursing services,
TABLE I1
Use of services 3 months post discharge (~)
Social admissions All admissions
Meals on wheels 11 8
Home help 20 25 Social worker 43 23 District nurse 74 37 Health visitor 43 15 G.P. 56 69 Day hospital 25 18 Outpatients 23 64 Physiotherapy 15 8 Occupational therapy 4 3 Speech therapy 0 1
n 64 1866
37
physiotherapy and social work services whilst making less use of the home help and outpatient services. Social admission patients were also less likely to see their GP. At 12 months, use of services presented a similar pattern.
Re-admissions Within 3 months of discharge 26% of social admission survivors had been
re-admitted to hospital compared with 17% for the whole sample. Annual re-admis- sion rates were 43% and 27%, respectively. The majority of re-admissions, 78%, were again for social reasons. Overall 545 of re-admissions were for further treatment to the patients initial condition. Multiple re-admissions were typical of social admis- sion patients. Fifty per cent of this group were re-admitted more than once during the 12 months follow-up compared with 9% for the whole sample.
Outcome
Outcome after discharge was recorded by two indices, mortality and disability. Data on mortality were obtained from the National Health Service Central Registry.
Mortafity Mortality at 3 months was high for the social admission group, 36q[ compared
with 12~ for the whole sample. Annual mortality rates were 43~ and 20~, respectively. The major causes of death for the social admissions group were circulatory disease, respiratory disease and cancer; they were very similar to those for the rest of the sample.
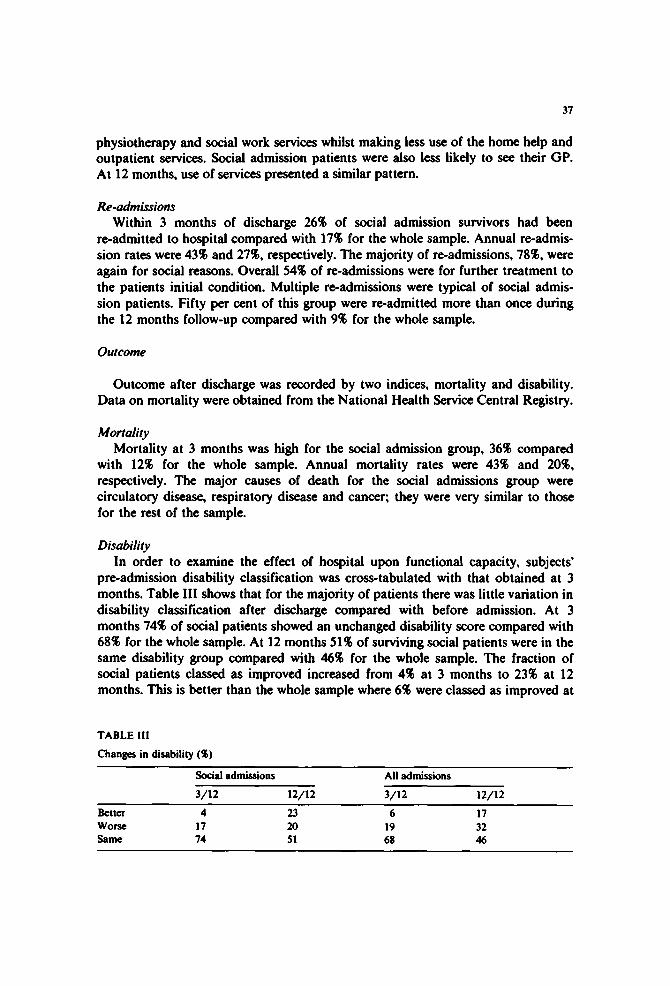
Disability In order to examine the effect of hospital upon functional capacity, subjects'
pre-admission disability classification was cross-tabulated with that obtained at 3 months. Table Ill shows that for the majority of patients there was little variation in disability classification after discharge compared with before admission. At 3 months 74~$ of social patients showed an unchanged disability score compared with 68~ for the whole sample. At 12 months 51q[ of surviving social patients were in the same disability group compared with 46~ for the whole sample. The fraction of social patients classed as improved increased from 4~ at 3 months to 23~ at 12 months. This is better than the whole sample where 6% were classed as improved at
TABLE I!1 Changes in disability ($)
Social admissions All admissions
3/12 12/12 3/12 12/12 Better 4 23 6 ! 7 Worse 17 20 19 32 Same 74 51 68 46
38
3 months and 17~ at 12 months. The fraction of social patients deteriorating after discharge remained constant whilst for the group as a whole disability became worse with increased length of time after discharge.
Conclusions and Discussion
Patients admitted to hospital primarily for social reasons are a very elderly and extremely disabled sub-group of the elderly population admitted to hospital. They are much more likely to be living with their children than other admissions of the same age. Typically they demonstrate many physical problems as well as social problems.
The majority of these patients, 60~, lived with their children. The main reason for admission was to provide relief to those caring for them. This is reflected in the high proportion of planned admissions. However, for one third of cases the admission was classed as an emergency, suggesting a crisis in the care arrangements of the elderly person. Geographical variations in the availability of such respite care were clearly demonstrated. Thirty per cent of the social admissions studied were drawn from the County of South Glamorgan whilst the counties of West Glamor° gan, Clwyd and Dyfed admitted very few patients for social reasons.
The admission of elderly people to hospital for social reasons is often said to be associated with the blocking of beds. However, in this survey mean length of stay, at 8 days, was short, providing no evidence to support the bed blocking hypothesis.
Re-admission rates were extremely high compared with other types of admission for the same age groups. However, for three quarters of social patients re-admission was again for social reasons, suggesting a routine pattern of respite care.
The use of domiciliary medical services such as the nurse and health visitor was extremely high. Social service use was generally, with the exception of social worker visits, typical of that of the whole sample. However, the provision of home helps was lower to the social admissions group, possibly because the majority were being assisted by 'informal' carers such as sons or daughters and thus not considered to need the services of a home help.
Outcome 3 months after discharge, as measured by mortality, was poor compared with the main study group. One third of social admissions were dead compared with 20~ for the group overall. Disability showed little variation at 3 months compared with pre-admission for both groups. However, the social admissions did not seem to deteriorate as much after discharge as did the whole group, possibly because of the higher mortality and the greater degree of disability amongst social patients before admission. However, more social patients than the whole group improved over the study period, indicating that hospital care did result in some improvement in their functional capacity.
Such admissions are of undoubted value to those caring for the elderly (Jones et al., 1983), and the provision of respite care is a service often requested by carers. However, we have demonstrated that within Wales there are substantial inequalities in the availability of such care given in hospital. We have shown that such patients

39
have only a short length of stay. Thus, providing such a service does not greatly restrict the other activities of the geriatric departments and should be seen as important aspect of the care of the elderly in the community.
Admission seemed to have only a marginal effect upon the morbidity of the elderly themselves. Consequently it could be that some alternative service other than hospital admission could provide the essentially nursing care that such patients seem to need. Establishing a national service to provide respite care in an environ- ment, such as nursing homes, may be a more appropriate service. Our data indicated that social admission patients were less likely to receive a home help. We speculated that it might be because the elderly person was living with a relative and thus were not eligible for the service. However, expanding the provision of home helps to those caring for the elderly may well prevent the admission of the elderly to hospital for primarily social reasons. Alternatively, establishing a home care aid service which would be a basic nursing and domestic care service, might be a more appropriate method of providing help to carets, and prevent admission of the elderly to hospital for social reasons.
References
Jones, D., Victor, C.R. and Vetter, N.J. (1983): A survey of those caring for the elderly. J. Roy. Coll. Gen. Practit., 33, 707-710.
Townsend, P. (1979): Poverty in the United Kingdom. Penguin, Harmonds Worth. Victor C.R. (1984): A survey of the elderly after discharge from hospital in Wales, Unpublished Ph.D.
Thesis, Welsh National School of Medicine.