Embed Size (px)
Citation preview
A Systematic Review of Interventions to ImproveOutcomes for Elders Discharged from theEmergency Department
Susan N. Hastings, MD, Mitchell T. Heflin, MD
AbstractObjectives: To evaluate the evidence for interventionsdesigned to improve outcomes for elders discharged fromthe emergency department (ED). Methods: The study wasa systematic review of English-language articles indexedin MEDLINE and CINAHL (1966–2005) with 1) key words‘‘geriatric,’’ ‘‘older adults,’’ or ‘‘seniors,’’ or 2) MedicalSubject Heading (MeSH) terms ‘‘Geriatrics’’ or ‘‘HealthServices for the Aged’’ AND key word ‘‘emergency,’’ or3) MeSH terms ‘‘Emergencies,’’ ‘‘Emergency Service, Hos-pital,’’ or ‘‘Emergency Treatment.’’ Bibliographies of theretrieved articles were reviewed for additional references,and the authors consulted with content experts to identifyrelevant unpublished work. Patients of interest were com-munity-dwelling elder patients discharged home from theED. Data were abstracted from selected articles by theauthors. Studies with interventions limited to patients witha single presentation or diagnosis (falls, delirium, etc.) ordelivered only to patients who would have otherwise beenhospitalized were not included. Results: Of 669 citations, 27studies (reported in 33 articles) met study criteria and were
reviewed; six randomized controlled trials (RCTs), twononrandomized clinical trials, and 19 observational studiesor program descriptions. Three of four RCTs designed tomeasure functional outcomes showed a reduction in func-tional decline in the intervention group. The trials thatresulted in functional benefits enrolled high-risk patientsand included geriatric nursing assessment and home-basedservices as part of the intervention. Results of trials todecrease health service utilization rates following an EDvisit were mixed. Conclusions: A significant number ofprograms to improve outcomes for elders discharged fromthe ED exist, but few have been systematically examined.Development of interventions to improve the care of elderpatients following ED visits requires further research intosystem and patient-centered factors that impact health caredelivery in this situation. Key words: older adults; patientdischarge; emergency department; geriatric assessment;outcomes; elderly. ACADEMIC EMERGENCY MEDICINE2005; 12:978–986.
Older adults account for an increasing number of visitsto emergency departments (EDs) each year.1 Personsaged 75 years and over now have the highest ED visitrate of any segment of the population.1 Elder adultsseek care in the ED for a variety of reasons, includingfalls, cardiopulmonary and abdominal symptoms, de-hydration, and urinary tract infections.2 Although asignificant number of these patients require hospitaladmission, most are treated and discharged.2
A growing body of evidence suggests that olderpatients discharged home from the ED suffer a high
rate of adverse health outcomes, including func-tional decline, reduced health-related quality of life,and death.3–5 A 2002 systematic review estimatedthe average mortality rate to be 10% in the threemonths following an index ED visit.2 Increased ratesof health service utilization following an ED visit havealso been documented.2,5,6 As many as 24% of eldersdischarged home from the ED return for a repeat visitwithin three months, and up to 25% are hospitalized.2
One study reported rates of return ED visits at sixmonths to be as high as 44%.6
A greater understanding of the risks associatedwith an ED visit has led to a number of programsand initiatives to improve outcomes in this high-riskgroup. The Research Agenda Setting Process (RASP), aproject convened by the American Geriatrics Societywith support from the John A. Hartford Foundation,recently established a research agenda for geriatricemergency medicine. Research on whether alterationsin the process of ED care may improve the outcomesof older ED patients was judged to be of the highestpriority.7
Favorable outcomes depend not only on thecare received in the ED, but also on the successfultransition of care from the ED to the patient’s home.
From Geriatrics Research, Education and Clinical Center, VA Med-ical Center (SNH, MTH), Durham, NC; the Division of Geriatrics,Department of Medicine, Duke University Medical Center (SNH,MTH), Durham, NC; the Center for Health Services Research, VAMedical Center (MTH), Durham, NC; and the Center for the Studyof Aging and Human Development, Duke University MedicalCenter (MTH), Durham, NC.Received July 29, 2004; revisions received November 22, 2004,March 7, 2005, and April 19, 2005; accepted May 12, 2005.Address for correspondence and reprints: Susan N. Hastings, MD,Durham VAMC, GRECC 182, 508 Fulton Street, Durham, NC 27705.Fax: 919-286-6823; e-mail: [email protected]; or Mitchell T.Heflin, MD, 2511 Blue Zone, Duke South, Duke University MedicalCenter, Durham, NC 27710. E-mail: [email protected]:10.1197/j.aem.2005.05.032
978 Hastings and Heflin d OUTCOMES OF DISCHARGED ELDERS

High-quality transitional care for frail seniors requiresthe coordination of necessary resources, education ofthe patient and family, and communication amonghealth professionals.8 Many studies have examineda variety of interventions targeting the transition fromthe ED to home. To better understand the evidencesupporting interventions aimed at improving out-comes for elders discharged from the ED, we system-atically reviewed the current literature.
METHODS
Study Design. This was a systematic review ofarticles indexed in MEDLINE and CINAHL.
Study Identification. A MEDLINE search (from 1966to January 2005) was conducted for English-languagearticles containing 1) key words ‘‘geriatric,’’ ‘‘olderadults,’’ or ‘‘seniors,’’ or 2) Medical Subject Heading(MeSH) terms ‘‘Geriatrics’’ or ‘‘Health Services forthe Aged’’ AND key word ‘‘emergency,’’ or 3) MeSHterms ‘‘Emergencies,’’ ‘‘Emergency Service, Hospital,’’or ‘‘Emergency Treatment.’’ The same search wasperformed in CINAHL using subject headings ‘‘emer-gency service’’ AND ‘‘aged.’’ Bibliographies of theretrieved articles were reviewed for additional refer-ences. In addition, the authors consulted with contentexperts to identify unpublished work relevant to thegoals of this review.
Study Selection. Each author independently re-viewed titles and abstracts to select citations thatseemed to describe an intervention to improve out-comes for senior adults discharged from the ED. Allarticles identified by one or both screeners as poten-tially relevant were obtained for further review. Weexcluded articles that described and/or tested anintervention 1) limited to patients with a single presen-tation or diagnosis (e.g., falls, delirium) or 2) deliveredonly to patients who would have otherwise beenhospitalized. An assessment of methodologic validityof the relevant clinical trials was performed based onthe following parameters: 1) random assignment ofsubjects to treatment groups, 2) analysis of patients inthe group to which they were randomized (intention-to-treat [ITT] analysis), 3) blinding of outcome asses-sors to group allocation, and 4) completeness offollow-up. In cases where this information was notincluded in the published article, attempts were madeto contact the study authors for clarification. Ameta-analysis was judged infeasible due to obviousheterogeneity in trial design, interventions, and out-come measures.
RESULTS
The initial search yielded 669 citations. Fifty-sevenarticles were identified during initial screening as
potentially relevant and in need of further review. Ofthose, 18 were excluded because they did not meetinclusion criteria (description of an intervention toimprove outcomes for elders discharged from theED), eight were excluded because they describedinterventions limited to a single presentation or diag-nosis, and five were excluded because they describedinterventions delivered only to patients who wouldhave otherwise been hospitalized. A total of 26 articleswere judged relevant to the aims of this review andappropriate for inclusion. Further bibliographicreview identified seven additional references. Theretrieved articles described 19 observational studiesor program descriptions, two nonrandomized clinicaltrials, and six randomized controlled trials (RCTs).Interventions reported in a descriptive manner arebriefly summarized first, followed by nonrandomizedclinical trials, then RCTs.
Observational Studies. A wide variety of programshave been designed and implemented to improve thecare of elder patients discharged from the ED. Pro-grams based in the ED include telephone follow-up,use of a specially trained nurse or team for geriatricassessment, and education for ED nurses in geriatricissues. Home-based programs include rapid referralto community home care services, as well as use of aspecially trained provider to perform in-home assess-ments. Observational studies describing interventionsto improve outcomes for elders discharged from theED are included in Table 1.
Telephone Follow-up. In a prospective, cohort studyperformed at a community teaching hospital, con-secutive patients older than 60 years who weredischarged from the ED were selected for telephonefollow-up by a research nurse within 72 hours of thepatient’s ED visit. Seventy-nine percent of patientswere successfully contacted and 40% received furtherclarification of their home care instructions. No infor-mation on outcomes or future service utilization wasprovided.9 Others have demonstrated the feasibilityof telephone follow-up and identified a large numberof unmet needs in this population.10–12
Specially Trained Nurse/Team in the ED.
Comprehensive Geriatric Assessment. A geriatric nursepractitioner performed comprehensive geriatric as-sessment on older adults discharged home from anED in Australia and found that 71% warranted sometype of community-based referral. Eighty-one percentof these patients were dependent in at least oneactivity of daily living (ADL).13
Geriatric Consultation Service. Gold and Bergmandescribed an ED geriatric consultation service staffedby a geriatrician, a full-time nurse clinician, and part-time physical and occupational therapists.14 Two-year
ACAD EMERG MED d October 2005, Vol. 12, No. 10 d www.aemj.org 979

follow-up of patients seen by the consultation servicerevealed that this population had high rates of hos-pital admission (63.5%), long-term institutionalization(51%), and mortality (33.7%); however, there was nocontrol group for comparison.15
Functional Assessment. A consultation service consist-ing of occupational and physical therapists providedcomprehensive functional assessment of patients iden-tified using a screening checklist. Results of the assess-ment were reported to ED staff, and therapists fromthe consultation service assisted with arranging com-munity resources for discharge care. Unfortunately,the authors were not able to obtain the plannedfollow-up data regarding outcomes.16
Care Coordination Team. Moss et al. described multi-disciplinary care coordination teams using a riskscreen with referral model. Overall ED admissionrates fell, but outcomes were not reported for theintervention cohort.17
Staff Educational Programs. A Canadian group con-ducted a one-day case-based workshop on geriatricissues attended by 101 emergency nurses. In one ofthe participating EDs, a persistent increase in thenumber of referrals to the home care program and theregional geriatric program was noted for one yearfollowing the workshop. This increase in referrals alsocoincided with the introduction of a quick responseinitiative (as described below), so it is not certainwhich intervention was responsible for the apparentchange in practice.18
Home-based Services.
Rapid Referral. Multiple Canadian studies have re-ported quick response initiatives, designed to pre-vent unnecessary hospitalizations of frail elders bypromptly coordinating services to their homes.19–24
This model has been adapted and described inAustralian settings as well.25,26 In a program designedby Brazil and colleagues, home services were rapidlyarranged following an ED-initiated referral. A case
manager visited the patient in the home within 72hours, and at five days the patient was transferred tothe most appropriate level of care.27 In an Americanstudy reported by Brookoff and Minniti-Hill, a nursecoordinator assessed adults about to be dischargedfrom the ED. Though a significant number of sur-veyed patients were judged eligible for home careservices, no information was reported on patientoutcomes.28
Health Visitors. In a project described by Bridges et al.,designated health visitors screened ED charts twiceweekly to identify potential clients aged 75 years andover discharged from the ED. Interventions includedtelephone calls, home visits, or referrals for eldersdeemed vulnerable by the health visitor, but nooutcome data were reported.29
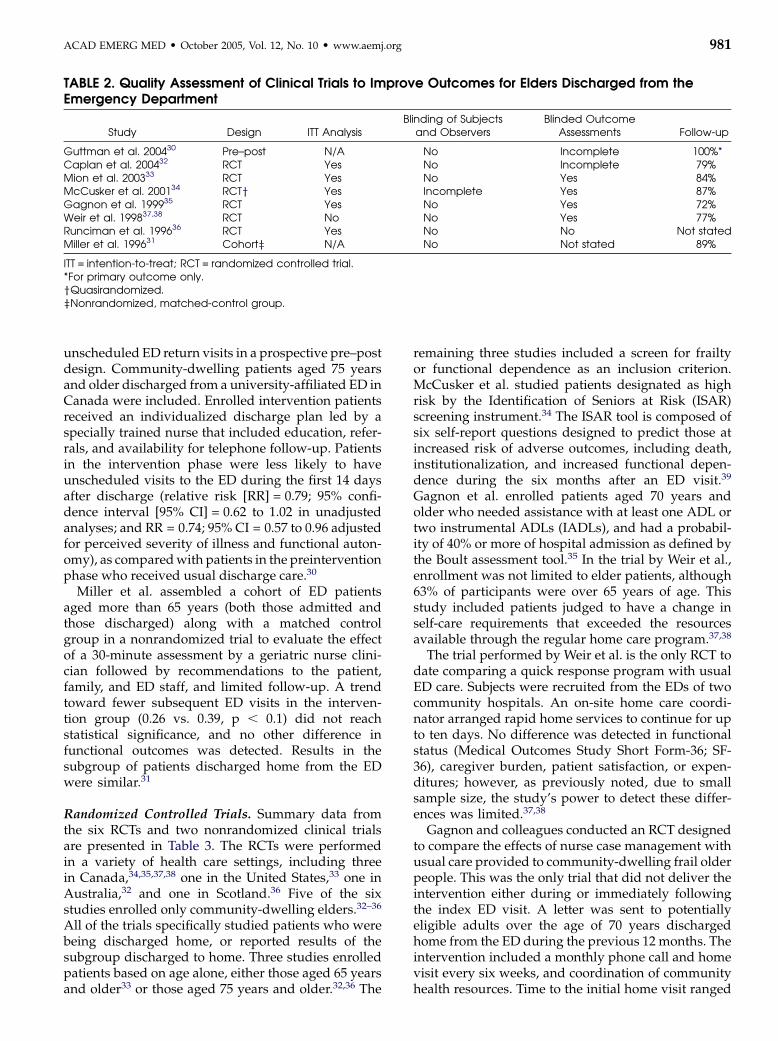
Clinical Trials. Table 2 shows the results of theassessment of methodologic quality for each of theclinical trials. Two studies were nonrandomized,one using a pre–post design30 and the other usinga prospective cohort with matched controls.31 SixRCTs were identified. The trials performed by Caplanet al., Mion et al., McCusker et al., and Gagnon et al.were of comparable quality; all were randomized,used ITT analysis, and had acceptably high rates offollow-up.32–35 Of note, the randomization in theMcCusker study was by day of visit instead of atthe patient level.34 While blinding of patients andinvestigators was not possible given the nature of theinterventions, outcome assessments were masked inmost cases. Exceptions included the DEED II trialperformed by Caplan and colleagues and the trial byRunciman and colleagues.32,36 In both cases, onlypartial blinding of outcome assessment was achieved.The study by Weir et al. had an insufficient samplesize to detect statistically significant differences inoutcomes and did not use ITT analysis.37,38
Nonrandomized Trials. A recent study by Guttmanet al. examined the effect of an ED-based nursedischarge plan coordinator versus usual care on
TABLE 1. Interventions to Improve Outcomes for Elders Discharged from the Emergency Department(ED): Observational Studies and Program Descriptions
Telephone Follow-upTrained Nurse/Team
in the ED Rapid Home-based Services Health VisitorsStaff Education
Programs
Poncia et al. 200010 Basic et al. 200213 Sinclair and Ackroyd-Stolarz 200021 Bridges et al. 200029 Brymer et al. 200118
Allen 199711 Moss et al. 200217 Brazil et al. 199827
Jones et al. 19979 Lee et al. 200116 Fry et al. 199626
McDonnell 198512 Gold and Bergman 199714 O’Grady et al. 199625
Sinoff et al. 199815 Rajacich and Cameron 199523
Brookoff and Minniti-Hill 199428
Freeman 199422,24
Darby 199219
Dawson and Critchley 199220
980 Hastings and Heflin d OUTCOMES OF DISCHARGED ELDERS
unscheduled ED return visits in a prospective pre–postdesign. Community-dwelling patients aged 75 yearsand older discharged from a university-affiliated ED inCanada were included. Enrolled intervention patientsreceived an individualized discharge plan led by aspecially trained nurse that included education, refer-rals, and availability for telephone follow-up. Patientsin the intervention phase were less likely to haveunscheduled visits to the ED during the first 14 daysafter discharge (relative risk [RR] = 0.79; 95% confi-dence interval [95% CI] = 0.62 to 1.02 in unadjustedanalyses; and RR = 0.74; 95% CI = 0.57 to 0.96 adjustedfor perceived severity of illness and functional auton-omy), as compared with patients in the preinterventionphase who received usual discharge care.30
Miller et al. assembled a cohort of ED patientsaged more than 65 years (both those admitted andthose discharged) along with a matched controlgroup in a nonrandomized trial to evaluate the effectof a 30-minute assessment by a geriatric nurse clini-cian followed by recommendations to the patient,family, and ED staff, and limited follow-up. A trendtoward fewer subsequent ED visits in the interven-tion group (0.26 vs. 0.39, p , 0.1) did not reachstatistical significance, and no other difference infunctional outcomes was detected. Results in thesubgroup of patients discharged home from the EDwere similar.31
Randomized Controlled Trials. Summary data fromthe six RCTs and two nonrandomized clinical trialsare presented in Table 3. The RCTs were performedin a variety of health care settings, including threein Canada,34,35,37,38 one in the United States,33 one inAustralia,32 and one in Scotland.36 Five of the sixstudies enrolled only community-dwelling elders.32–36
All of the trials specifically studied patients who werebeing discharged home, or reported results of thesubgroup discharged to home. Three studies enrolledpatients based on age alone, either those aged 65 yearsand older33 or those aged 75 years and older.32,36 The
remaining three studies included a screen for frailtyor functional dependence as an inclusion criterion.McCusker et al. studied patients designated as highrisk by the Identification of Seniors at Risk (ISAR)screening instrument.34 The ISAR tool is composed ofsix self-report questions designed to predict those atincreased risk of adverse outcomes, including death,institutionalization, and increased functional depen-dence during the six months after an ED visit.39
Gagnon et al. enrolled patients aged 70 years andolder who needed assistance with at least one ADL ortwo instrumental ADLs (IADLs), and had a probabil-ity of 40% or more of hospital admission as defined bythe Boult assessment tool.35 In the trial by Weir et al.,enrollment was not limited to elder patients, although63% of participants were over 65 years of age. Thisstudy included patients judged to have a change inself-care requirements that exceeded the resourcesavailable through the regular home care program.37,38
The trial performed by Weir et al. is the only RCT todate comparing a quick response program with usualED care. Subjects were recruited from the EDs of twocommunity hospitals. An on-site home care coordi-nator arranged rapid home services to continue for upto ten days. No difference was detected in functionalstatus (Medical Outcomes Study Short Form-36; SF-36), caregiver burden, patient satisfaction, or expen-ditures; however, as previously noted, due to smallsample size, the study’s power to detect these differ-ences was limited.37,38
Gagnon and colleagues conducted an RCT designedto compare the effects of nurse case management withusual care provided to community-dwelling frail olderpeople. This was the only trial that did not deliver theintervention either during or immediately followingthe index ED visit. A letter was sent to potentiallyeligible adults over the age of 70 years dischargedhome from the ED during the previous 12 months. Theintervention included a monthly phone call and homevisit every six weeks, and coordination of communityhealth resources. Time to the initial home visit ranged
TABLE 2. Quality Assessment of Clinical Trials to Improve Outcomes for Elders Discharged from theEmergency Department
Study Design ITT AnalysisBlinding of Subjects
and ObserversBlinded Outcome
Assessments Follow-up
Guttman et al. 200430 Pre–post N/A No Incomplete 100%*Caplan et al. 200432 RCT Yes No Incomplete 79%Mion et al. 200333 RCT Yes No Yes 84%McCusker et al. 200134 RCTy Yes Incomplete Yes 87%Gagnon et al. 199935 RCT Yes No Yes 72%Weir et al. 199837,38 RCT No No Yes 77%Runciman et al. 199636 RCT Yes No No Not statedMiller et al. 199631 Cohortz N/A No Not stated 89%
ITT = intention-to-treat; RCT = randomized controlled trial.*For primary outcome only.yQuasirandomized.zNonrandomized, matched-control group.
ACAD EMERG MED d October 2005, Vol. 12, No. 10 d www.aemj.org 981
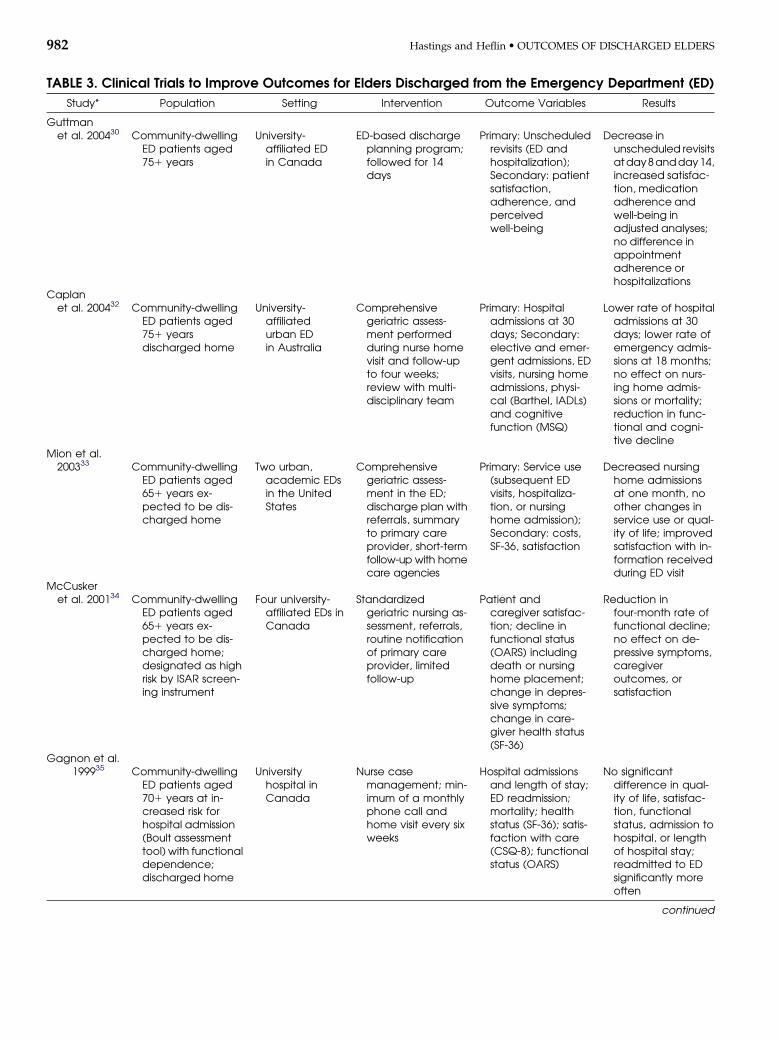
TABLE 3. Clinical Trials to Improve Outcomes for Elders Discharged from the Emergency Department (ED)
Study* Population Setting Intervention Outcome Variables Results
Guttmanet al. 200430 Community-dwelling
ED patients aged751 years
University-affiliated EDin Canada
ED-based dischargeplanning program;followed for 14days
Primary: Unscheduledrevisits (ED andhospitalization);Secondary: patientsatisfaction,adherence, andperceivedwell-being
Decrease inunscheduled revisitsatday8andday14,increased satisfac-tion, medicationadherence andwell-being inadjusted analyses;no difference inappointmentadherence orhospitalizations
Caplanet al. 200432 Community-dwelling
ED patients aged751 yearsdischarged home
University-affiliatedurban EDin Australia
Comprehensivegeriatric assess-ment performedduring nurse homevisit and follow-upto four weeks;review with multi-disciplinary team
Primary: Hospitaladmissions at 30days; Secondary:elective and emer-gent admissions, EDvisits, nursing homeadmissions, physi-cal (Barthel, IADLs)and cognitivefunction (MSQ)
Lower rate of hospitaladmissions at 30days; lower rate ofemergency admis-sions at 18 months;no effect on nurs-ing home admis-sions or mortality;reduction in func-tional and cogni-tive decline
Mion et al.200333 Community-dwelling
ED patients aged651 years ex-pected to be dis-charged home
Two urban,academic EDsin the UnitedStates
Comprehensivegeriatric assess-ment in the ED;discharge plan withreferrals, summaryto primary careprovider, short-termfollow-up with homecare agencies
Primary: Service use(subsequent EDvisits, hospitaliza-tion, or nursinghome admission);Secondary: costs,SF-36, satisfaction
Decreased nursinghome admissionsat one month, noother changes inservice use or qual-ity of life; improvedsatisfaction with in-formation receivedduring ED visit
McCuskeret al. 200134 Community-dwelling
ED patients aged651 years ex-pected to be dis-charged home;designated as highrisk by ISAR screen-ing instrument
Four university-affiliated EDs inCanada
Standardizedgeriatric nursing as-sessment, referrals,routine notificationof primary careprovider, limitedfollow-up
Patient andcaregiver satisfac-tion; decline infunctional status(OARS) includingdeath or nursinghome placement;change in depres-sive symptoms;change in care-giver health status(SF-36)
Reduction infour-month rate offunctional decline;no effect on de-pressive symptoms,caregiveroutcomes, orsatisfaction
Gagnon et al.199935 Community-dwelling
ED patients aged701 years at in-creased risk forhospital admission(Boult assessmenttool) with functionaldependence;discharged home
Universityhospital inCanada
Nurse casemanagement; min-imum of a monthlyphone call andhome visit every sixweeks
Hospital admissionsand length of stay;ED readmission;mortality; healthstatus (SF-36); satis-faction with care(CSQ-8); functionalstatus (OARS)
No significantdifference in qual-ity of life, satisfac-tion, functionalstatus, admission tohospital, or lengthof hospital stay;readmitted to EDsignificantly moreoften
continued
982 Hastings and Heflin d OUTCOMES OF DISCHARGED ELDERS

from 1 to 16 weeks, with an average of 4.5 weeks.Following the ten-month intervention period, outcomedata were collected by questionnaire and medicalrecord abstraction on hospital admissions, length ofstay, ED readmission rates, and mortality. Outcomemeasures also included quality of life (SF-36), satisfac-tion with care (Client Satisfaction Questionnaire; CSQ-8), and functional status (Older American Resourcesand Services Scale; OARS). No difference was detectedbetween the intervention and control groups with theexception of increased average number of ED visits inthe nurse case-management group (mean difference0.32; 95% CI = 0.01 to 0.63).35
Two trials tested an intervention that includedgeriatric assessment performed by a specially trainednurse in the ED.33,34 An RCT conducted by Mion et al.examined rates of service use (subsequent ED visits,hospitalizations, or nursing home admissions) amongcommunity-dwelling elders discharged from the EDfollowing a nurse-practitioner-led intervention. Theintervention included comprehensive geriatric assess-ment in the ED, formulation of a discharge planwith appropriate referrals, provision of a summaryto the patient’s primary care provider, and short-termfollow-up with home care agencies. There was noeffect on the primary outcome of overall service use,although nursing home admissions were reduced at30 days. These results must be interpreted withcaution, as the overall number of patients admittedto nursing homes was low: two (0.7%) in the inter-vention group vs. nine (3%) in the usual care group
(odds ratio [OR] 0.21; 95% CI = 0.05 to 0.99). Subgroupanalyses suggested that the intervention may havebeen more effective in decreasing service use amonghigh-risk patients. The SF-36 Physical and MentalComponent Subscale scores and health care costs didnot differ significantly between the groups. Partici-pants in the intervention group were more satisfiedwith the information received during the ED visit.33
McCusker et al. conducted a study of elder, commu-nity-dwelling ED patients who were expected to bedischarged home and had been designated as high riskby the ISAR screening instrument. The interventionconsisted of standardized geriatric nursing assessmentfollowed by appropriate referrals to primary care andhome services, routine notification of the patient’sprimary physician, and limited follow-up. Primaryoutcomes were patient and caregiver satisfaction,change in depressive symptoms, change in caregiverphysical and mental health, and change in functionalstatus defined as a three-or-more-point difference onthe OARS, institutionalization, or death. Results in-cluded a significant reduction in the four-month rate offunctional decline (adjusted OR 0.53; 95% CI = 0.31 to0.91). There was no effect on depressive symptoms,caregiver outcomes, or satisfaction. Return visits to theED were somewhat more likely in the interventiongroup (adjusted OR 1.6; 95% CI = 1.0 to 2.6).34
In two studies, the primary assessment was per-formed in the patient’s home.32,36 In the DEED II trial,Caplan et al. performed a comprehensive geriatricassessment in the patient’s home within 24 hours of
TABLE 3. Continued
Study* Population Setting Intervention Outcome Variables Results
Weir et al.199837,38 Adults being dis-
charged from theED with a changein care require-ments (63% age.65 years)
Two communityhospital EDsin Canada
Home carecoordinators in theED arrangedprompt delivery ofmultidisciplinaryin-home services
Primary: Health status(SF-36); Secondary:Caregiver burden,patient satisfaction,expenditures
No significantdifference de-tected, but smallsample size; powerto detect signifi-cant outcomedifferences 60%
Runcimanet al. 199636 Community-dwelling
ED patients aged751 years dis-charged home
Single center inScotland
Home visit by healthvisitor for standard-ized assessmentand referral tocommunity services
Dependencewith ADLs andIADLs at four weeks;readmission rates
Less dependent inIADLs; no significantdifference in ADLdependence orreadmission rates
Miller et al.199631 Adults aged 651
years seen in theED on study days(both admittedand discharged)
Urban ED inthe UnitedStates
Comprehensivegeriatric assess-ment in ED by nurseclinician; recom-mendations to pa-tient and ED staffand referrals; tele-phone follow-up
Mortality,institutionalization,health status, use ofmedical and socialservices, advancedirective, quality oflife
No significantdifference; trendtoward fewer sub-sequent ED visits inintervention group
*For complete reference citations, see the reference list.RCTs = randomized controlled trials; ISAR = Identification of Seniors at Risk35; ADLs = activities of daily living; IADLs = instrumentalactivities of daily living; MSQ = Mental Status Questionnaire; SF-36 = Medical Outcomes Study Short Form-36; OARS = Older AmericanResources and Services Scale; CSQ-8 = Client Satisfaction Questionnaire.
ACAD EMERG MED d October 2005, Vol. 12, No. 10 d www.aemj.org 983

discharge from the ED, and provided follow-up by amultidisciplinary outreach team for up to four weeks.The study was conducted in an academic urban EDin Sydney, Australia, and involved 739 patients aged75 years or more. The primary outcome measure wasall hospital admissions within 30 days. Secondaryoutcomes included elective and emergency admis-sions, nursing home admissions, mortality, physicalfunction (Barthel and IADL indexes), and cognitivefunction (Mental Status Questionnaire; MSQ). Patientsin the control group experienced a decline in theirmean Barthel score at six months (0.75 points; p ,
0.001 as compared with baseline) that was not ob-served in the intervention group. There was nodifference with regard to functional outcome scoresat 18 months. The intervention group had a lower rateof admission to the hospital during the first 30 daysafter the initial ED visit (16.5 vs. 22.2%; p = 0.049) but anonsignificant increase in the number of subjectsvisiting outpatient clinics and the ED. Only theDEED II trial investigated the long-term effect of in-terventions on health service utilization. The authorsobserved a significant reduction in emergency admis-sions at 18 months in the intervention group (44.4 vs.54.3%; p = 0.007).32
Runciman et al. conducted an RCT at a single centerin Scotland to assess the value of a research healthvisitor for patients aged 75 years and older dischargedfrom the ED. Intervention patients were visited athome, most within 24 hours, for a standardized assess-ment and referral to appropriate community services.Four weeks later, all patients (control and interventiongroup) were visited by a research occupational thera-pist, and the same assessment was performed. Out-comes included dependence with ADLs and IADLs atfour weeks, and readmission rates. Validated measure-ment instruments were not described. Interventionpatients were found to be less dependent in IADLs(60% vs. 74%, p = 0.027). There was no significantdifference in ADL dependence or readmission rates.The authors commented that differential compliancewith follow-up within the control group may haveaccounted for some of the observed differencesbetween the groups, but numbers are not providedto estimate the magnitude of the effect.36
DISCUSSION
Older patients discharged home from the ED face asignificant risk of adverse outcomes, including func-tional decline, return to the ED, hospitalization, anddeath.2–6 A variety of interventions ranging from staffeducation programs to comprehensive geriatric as-sessment and referrals have been developed thatspecifically target this population. A significant num-ber of observational studies demonstrate the feasi-bility of such interventions, and document a largeburden of unmet home care needs in this population.
Although we identified relatively few trials with acontrolled experimental design and rigorous evalua-tion of outcomes, important conclusions may bedrawn from the available data. Three of four RCTsdesigned to measure functional outcomes showedimprovements in the functional status of elders en-rolled in the intervention.32,34,36 The three positivetrials included 1) use of a specially trained nurse toperform geriatric assessment and 2) a component ofhome-based care. In the trials by Caplan et al. andRunciman et al., the assessment itself was performedin the patient’s home.32,36 In the McCusker trial, homecare referrals were initiated in the ED.34 A secondaryanalysis on process of care performed by McCuskeret al. found an increased rate of home care utilizationin the intervention group, suggesting that this mayhave been primarily responsible for the observedbenefit in functional status.40 No difference in func-tional status was detected in the trial by Gagnon et al.;however, the time between the ED visit and deliveryof the intervention was markedly longer than thosefor the other trials, potentially explaining this lack ofeffect.35
Another notable feature of the trials showing im-provement in functional status was their selection ofpatients at high risk of adverse outcomes. The trialsby Caplan et al. and Runciman et al. included onlypatients over 75 years of age.32,36 McCusker et al.enrolled patients designated as high risk by the ISARscreening instrument.34 Targeting a high-risk groupappears to be more effective than applying theseintensive interventions more broadly. It is not knownwhether this high-risk group should be the ‘‘olderold’’ group, or a group identified with a screeninginstrument. Keeping the identification of at-risk eldersin the ED brief and moving more of the interventionto the patient’s home have tremendous appeal as aneffective strategy for future study.
Is it possible to improve clinical outcomes forseniors discharged from the ED, and decrease serviceutilization rates? Clinical trial results available to datehave been mixed. The DEED II trial demonstratedreductions in hospital admissions at 30 days andemergency hospital admissions at 18 months.32 To thebest of our knowledge, this is the only RCT to dateto show any reduction in health service utilizationexcepting the decrease in nursing home admissionsdescribed by Mion and colleagues.33 The recent non-randomized trial by Guttman and colleagues foundthat unscheduled ED visits could be reduced at14 days.30 Conversely, ED return visits were actuallyincreased in the intervention groups described byMcCusker et al.34 and Gagnon et al.,35 and there wasa nonsignificant trend toward increased visits to theED and other outpatient providers in the DEED IIstudy.32 The potential for increased rates of serviceutilization in health services intervention trials hasbeen previously documented.41 Providing additional
984 Hastings and Heflin d OUTCOMES OF DISCHARGED ELDERS

care to relatively underserved populations is likely touncover more needs that require additional services.
Performing health services intervention trials inthis setting and population is extremely challenging.Interventions are difficult to standardize, blind, andrandomize. It should be noted that two RCTs thatshowed positive effects did not perform blinded out-come assessments.32,36 It is critical that future researchbe designed to minimize this potential source of bias. Inaddition, further work needs to be done to investigatethe current process of care for elders discharged fromthe ED. High-quality studies are needed to evaluatecommunication between the ED and primary physi-cian, rate and length of time until follow-up, andappropriateness of prescription medication. A morecomplete understanding of all of the factors that impactclinical outcomes and health service utilization is crit-ical to building effective interventions.
LIMITATIONS
Potential limitations of this review include incompleteidentification of relevant studies and publication bias.We conducted searches of bibliographies and consultedwith content experts in the field in order to minimizethese possibilities. Although a meta-analysis of resultswould have been ideal, quantitative analysis was notappropriate due to heterogeneity in trial design andoutcome measurements. The studies were also per-formed in very different health care systems, whichmay potentially limit the generalizability of results.
CONCLUSIONS
The discharge of elder patients from the ED to homerepresents an important transition of care for olderadults, and a key opportunity for interventions toprevent further health decline. Leaders in both emer-gency medicine and geriatric medicine have issueda call for further research in this area.7 Randomizedclinical trial data have shown that functional declinein high-risk elders following an ED visit can bereduced using various intervention models that in-clude geriatric nursing assessment and home-basedservices. It is not clear whether further health serviceutilization can be consistently altered. Developmentof interventions to improve the care of elder patientsfollowing ED visits requires further research intosystem and patient-centered factors that impact healthcare delivery in this situation.
The authors thank Harvey J. Cohen, MD, and Eleanor McConnell,RN, PhD, for their thoughtful review of the manuscript.
References
1. McCaig LF, Burt CW. National Hospital Ambulatory MedicalCare Survey: 2002 ED Summary. Advance data from Vital and
Health Statistics. Hyattsville, MD: National Center for HealthStatistics, 2004.
2. Aminzadeh F, Dalziel WB. Older adults in the emergencydepartment: a systematic review of patterns of use, adverseoutcomes, and effectiveness of interventions. Ann Emerg Med.2002; 39:238–47.
3. Denman SJ, Ettinger WH, Zarkin BA, Coon PJ, Casani JA.Short-term outcomes of elderly patients discharged from anemergency department. J Am Geriatr Soc. 1989; 37:937–43.
4. Rowland K, Maitra AK, Richardson DA, Hudson K,Woodhouse KW. The discharge of elderly patients from anaccident and emergency department: functional changes andrisk of readmission. Age Ageing. 1990; 19:415–8.
5. Caplan GA, Brown A, Croker WD, Doolan J. Risk ofadmission within 4 weeks of discharge of elderly patientsfrom the emergency department—the DEED study. Dischargeof elderly from emergency department. Age Ageing. 1998;27:697–702.
6. McCusker J, Cardin S, Bellavance F, Belzile E. Return to theemergency department among elders: patterns and predictors.Acad Emerg Med. 2000; 7:249–59.
7. Wilber ST, Gerson LW. A research agenda for geriatricemergency medicine. Acad Emerg Med. 2003; 10:251–60.
8. Coleman EA. Falling through the cracks: challenges andopportunities for improving transitional care for personswith continuous complex care. J Am Geriatr Soc. 2003; 51:549–55.
9. Jones JS, Young MS, LaFleur RA, Brown MD. Effectiveness ofan organized follow-up system for elder patients released fromthe emergency department. Acad Emerg Med. 1997; 4:1147–52.
10. Poncia HD, Ryan J, Carver M. Next day telephone follow upof the elderly: a needs assessment and critical incidentmonitoring tool for the accident and emergency department.J Accid Emerg Med. 2000; 17:337–40.
11. Allen D. Telephone follow up for older people dischargedfrom A&E. Nurs Stand. 1997; 11:34–7.
12. McDonnell L. Emergency room follow-up program fordischarged elderly. Health Prog. 1985; 66:24.
13. Basic D, Conforti D, Rowland J. Standardised assessmentof older patients by a nurse in an emergency department.Aust Health Rev. 2002; 25:50–8.
14. Gold S, Bergman H. A geriatric consultation team in theemergency department. J Am Geriatr Soc. 1997; 45:764–7.
15. Sinoff G, Clarfield AM, Bergman H, Beaudet M. A two-yearfollow-up of geriatric consults in the emergency department.J Am Geriatr Soc. 1998; 46:716–20.
16. Lee V, Ross B, Tracy B. Functional assessment of older adults inan emergency department. Can J Occup Ther. 2001; 68:121–9.
17. Moss JE, Flower CL, Houghton LM, Moss DL, Nielsen DA,Taylor DM. A multidisciplinary care coordination teamimproves emergency department discharge planning practice.Med J Aust. 2002; 177:435–9.
18. Brymer C, Cavanagh P, Denomy E, et al. The effect of ageriatric education program on emergency nurses. J EmergNurs. 2001; 27:27–32.
19. Darby PW. Quick response teams: a new approach inutilization management. Leadersh Health Serv. 1992; 1:27–31.
20. Dawson JI, Critchley L. Community-hospital partnerships.The quick response team. J Nurs Admin. 1992; 22:33–9.
21. Sinclair D, Ackroyd-Stolarz S. Home care and emergencymedicine: a pilot project to discharge patients safely from theemergency department. Acad Emerg Med. 2000; 7:951–4.
22. Freeman M. Quick response programs: effective managementof a population in crisis. Leadersh Health Serv. 1994; 3:36–9.
23. Rajacich DL, Cameron S. Preventing admissions of seniors intothe emergency department. J Gerontol Nurs. 1995; 21:36–40.
24. Freeman M, Zack E. Triaging seniors in health crisis in theemergency department: a three-year summary. Perspectives.1996; 20:8–11.
ACAD EMERG MED d October 2005, Vol. 12, No. 10 d www.aemj.org 985

25. O’Grady S, Fairbrother G, Farrington C. Matching needs toservices: the quick response. Case study: St. George Hospitaland Community Health Services Best Practice Project. AustHealth Rev. 1996; 19:100–12.
26. Fry M, Ekholm J, Farrington C. Quick response program: anew emergency initiative for the elderly. Aust Emerg Nurs J.1996; 1:42–5.
27. Brazil K, Bolton C, Ulrichsen D, Knott C. Substituting homecare for hospitalization: the role of a quick response service forthe elderly. J Community Health. 1998; 23:29–43.
28. Brookoff D, Minniti-Hill M. Emergency department-basedhome care. Ann Emerg Med. 1994; 23:1101–6.
29. Bridges J, Meyer J, McMahon K, Bentley J, Winter J. A healthvisitor for older people in an accident and emergencydepartment. Br J Community Nurs. 2000; 5:75–80.
30. Guttman A, Afilalo M, Guttman R, Colacone A, et al. Anemergency department-based discharge coordinator for elderpatients: does it make a difference? Acad Emerg Med. 2004; 11:1318–27.
31. Miller DK, Lewis LM, Nork MJ, Morley JE. Controlled trial ofa geriatric case-finding and liaison service in an emergencydepartment. J Am Geriatr Soc. 1996; 44:513–20.
32. Caplan GA, Williams AJ, Daly BD, Abraham K. A randomizedcontrolled trial of comprehensive geriatric assessment andmultidisciplinary intervention after discharge of elderly fromthe emergency department—the DEED II study. J Am GeriatrSoc. 2004; 52:1417–23.
33. Mion LC, Palmer RM, Meldon SW, et al. Case finding andreferral model for emergency department elders: arandomized clinical trial. Ann Emerg Med. 2003; 41:57–68.
34. McCusker J, Verdon J, Tousignant P, de Courval LP, DendukuriN, Belzile E. Rapid emergency department intervention forolder people reduces risk of functional decline: results of amulticenter randomized trial. J Am Geriatr Soc. 2001; 49:1272–81.
35. Gagnon AJ, Schein C, McVey L, Bergman H. Randomizedcontrolled trial of nurse case management of frail older people.J Am Geriatr Soc. 1999; 47:1118–24.
36. Runciman P, Currie CT, Nicol M, Green L, McKay V. Dischargeof elderly people from an accident and emergency department:evaluation of health visitor follow-up. J Adv Nurs. 1996; 24:711–8.
37. Weir R, Browne G, Byrne C, et al. The quick response initiativein the emergency department: who benefits? Health CareManag Sci. 1999; 2:137–48.
38. Weir R, Browne G, Byrne C, et al. The efficacy and efficiency ofthe quick response program: a randomized controlled trial.Can J Aging. 1998; 17:272–95.
39. McCusker J, Bellavance F, Cardin S, Trepanier S, Verdon J,Ardman O. Detection of older people at increased risk ofadverse health outcomes after an emergency visit: the ISARscreening tool. J Am Geriatr Soc. 1999; 47:1229–37.
40. McCusker J, Dendukuri N, Tousignant P, et al. Rapid two-stageemergency department intervention for seniors: impact oncontinuity of care. Acad Emerg Med. 2003; 10:233–43.
41. Weinberger M, Oddone EZ, Henderson WG. Does increasedaccess to primary care reduce hospital readmissions?Veterans Affairs Cooperative Study Group on PrimaryCare and Hospital Readmission. N Engl J Med. 1996; 334:1441–7.
986 Hastings and Heflin d OUTCOMES OF DISCHARGED ELDERS