Embed Size (px)
Citation preview

A Systems Approach to Preventing and Controlling Non-communicable Diseases in Low Resource and Emerging Economies:
K.M.Venkat NarayanRuth and O.C. Hubert Professor
Emory University, AtlantaConsortium of Universities of Global Health, Seattle, 20 September, 2010


Two types of approaches to combating a problem
Transformational – that aims to achieve large, permanent improvements in broad social and economic indicators
Marginal – that attempts to solve a specific problem for a targeted group of beneficiaries
Bendavid, Miller. JAMA, 2010

Some desirable qualities of a health system for NCD
Data for decision-making & evaluation Decisions should be evidence-based Resource allocation proportional to expected
outcomes Integrated and organized care Low-cost & affordable interventions Scalablity

Setting intervention priorities in developing countries - Challenges
Little direct evidence on the effectiveness or cost-effectiveness of interventions in developed countries
Translating evidence from developed countries to the context of developing countries

Assessing Priorities for ImplementationDisease Control Priorities-2 Chapter 30
http://www.dcp2.org/pubs/DCP
Program Priorities
R&D Priorities
1. Burden
2. Intervention effectiveness & cost-effectiveness
3. Level of implementation or quality of care

Methods for setting intervention priorities in developing countries
Translating the cost-effectiveness evidence from developed countries to the context of developing countries by assuming
• Same effectiveness• Different costs for the intervention and medical care
Feasibility of interventions • Reach• Technical complexity• Capital intensity• Cultural acceptability
Ranking interventions to set implementation priority

Levels of Intervention Priorities
OneCost saving and highly feasible
TwoCost saving or cost <1,500/QALY and pose some
feasibility challenges Three
Cost 1,500-8,550/QALY and pose considerable feasible challenges

Primary Prevention Interventions for Diabetes
Intervention Cost/QALY (2001 $)
Feasibility Priority
Prev (L/S) 130 ++ 1
Prev (Metformin) 3,630 ++ 3

Secondary Prevention - Priority One Interventions
Intervention Cost/QALY (2001 $)
Latin America
Feasibility
Control HbA1c <9% Cost saving ++++
BP <160/95 Cost saving ++++
Foot care Cost saving ++++

Secondary Prevention - Priority Two Interventions
Intervention Cost/QALY (2001 $)
Latin America
Feasibility
Preconp care Cost saving ++
Fluvac 360 ++++
Eye exam 700 ++
Smoking cessation
1,450 ++
ACE-I for all 1,020 +++

Secondary Prevention - Priority Three Interventions
Intervention Cost/QALY (2001 $)
Latin America
Feasibility
TC <200 mg/dl 7,350 +++
HbA1c<8% 4,000 ++
Screening DM 8,550 ++
Microab test 5,510 ++

Need direct evidence from developing countries
Two examples
1. Primary prevention translation trial in Chennai, India
2. Secondary prevention translation trial in eight centers in India/Pakistan

CDCCENTERS FOR DISEASE COTROL
AND PREVENTION
Intervention Studies: 1 Prevention
IDF BRiDGES Translation Trial (D-CLIP)Evaluate effectiveness, cost-effectiveness, sustainability of
culturally-congruent , low-cost 1 prevention strategies
• Screening 12-15,000 people; n=700 Pre-diabetes (IFG, IGT, both) randomized
• Lifestyle delivered by lay educators / community ambassadors + Peer support groups
• Metformin after 4 m, if needed (ADA guidelines)

Program Evaluation
1. Effectiveness
2. Cost-effectiveness
3. Sustainability
4. Scalability under discussion

CDCCENTERS FOR DISEASE COTROL
AND PREVENTION
NHLBI/OvationsNHLBI/Ovations C Centre for Centre for CAArdiometabolic rdiometabolic RRisk isk RReduction eduction in in SSouth Asia - outh Asia - CARRSCARRS
New DelhiNew Delhi
ChennaiChennai
KarachiKarachiAtlantaAtlanta
K.M. Venkat K.M. Venkat NarayanNarayanM.K. AliM.K. Ali
E.W. GreggE.W. Gregg
M. KadirM. Kadir D. D. PrabhakaranPrabhakaranK. Srinath K. Srinath ReddyReddy
N. Tandon N. Tandon V. Mohan V. Mohan
Research Coordinating Centre (RCC) atResearch Coordinating Centre (RCC) atPublic Health Foundation of India (PHFI)Public Health Foundation of India (PHFI)

CDCCENTERS FOR DISEASE COTROL
AND PREVENTION
Intervention Studies: 2 Prevention
Ovations/NHLBI Translation Trial (CARRS)Evaluate effectiveness, cost-effectiveness, sustainability of low-
cost, multi-factorial 2 prevention strategies
• n=1,120 people with diabetes at 8 centers
• Care coordinator
• Decision support software
• Guidelines driven comprehensive diabetes and CVD management

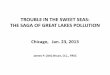
SiteRandomized Individuals Assignment Outcomes
CARRS Translation TrialCARRS Translation Trial
14070
140
14070
70
70
70
70
8 sites Total sample ~ 1,120
ControlUsual care
InterventionSupported
Intensive care
1.Care coordinator2.Decision Support3.Guidelines
1° OutcomeProportion achieving multiple RF control (HbA1c & 1 other)
2° Outcomes•Cost-effectiveness•QOL •Satisfaction

Conclusions By systematically implementing known cost-
effective interventions• Diabetes incidence can be halved
• Diabetes complications can be halved
Better data on effectiveness and cost-effectiveness in developing country settings are needed
Investing in programs of unproven effectiveness or cost-ineffectiveness is a waste of limited resources
Need to invest in system infrastructure

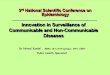
Quantity of Unmet MDG Progress
IMR Child Mortality
TB Mortality HIV Prevalence
10% higher GDP per capita
-0.17% -0.16% -1.80% 1.10%
1% GDP Higher health spending
-2.23% -2.35% -3.57% -2.96%
1 Additional physician/10,000
-0.38% -0.26% -1.47% -0.09%
10% Higher NCD Mortality rate
6.32% 5.78% 7.56% 2.03%
Stuckler et al. PLoS 2010
Why Child Health and Infectious Disease Improvements Depend on Reducing NCD Mortality?