Embed Size (px)
Citation preview
The New England Deaconess Hospital shares with our readers their objectives and experiences in the training of technicians for the operating room.
A TRAINING PROGRAM
FOR TECHNICIANS Ruth E. Pendleton, R.N.
It is generally recognized that a shortage of graduate registered operating room nurses exists. We may understand the factors which
This paper was presented at the 12th Annual AORN Congress in New York City, Febru- ary, 1965, and it reports experiences only through 1964. The author i s Director of
Surgical Services at the New England Dea- coness Hospital in Boston. She attended the Walthum School of Nursing in Waltham, Massachusetts, Cornell University-New York Hospital, and Boston University. Active in AORN activities, Miss Pendleton has held the ofices of President, Vice President and Treasurer in her local chapter and has been a member of the Board of Directors and the Educational Committee for National AORN. She is currently Chairman of the Editorial Committee.
contribute to this shortage, and may agree or disagree with the educators’ beliefs re- garding the place of the operating room in the education of student nurses, but it is imperative that we realize and accept the need to supplement the operating room nursing staff. Note that the word “supple- ment” is used. The operating room cannot use substitutes.
For many years nurses’ aides and licensed practical nurses have been employed in gen- eral nursing services to supplement the pro- fessional nursing staff, but the operating room has been slower to use such personnel. Today, therefore, the education, training and employment of supplementary operating room personnel (technicians) is of major concern to operating room nursing. The fol- lowing discussion concerns the training pro- gram and employment of technicians in the
Jan-Feb 196G 63

operating rooms of the New England Deaconess Hospital, Boston, Massachusetts.
BACKGROUND Most operating room nurses are familiar
with the Surgical Technical Aide Instructor’s Manual which was published by the Ameri- can Hospital Association in 1954. This much- needed manual has been widely used to set up instruction programs. It was the first attempt to set forth standards of qualifica- tions and curriculum for the training of surgical technicians. The manual proposes a five-week course but many throughout the country have expanded this to six, nine or twelve-month programs. This has been found necessary to provide a lay person with ade- quate theoretical knowledge and clinical practice for effective and safe participation in care of the operative patient. Personnel with such a background should be classified as technicians, not as technical aides.
Despite the fact that 11 years have passed since this publication became available, defi- nitions are still needed for the scope of the technician’s responsibilities, for the stand- ards for qualifications, and for a basic cur- riculum. These statements should come from one or more of the recognized authoritative organizations directly concerned with, and established by, nurses. The development of the ANA-AORN Conference Group on Operating Room Nursing is most encourag- ing and we hope that this will be the body which will set forth these needed statements. This would do much to promote standardi- zation of programs throughout the country.
BACKGROUND OF NEW ENGLAND DEACONESS PROGRAM
In 1958, the decision was made to pro- vide a program to train technicians for em- ployment in our own hospital. Miss Margaret A. Burns, Associate Director of the Depart- ment of Surgeries, assumed complete respon- sibility for developing the curriculum, and
for the teaching of the program. This was to be a six-month, intensive course in theory and practice. Our first technician (there was only one student in the first class), and all subsequent students who were trained for the express purpose of employment in our hospital, were given this same six-month course.
In 1963, i t was decided that we could take larger classes and train technicians for em- ployment in other hospitals. At this time, the course and training period were ex- panded to one year. The extended period and the larger classes are shown in Figure 1.
Total Number of Students Trained and Certified
1958 1959 1960 196 I I 962 1963 1964- I 1964-9
Fig. 1
I 6 month course I I 3 I 5 I year course 3 9 (student trainees)
I1
I1
I1
I1
I1
Through past experience, and from the ex- pressed opinions of students, we had learned that the technician needed more than six months to function adequately. An addi- tional six months of clinical practice was needed to become an efficient team member, capable of participating in all types of surgi- cal procedures.
PURPOSE AND OBJECTIVES The purpose of our program is to prepare
non-professional ancillary workers through theoretical instruction and practical exper- ience to carry out operating room techniques and procedures, under supervision.
The objectives are threefold: 1 ) To develop complete understanding
of proper aseptic techniques, and also a basic
64 AORN Journal

understanding of the fundamentals of anatomy, microbiology, anesthesia and var- ious surgical procedures.
2 ) To become aware of and understand the importance of teamwork, and of the technician’s role on the team.
3) To become aware that several major factors contribute to successful surgery.
SELECTION AND QUALIFICATIONS OF CANDIDATES
In the past our philosophy has been to re- cruit from our orderly and aide personnel, and from all levels of interested persons out- side the hospital. As a result of an initial statement from the ANA-AORN Conference Group on Operating Room Nursing, concern- ing the qualifications of the surgical assistant, we are attempting to recruit only licensed practical nurses for our next class. We are anxious to have this opportunity of compar- ing a group with 15 to 24 months’ formal training with other groups which have had a variety of preparation. [The class referred to was started in March 1965.1
Qualifications for recruitment have been established which we do not consider in- fallible, but which do give us a guide for evaluating the prospective student. In the initial contact, we use interviews by the Personnel Department, and by the Director and Associate Director of the Department of Surgeries. Candidates must be high school graduates, or the equivalent, with a satisfac- tory scholastic record. The L.P.N.s must be graduates of an accredited school and prefer- rably licensed; however, we will admit them pending results of their examination if they come to us directly from school. We require them to take the General Aptitude Test Bat- tery; we check work references; and we try to determine whether or not the prospect has a genuine interest in the field.
CURRICULUM The curriculum appears below, with the
total number of hours devoted to each subject : Orientation 24 hours Circulating responsibilities 12 hours Anatomy and Physiology 22 hours Principles and application of
aseptic techniques 85 hours Bacteriology, and principles and
methods of sterilization 10 hours Anesthesia 4 hours Terminology 4 hours Surgical procedures 55 hours
Orientation includes tours of the hospital and the department; introduction to the course; discussion of hospital policies; ethics and legal aspects; definition, aims and his- tory of surgery; technician responsibilities and details of duties; and specific location of supplies and equipment in the main storage rooms and in the operating rooms.
Circulating responsibilities include all as- pects in the care of the patient, the operating room, and the team.
Principles and application of aseptic tech- niques include study of theory, demonstra- tions, return demonstrations, and practice or drill prior to participation in operations.
As each aspect is mastered the student is allowed to scrub, as a member of the team, in progressively more complicated opera- tions. Initially, he scrubs with an instructor and only when he is considered capable is he allowed to scrub alone. The instructor scrubs with the student, as needed, to introduce him to more complicated procedures. The stu- dents average about 165 scrubs for opera- tions during their first year with us. They scrub on every type of operation except cardiac surgery but they do have an op- portunity to observe and assist the circula- tion nurse with that.
The student is required to write a case study during the second section of the first 25 weeks. He is helped with this project by the nurse in charge of the rooms where he is
Jan-Feb 1966 65

working at the time. The nurse goes with him to the patient floor to discuss the chart, and to visit the patient pre- and postopera- tively. While the student is writing the study he participates in a preliminary instruction class, and in discussion periods. On comple- tion, each student presents his case study to the class.
Only four hours are devoted to the basics of terminology; however, the topic is stressed in all subjects presented, particularly throughout the discussion of surgical pro- cedures. For each surgical procedure there is detailed discussion of all the anatomical systems and organs involved, supplemented with illustrations, films, and study.
Because we find that it takes time for the students to comprehend and retain the ma- terial, we try not to overwhelm them with too much at a time. We find that in order to get through the curriculum in a reasonable time we must plan an average of 22 hours of class weekly for the first six weeks; six hours of class weekly for the second six- week period; and four hours of class per week for the next 13 weeks. With the re- duction of daily classes, increased time is spent in observation and clinical practice.
There is one hour of planned study during on-duty time each day for the first 25 weeks. A quiz is given at the end of each two-week period, and examinations at the end of the twelfth and twenty-fifth weeks. Reading as- signments are given to correspond with each class, and many films are used to supple- ment the material given in class. Ample op- portunity is given for conferences with the students who are encouraged to question and discuss those things which they see and do during their observation periods and in clinical practice.
Practical apprentice training is carried out for the final 25 weeks, with careful plan- ning to assure that the student is “exposed” to all types of surgery. The students are on duty eight hours per day, Monday through
Friday. During the latter part of their clini- cal practice they are assigned to take call, in order to acquaint them with this part of operating room nursing. A week of vacation is given at the end of the twenty-fifth week and terminally, the fifty-second week. Ten days sick leave are permitted, and ten holi- days are given throughout the year.
Upon successful completion of the pro- gram, the student is presented with a certifi- cate which indicates that he or she has satisfactorily completed a one-year course of instruction and practical experience, as pre- scribed by our hospital, and that he is a qualified surgical technician. On the inner fold of the certificate we include a statement of exactly what responsibilities we have prepared the technician to accept.
RESULTS OF THE PROGRAM In the past seven years (through 1964) a
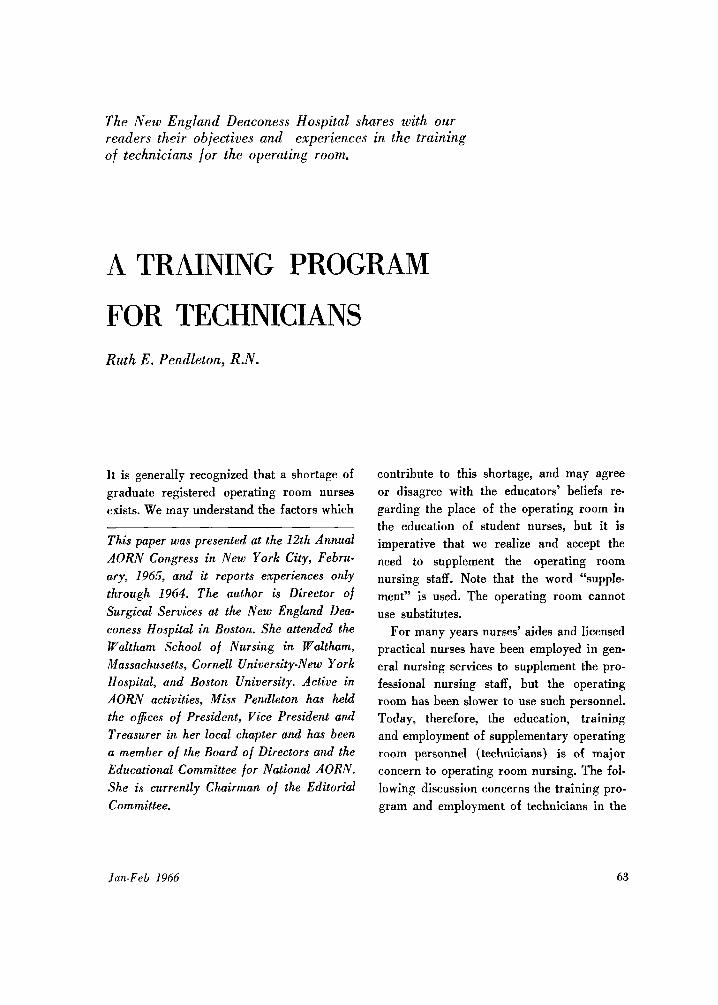
total of 34 students have begun the program. Of these, 15 have been trained and certified, nine are student trainees, and ten have dropped out. The educational and work backgrounds of these students vary widely, as will be seen in Figure 2. In this Figure, the classification “College, etc.” represents the following: college, university, secretarial school, dental technician school, and junior college.
“A,” with only one year of high school, and “B,” with three years, were taken from our orderly staff. We had not established formal criteria for qualifications at this time and we felt the students could do well with- out having had four years of high school. They have proved to be excellent workers.
E has an excellent educational back- ground, obtained mostly in the Ukraine. I t cannot be recognized in the United States, however, since she is unable to produce the necessary papers. She is licensed as an L.P.N. by waiver. Two girls (“My’ and “0”) had to leave
nursing school and perhaps would have
LL 7,
66 AOKN Journal
EDUCATIONAL BACKGROUND OF 15 TRAINED TECHNICIANS
High School
lxn
Years I 2 3 4 5 6
Col lege,etc.
I 2 3
LPN USAF Nursing Medical School School
m m
m m
15mo. 1 2 1 2 3 4 1 2
WORK BACKGROUND OF 15 TRAINED TECHNICIANS
NEDH Orderly -I years Train Salesman - 2years; Cook - 3yeors; NEDH Orderly-Gmonths
LPN-Syears USAF -2years; Nurse Assistant-2years; NEDH Orderly-2months L P N - 9 years NEDH Orderly - I4yeor-s
Secretary- 2 years; LPN -20months NEDH Orderly - I month NEDH Ward Hostess - 4 &months
Calculator Operator - 5 Y! years
Student NE OH Orderly - 3 years
Clerk Typist - l year; Nursing School -15months
General Office Work and Bookkeeper - I5 years Student; Nursing School - I & years
Jan-Feb 1966 67
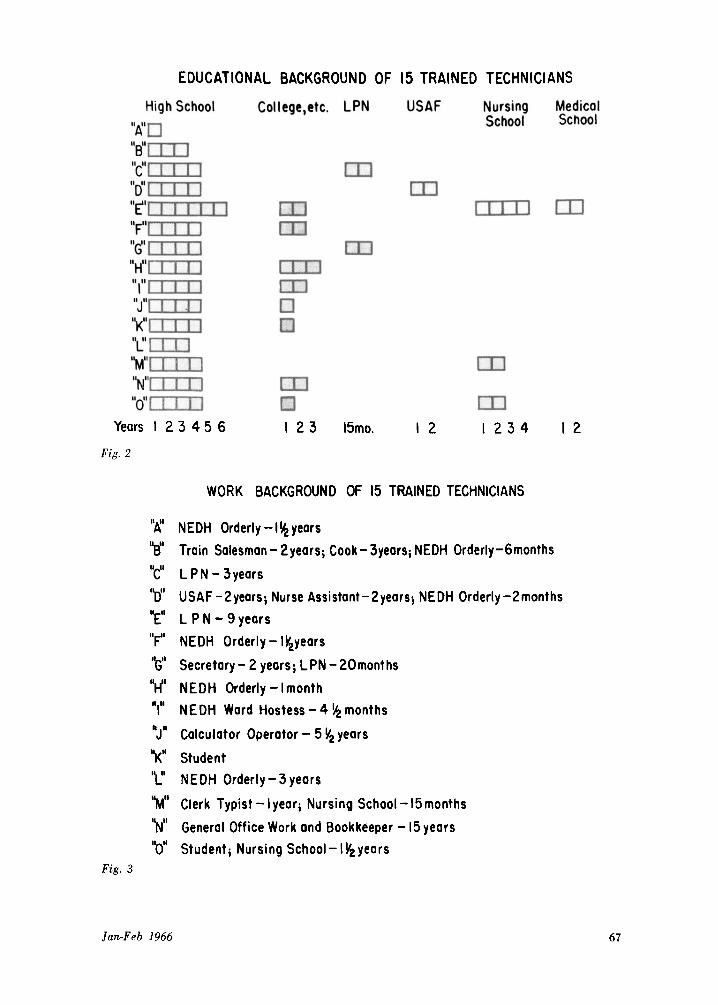
been lost to the medical field. the nine student technicians (Figure 4) It is interesting to note that in the work show that six of the nine had some sort of
background (Figure 3) of these 15 techni- medical experience. We have found that the cians, only three had no experience in hospi- more experience a student has in the medical tal or medical environments prior to taking field, the more readily he adjusts; some ex- the course. perience is better than none, but (logically)
The educational and work backgrounds of the more, the better.
NEW ENGLAND DEACONESS HOSPITAL BACKGROUND OF 9 STUDENT TECHNICIANS
High School
Years I 2 3 4 5 Fig. 4
Colleqe,etc. Nursing
Medical Secretary- I year Medical Secretary-3years Electronics Asst.Cont.Prod.Mgr.-I!$ yeors Marine Corps - 4years; Medical Attendont -4years Nurses Aide - 4 years Salesgirl - 4 years WAC, Lab Technician - I year Dental Assistant - 2 yeors General Office Work-9weeks
I 2 3 I
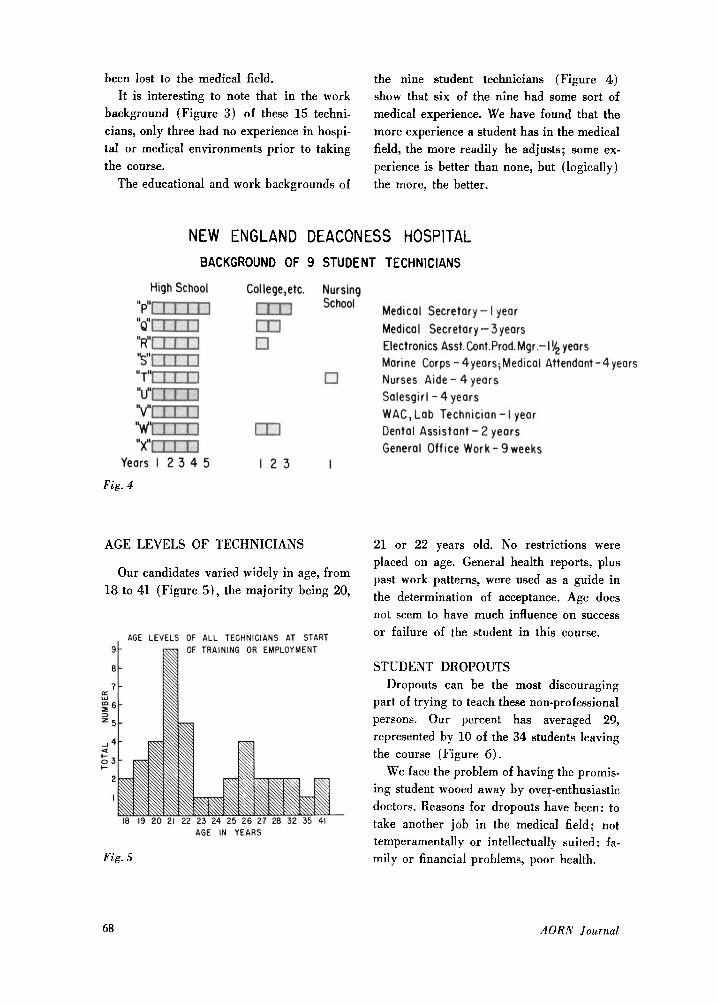
AGE LEVELS OF TECHNICIANS 21 or 22 years old. No restrictions were placed on age. General health reports, plus past work patterns, were used as a guide in Our candidates varied widely in age, from
l8 to 41 (Figure 5), the majority being 20, the determination of acceptance. Age does not seem to have much influence on success
AGE LEVELS OF ALL TECHNICIANS AT START or failure of the student in this course. 9 OF TRAINING OR EMPLOYMENT
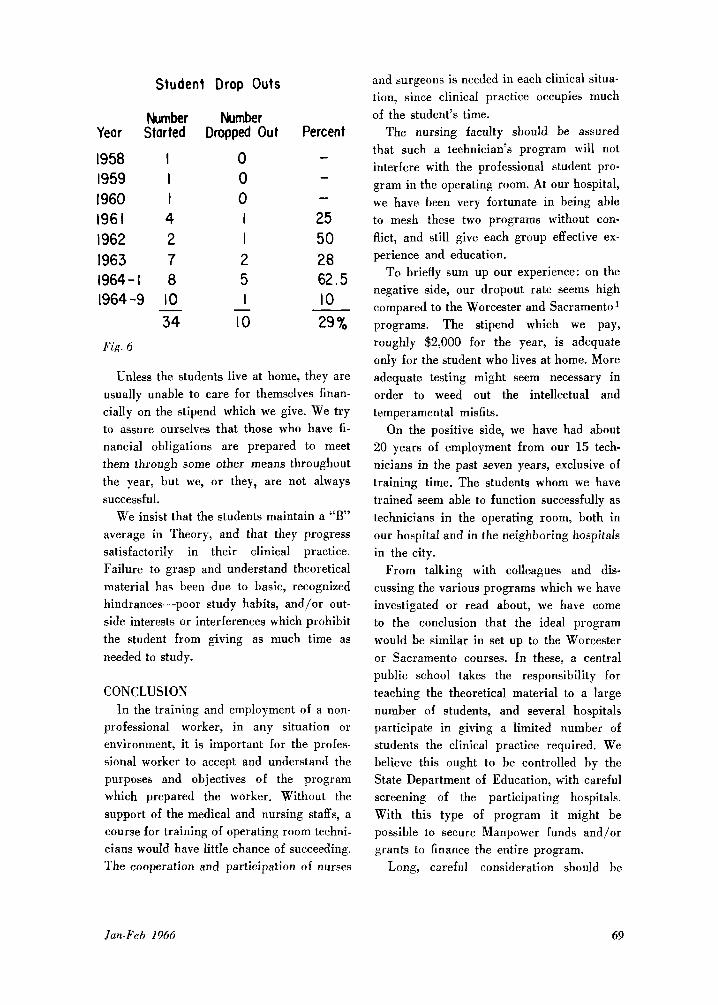
8 STUDENT DROPOUTS 7 Dropouts can be the most discouraging
part of trying to teach these non-professional Z 6 = 5 persons. Our percent has averaged 29,
represented by 10 of the 34 students leaving 2 4 the course (Figure 6 ) . 53
We face the problem of having the promis- ing student wooed away by oveq-enthusiastic doctors. Reasons for dropouts have been: to take another job in the medical field; not temperamentally or intellectually suited; fa- mily or financial problems, poor health.
II: w
3
a
!-
2
I
18 19 20 21 22 23 24 25 26 27 28 32 35 41 AGE IN YEARS
Fig. 5
68 AORN Journal
Year
1958 1959 I960 196 I I962 1963
Student Drop Outs
Number Started
I I I 4 2 7
Number Dropped Out
0 0 0 I I 2
1964-1 8 5 I 1964-9 10
34 10 - -
Fig. 6
Percent - - - 25 50 28 62.5 10 29 %
Unless the students live at home, they are usually unable to care for themselves finan- cially on the stipend which we give. We try to assure ourselves that those who have fi- nancial obligations are prepared to meet them through some other means throughout the year, but we, or they, are not always successful.
We insist that the students maintain a “B” average in Theory, and that they progress satisfactorily in their clinical practice. Failure to grasp and understand theoretical material has been due to basic, recognized hindrances-poor study habits, and/or out- side interests or interferences which prohibit the student from giving as much time as needed to study.
CONCLUSION In the training and employment of a non-
professional worker, in any situation or environment, it is important for the profes- sional worker to accept and understand the purposes and objectives of the program which prepared the worker. Without the support of the medical and nursing staffs, a course for training of operating room techni- cians would have little chance of succeeding. The cooperation and participation of nurses
and surgeons is needed in each clinical situa- tion, since clinical practice occupies much of the student’s time.
The nursing faculty should be assured that such a technician’s program will not interfere with the professional student pro- gram in the operating room. At our hospital, we have been very fortunate in being able to mesh these two programs without con- flict, and still give each group effective ex- perience and education.
To briefly sum up our experience: on the negative side, our dropout rate seems high compared to the Worcester and Sacramento1 programs. The stipend which we pay, roughly $2,000 for the year, is adequate only for the student who lives at home. More adequate testing might seem necessary in order to weed out the intellectual and temperamental misfits.
On the positive side, we have had about 20 years of employment from our 15 tech- nicians in the past seven years, exclusive of training time, The students whom we have trained seem able to function successfully as technicians in the operating room, both in our hospital and in the neighboring hospitals in the city.
From talking with colleagues and dis- cussing the various programs which we have investigated or read about, we have come to the conclusion that the ideal program would be similar in set up to the Worcester or Sacramento courses. In these, a central public school takes the responsibility for teaching the theoretical material to a large number of students, and several hospitals participate in giving a limited number of students the clinical practice required. We believe this ought to be controlled by the State Department of Education, with careful screening of the participating hospitals. With this type of program it might be possible to secure Manpower funds and/or grants to finance the entire program.
Long, careful consideration should be
Jan-Feb 1966 69

given if one contemplates setting up a pro- gram to teach surgical technicians. The cost of such a program is high. There are the direct costs of instructors’ salaries, stipends paid to the students, texts, films, uniforms and laundry. There are also indirect costs which are difficult to compute, such as re- cruitment, and time of the graduate staff spent in helping to teach these students.
The mistakes of others should be recog- nized and used profitably. One should avoid training a student who can funotion only in a selected hospital, or worse still, one who functions mechanically, without the neces- sary background knowledge to act intelli- gently.
The success of others should be used to best advantage so that the most effective programs can be set up in those institutions desiring to conduct them.
In preparing technicians, we mud think beyond the needs of our individual situa- tions and current practices to anticipate the future, so that those who graduate today will be eligible for registration or licensure, if and when this becomes necessary.
REFERENCES
1. Worcester program conducted at the David Hale Fanning Trade High School and St. Vincent’s Hospi- tal in Worcester, Massachusetts. Sacramento program conducted by the Sacramento City College and the Sutter Community Hospitals in Sacramento, Cali- fornia. 2. Keaveney, Marie Helen, “Responsibilities of Im- plementing a Surgical Technical Aide Program,” AORN Journal, Vol. 2, # 3 , 1964, pp. 51-58. 3. Peers, Jerry G., “Today’s Challenge to the Pro- fessional Operating Room Nurse,” AORN Journal,
4. Surgical Technical Aide Instructor’s Manual, American Hospital Association, Chicago, 1954. 5. Visintainer, Lena; Wood, Rae Pittiman; Sunder- land, Della and Burnside, Frances, “Training the Surgical Technician,” O.R. Nursing, Vol. 2, # 5 ,
Vol. 2, #1. 1964, pp. 69-13.
1961, pp. 31-84.
70 AORN Journal





























