-
7/30/2019 Abdullah 333
1/9
ADVNCED CYTOPATHOLOGY
MEDS2135Case study 3: Non-Gynae
Coordinator: Karin Bradshaw
Student Name: Abdullah Bandar Almutiri
Student Number: 3276950
Date Submitted: 14/05/2013
-
7/30/2019 Abdullah 333
2/9
Student Name: Abdullah Bandar Almutiri, Student Number: 3276950
Page 2
Introduction
The cytology laboratory is considered as one of the most
important tool to help in diagnosis of
many diseases. Many ancillary tests work as complementary to get
a final diagnosis. In this case
study of 64 years old female, Respiratory cytology is used to
get the precise diagnosis. Which is the
study of the cells that exfoliate within the respiratory tract
whether they are originating from
respiratory system or they belong to a tumor that metastasis to
the lung or other parts of the
respiratory tract.
The use of endoscope to sample cells from the lower portion of
respiratory tract lead to an
improvement in the result that can be obtained compared to the
conventional sputum sample (4).
Bronchial wash is mainly dependent on the use of a bronchoscope
through washing the mucosa by
saline and consequent aspirate of that saline which contains the
cells that can be centrifuged and
smeared into the slide. By examining the wash return fluid, the
doctor can identify any
abnormality such as bleeding, fungal infections and different
kinds of lung tumor. Patients
undergoing bronchial washing usually have mild side effects
which include coughing, sore throat
and a sleepy feeling from being sedated (4, 8).
Case Report
CLINICAL DETAILS
Type of specimen: Bronchial washing.
Age: 64 years old.
Gender: Female.
Clinical notes: The patient has a mass in the upper right lobe
of the lung.
Material and Method
The specimen collected from the upper right lobe of the lung by
using bronchoscopetechnique.
Bronchial washing or bronchoscopy is a procedure used to
investigate diseases in the lung.During the procedure, the patient
is injected with saline into the lung through a fiberoptic
bronchoscope (4). The bronchial wash then sucked out and sent to
the cytology laboratory
for the investigation. Bronchial washings are easily obtained
and are useful in diagnosis of
many respiratory diseases including the centrally located
lesions, but in bronchial washing
the cytology must prepare the smear without any delay because
the cells in the saline can
undergo degenerative changes.
One slide was reserved for screening any abnormality.
-
7/30/2019 Abdullah 333
3/9
Student Name: Abdullah Bandar Almutiri, Student Number: 3276950
Page 3
CASE DESCRIPTION
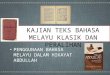
Microscopic description:
The smear of bronchial washing is satisfactory, because at low
power the smear ishypercellular and containing crowded branching
groups Cells present in acinar groups. Thesmears show abundant
ciliated bronchial cells in significant numbers. Macrophages
and
red blood cell present. The background of the slide is mucoid
(Figure 1A, 1B).
Bronchial cells (ciliated bronchial cells) are seen in
significant numbers in bronchialwashing specimens. Columnar shaped
cells with cytoplasmic tail present singly and in
loosely cohesive groups, basally located nucleus, Round / oval
nuclei, Smooth, fire to mildly
coarse dark chromatin, Nucleoli is also seen (Figure 1B).
Macrophages have round shaped nuclei which are centric or
eccentric, finely granularchromatin; some have more nuclei and
other bi nuclei, foamy cytoplasm (Figure 1C).
Squamous cells present in very few numbers which reflect
contamination from the upperrespiratory tract in sputum or
bronchial washings. Predominately superficial squamous
cells (Figure 1D).
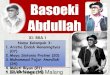
Small cell carcinoma:
Small cells presents singly and in groups lined up with scant to
absent cytoplasm (Figure2A, 2B).
Nuclear molding is prominent, which is feature of small cell
carcinoma (Figure 2C, 2D).
A high N\C ratio. Small cell nuclear staining ranges from dark
to pale. Hyperchromatic, Nucleoli is invisible
(Figure 2A, 2D).
In the cropped image of C (Figure 2D) it show elongated
groupings of small cell with Scantcytoplasm or absent cytoplasm and
irregular moulded nuclei; dark chromatin,
inconspicuous nucleoli; very high N\C ratios.
-
7/30/2019 Abdullah 333
4/9
Student Name: Abdullah Bandar Almutiri, Student Number: 3276950
Page 4
Figure 1. A At low power the smear is hypercellular and
containing crowded branching groups
Cells with mucoid background Pap stain x20. B Shows bronchial
cells with cilia Pap stain x20. C
Macrophages and other material are present in the background Pap
stain x20. D Squamous cells
present in very few numbers Pap stain x20.
A B
C D
-
7/30/2019 Abdullah 333
5/9
Student Name: Abdullah Bandar Almutiri, Student Number: 3276950
Page 5
Figure 2. A Small cell carcinoma presents singly and in groups
Pap stains x40. B small cell
carcinoma seen in a linear Pap stain x20. C The molding of
nuclei around each other; which is
feature of small cell carcinoma Pap stain x40. D cropped image
of C to show the molding, PAP
stain.
A B
C D
-
7/30/2019 Abdullah 333
6/9
Student Name: Abdullah Bandar Almutiri, Student Number: 3276950
Page 6
DIAGNOSIS AND RECOMMENDATION
Diagnosis: Bronchial washing/ Malignant cells present (Small
cell carcinoma).
Recommendation: Referralfor oncologist; chemotherapy or
combination chemotherapy with
concurrent chest radiotherapy (RT) for treatment (9, 10).
DISCUSSIONSmall-cell carcinoma
Small cell lung cancer (SCLC) is a malignantcancer which is most
commonly arises inside the lung,
commonly called Small cell carcinoma. This tumor usually occurs
centrally and metastasizes very
early to the hilary lymph nodes, bones, brain, and liver. Also
it can infrequently happen in otherbody sites, like for example the
gastrointestinal tract and prostate in man. When SCLC infects
the
lung, it is sometimes called "oat cell carcinoma" due to the
scanty cytoplasm and flat cell shape (6).
In the cytology definition of the small cell carcinoma
characteristics is small cells with finely
granular nuclear chromatin and not easily seen nucleoli, scant
cytoplasm. There are a high mitotic
count and nuclear molding (7).
Small cell carcinomas are smaller than normal cells, and the
primary stage of this cancer is too
difficult to diagnose because the cell is too small and
difficult to find. Small cell carcinoma belongs
to a group of tumors know as (bronchial neuroendocrine tumors).
As they arise from
neuroendocrine cells in the bronchus. Neuroendocrine cells found
throughout the body and they
release hormones when they stimulate by neural stimulus (1, 6).
Pulmonary neuroendocrine cells
involved in the regulation of oxygen levels. By detecting
increase oxygen or increased carbon
dioxide levels and sending chemical message to help the lung
adjust to these changes. The people
who living at high altitudes, where oxygen levels are lower,
have a higher number of
neuroendocrine cells in their lungs.
The main cause of small cell cancer is tobacco smoking and the
majority of patients how infected
have strong smoking history of all histological types of lung
cancer, Squamous cell carcinoma and
SCLC have the strongest relationship to tobacco. Approximately
98% of patients with SCLC have a
smoking history. Patients with SCLC should be encouraged to stop
smoking, as smoking cessation
is associated with improved survival (6).
http://en.wikipedia.org/wiki/Malignanthttp://en.wikipedia.org/wiki/Cancerhttp://en.wikipedia.org/wiki/Lunghttp://en.wikipedia.org/wiki/Prostatehttp://en.wikipedia.org/wiki/Cytoplasmhttp://en.wikipedia.org/wiki/Cytoplasmhttp://en.wikipedia.org/wiki/Prostatehttp://en.wikipedia.org/wiki/Lunghttp://en.wikipedia.org/wiki/Cancerhttp://en.wikipedia.org/wiki/Malignant
-
7/30/2019 Abdullah 333
7/9
Student Name: Abdullah Bandar Almutiri, Student Number: 3276950
Page 7
DIFFRENTIAL DIAGNOSIS
Problems in diagnosis are to differentia between small cell and
poorly differentiated non-small
cell carcinomas and a tendency to include tumors with larger
than expected nuclei in the non-small cell category. In general, if
the nuclear features of a problematical tumor are those of
small
cell carcinoma- that is, granular chromatin without prominent
nucleoli- the neoplasm will fall into
the small cell carcinoma group Histologically; vesicular nuclei
with prominent nucleoli would
generally be evidence of non-small cell tumor. Also,
immunocytochemistry is also helpful in
differentiating between non- small cell lung cancer and small
cell; small cell carcinomas are
reactive with CD 56, and other neurondocrine markers, whereas
non-small cell carcinomas are
generally unreactive(2, 3).
In addition, it is sometimes very difficult to distinguish small
cell carcinoma from lymphomas,particularly those of follicular
center cell origin with pronounced cell polymorphism and
nuclear
irregularity. Cell dispersal together with a rim or tail of
intact cytoplasm in individual cells and a
background of round, cytoplasmic fragments staining blue with
MGG (lymphoid globules\ lymph
glandular bodies) are helpful features in making a diagnosis of
lymphoma. Dispersed cells of small
cell carcinoma are usually bare nuclei. Some low-grade lymphomas
can show pseudomoulding
due to clustering of the nuclei. However, significant true
nuclear moulding is not seen in
lymphoma and cytoplasm is usually maintain while, small cell
carcinoma usually do not maintain
cytoplasm (2, 9).
Furthermore, Reserve cell hyperplasia. Reserve cells are rarely
seen except in reactive states. They
are small in size (compare the size with adjacent columnar
cell), have hyperchromatic nuclei, and
may show evidence of nuclear molding. It is important not to
confuse them with small cell
carcinoma.
TREATMENT and PROGNOSIS
Treatment
Treatment options depend on factors such as stage of the cancer,
the position of the tumor, andpatients fitness to tolerate the
therapy. There are two stages of small cell carcinoma that is
usually
determined by the presence or absence of metastases which are
extensive stage (ES) and
including limited stage (LS). In cases of LS-small cell
carcinoma, combination chemotherapy is
administered together with concurrent chest radiotherapy (RT)
for treatment.
Generally, Small cell carcinoma spreads very quickly throughout
out the body and patients do not
benefit from surgery. Chemotherapy is the main treatment is
given to patients with extensive
disease, to prolong their life and relieve their symptoms (5,
10).
-
7/30/2019 Abdullah 333
8/9
Student Name: Abdullah Bandar Almutiri, Student Number: 3276950
Page 8
Prognosis
Lung cancer has one of the worst survival outcomes of any
cancer. The outcome is dependent on
the stage and type of lung cancer. Overall, for all types of
lung cancers irrespective of the stage atthe time when the cancer
is diagnosis, only 25% of patients will live for one year and 8%
will live
for five years. For small cell lung cancer the Surviving for
five years is 1% for stage 4. Indicators of
poor diagnosis include relapsed disease, weight loss, and poor
performance status (5, 10). For all
patients with SCLC, activity should be encouraged and a dietary
consultation should be obtained.
SUMMARY
The patient is 64 years old, Female that has a mass in the upper
right lobe of the lung the specimen
collected by using bronchoscope technique. One slide was
reserved for screening any abnormality.
This case is reported as Malignant cells present (Small cell
carcinoma) as there is indication of
abnormality. Chemotherapy is the main treatment for this patient
when considering his age as
well, to prolong their life and relieve their symptoms.
Small cell carcinoma is highly aggressive as it usually
characterized by aggressive actions, fast
growth, early spread to other sites in the body organs,
exquisite sensitivity to chemotherapy and
radiation the survival rate is always low. Therefore advice to
avoid the risk factors for
development of disease such as smoking because smoking is the
main cause of lung cancer, the
only means of decreasing the occurrence of this disease as well
as that of small cell carcinoma
specifically, is to decrease the occurrence of smoking.
Furthermore, development of highly advanced early diagnostic
facilities and increase public
awareness of the effects of smoking should be the main primary
concern of medical centers and
government.
-
7/30/2019 Abdullah 333
9/9
Student Name: Abdullah Bandar Almutiri, Student Number: 3276950
Page 9
REFERENCES
1. Stuff.com. c. Gyn Atlas Section 4c. Copyright 2013 Hologic,
Inc. All Rights Reserved; 2013;Available
from:http://www.cytologystuff.com/study/section4c.htm#squamous.
2. Ducztman BSD, Edmund S. Cibas. Cytology Diagnostic Principle
and Clinical Correlates.Saunders: Linda Belfus; 2009.
3. Marluce Bibbo DW. Comprehensive Cytopathology.
SAUNDERS2008.4. Collins W. Bronchial Washing Procedures. 2013;
Available from:
http://www.livestrong.com/article/161434-bronchial-washing-procedures/.
5. Austin JHM, Yip R, D'Souza BM, Yankelevitz DF, Henschke CI.
Small-cell carcinoma of the lungdetected by CT screening: Stage
distribution and curability. Lung Cancer. 2012;76(3):339-43.
6. Behded Shambayati. CYTOPATHOLOGY. United States: Oxford
University Press; 2011.7. DeMay RM. The pap test: Chicago : ASCP
Press c2005 .8. Fernndez-Villar A, Gonzlez A, Leiro V, Represas C,
Isabel Botana M, Blanco P, et al. Effect of
Different Bronchial Washing Sequences on Diagnostic Yield in
Endoscopically Visible Lung
Cancer. Archivos de Bronconeumologa ((English Edition)).
2006;42(6):278-82.
9. Kocjan WGWG. Diagnostic cytopathology. 3rd ed: Edinburgh :
Churchill Livingstone/Elsevier;2010.
10.Sun J-M, Ahn M-J, Ahn JS, Um S-W, Kim H, Kim HK, et al.
Chemotherapy for pulmonary large cellneuroendocrine carcinoma:
Similar to that for small cell lung cancer or non-small cell
lung
cancer? Lung Cancer. 2012;77(2):365-70.
http://www.cytologystuff.com/study/section4c.htm#squamoushttp://www.cytologystuff.com/study/section4c.htm#squamoushttp://www.livestrong.com/article/161434-bronchial-washing-procedures/http://www.livestrong.com/article/161434-bronchial-washing-procedures/http://www.livestrong.com/article/161434-bronchial-washing-procedures/http://www.cytologystuff.com/study/section4c.htm#squamous