Embed Size (px)
Citation preview

CASE REPORT
Absence of supra-renal inferior vena cava: case reportAusência de veia cava inferior suprarrenal: relato de caso
Elton Correia Alves1, Gabriela Bóia Rocha Ferro1, Luciana Karla Lira França1, Mabel Batista Jacó1, Guilherme Benjamin Brandão Pitta2
Introduction
Inferior vena cava (IVC) is a large-caliber vessel that drains blood from the lower limbs, from most of the trunk, besides abdominal and pelvic organs. It is formed by the junction of the common iliac veins and lies right of the ab-dominal aorta, draining into the right atrium. The azygous system connects the superior and inferior venae cavae di-rectly or indirectly1,2. Congenital absence of IVC is an oc-casional finding in imaging exams. Because most patients without other malformations are asymptomatic, it is diffi-cult to estimate the prevalence of such anomaly.
Case report
A 28-year-old male patient was admitted to the Hospital São Sebastião, Maceió (AL), Brazil, with high fever (39oC), not responding to medication, being referred for radiogra-phy of the sinus cavities and chest. He had no relevant past medical history. Chest radiography was suggestive of azygous vein dilatation. The fever came down spontaneously after a week, and no infection or other cause was found. After hos-pital discharge, he was referred to an angiologist in order to investigate the chest radiograph finding. At the Clínica de Especialidades (MedAngio), the patient reported chest pain
Abstract
The congenital absence of the inferior vena cava is a rare and occasional finding at complementary exams or abdominal surgeries. As the majority of patients without other malformations are asymptomatic, it is hard to estimate the prevalence of these anomalies. Our goal was to report a case of a 28-year-old patient, male, referred to thorax X-ray due to high fever state (39ºC), nonresponder to medication. The X-ray suggested azygos vein dilatation. The interview about cardiovascular symptoms revealed thoracic pain during both physical exercises and at rest, and occasional dyspnea during sleep related to the period of intensification of physical exercises. Computadorized tomography with and without contrast did not solve the case, what explain the request of an angiotomography, that showed absence of thoracic inferior vena cava.
Keywords: Vena cava, inferior/abnormalities; azygos vein/abnormalities; venous thrombosis/etiology.
Resumo
A ausência congênita de veia cava inferior é achado incomum e ocasional durante exames complementares ou cirurgias do abdome. Em razão de a maioria dos pacientes sem outras malformações serem assintomáticos, há dificuldade em estimar a prevalência dessas anomalias. O objetivo deste trabalho foi relatar o caso de um paciente de 28 anos, sexo masculino, referido para radiografia de tórax devido a quadro de febre alta (39ºC) não-responsiva à medicação. Radiografia de tórax sugeriu dilatação de veia ázigos. Em inquérito dirigido para sintomas cardiovasculares, referiu dor torácica (durante atividade física e em repouso) e dispneia ocasionais durante o sono associada ao período em que intensificou a prática de exercícios. Realizada tomografia computadorizada sem contraste e, posteriormente, contrastada. As mesmas não esclareceram o caso, fazendo-se necessário angiotomografia, a qual evidenciou ausência de veia cava inferior torácica.
Palavras-chave: Veia cava inferior/anormalidades; veia ázigos/anormalidades; trombose venosa/etiologia.
Study carried out at Clínica de Especialidades (MedAngio), Maceió (AL), Brazil.1 Medical Students (5th period) at Universidade Federal de Alagoas (UFAL), Maceió (AL), Brazil.2 Adjunct Professor at Universidade Estadual de Ciências de Saúde de Alagoas (Uncisal), Maceió (AL), Brazil.No conflict of interest was declared concerning the publication of this article.Received on: Oct 26, 2009. Accepted on: Jun 1, 2010.J Vasc Bras. 2010;9(4):254-256.

Supra-renal inferior vena cava anomaly - Alves EC et al J Vasc Bras 2010, Vol. 9, Nº 4 255
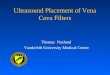
at exercise and at rest, and occasional dyspnea associated with a period of intense physical exercise. Computed tomo-graphy (CT scan), first performed without a contrast agent and, later on, with a contrast agent, was inconclusive. Spiral CT angiography was indicated and showed:1) continuous IVC azygous (Figure 1); 2) no aneurysms or thrombi; 3) retroaortic renal vein.
The patient was then oriented to discontinue heavy physical activities due to the high risk of venous thrombo-sis. He has been asymptomatic for six months.
Discussion
The IVC is formed between the sixth and eighth we-eks of embryonic life in a complex process involving three primitive vein pairs (posterior cardinal, subcardinal and supracardinal veins), which are extensively anastomosed. Such anastomosis recede during the embryologic process, thus originating the IVC3,4. When abnormalities occur du-ring this development, anomalies of IVC such as partial or total agenesis, may occur3-5. The azygous system tends to dilate as a compensatory mechanism.
As these anomalies may be asymptomatic, their fre-quency is hard to measure. However, their prevalence in the
general population is estimated to be 0.5%6. About 90% of the cases are related to partial absence of the supra-hepatic segment of the IVC4. Total absence of the renal and supra-renal IVC segments is very rare.
IVC anomalies may be accompanied by vascular, car-diac, bowel, portal and liver malformations, and polyes-plenia4. Most cases are asymptomatic and occasionally found by routine exams not related to the malformation. However, in case of insufficiency of collateral veins, blood drainage from the lower limbs and pelvis becomes inadequate, causing venous stasis and a predisposition to venous thrombosis7. Bilateral and recurrent deep vein thrombosis (DVT) in the proximal vein of young pa-tients without history of coagulopathies may imply IVC anomaly, so imaging methods are required. About 5 to 7% of the patients with DVT present some IVC anomaly; the incidence is higher in young patients and those with bilateral DVT6.
There is no indication for interventional treatment in case of partial IVC absence. However, knowing this entity is important in order to avoid unnecessary surgi-cal procedures. Since this condition may predispose the patient to DVT, some authors recommend anticoagulant therapy, but this is no consensus4. In the present case, oral anticoagulation therapy and thrombophilia inves-tigation were not necessary because the patient had an
Figure 1 – (A) Abdominal inferior vena cava; (B) IVC with azygous continuation; (C) azygous vein; (D) cava-azygous transition; (E) azygous vein; (F) hemiazygous vein; (G) azygous vein draining into the right atrium.

Supra-renal inferior vena cava anomaly - Alves EC et alJ Vasc Bras 2010, Vol. 9, Nº 4256
anatomical congenital alteration, not an acquired func-tional one; the only recommendation was to restrict heavy physical activities. Anticoagulant therapy is qui-te expensive for the patients and, when the disease can be controlled with behavioral measures, patients accept the treatment more easily, besides having their quality of life improved. The patient has been followed for one year and has been asymptomatic, under the cardiovascular point of view.
References
1. Gardner E, Gray DJ, O’rahilly R. Anatomia. 4. ed. Rio de Janeiro: Guanabara Koogan; 1978.
2. Moore K, Dalley AS. Anatomia orientada para a clínica. 4. ed. Rio de Janeiro: Guanabara Koogan; 2001.
3. Viana SL, Mendonça JLF, Freitas FMO, et al. Hipoplasia da veia cava inferior: relato de caso e revisão da literatura. Revista Imagem. 2006;28:203-7.
4. Felicio ML, Martins AS, Andrade RR, et al. Ausência parcial de veia cava inferior associada à malformação intestinal. Revista Brasileira de Cirurgia Cardiovascular. 2007;22:362-4.
5. Lichtenfels E, Becker AS, Pires VC, et al. Diagnóstico etiológico da trombose venosa profunda de repetição dos membros inferiores. Jornal Vascular Brasileiro. 2006;5:157-9.
6. Onzi RR, Costa LF, Angnes RF, et al. Malformação de veia cava in-ferior e trombose venosa profunda: fator de risco de trombose venosa em jovens. Jornal Vascular Brasileiro. 2007;6:186-9.
7. Obernosterer A, Aschauer M, Schnedl W, et al. Anomalies of the inferior vena cava in patients with iliac venous thrombosis. Ann Intern Med. 2002;136:37-41.
Correspondence:Guilherme Benjamin Brandão Pitta
Rua Desportista Humberto Guimarães, 1.081/702 – Ponta Verde CEP 57035-030 – Maceió (AL), Brazil E-mail: [email protected]
Authors’ contributions
Study conception and design: ECA Data analysis and interpretation: ECA, LKLF and GBBP
Data collection: GBRF, ECA and MBJ Writing: LKLF, MBJ, ECA and GBRF
Critical analysis: GBRF and GBBP Final text approval*: ECA, GBRF, LKLF, MBJ, GBBP
Statistical analysis: MBJ Overall responsibility: GBBP
Financing information: N/I *All authors have read and approved the final version of the paper submitted
to the J Vasc Bras.