Embed Size (px)
Citation preview
Nursing and Health Sciences
(2003),
5
, 219–228
Blackwell Science, LtdOxford, UKNHSNursing and Health Sciences1441-07452003 Blackwell Publishing Asia Pty LtdSeptember 200353219228Research Article
Guidelines in nursing educationM. Jerlock
et al.
Correspondence address: Margaretha Jerlock, Lerskäddegatan 52 A,SE-426 58 V. Frölunda, Sweden. Email: [email protected] 17 December 2002; accepted 20 February 2003.
Research Article
Academic nursing education guidelines: Tool for bridging the gap between theory, research and practice
Margaretha Jerlock,
rn, rnt, ms
c
,
1
Kristin Falk,
rn, rnt, ms
c
1
and Elisabeth Severinsson,
rpn, rnt, ms
c
, p
h
d
2
1
Sahlgrenska Academy at Göteborg University, Faculty of Health and Caring Science, Institute of Nursing, Göteborg, Sweden and
2
Faculty of Health Studies, Hedmark University College and Institute of Nursing Science, University of Oslo, Oslo, Norway
Abstract
The aim of the present study was to develop educational guidelines to be used as a tool for the inte-gration of theory, research and practice to ensure that nursing knowledge and practical skills formthe basis of academic nursing education. An additional aim was to describe the nursing competenceexpected of the students at four academic levels: introductory, intermediate and advanced levels Iand II. Clinical nursing education plays a crucial role in assisting nursing students to integrate thetheory and practice of nursing at the baccalaureate level, as well as in further specialization and in-depth nursing studies at the advanced level. A research group consisting of lecturers from the Insti-tute of Nursing, Göteborg University, Sweden, was given the objective to formulate educationalguidelines for clinical practice within nursing education. The study took the form of a literaturesearch. In addition, the Delphi method, aimed at reaching a consensus of opinion among col-leagues, was used. Based on the literature review and the collegial discussions, four core conceptsemerged: professional stance, reflective processes, problem-solving processes, and practical skills,from which the educational guidelines were developed. Guidelines were formulated both in gen-eral and abstract form. They were not connected to a specific care context, specific patient groupor specific nursing problems. The most important objective of academic education is that the stu-dent develops abilities and techniques necessary for life-long learning. Students will, in their pro-fessional life as nurses, continuously meet situations where they are challenged to take appropriatedecisions and actions. This demands training in problem-solving, reflection, decision-making andthe ability to use both deductive and inductive learning strategies. The guidelines describe what isexpected of the students in terms of nursing competence and personal qualifications to ensure thatthey will be ready to meet the demands of their future profession.
Key words
clinical nursing education, decision-making, guidelines, practical skills, problem-solving, profes-sional stance, reflection.
INTRODUCTION
Clinical nursing education (CNE) plays a crucial rolein assisting nursing students to integrate theory,research and nursing practice, which is required for thebachelor’s degree as well as for further specializationand in-depth studies in advanced nursing. Teaching and
learning in academic nursing education demands fur-ther development of the learning environment in clin-ical settings, including cooperation between the nursesupervisor and the faculty concerned, in order to sup-port the student in the learning process.
In Sweden, during the last few decades nursing edu-cation has undergone radical changes regarding orga-nization, objectives, content and teaching methods. Inthis regard, one of the most important political deci-sions was the governmental reform of higher educa-tion for paramedical professions in 1977 whichelevated the nursing program to the higher education

220 M. Jerlock
et al.
level, to be organized in colleges of health sciences.Twenty years later, the nursing program in Swedenwas integrated into universities, and the awarding ofbachelor, master and doctoral degrees in nursing wasauthorized. The history of nursing education in Swe-den has primarily followed the international (e.g.USA) trend for curriculum development, from a prac-tical, via a technical, behavioral objective, to an aca-demic-based curriculum (Bevis, 1988). During thistime, the education of nurses has developed from anapprentice-training program to an academic educa-tion, which includes scientifically-based theoreticaland clinical courses (The Higher Education Ordi-nance, 1993). It has been a great challenge for theInstitute of Nursing to construct a clinical curriculumbased on academic tradition and scientific knowledgecombined with task-oriented training and practicalknow-how. Cognitive development worth striving foris not just rational, logical or intellectual thinking. It isalso a question of how students reflect on issues, howthey consider different viewpoints, their ability toorganize knowledge and experience, as well as howthey tolerate ambiguity and conflicting information(Valiga, 1988). One major prerequisite for such profes-sional cognitive development is the combination andintegration of clinical and theoretical studies (Schön,1987). The clinical part of nursing education at theInstitute of Nursing, Göteborg University, is built ontwo basic assumptions: (i) real-time situations consti-tute the basis for training and learning. The students’activities in nursing practice are based on knowledgefrom a multiplicity of theories from different scientificfields, integrated with personal and evidence-basedexperience. In that sense, the educational strategy is
inductive
. (ii) Students’ theoretical knowledge consti-tutes the basis for learning because it prepares them tofocus on specific nursing situations and helps them toobtain different perspectives on the reality of caring.In this sense, the educational strategy is
deductive
.The dialectic relation between these two learning
approaches constitutes the integration of theory andpractice, where the students have the opportunity toidentify, reflect and solve problems. In combinationwith a flexible learning environment, this permits thestudents to develop creativity, intuition and originalsolutions in accordance with academic education stan-dards (Bowden & Marton, 1998).
The Higher Education Ordinance (1993) sets out therequirements for a bachelor’s or master’s degree. Onecondition for a bachelor’s degree is that the main sub-ject can be identified in courses at introductory, inter-mediate and advanced level I and, for a master’sdegree, at advanced level II. There is a tradition inSwedish universities of organizing the main theoretical
subject courses at these four levels, but there is lessexperience in systematizing practical training courses.However, the challenge is to combine the traditionalway of systematizing theoretical major subjects with aclinically-based multidisciplinary content, and to for-mulate educational guidelines pertaining to these dif-ferent levels of required professional competence.Therefore, the present study was established with theaim of developing educational guidelines, based onnursing knowledge, nursing experience and practicalskills.
AIM
The aim of the current study was to develop educa-tional guidelines as a tool for the integration of theory,research and practice in order to create an academicnursing education based on nursing knowledge, nursingexperience and practical skills. An additional aim wasto describe what is expected of students in terms ofnursing competence at four academic levels: introduc-tory, intermediate and advanced levels I and II.
ISSUES
The main research issues addressed in this study were:• How can the CNE guidelines be described at
four academic levels: introductory, intermediate andadvanced levels I and II?
• In what way can educational guidelines facilitatethe integration of theory, research and practice?
THEORETICAL BACKGROUND
Clinical guidelines
Clinical guidelines underpinned by scientific evidencehave been developed to support the implementation ofevidence-based practice. The guidelines combine thebest external and internal evidence necessary for deci-sion-making in nursing (Sacket
et al
., 1997). Guidelinesare not rules or goals but should be an adjunct in sup-porting the decision-making process in nursing practice(Mead, 2000). In nursing education, the learning anddecision-making processes are the focus, and educa-tional guidelines are aimed at supporting these pro-cesses. The pedagogical contributions from the facultyand the nurse supervisors in clinical settings are aimedat supporting the student in operationalizing and indi-vidualizing the guidelines in relation to each student’sprevious experience and knowledge. Practical knowl-edge is developed through critical reflection and prob-lem-solving in close consultation with the patient andincludes, besides theoretical knowledge, empathy and

Guidelines in nursing education 221
moral sensitivity (cf. Schön, 1987; Rolf, 1991; Lützén,1993).
Decision-making
Nursing education is both theoretical and practical.The student has the opportunity to apply theoreticalknowledge to practical situations in the clinical part oftheir education. The final goal is a confident student,capable of independently making decisions and per-forming nursing activities towards patients, relativesand other health professionals. Decision-making is acomplex process in which both individual and envi-ronmental factors play important roles in terms ofoutcome. Closs and Cheater (1999) stated that inter-play between multiple factors, such as amalgamationof evidence, context, experience and patient prefer-ences/wishes, influences decisions in patient care.Nurses carry out a variety of activities to obtain,recover and develop the patient’s health and well-being. In order to attain these goals, actions should bepreceded by clinical decision-making built on rationalthought and moral judgment. According to this per-spective, nursing is not only technical but also moral,and the student has to learn how decision-making isverbalized and expressed within the nurse-patientrelationship (Harbison, 2001). According to Long andHarrison (1997), evidence-based nursing is the ‘pro-cess of systematically finding, appraising and usingcontemporaneous research findings as the bases forclinical decisions’ (p. 2). To make well-grounded deci-sions and deliver evidence-based nursing, the studentnurse must develop cognitive and emotional knowl-edge, technical skills and be able to apply this knowl-edge in the delivery of skilled practices (McSherry &Proctor-Childs, 2001). The nature of decision-makingis therefore related to the student’s knowledge, expe-rience and degree of independence in relation to thecomplexity of the situation and the learning environ-ment. Context naturally influences the decision-making process. In acute situations, the student has tomake clinical judgments which involve triage within ashort space of time, while decision-making related tochronic conditions often has to be built on multipleconsiderations and requires creativity and flexibility(Cioffi, 1999; Watt, 2000). The unique patient and sit-uation require reflection and problem-solving tech-niques to underpin decision-making in relation tonursing activities. An excellent nurse is oftendescribed as a person who makes appropriate deci-sions in relation to the specific situation and who car-ries out the required activities. Rolf’s (1991)discussion about competence confirms this statement.
He describes competence as the ability to create con-ditions in a practical situation, where theoretical andpractical knowledge and experiences are integratedand become apparent through intellectual and practi-cal actions.
Educational guidelines can be used by the student asa tool for bridging theory, research and practice as wellas a starting point for reflection. This, in turn, couldpromote the decision-making process, thus leading tothe development of nursing competence.
Clinical nursing supervision
Transformation of theory into practice by adopting aclinical supervision approach may support the stu-dent’s decision-making and clinical judgment innursing practice (Berggren & Severinsson, 2000).The effectiveness of implementing clinical nursingsupervision ultimately depends on the supervisor’scompetence as well as the nursing student’s motiva-tion and ability to integrate knowledge and makeuse of new information relevant to the resolution ofclinical problems. In addition, the way in whichnursing students integrate new information withexisting knowledge and generate hypotheses thatwill solve the problems at hand is of great impor-tance. Clinical supervision is aimed at influencingstudents’ learning processes in a positive way and atpromoting and implementing the decision-makingprocess in nursing.
The primary goal of clinical nursing supervision isto support the development of the supervisee’s jobidentity, competence, skills and ethics (Severinsson,2001). This development of self-understanding andintegration of theory is confirmed by Holm
et al
.(1998) who emphasize the importance of clinicalsupervision in the development of nursing studentsinto professional nurses. In addition, it has beenreported that it is possible, by means of clinicalsupervision, to guide the ethical development andmaturation of nursing students (Nylund & Lind-holm, 1999). Clinical supervision enhances nurses’ability to provide care and forms the basis of theirdecision-making. This is in line with Bégat and Sev-erinsson (2001), who reported that in supervision,nurses reflected on episodes occurring during theirprovision of care. Reflection was reported to beone way of bridging the gap between theory andpractice and demonstrated the need for an innova-tive approach to the provision of quality learning inclinical institutions. Moreover, Holm
et al
. (1998)found that continuous process-oriented group super-vision increased nursing students’ attentiveness,
222 M. Jerlock
et al.
empathy and insight towards patients as well asproviding them with feelings of security in theirrole as nurses.
Examination
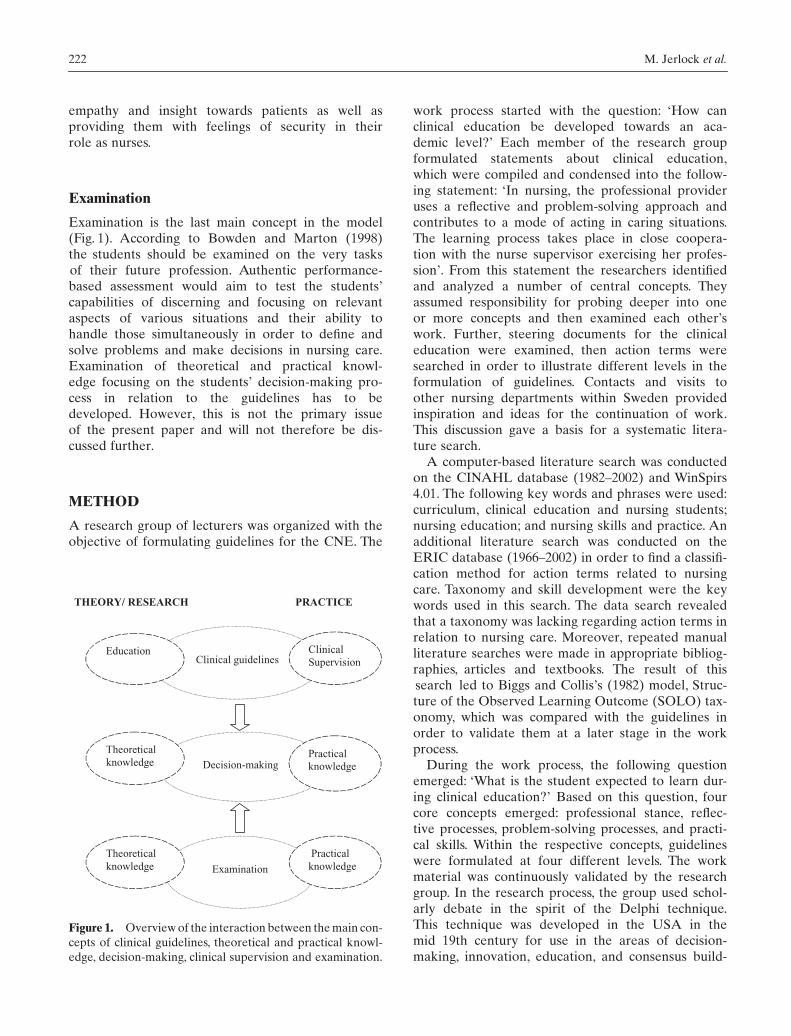
Examination is the last main concept in the model(Fig. 1). According to Bowden and Marton (1998)the students should be examined on the very tasksof their future profession. Authentic performance-based assessment would aim to test the students’capabilities of discerning and focusing on relevantaspects of various situations and their ability tohandle those simultaneously in order to define andsolve problems and make decisions in nursing care.Examination of theoretical and practical knowl-edge focusing on the students’ decision-making pro-cess in relation to the guidelines has to bedeveloped. However, this is not the primary issueof the present paper and will not therefore be dis-cussed further.
METHOD
A research group of lecturers was organized with theobjective of formulating guidelines for the CNE. The
work process started with the question: ‘How canclinical education be developed towards an aca-demic level?’ Each member of the research groupformulated statements about clinical education,which were compiled and condensed into the follow-ing statement: ‘In nursing, the professional provideruses a reflective and problem-solving approach andcontributes to a mode of acting in caring situations.The learning process takes place in close coopera-tion with the nurse supervisor exercising her profes-sion’. From this statement the researchers identifiedand analyzed a number of central concepts. Theyassumed responsibility for probing deeper into oneor more concepts and then examined each other’swork. Further, steering documents for the clinicaleducation were examined, then action terms weresearched in order to illustrate different levels in theformulation of guidelines. Contacts and visits toother nursing departments within Sweden providedinspiration and ideas for the continuation of work.This discussion gave a basis for a systematic litera-ture search.
A computer-based literature search was conductedon the CINAHL database (1982–2002) and WinSpirs4.01. The following key words and phrases were used:curriculum, clinical education and nursing students;nursing education; and nursing skills and practice. Anadditional literature search was conducted on theERIC database (1966–2002) in order to find a classifi-cation method for action terms related to nursingcare. Taxonomy and skill development were the keywords used in this search. The data search revealedthat a taxonomy was lacking regarding action terms inrelation to nursing care. Moreover, repeated manualliterature searches were made in appropriate bibliog-raphies, articles and textbooks. The result of thissearch led to Biggs and Collis’s (1982) model, Struc-ture of the Observed Learning Outcome (SOLO) tax-onomy, which was compared with the guidelines inorder to validate them at a later stage in the workprocess.
During the work process, the following questionemerged: ‘What is the student expected to learn dur-ing clinical education?’ Based on this question, fourcore concepts emerged: professional stance, reflec-tive processes, problem-solving processes, and practi-cal skills. Within the respective concepts, guidelineswere formulated at four different levels. The workmaterial was continuously validated by the researchgroup. In the research process, the group used schol-arly debate in the spirit of the Delphi technique.This technique was developed in the USA in themid 19th century for use in the areas of decision-making, innovation, education, and consensus build-
Figure 1.
Overview of the interaction between the main con-cepts of clinical guidelines, theoretical and practical knowl-edge, decision-making, clinical supervision and examination.
THEORY/ RESEARCH PRACTICE
Clinical guidelines
Decision-making
Practical knowledge
Education Clinical Supervision
Theoreticalknowledge
Examination
Practicalknowledge
Theoreticalknowledge

Guidelines in nursing education 223
ing (Linstone & Turoff, 1975; Hasson
et al
. (2000).Characteristics of this method are: anonymity ofrespondents, the selection of ‘experts’ as respon-dents, and the use of controlled iteration and feed-back (Armstrong
et al
., 2000). This method isimplemented as a series or ‘rounds’ to gather dataand feedback in the form of the respondents’ viewsand explanations/refinements of earlier responses.The expert panel revises the material several times(Eriksson, 1991). According to Roberts-Davis andRead (2001), Delphi studies may achieve a consen-sus of opinion among the respondents. Concepts andguidelines were validated by means of feedback tocolleagues and the expert panel of senior lecturers.Guidelines were modified to take into account bothoral and written viewpoints. In addition to this vali-dation, the guidelines were compared with Biggs andCollis’s (1982) SOLO taxonomy. This taxonomydescribes cognitive development and its outcome atdifferent levels and comprises five steps: the pre-structural, unistructural, multistructural, relational,and extended abstract steps. A comparison showedsimilarities between this taxonomy and the guide-lines at all four levels. The introduction level can becompared to prestructural and unistructural develop-ment, where knowledge is sought from other disci-plines in an attempt to improve understandingwithin nursing care. Compared with the multistruc-tural step, the intermediate level deals with the com-plexity of nursing care. Advanced levels can becompared to the fourth and fifth step in the taxon-omy, where the student can relate to and integrateknowledge in specific experienced situations and sit-uations not yet experienced.
FINDINGS
Four core concepts: professional stance, reflective pro-cesses, problem-solving processes, and practical skillswere identified and transformed into educationalguidelines at four academic levels: introductory, inter-mediate and advanced levels I and II.
Professional stance
Different professions within the field of health careshare the specific goals of satisfying human needsand contributing to the patient’s perception of well-being. A professional stance is rooted in value-related philosophical assumptions that are specific toa profession. This means, among other things, thatthe professional activity is governed by uniqueknowledge as well as by professional codes of eth-ics. The professional group shares certain values, has
a professional culture and monopolizes their ownactivities. The nurse has an independent profes-sional responsibility, a scientific base for the exer-cise of the profession. Nursing actions are based ona holistic and humanistic view of the human being(Strömberg, 1997). Severinsson (1995) states that apositive relationship exists between value founda-tion and professional stance, which is expressed inthe encounter between patients and nurses. Profes-sional stance is also influenced by the nurse’s self-perception and self-respect.
Development of the professional stance requiresmoral judgment as well as awareness of the autonomyof the nursing profession and its areas of knowledgeand responsibility (McAlpine, 1996). Furthermore, ascientific stance in relation to research findings isincluded as well as how these can be properly used innursing practice (Benner, 1984; Closs & Cheater, 1999)(Table 1).
Reflective and problem-solving processes
Reflective and problem-solving processes have a tra-jectory structure consisting of different phases. In thefirst phase, the problem/situation is described anddefined. The second phase is denoted as the analysisphase, where an understanding is sought by clarify-ing the constituent parts of the problem and/or situa-tion. The third phase implies the decision-makingprocess (Knowles, 1970). The problem-solving modelis used in relation to specific situations, information,instruction and leadership, to train and develop a stu-dent’s problem-solving ability in the complex realityof care.
Reflection means returning to oneself, mirroringone’s actions and professional stance in relation tooneself (self-reflection) and others (collegial reflec-tion). Reflection can both precede and follow anaction in the form of problem-solving and evalua-tion. Reflective thinking can take place at an indi-vidual, common and overarching level (Bengtsson,1993). A reflecting practitioner is basically an atten-tive, learning practitioner who contributes to thedevelopment of self-knowledge and professionalskills (Schön, 1983). The more experienced the prac-titioner, the more tacit this knowledge may be. In
reflection-in-action
the practitioner is in dialoguewith the situation, which increases the understand-ing of the situation, the ability to formulate prob-lems and decide what action needs to be taken.Schön (1983) also highlights
reflection-on-action
,which is when the practitioner assesses the situationat hand in light of their experience-based knowl-edge. Nursing care can be made visible and under-

224 M. Jerlock
et al.
standable through supervised reflection but thispresupposes a dialogue in the relationship betweensupervisor and supervisee.
According to Adams (1999), problem-solving, cre-ative thinking, clinical judgment and nursing processesmay be synonyms for critical thinking. Conversely, theycan be components of the concept of critical thinking(Table 2).
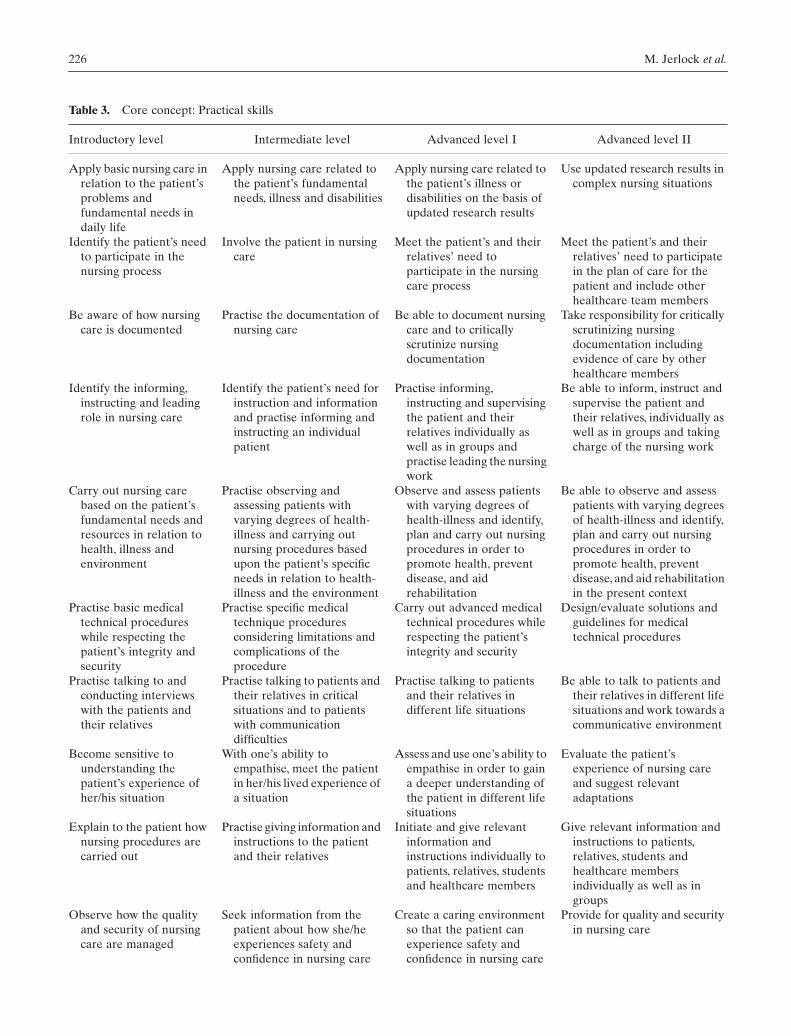
Practical skills
The concept of practical skills is described as art andpsycho-motor skills (Björk, 1997). The dimension ofart represents the creative dimension of nursing
care. Practice is practical actions in a real setting,and practical skills include the development of nurs-ing methods and techniques. Each situation is, inpractice, unique and connected to specific individu-als at a given point in time and is the result ofthoughts, values, feelings and judgments expressed indecisions and acts (Granum, 2001). Benner (1984)considers that components of practical knowledgeare handicraft skills, personal qualities and the abil-ity to cope with unexpected situations. Practicalskills include nursing care actions and techniques inaccordance with rules and regulations as well as doc-umentation and evaluation of the nursing process(Table 3).
Table 1.
Core concept: Professional stance
Introductory level Intermediate level Advanced level 1 Advanced level II
Maintain understanding and respect for people’s life situations regardless of gender, age or ethnicity
Be able to identify, reflect upon and describe personal fundamental values and one’s own view of people
Reflect upon, evaluate and understand how fundamental values affect nursing care
Safeguard the patient’s dignity and take responsibility for ensuring that the patient receives the best care and explicitly advocate as a voice for the patient
Be aware of how one’s own view of the human being affects one’s attitudes, and understanding the implications of values, norms and attitudes
Be able to identify, reflect upon and evaluate ethical positions within nursing care
Critically analyze decisions and their consequences for patients in nursing situations in accordance with ethical principles
Take moral responsibility for creating a caring culture aimed at preventing value conflicts
Be aware of the conditions of health care
Be aware of the nurse’s social and legal responsibilities
Be able to assume one’s social and legal responsibilities
Influence the conditions of health care on the basis of one’s social and legal responsibilities
Be able to identify and describe the knowledge and field activity of the nurse
Gain an understanding of the nurse’s fields of knowledge and responsibility in relation to other professional categories within health care
Be able to evaluate and respect the value and knowledge base of nurses in relation to their own and other’s professional boundaries
Be able to illuminate the specialist nurse’s areas of competence and responsibility, from the perspective of nursing science
Be aware of and understand the philosophical and theoretical science tradition of nursing care
Scrutinize and interpret research-based knowledge
Scrutinize and interpret research-based knowledge with a view to application in nursing care
Evaluate one’s own knowledge development in relation to national and international research
Be able to make use of one’s own interaction with patients and care teams
Be able to identity and reflect on one’s own interaction with patients and other caregivers
Be able to use one’s interactive ability in relation to the needs and integrity of the other person
Use one’s interactive ability to interpret and give a voice to the needs and will of the patient
Be aware of the meaning of empathy and creative ability in nursing care
Be able to identify and reflect upon one’s empathy and creativity in nursing care
Be able to make use of empathy and creative ability in nursing care
Be able to contribute to permitting a caring environment that promotes creativity and empathy

Guidelines in nursing education 225
Table 2.
Core concepts: Reflective processes and problem-solving processes
Introductory level Intermediate level Advanced level 1 Advanced level II
Reflect on how health is maintained and how sickness is counteracted
Reflect on how the individual patient may maintain health and counteract sickness
Be able to identify and analyze risk factors for illness and suggest preventive nursing procedures for an individual
Identify and reflect on risk factors in society and/or groups and recommend preventive nursing actions for individuals or groups
Reflect on different ethical principles and their consequences for nursing care
Carry out nursing care in accordance with sound ethics and moral principles
Critically analyze decisions and their consequences for patients in nursing situations in accordance with ethical principles
Take responsibility for seeing that nursing care is carried out in accordance with ethical and moral principles
Be aware of how nursing is guided by rules and regulations and organizational theories
Reflect on the norms and values which form the basis for the organization of nursing care
Reflect on whether one’s own nursing actions are in accordance with rules and regulations
Re-evaluate rules, regulations and caring organization to ensure an evident and safe care for the patient
Identify and reflect on all phases of the nursing process
Reflect on and interpret connections in the process of nursing care and provide continuity throughout the process for one patient
Reflect on and interpret connections in the process of nursing care and provide continuity throughout the process for more than one patient
Reflect on, interpret connections and provide continuity throughout the process of nursing care in complex situations
Be aware of the patient’s requirements and resources
Be able to identify and analyze the patient’s requirements and resources
Analyze and assess nursing requirements and suggest nursing procedures
In a complex nursing situation, suggest appropriate nursing procedures, make decisions and assess their consequences
Reflect on relevant knowledge required for solving nursing problems
Further develop competence for problem-solving in relation to current care situations
Deepen and broaden competence with regard to problem-solving in practical care situations
On the basis of current research, analyze problems related to nursing, organization and leadership, as well as critically assessing various solutions
Begin to develop competence in problem solving in relation to nursing situations
Further develop competence in problem-solving in relation to nursing situations
Deepen and broaden competence in problem-solving in relation to nursing situations
Identify problem areas and draw up proposals for improvements using a relevant problem-solving model
Become aware of the nurse’s leading, informational and instructive role
Be able to relate the nurse’s leading, informational and instructive role to the nursing process
Identify and analyze problems/needs which are related to the nurse’s leading, informational and instructive role in nursing care
Identify and analyze problems/needs which are related to the nurse’s leading, informational and instructive role in nursing care and propose appropriate actions
Become aware of the importance of research results for nursing care
Assess nursing care in relation to research results
In nursing situations, to plan and propose relevant evidence-based nursing actions and be aware of the consequences
In complex nursing situations, to propose relevant evidence-based nursing actions, make decisions and assess the consequences
Reflect on quality and security in nursing care
Reflect on conditions necessary for the patient and their relatives to experience safety and confidence in nursing care
Be responsible for the quality and security of nursing care
Evaluate and suggest solutions for development of quality and security in nursing care
Become aware of suffering as a phenomenon
Reflect on the nurse’s possibilities and responsibility to reduce suffering from illness and treatment
Be able to meet patients with different forms of suffering and contribute to the experience of well-being of the patient and their relatives
In relation to nursing work, create an environment contributing to patients’ and relatives’ experience of well-being despite suffering
226 M. Jerlock
et al.
Table 3.
Core concept: Practical skills
Introductory level Intermediate level Advanced level I Advanced level II
Apply basic nursing care in relation to the patient’s problems and fundamental needs in daily life
Apply nursing care related to the patient’s fundamental needs, illness and disabilities
Apply nursing care related to the patient’s illness or disabilities on the basis of updated research results
Use updated research results in complex nursing situations
Identify the patient’s need to participate in the nursing process
Involve the patient in nursing care
Meet the patient’s and their relatives’ need to participate in the nursing care process
Meet the patient’s and their relatives’ need to participate in the plan of care for the patient and include other healthcare team members
Be aware of how nursing care is documented
Practise the documentation of nursing care
Be able to document nursing care and to critically scrutinize nursing documentation
Take responsibility for critically scrutinizing nursing documentation including evidence of care by other healthcare members
Identify the informing, instructing and leading role in nursing care
Identify the patient’s need for instruction and information and practise informing and instructing an individual patient
Practise informing, instructing and supervising the patient and their relatives individually as well as in groups and practise leading the nursing work
Be able to inform, instruct and supervise the patient and their relatives, individually as well as in groups and taking charge of the nursing work
Carry out nursing care based on the patient’s fundamental needs and resources in relation to health, illness and environment
Practise observing and assessing patients with varying degrees of health-illness and carrying out nursing procedures based upon the patient’s specific needs in relation to health-illness and the environment
Observe and assess patients with varying degrees of health-illness and identify, plan and carry out nursing procedures in order to promote health, prevent disease, and aid rehabilitation
Be able to observe and assess patients with varying degrees of health-illness and identify, plan and carry out nursing procedures in order to promote health, prevent disease, and aid rehabilitation in the present context
Practise basic medical technical procedures while respecting the patient’s integrity and security
Practise specific medical technique procedures considering limitations and complications of the procedure
Carry out advanced medical technical procedures while respecting the patient’s integrity and security
Design/evaluate solutions and guidelines for medical technical procedures
Practise talking to and conducting interviews with the patients and their relatives
Practise talking to patients and their relatives in critical situations and to patients with communication difficulties
Practise talking to patients and their relatives in different life situations
Be able to talk to patients and their relatives in different life situations and work towards a communicative environment
Become sensitive to understanding the patient’s experience of her/his situation
With one’s ability to empathise, meet the patient in her/his lived experience of a situation
Assess and use one’s ability to empathise in order to gain a deeper understanding of the patient in different life situations
Evaluate the patient’s experience of nursing care and suggest relevant adaptations
Explain to the patient how nursing procedures are carried out
Practise giving information and instructions to the patient and their relatives
Initiate and give relevant information and instructions individually to patients, relatives, students and healthcare members
Give relevant information and instructions to patients, relatives, students and healthcare members individually as well as in groups
Observe how the quality and security of nursing care are managed
Seek information from the patient about how she/he experiences safety and confidence in nursing care
Create a caring environment so that the patient can experience safety and confidence in nursing care
Provide for quality and security in nursing care

Guidelines in nursing education 227
CONCLUSION AND IMPLICATIONS FOR NURSING EDUCATION
The aim of the present study was to develop educa-tional guidelines to be used as a tool for the integrationof theory, research and practice in order to create anacademic nursing education based on nursing knowl-edge, experience and practical skills. An additional aimwas to elucidate the students’ expected competence innursing at four academic levels: introductory, interme-diate and advanced levels I and II.
In the model, the guidelines take both a general andan abstract form. They are not connected to a specificcare context, patient group or to specific nursing prob-lems. They are intended for use as a tool in the deduc-tive and inductive learning process to bridge the gapbetween theory, research and practice. The guidelineswere developed from collegial discussions dealing withresearch and optimum nursing experiences of the pro-vision of excellent nursing care in accordance with theDelphi technique. Criticisms of the Delphi methodusually focus on, for example, lack of accountabilityfrom respondents and unrepresentative samples (Sack-man, 1975). There are several limitations to this studythat need to be addressed. One is related to the size ofthe expert panel. It can be argued that a group of eightparticipants does not provide a fair representation of acollegial population. Another limitation of the studywas that the participant group was selected from oneuniversity. It may have been better to research theviews of lecturers from a number of different universi-ties to gain a more generalized view of the issue. There-fore, the guidelines should not be seen as definitivegoals but rather as guidelines for the ongoing learningprocess with individual freedom of interpretation andrevision as well as encouraging the development ofexcellence in nursing. Yet, now that the guidelines inthis area have been identified they could be furthertested in clinical nursing education.
Problem-solving and reflection are foundations ofthe learning process. Decision-making based on theo-retical knowledge, experiences and judgment in rela-tion to the unique situation could make the learningprocess visible if the student formulates and verbalizes
the motive and prerequisites for the decision. Scientificknowledge, experiences and moral judgment must beintegrated inductively, and the student must have theopportunity to combine experiences with evidence-based knowledge in order to develop preparedness fordecision-making and nursing actions. The guidelineselucidate the level of competence expected of studentnurses and challenge their personal qualifications inrelation to professional demands.
Modern day knowledge reproduction demandsopenness, creativity and flexibility in the continuousreassessment of old ‘truths’ as well as their substitutionwith new knowledge. An active search for knowledgerequires structural and environmental prerequisitesthat create freedom and curiosity and should be a cen-tral aspect of academic education. It is a necessity for aprofessional life-learning process and for anyone whowants to develop and influence the future.
An academic nursing program should produce inde-pendent and autonomous nurses with the ability toacquire, update and assimilate new knowledge, skillsand attitudes. In their future professional life as nurses,the students will be continuously faced with situationswhere they have to take ethically motivated and cor-rect decisions and act in a professional way. Thisdemands training in problem-solving, reflection, deci-sion-making and use of both deductive and inductivelearning strategies.
In addition to traditional examinations of theoreticalknowledge and practical skills, an examination of thestudent’s decision-making process related to a specificnursing problem could act as an incentive for this learn-ing process. The examination aims to make explicit thestudent’s theoretical knowledge, judgment ability, cre-ativity and flexibility vis-à-vis any given situation. Thedecision can also be judged based on the student’s pre-paredness for nursing actions and their consequences.The guidelines could be used as criteria for outcomestandards on the four levels of the education. Anotheraspect of the examination is the importance of assessinga student’s ability for self-directed learning throughidentifying human and material resources, formulatingown needs, setting goals, choosing strategies, and eval-uating results of the learning process.
Practise scrutinizing research results in nursing
Systematize and analyze research results in nursing
Carry out a paper based on earlier research and apply the knowledge to the relevant context
Develop methods and techniques based on research results in nursing care
Introductory level Intermediate level Advanced level I Advanced level II
Table 3.
Continued

228 M. Jerlock
et al.
ACKNOWLEDGMENTS
The authors wish to thank the lecturers at the Sahlg-renska Academy at Göteborg University, Faculty ofHealth and Caring Science, Institute of Nursing, fortheir participation and Gullvi Nilsson for reviewing theEnglish.
REFERENCES
Adams BL. Nursing education for critical thinking: an inte-grative review.
J. Nurs. Educ.
1999;
38
: 111–119.Armstrong AE, Parsons S, Barker PJ. An inquiry into moral
virtues, especially compassion, in psychiatric nurses: find-ings from Delphi study.
J. Psychiatr. Mental Health Nurs.
2000;
7
: 297–306.Bégat I, Severinsson E. Nurses’ reflections on episodes
occurring during their provision of care—An interviewstudy.
Int. J. Nurs. Stud.
2001;
38
: 71–77.Bengtsson J. Theory and practice: Two fundamental catego-
ries in the philosophy of teacher education.
Educ. Rev.
1993;
3
: 21–32.Benner P.
From Novice to Expert: Excellence and Power inClinical Nursing
. Wokingham: Addison-Wesley, 1984.Berggren I, Severinsson E. The influence of clinical supervi-
sion on nurses’ moral decision-making.
Nurs. Ethics
2000;
7
: 124–133.Bevis EO.
New Directions for a New Age in Curriculum Rev-olution: Mandate for Change.
New York: National Leaguefor Nursing, 1988.
Biggs JB, Collis KF.
Evaluating the Quality of Learning
. NewYork and Sydney: Academic Press, 1982.
Björk IT. Changing conceptions of practical skill and skill ac-quisition in nursing education.
Nurs. Inq.
1997;
4
: 184–195.Bowden J, Marton F.
The University of Learning. BeyondQuality and Competence in Higher Education.
London:Kogan Page Ltd, 1998.
Cioffi J. Triage decision making: Educational strategies.
Acci-dent Emerg. Nurs.
1999;
7
: 106–111.Closs SJ, Cheater FM. Evidence for nursing practice: a clar-
ification of the issues.
J. Adv. Nurs.
1999;
30
: 10–17.Eriksson K.
Bridges: Introduction to the Methods of CaringScience.
Abo: Abo Akademis kopieringscentral, 1991.Granum V.
Students’ perceptions about nursing as a subjectand as a function.
[Dissertation]. Göteborg: Acta Univer-sitatis Gothenburgensis, 2001.
Harbison J. Clinical decision making in nursing: theoreticalperspectives and their relevance to practice.
J. Adv. Nurs.
2001;
35
: 126–133.Hasson F, Keeney S, McKenna H. Research guidelines for the
Delphi survey technique.
J. Adv. Nurs.
2000;
32
: 1008–1015.Holm A-K, Lantz I, Severinsson E. Nursing students’ expe-
riences of the effects of continual process-oriented groupsupervision.
J. Nurs. Manage.
1998;
6
: 105–113.Knowles M.
The Modern Practice of an Adult Education.
New York: Association Press, 1970.
Linstone HA, Turoff M.
The Delphi Method. Techniques andApplication.
Massachusetts: Addison-Wesley Reading,1975.
Long A, Harrison S. Evidence-based decision making.
Health Service Journal
1997;
6
: 1–11.Lützén K.
Moral sensitivity: A study of subjective aspects ofthe process of moral decision making in psychiatric nursing.
[Dissertation]. Stockholm: Karolinska Institute, HuddingeUniversity Hospital, 1993.
McAlpine H. Critical reflections about professional ethicalstances: have we lost sight of the major objectives?
J. Nurs.Educ.
1996;
35
: 119–125.McSherry R, Proctor-Childs T. Promoting evidence-based
practice through an integrated model of care: patient casestudies as a teaching method.
Nurs. Educ. Prac.
2001;
1
:19–26.
Mead P. Clinical guidelines: promoting clinical effectivenessor a professional minefield?
J. Adv. Nurs.
2000;
31
: 110–116.
Nylund L, Lindholm L. The importance of ethics in the clin-ical supervision of nursing students.
Nurs. Ethics
1999;
6
:278–286.
Roberts-Davis M, Read S. Clinical role clarification: usingthe Delphi method to establish similarities and differencesbetween Nurse Practitioners and Clinical Nurse Special-ists.
J. Clin. Nurs.
2001;
10
: 33–43.Rolf B.
Profession, Tradition and Silent Knowledge
. Nora:Nya Doxa, 1991.
Sacket D, Richardson S, Rosenberg W, Haynes B.
Evidence-Based Medicine. How to Teach and Practice EBM
. Edin-burgh: Churchill Livingstone, 1997.
Sackman H.
A Delphi Critique.
Massachusetts: LexingtonBooks, 1975.
Schön DA.
Educating the Reflective Practitioner: Toward aNew Design for Teaching and Learning in the Professions
.San Francisco: Jossey-Bass, 1987.
Schön DA.
The Reflective Practitioner—How ProfessionalsThink in Action
. New York: N.Y. Basic Books, 1983.Severinsson E.
Clinical Nursing Supervision in Health Care
.[Dissertation]. Gothenburg: The Nordic School of PublicHealth, 1995.
Severinsson E. Confirmation, meaning and self-awareness ascore concepts of the nursing supervision model.
Nurse Eth-ics
2001;
8
: 36–44.Strömberg B.
Professional Attitudes and Nurses. A study ofconceptions.
[Dissertation]. Göteborg: Acta UniversitatisGothenburgensis, 1997.
The Higher Education Ordinance.
UFB 3 1999/2000.
Stock-holm: Norstedts Juridik AB, 1993 (in Swedish).
Valiga TM.
Curriculum Outcomes and Cognitive Develop-ment: New Perspectives for Nursing in Curriculum Revolu-tion Mandate for Change.
New York: National League forNursing, 1988.
Watt S. Clinical decision-making in the context of chronic ill-ness.
Health Expectations.
2000;
3
: 6–16.










