Embed Size (px)
Citation preview

Itcprinted from IJr I lnlrt J 1982; 48: 572-9 (,'('pvrighr IYc?2 Ilvirislr I-leart Jolonal All rights of reproduction of rhis reprint are resewed in all countries of the world
Accuracy and reliability of two indirect ambulatory blood pressure recorders: Remler M2000 and Cardiodyne Sphyginolog
1) J l:I'I'%GI:RALD, W ti O'CI\I,I,I\CIIAN, li hlcQUAIU, K O'MALLEY, E 0'13RIEN
Brin'sh Medical Association, Tavistock Square, London IVCIH 9JR
Accuracy and reliability of two indirect anlbulatory blood pressure rccordcrs: Kemlcr M2000 and
S I I ~ I A I , \ I < Y 'I'lie Ke~iilcr h1200U and Cardiodyoe Spl~ygtilolog are seniiautotnatic recorders dcsigtied to t i ic;~s~r~.c a~i ib \~la tory blood pressure non-invasivcly. 'I'licsc recorders wcre assessed for accuracy and 1-clial)ility ill a study dcsigrlcd ill tlircc stages. 17irstly, tlie i~itcrdevice variability was assessed separately ,. for cacll type of recorder by cotiiparing the recordi~igs of t11ree devices against each otlier and against sitil~rlta~leous rccortli~lgs by a lticrcury star~dard i r i 12 ~)iitic~its, ~iiultiple recordings bciiig tiiade it1 a 1.illl~I0111 order in each ~)atietit. 'l'he n~crcury staticlard used was tlie L o ~ i d o ~ i Scliool of Ilygierie (LSII) s l~l iygl i io~i ia~lo~~~cter arid the I Iawksley ratidotn zero spl~yg~iiotiianonieter duririg assessment of the I<ct~ilcr ilnil Spliyg~~iolog, rcspcctively. 'I'liougli tlierc were tio dif'ferctices between the tliree Kemler rccortlcrs tcstetl, o ~ i c Spliyg~iiolog rccorder gave Iiigher recorditigs tliari tlie two otllcr Spliyg~~iolog rccortlcrs testcd because of a zero tlril't of 3 to 4 o ~ u i l l g it1 [lie pressure transducer. Reniler recordirigs were liiglicr t11ati s i~~ i i t l t a~ icv i~s 1,SII sl~liygtiio~iiatio~i~eter rccordiiigs for boll1 systolic and diastolic prcssl~rcs. 111 tllc seco~id part of tllc study, the Kc~nlcr was co11il)ared with tlic 1.Iawkslcy using si~iiulta~ieous recordings in the sanie arnl in 58 patients. No difference was fourld betweell Hawksley aucl Kcnilcr rccorditlgs. 'I'lic discscpa~icy bctwcc~i tllis a~lcl t l ~ c Rcmlcr-LSII con~parisoo resulted Irotii a t e ~ ~ d c ~ i c y for tlic LSI.1 s~)l~ygtiionia~io~i~etcr to ur idcres t i~~~ate blood pressure. Siniilarly, tlie Sl>l~yg~iiolog rccorditlgs wcrc corul7arcd wid1 si~~iultarieous I lawkslcy recordirigs in 100 patients. N o sig~iifica~lt tliffcrei~ce was foutid bcttvcc~i paired systolic pressure rccorclirigs tllougli Sl)liygmolog rcco~~tlings u~irlcrcsti~~iatcd diastolic blood pressure. 111 tlic t l~ i rd part oftllc study, tlie reliability of [lie I<a~ i l c r was assessed froin 69 atte~rlptcd day rccordirlgs. Five Rcniler day recordiligs failed, a tiiajor cause of lost rccordi~lgs being a defect in tlie niicroplionc lead. 'I'lie reliability of [lie Spllygniolog was cotnparcd with the Kcoiler by atte~iipting day recortli~tgs with each device in 13 patients. 'I'he rcli:ihility of tllc Sl ) l~ygt~~olog was sigriificailtly poorer, o~ i ly live of 13 Spliygniolog day recordings bciog dccodablc because of d i s l v d g c ~ ~ ~ e n t of tllc recordit~g disc cl t~ri~ig a~ i~bu la t io~ i .
Sirlgle cliilic rccordi~lgs niay tiot rellect rlie blood pressure I>eliavioitr of ttlany patie11rs.1-3 ~l'licrcfore, tlletllods of assessiti~ I)lotd pressrtre beliaviour o~trside tllc clioic llavc been dcvclol)ed atid i~lclude I~olrle rccorditig Ity tllc 1)aticti1~5 or a relative,%tld i11tl.a- arterial1 and illdirect n~~ibularory recorditig.7 8
Ititra-arterial recvrditlg is an itlvasive procedure which is not witliout risk.9 Ilome recordirig tiiay be itlaccurate I,ccause of patietit bias.10 ltldirect :~tlll~rllatory blood pressrlre recorditig sllould be free of tllcse rlisadvatltagcs but tliere llave llot bccti tiiariy Arn.1~1rtl For ~ ? ~ ~ l > l i c n l i v n 14 ~\riglirl 1981
stuilics otl tlic accuracy of tlte recorders that are riow avnilnhle.
111 ~llis p:lpcr we presetit our fi~iditlgs oti tlie accuracy atlcl ~.clial)ility of two att1bitl:ltory blwJ pressure rccorders, tlle I<eallcr M2WO attd Cardiodyne S~,llyglllolog.
Med~ods and results
'I'lie I<crlilcr MZOOO is a portable blood pressure recorder co~isisti~lg of a cuff and tiiicrol~liotie con- ilcctcd to a ~)ressurc tra~isduce~. atid ttiicrocassette
fig. I 7%e Ren~let. hlZO00 (right) ntld dcrod~r ( I t f I ) wirh extrr~lp/e of pressure rccordittg OII (he s~rip churl.
Fig. 2 l'he Curdiod-vtre Spl~ygntolog.

recorder worii or1 the patient's waist (Fig. 1). 'l'lie cuff is inflatecl hv the patierit at prescribed intervals and deflates ai~tomatically. l h r i ng deflation the Korotkoff sor~rids and ci~ff nressurc are recorded on a magnetic - t:lpc. The tape is later analysed through a separate dccotlcr ~vliich gives a strip chart recording of the so1111ds sul>erinllwsed on a tracing ofcuff pressure (Fig. I). 'l'tie pressures correslx)~idirig to the first and last sou~ids are rccordctl ;IS tlie systolic and diastolic end- 1>oi1its, resl>ectively. As weaker sounds mav not deflect the 17cri in the tlecoder an observer listens to tlic tape tluri~ig Jccotlitig slid 11i:irks on tlic pressure traci~ig the lwsi~iori of the first ;11ii1 1;lsr sountls. I'eri tlcllcctions c:ir~scil by i~rtcli~cts car1 he cxcliidcd at the sanie tinic.
'I'llc Cal.cliodyrie Sl>liygnlolog also corisists of a s ~ ~ I i y g ~ ~ i o ~ i ~ ; ~ ~ ~ o ~ i i e t c r cuff ~vliicli is i~ifliite(l hy the ljarient illid ~vliicl~ CICII;I~CS a~to~natic:~Ilv tliroiigh a ~iectllc valve (Fig. 2). 'l'lle cuff pressure is niouitored hv a Iwcssurc transducer wliicli drives a pen suspended over a paper disc. 'I'hc Korotkoff sourids arc tletected hy ;I niicrophone placed heneatli the lower cuff margin arid are recorded on to the paper disc by the pen as it nioves across tlie disc. As the disc is calibrated for I'ressilrc, tlie first a~itl last pen niarks are recorded as tlicsys~olic arid diastolic point, respectively. l'he paper disc is drivcri by a clockwork ~ilechanisrii and revolves ot~cc in 24 Iiours. 111 this way, a real-time recording of claily hlood pressures is nlade. I;urtlier~liore. the hlood pressure recortlings are read directlv from the disc, so that a separate decoder or analvser is not required.
For each iristrume~it three devices were tested to iletcct interdcvicc varinhility. a source of possihlc error in automated devicesll wliicli may bias the overall assessliient of their accuracy. 'l'lie accuracy of one of eacli tvpe of recorder was then tested against a mercury standard. As the decision entl-points for svstolic ant1 di;istolic pressures are observer dependent, inter- observer variability in the decoding of pressure record- ings was also assessed. 'I'he results were analysed by S t u d c ~ ~ ' s t rest for paired data and by linear regression analysis. 111 all cases phase V was used as the diastolic c~id-poirit.
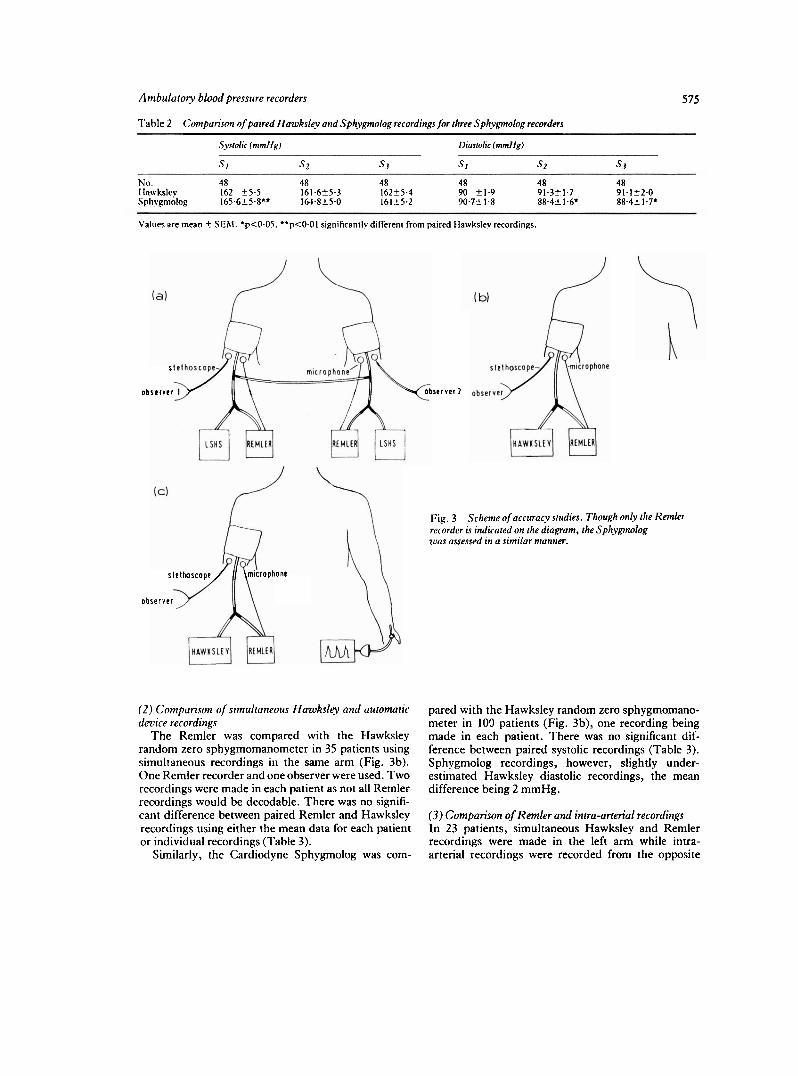
A(;(:tIItA(;S S I l l l > l l ~ S ( I ) 11rrerderic.e v~iriabilr~v .l'lie Kemler was conipared with the London School of 1 lygierie (l.SI 1) spliygnio1nanometer~2 in 12 patients as part of all interdevice variability study of three Kemler recorders. I'aired 1,SI I spllygmomarionieter and I<emler recordings were ~ilade in the sanie arm by connecting both devices to a single cuff through a Y connector (Fig. 3a). The stethoscope head and rnicro- phone were applied to the sanie brachial artery without difficulty. Si~nr~ltaneously a second observer recorded paired Rc~nler-I.SEI sl>Iiygmonlancrtneter recordings in the oppc)site arm by the same tech~iiclue. As the two
cuffs were interconnected we were able to compare si~nultaneous Kemler recordings in opposite arms and also simultaneous Remler and LSEI sphygmomano- meter recordings in the same arm. Tlie order of Kemler recorders, the arm to which the recorders were applied, '
and the observers was randomised according to a Graeco-Latin square design. In this way observer and sequential bias, or bias resulting from differences between arms would not influence results. 'She rate of deflation ofthe system was set at 3 mmI-lg per second as we observed that lower deflation rates caused attenu- ation of the Korotkoff sounds.
'I'lie interdevice variability of the Cardiodyne Spliygr~iolog was assessed in the same way (Fig. 3a) except that instcad of the [,St1 sl~liygmo~i~atiomctcr (lie I Iawkslcy rantlotn-zero spliyg~lioniano~lictcr~ was used as tlie mercury standard.
'I'here was no significarit difference between observers or between the three Remler recorders (*l'ahle 1). Remler recordings were higher than LS1-l sphyg~llo~nanometer recordings for both systolic and -"
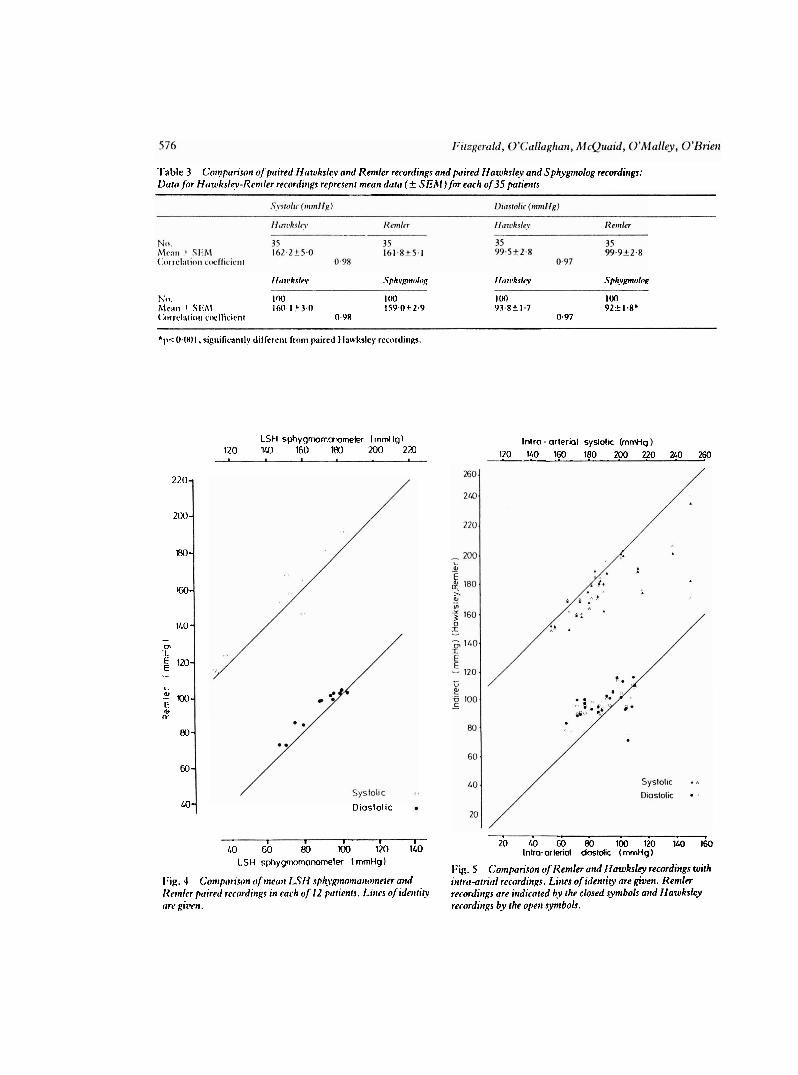
diastolic blood pressures, the mean differences being 4.8 11in11ig (p<O.OS) and 4.7 mnlI-lg (p<O.005), respectively. This was true whether the niean Rernler ant1 1,SEI spliygmo~nanometer recordings for eacli of the 12 patients (Fig. 4) or individual recordings were compared. Furrllermore, the mean differences between paired Kemler and LSH sphygmon~ano~neter record- ings were negatively correlated with heart rate for diastolic (r,-0.69 n=12, p<0.02) but not systolic blood pressures.
'I'nhlc I (,'o~~rp,rrison q/!ltree Kemler r~rovders
Sysrolk (ntrnl1,q) 1)icrrolir (mmllg)
I~enilrr I 161.6f 4.5 94.7t 1.8 I<e111lcr 2 163.4k4.4 Y3.7-tZ.I I<ettiler 3 161 t4.3 93.4+ 1.6
V a l ~ ~ e s are mean f SEM.
Overall, there was no significant difference between paired Sphygmolog and I-Iawksley recordings in the 12 patients whether the mean data for each patient or individual recordings were compared. One Sphygmolog recorder (S,), however, significantly overestimated paired IIawksley systolic recordings ('l'able 2) and co~tiparison of individual paired Sphygmolog record- ings in opposite arms showed that S, recordings were higher than S2 and S, recordings, the mean difference being 4.3 m~ill-Ig (p<0.01) for systolic and 2.4 mmHg (p<0.06) for diastolic recordings. S2 and S3 Spllygmolog recordings tended to underestimate Elawksley diastolic pressure recordings (by 2.8 mmHg on average) while S I recordings sliowed a niean excess 010.7 1111111 Ig over the 1 lawksley.
Amblilutory blood pressure recorders 575
Table 2 (;omparisml of paired Fiawks1e.v and Sphygmolog recordings for three Sphygmolog recorders
Svsn~lic ( r n ~ n H ~ f Diasrol ic (mmlfg)
S 1 S 2 -7.i S 1 Sz s.3
No. 48 48 48 48 48 48 Ila~vkslev 162 i.5.5 161.6-15.3 162-1 5.4 90 -11.9 91.3C1.7 91.1t2.0 Sphygmolog 165.6-15.8" 164.8-1 5.0 161t5.2 90.7-1 1.8 88.4-1 1.6' 88.4-1 1.7.
Values are mean + SEA!. 'p<O.O5. '*p<0.01 significantlv different from paired Flawkslev recordings.
S
observer se r
slelhoscope microphone
observer
( 2 ) Compurisor~ of simultaneous Hawksl ty and automaric device recordings
'The Remler was compared with the Hawksley random zero sphygmomanometer in 35 patients using simultaneous recordings in the same arm (Fig. 3b). One Remler recorder and one observer were used. Two recordings were made in each patient as not all Remler recordings would be decodable. There was no signifi- cant difference between paired Remler and Hawksley recordings using either the mean data for each patient or individual recordings (Table 3).
Similarly, the Cardiodyne Sphygmolog was com-
v c r 2
Fig. 3 Scheme ojaccuracy srudies. Though on(y ~l te Remler recorder is indicated on the diagram, the Sphygmolog was assessed in a similar manner.
pared with the Hawksley random zero sphygmomano- meter in 103 patients (Fig. 3b), one recording being made in each patient. There was no significant dif- ference between paired systolic recordings (Table 3). Sphygmolog recordings, however, slightly under- estimated Hawksley diastolic recordings, the mean difference being 2 mmHg.
(3) Comparison of Remler and intra-arterial recordings In 23 patients, simultaneous Hawksley and Remler recordings were made in the left arm while inua- arterial recordings were recorded from the opposite
'['able 3 Cotnpurisort o[puired Hawksle-v and Remler ret.ordings and paired Nawksley andsphygtnolog recordiirgs: 1)trtofor Ifou~kslev-Remler recorciitrgs represent mean dutu (+ SEAf) for each of 35 ptrrienrs
Il~nrkrln. .Yph\yp~tak~g I i r r r ~ ~ k r l ~ Sph.vprok~~
No. IfW 100 100 100 Alc:~ri 1 Slthl 160.1 .t3.0 159.0 t 2.9 93.8+ 1.7 92+ 1.8* ( ;~~rrc l : t l i o~~ c~wl'licirr~r 0.98 0.97
'I~<O.IH)I, sigriifican~lv dilfcrerir f rc~~n paired Ila~vkslcy rccordir~~s.
220-
200-
m-
1M-
1LO- - cn I E 120- E .- L
.A' m- C- 0 (L
80-
60 -
LO-
LSH sphygmorconornekx lrnmHgl 120 1 160 180 200 220
Diaslolic
Intra - arterial syslolic (mrnHg 120 140 160 180 2?0 q 0 260
I I I I I
LO 60 80 100 120 1LO 20 LO 60 80 100 120 l40 160
Inlra-arterial dastdic (mmHg) LSH spt~ygmomonorneler I mmtig
Fig. 5 Cotnparicon oJReinler oitd Ilawksley recordiitgs with I . 4 (;onrptmrisotr of rnea~r I,TN sp/t\~gtirottrcrittttne~er u i d ittrrcm-atrial recorditrps. Lines o f itietrrirv are aiven. Remler ~d;ittlcr puirecf rrcodit;gs in c0c.h of 12 polients. Liirrs of ide,rricv recorditrgs are i t t dk i ed by thhlosed s j m b o i and Ifowkrley clrc. gkr,ir. recordings by the open synrbols.

railii~l artery through a I%ell and kiowell pressure trans- ducer o n to light sensitive paper (Fig. 3c). 'l'lirce rccorcli~lgs were nlade in ciicll paticlit as not i11I Kclillcr recorditigs n.ould he dccodalile.
'l'lie relation hctwecn Kenller and intra-arterial recordi~lps was tlie sarne as between llawkslev a ~ l d intril-arterial rccortlings for Iiotli systolic and diastolic blood pressures (Fig. 5, 'l'ahle 4). Again. there was no significant difference het\vcen tla\vkslcy arid Rcrnlcr recordi~igs.
lZlil.1AltII.l'l'Y S.l'tll)Y 'I'lic rclial)ility of rllc Hcnilcr ill recorlling anibulatory I)looil I)rcssrlrc was nsscsscd bv tlctcr~ilining tlle ~lunll)cr of dccoclable recordings lroni 69 attc~nljtcd I<cnller anlliulatory dav rccordi~lgs. Of these, five fiiilcd coinlllctcly, in three cases because the n~icro- l i l~o~lc Icail I7rokc 2nd in two hccat~sc of a tlcfcct in the "(ill" pressure switcli wllicll failed despite rior~nal ~ilclliitio~l. 111 the reriiaining 64 tapes, 1 129 pressure rcct)rtli~lgs wcrc a t t a ~ ~ p t c d and I04 (9.2'51) of t hcsc were u~idccodahlc. 111 35 (3. IIY/n this was bccausc ol'the failure of tllc n~icrophonc to detect any sounds arid il l
tile rernai~~der because of either incorrect setting of the on-off pressure switclies or patient movcnlent.
In 13 hypertensive patients the reliahilitv of S~~liyg~iiolog nnlhr~larory recordings was conil~arcd with that of Kcnller an~bulatory recordings. Kecord- ings with each device were carried out in each patient on separate days during normal daily activities. .She orilcr of r~iachirles was randotnised to ~ ~ r e v c n t a training cllcct and trcatllicllt betwccri tlie two clays was not itltcred.
111 o~ily live of 13 Sphygniolog day recordings could a reasonable attempt be made at analyses conlpared with 12 of 13 Rcniler day recordings (X2 5.42 after Yates correction, p<0.02). 111 tlie remaining eight, ~ h c r e \vcrc I I ~ decodal~le recordings. 111 six cases this was the due to dislodgement of the paper disc from the motor spindle and in two a large number of artefacts made decoding impossible. *I'he one Remler failure resulted from an excessive cuff deflation rate.
I N ' l ' l i R O l t S l i R V I U VARIAIIII.I~rY I N 1)ECOUINti I~itcrobservcr variability in decoding was assessed by conllxtring tlic decoded results of two observers for I20
Kc~nler and 88 Sldiygn~olog blood pressure recordings ~liacle il l the laboratory.
There was no significant difference betu.eerl the two ohservers in decoding Kemler recordings, but 10°/o of all decodcd recordi~lgs'differed by more than +5 m1n1 lg, the niean difference being 0.7k4.2 rnniklg for systolic and 0.625.4 n11nHg for diastolic blood pressure recordings. *l'he paired decoded recordings were highly correlated for systolic (r, 0.99, p<0.001) and diastolic (r, 0.93, p<0.001) recordings. Similarly, there was no significant difference between observers for decoding Sphygrnolog systolic recordings though tllere was a sn~all difference for diastolic recordings, the rlieall being I t i in~l lg (p<0.01). The paired decodcd recordirigs were again Ilighly correlated for both systolic ( r , 0.98, p<0.001) and diastolic (r, 0.99, 17<0.001) pressures. Of the 88 paired decoded recordings, 9.2%" of systolic and 5% of diastolic recordings differed by more than 5 mmklg.
Accuracy sruclies of auto~ilated blood pressure recordcrs arc beset with problems, including the vari- ation between repeated blood pressure measurements, interdevice variability,ll observer error,14 and the type of standards against which they should be tested.15 l6
Where it is possible, as for these two machines, toapply both the standard and automatic recorders to the same brachial artery, conlparison ofsinlultaneous recordings in the sanie arm is the ideal rnetllod of assessmet~ t .~~ This re~noves the effect of blood pressure variability, whicli [nay othenvise be ascribed to the method of hlood pressure recording under test. I:urthermorc, by co~nparing the recordings of a number of test instru- ments niade repeatedly in a small group of patients, interdevice differences are easily detcctcd which would otlienvise require recordings from large riunlbers of subjects. Sunultaneous mercury sphygtnomanometer recordings can be used as a standard against which these differences are confinned, excluding blood pressure variability as a possible cause.
'I'lie accuracy of the Kemler M2000 has been assessed previously with varying results.lR-22 In two studies in which the standard used for comparison was the LSFI sphygmomanometer, tlie Kemler was found to over-
ial recordr~ras in enrh o f 23 ~ariettrs

estinlate systolic and diastolic blood pressures.lR z" 111 contrast. wllen compared with the I I a w k s l e ~ ~ ~ or a standard mercury spllygmo~nanonleter,'~ the I<err~ler showed no mean bias. In this study tlle Rernler recordings were higher than simultaneous LSH spl~ygmo~nanometer recordings, whereas there was no difference bctween Relnler and Hawksley recordings. 'I'his is consistent with our previous finding that the 1,SI I si~l~ypl~iolllallo~rleter urldercsti~natfs blood pressure partly because of incorrect ca1il)ration but also bcc:~usc of :III interl>rctative difference betwcen the 1,SI 1 spl~vpn~ornanon~etcr and other methods of blood pressure measurenlerlt.2' The interpretative difference results in arl error during blood pressure recording which is heart r:~tc dcpcndent2? and is corllirnled in tllis stu~lv by t l ~ c ricgative correlation between the mean Iicnllcr-1,SI I sl)l~ygrnolnanolneter differences for diastolic 1)lood pressurc and l~eart rate.
Comparison of Retriler and intra-arterial recordings has sliorvn a systematic error of +3 /+2 m111llg.2I l 'he relation of indirect to intra-arterial measurement, how- ever, is highly ~ariable.2.~26 Therefore, comparison of Iienller and intra-arterial recordings should be assessed by sirr~ultaneous comparison of Remler and mercury sl,l~ygnlo~~~anomctcr recordings witli intra-arterial recordings. In this study the mean bias and relation hetween direct and indirect recordings was the same for Iielnler and I lawksley recordings.
A possible source of variability ant1 bias in Remler recordings is the interobserver difference in the decotling process. Though 110 significant difference was found between observers, decoded results could differ by Illore tllan 5 rntnlig in 10% of recordings. l 'his may partly explain the scatter of Remler record- ings when colrlpared wit11 standard lnercury spllyg- monlanotneter recordings.2' This interobserver vari- ability, however, is no greater than for standard sphvgmon~anorneter recordings.I5
'l'he reliability of lieniler ambulatory recordings is reduced to a large extent by defects in the microphone lead. This also reduces the availability of the recorder as broken n~icropl~ones must be returned to the manu- facturer for repair, and recorders may lie idle for some time.
The Cardiodyne Sphygmolog is the simplest and most inexpensive complete ambulatory blood pressure systern available. l'hough on the market, it has not been previously evaluated. Accuracy studies showed that the Sl)liygmolog tended to underestin~ate diastolic prcssrlrc when compared with the I lawksley randoln- zero sl)l~yg~llol~ianometer. 'I'his difference, however, was small, and overall this device was reasonably accurate. Interdevice variability studies sliowed that one recorder gave higher recordings than the two other devices tested. This was the result of a zero drift of 3 to 4 rn111Hg in the pressure transducer.
lieliability of the Sphygrnolog recorder was low. ?'his was not the result of p w r technique by the patients as recordings with the Renller M2000 were successful. l 'he main derect, which appears easily correctable, is that the recording discs are displaced from the motor spindle when the niachine is in the uprigllt position during a~nbr~latory recording. Even if ' this were corrected, however, there were a large nunlbcr of artefacts in two of the remaining day record- ings. .I'liis nlay be because of oversensitivity of the recording system, which would explain the tendency to underestimate diastolic pressure, and the absence of any systern in the recorder for artefact suppression. Artefactual recording is a rnajor problem during auto- mated blood pressure recording,27 the commonest cause being movement of the patient's arm. This may be overcome by either using appropriate band lil1ers,2~2~ so that only sounds wit11 the frequency characteristics of Korotkoff are recorded, or by recording sounds occurring within a short period after the QKS complex of the electro~ardiogram.~ 31-33
Witli some systems7 34 the observer analyses the recorded data and artefacts are rejected on the basis of -' the occurrence of sounds in an expected position or sequence, or by rejecting recordings altogetller as undecodable. In contrast, the permanent record of the pressure measurements made by the Sphygmolog gives no indication whether pen marks are the result of Korotkoff sounds, arm ~novement, or extraneous sounds.
In conclusion, the Relnler MZOOO senliautomatic portable recorder is accurate in the measurement of blood pressure. Differences in the findings of previous studies can be explained by the different standards used for comparison. The reliability of the Remler M2OOO could be improved by strengthening the micro- phone lead attachment to the microcassette recorder. Tlie Spllygmolog is a reasonably accurate though un- reliable method of recording ambulatory blood pressure. Reliability is poor mainly because of a defect in the method used to retain the paper discs on the revolving spindle of the motor. The Cardiodyne Sphygmolog, as presently designed, cannot be recornmended for ambulatory blood pressure monitoring.
We acknowledge the support of the Royal College of Surgeons in Ireland and Ciba Laboratories, and Cardiodyne General, Inc., 455 Los Gatos Dlvd., Los (;atus, California, USA, for supl)lying us with three Spl~ygn~ologs for testing.
References
I Floras JS, Hassan MO, Sever PS, Jones JV, Osikowska B, Sleigl~t P. Cuff and ambulatory blood pressure in subjects
\villi cssctit~al Iiyl?crcc~isio~i. I.u?tc-rr 1981 ; i i : 107-9. 2 SokoIo!v hf, \X'crclc~:ir I), Kai~i IIK. Ili~ini;t~i /\'I..
Ilcl;c~io~isliil> het\vcc~i level of Iilos~d pressure rilcasr~rcd c:~sually and hv portalile rec~crrtlers aritl scvcrity ofco~npli- cations in essential h!perterision. Circrtlcrrioit 1966; 34: 279-98.
3 Julius S , Ellis CN. I'ascual r\V. cr (11. Iloriie tilood pressure dcterniination: value in bordcrli~ie(lat~ile\liyper- te~lsiori. J i \ ~ l l / \ 1974; 229: 663-6. - 4 Aymnn I), (;oldsliitle 1\11. Blood pressure dctertiiinatinns hy ~'atietits wit11 essential hy~ertensio~i . I. 'l'he difference I)rt\vec~i clinic ant1 Iion~c readings bcfore trcat~iierit. ~Itit.7 r\lctl Sri 1940; ZOO: 465-74.
5 Lauplilin K, Pislier 1.. Slierrard 1)J. Blood pressure reductions dr~rilig self-recorcling of Iiorne blood pressure. Aiir Ilcrrr1,7 1979; 98: 629-34.
6 l.:il~er MS. O'Hoylc (11'. Qr~inn (:. O'hlallcy K. 0'l)ricn 13'. I lo~iic liieasllretiicnt of blocid pressure: trai~ii~ig of relatives. Ir1\lrd,7 I981 : 74: 113-4.
7 l l i ~ ~ ~ l i a r i XI', Engel II'I', Bickford Al:. Portahle blood pressure recorder. Accr~racy and preliminary use in evalu- ating intra-daily variations in pressure. Am IlearrJ 1962; 63: 663-8.
8 I lo ra~i MJ. I'adget NE, Ken~iedv Ill.. Anibulatory blood pressure nionit,~ring: recent advances and clinical appli- catiolis. /\nr Ifcarr.7 1981; 101: 843-8.
9 1,ittlcr WA. Median lierve palsy-.I coniplication of hracliial artcry canr~lation. I'osr~rud AledJ 1976: 52, suppl 7: 110-1.
10 Kaftery llB. 'l'l~e nictliodologv of bltwd pressure rccord- ing. Ur.7 O'litt l'honnucol 1978: 6: 193-201.
I I 1,abarthe DK, llawkins CM, Remington RD. Evaluation of pcrforrnance of selected devices for measuring blood pressure. Am J Corfi l1973; 32: 546-53.
12 Ilose GA, llolland \V\V, Crowley EA. A sphygnioniano- meter for epidenliologis~s. Loirrc~ 1964: i: 296-300.
13 \Y:riglit DM, Dore CF. A randotn-zero spliyg~ilon~ario- meter. 1,uncer 1970; i: 337-8.
14 Rose ti. Standardisation of observers in blood pressure rneasurernent. Lancer 1965; i: 6 7 3 4 .
15 Association for the Advancetilent of Medical Instru~iien- tation. Standard for electronic or automated sl)liygrnonianorneters (propvsed) AAMI ESP-I). February revision. 1982. (Available on request from 1901 North Fort Myer Ilrive, Arlington VA 22209.)
16 Fitzgerald DJ, O'Malley K, O'Brien BI'. Assessing auto- mated blood pressure recorders (letter). Loi~cer 1981; ii: 993.
17 1)IIEW. Autoniatcd blood pressure nieasuring devices for tiiass screening. Publication No. (NIFI) 76-929. 1979.
18 Bcevers I)G, Bloxham CA, Backhouse CI, Lirn CC, Watson RIIS. l ' l~e Ke~illcr M2OOO semi-automatic blood pressure recorder (letter). Br Ifeorr J 1979; 42: 366.
I Y (:otvati It, Sokolow bl. I'erloffl). 'l'lic Reinler anil,ulatory I~loc~l pressure rccordinl: svste~n. Accuracy and relialiility clct~cr). IIrIlcrrrr.7 IYRO: 43: 715-6.
20 I'ong 1'1,. Wilson LI,, Richardson IJJ, O'llallora~i M. Kcriiler recorder (letter). Afec1.7 Ausr 1979; ii : 312.
21 (;orlld RA. Ilornung K. Kieso 11, Caslitnan I'hlM, Altrnan 1)G. Raftery ER. A validation of tlie Retiilcr A12000 and Avionic 1978 pressurorneter (abstract). Clir~ Sci 1981;61: 47p.
22 Scott AK, I'etrie JC. Asscssriient of the Re~iiler blood pressure recording system (abstract). UrJ G'litr Phun~racnl 1982; 13: 289-90.
23 1:itzgerald I)J, O'Mallev K. O'Urien El'. Inaccuracy of tlie 1,ontlon School of Ilygiene sphygmomanometer. 13r Alctl.7 1982; 284: 18-9.
24 IIreit SN, O'llourke MF. Conipariso~i of direct and illdirect ar~eri:il pressure Irieasurelnents in Iiospiraliscd patients. /\ttsr NZJ Me11 1974; 4: 485-91.
25 Ilollal~d WW, llunierfelt S. Measurement of blood- pressure: co~nparisotr of intra-arterial and cuff values. Ur Aled J 1964; ii: 1241-3.
26 Raftery 1 3 , Ward AP. 'rhe indirect method of recording hlcn~d pressure. Ccrrdim~asc Res 1968; 2: 2 10-8.
27 Kantrowitz P. A review of non-invasive b l t ~ d pressure ~neasurer~ient using a cuff, with particular respect to tnotion artefact. Hiotnediccll Ihgineerin~ 1973: 8: 480-1.
28 1,cwis PJ, Walker 1% Lee B, Qui~in ML. Indirect hlvnd- pressure nicasurelnent as part of a computer-controlled patient-riio~iitoring system. Biomed Compttr 7bch1rol 1976; 1: 39-44.
29 Katona Z, Bolvary G. Automatic indirect spliygmoman- onietry. Mion~cd I:'i~g 1975; 10: 405-10.
30 McCutclieon El', Kushmer RP. Korotkoff sounds. An experi~nental critique. Circ Res 1967; 20: 149-61.
31 Lagerwerff JM, Luce KS. Artifact suppression in indirect bl(n)d pressure measurements. Aerosp Med 1970; 41: 1157-61.
32 Steen SN, Grissman FL. A new system for the indirect nleasuretilent of systolic and diastolic blood pressures. Anesrh Ar~ulg (Cleve) 1962; 41: 39 1-6.
33 C;cddes LA, lloff FIE, Vallbona C, IIarrison ti, Spencer WA, Canzoneri J. Numerical indicatiori of indirect systolic and cfiastolic blood pressures and respiratory rate. Aitesrhesiology 1962; 25: 861-P.
34 Woltliins R, McAfoose D, llull D, Fischer J . Portable blcmd pressure measurements using tlie Korotkov sound technique-a study of measurement accuracy. BionredSci lt~srncn~ 1979; 15: 1 0 1 4 .
Requests for reprints 10 D r E O'Brien, l'he Blood Pressure Clinic, T h e Charitable Infirmary, Jervis Streer, Ditblin 1 .










![Accreditation Program: Ambulatory Health Care · PDF fileAccreditation Program: Ambulatory Health Care Chapter: National Patient Safety Goals Goal 1 Improve the accuracy of [patient]](https://img.pdfslide.net/doc/110x75/5a9dcb387f8b9a85318ca017/accreditation-program-ambulatory-health-care-program-ambulatory-health-care-chapter.jpg)







![[ ] Ambulatory Clinic.doc](https://img.pdfslide.net/doc/110x75/548171ffb4af9fbf0a8b463b/-ambulatory-clinicdoc.jpg)










