Embed Size (px)
Citation preview

Pediatr Blood Cancer 2006;46:773–779
Accuracy of Assessment of Distress, Anxiety, and Depressionby Physicians and Nurses in Adolescents Recently Diagnosed
With Cancer
Mariann Hedstrom, RN, PhD,1* Anders Kreuger, MD, PhD,2 Gustaf Ljungman, MD, PhD,2
Peter Nygren, MD, PhD,3 and Louise von Essen, PhD1
INTRODUCTION
Physicians and nurses are involved in medical treatment,
decision-making, and prioritizing care and use of health care
resources [1]. In pediatric care, it is thus imperative to findout
whether staff’s assessments of children’s health status agree
with the children’s assessments of their own health status.
When child-staff ratings of children’s health status have
been investigated, the focus has often been on associations. In
a study by Worchel et al. [2], children with cancer, their
parents, and nurses, rated the children’s levels of depression.
Neither child–parent nor child–nurse ratings were asso-
ciated, however, parent–nurse ratings were. Phipps et al. [3]
investigated the health related quality of life of children
undergoing bone marrow transplantation according to the
children, their parents, and nurses. Child–parent ratingswere
more associated than child–nurse and parent–nurse ratings.
Correlations were higher for somatic distress and activity
than for mood disturbances, compliance, and quality of
interactions. Demyttenaere et al. [4] investigated children’s
pain after surgery and showed that child–mother and child–
nurse ratings were not correlated, although mother–nurse
ratings were. Some investigators have investigated potential
differences between child and staff ratings of children’s
health status. Billson and Walker [5] investigated the health
status of survivors of childhood cancer according to the
survivors, their parents, and physicians. The physicians
identified fewer deficits than children and parents. Le Gales
et al. [6], investigated the health status among children on or
off treatment for brain tumors, according to the children, their
parents, and physicians. The parents underestimated the
children’s health status while physicians overestimated it. On
the basis of the few studies referred to above, it may be
speculated whether (a) parent–staff ratings of children’s
function and symptom are associated with each other but not
with the children’s ratings and (b) staff tend to underestimate
problems compared to children’s ratings. If the first specu-
lation holds true, and as parents often act as their child’s
spokespeople and communicate the child’s needs to medical
staff [7,8], there are implications for more direct child–staff
communication. This seems particularly important for adoles-
cents as Chang and Yeh [9] recently reported that parent-proxy
reports on adolescent health status provided significantly
different information than adolescent self-reports among
Background. As staff members prioritize medical resources forpatients, it is imperative to find out whether their assessments ofpatients’ health status agree with patients’ assessments. The degree towhich physicians and nurses can identify the distress, anxiety, anddepression experienced by adolescents recently diagnosed withcancer was examined here. Procedure. Adolescents undergoingchemotherapy (13–19 years, n¼53), physicians (n¼ 48), and nurses(n¼53) completed a structured telephone interview, 4–8 weeksafter diagnosis or relapse, investigating disease and treatment-relateddistress, anxiety, and depression. Results. The accuracy of staffratings of physical distress could be considered acceptable.However, problems of a psychosocial nature, which were frequentlyoverestimated, were difficult for staff to identify. Staff underestimatedthe distress caused by mucositis and worry about missing schoolmore than they overestimated distress. These aspects were some of
the most prevalent and overall worst according to the adolescents.Both physicians and nurses overestimated levels of anxiety anddepression. Nurses tended to show higher sensitivity than physiciansfor distress related to psychosocial aspects of distress, whilephysicians tended to show higher accuracy than nurses for physicaldistress. Conclusions. Staff was reasonably accurate at identifyingphysical distress in adolescents recently diagnosed with cancerwhereas psychosocial problems were generally poorly identified.Thus, the use of staff ratings as a ‘‘test’’ to guide specific supportseems problematic. Considering that the accuracy of staff ratingsoutside a research study is probably lower, identification of andaction taken on adolescent problems in relation to cancer diagnosisand treatment need to rely on direct communication. Pediatr BloodCancer 2006;46:773–779. � 2005 Wiley-Liss, Inc.
Key words: adolescents; anxiety; cancer; depression; distress; staff assessments
� 2005 Wiley-Liss, Inc.DOI 10.1002/pbc.20693
——————1Department of Public Health and Caring Sciences, Section of Caring
Sciences, Uppsala University, Uppsala, Sweden; 2Department of
Women’s and Children’s Health, Unit for Pediatric Hematology and
Oncology, University Children’s Hospital, Uppsala, Sweden;3Department of Oncology, Radiology and Clinical Immunology,
University Hospital, Uppsala, Sweden
Grant sponsor: Swedish Children’s Cancer Foundation; Grant sponsor:
Swedish Cancer Society.
*Correspondence to: Mariann Hedstrom, Department of Public Health
and Caring Sciences, Section of Caring Sciences, Uppsala University,
Dag Hammarskiolds v.10 B, Uppsala Science Park, S-751 83 Uppsala,
Sweden. E-mail: [email protected]
Received 10 February 2005; Accepted 10 October 2005

adolescents with cancer. If the last speculation holds true, it
may have serious consequences, as problems not acknowl-
edged may go without sufficient attention and treatment. In
adult care, inadequate pain management has been shown as a
possible consequence of disagreement between patient–
physician ratings of pain intensity in adult cancer patients [10].
The focus of the present study was to examine the degree
to which physicians and nurses can accurately identify the
distress, anxiety, and depression experienced by adolescents
with cancer. In this study, we take the adolescent’s assess-
ments as the point of reference. The aims were to compare
the ratings of physicians and nurses with the ratings of
adolescents, recently diagnosed with cancer. The study
evaluated ratings of the presence and levels of disease and
treatment-related aspects of distress, which aspects of dis-
tress were experienced as the worst for the adolescents as
well as the presence and levels of anxiety and depression.
METHODS
This report presents results based on data collected
4–8 weeks after diagnosis from adolescents, nurses, and
physicians, recruited from three of the six pediatric oncology
centers in Sweden, from February 1999 in Uppsala and from
March 2000 in Lund, and Umea until September 2003.
Participants
Swedish speaking adolescents (13–19 years of age),
diagnosed with a malignancy or relapse (after a minimum of
1 year post treatment), treated with chemotherapy at one of
the centers, and considered emotionally, cognitively, and
physically capable of participating by the project coordinat-
ing nurse or the treating physician at the center where the
adolescent was treated and cared for, were eligible. Of the
97 adolescents diagnosed with cancer and treated with chemo-
therapy, 18 were excluded for the following reasons: 4 spoke
very little Swedish, 7 were considered too physically or
cognitively affected by the disease or a neurological comor-
bidity (5 of whom died shortly after the diagnosis), and 7 were
diagnosed at the pediatric oncology centers, but thereafter
treated and cared for at a local hospital. Of the 79 adolescents
who met the eligibility criteria, 56 agreed to participate. Two
adolescents became too ill before they could be interviewed,
and one could not be found due to administrative failure.
Hence, 67% (53/79) of the eligible adolescents participated,
their characteristics are presented in Table I.
One physician and one nurse/nurse assistant were to be
interviewed for each participating adolescent. Twenty-six
physicians were interviewed concerning 48 adolescents
(5 interviews were not performed as the workload on the ward
did not allow any time for physicians to participate), with a
range of 1–7 interviews per physician (mean 1.8, SD 1.5).
Their mean age was 45 years (range 28–62), 9 were women
and 17 men. The physicians had worked in health care for an
average of 17 years (range 4–35), and with adolescents with
cancer for an average of 8 years (range 2 months–31 years).
Forty-four nurses/nurse assistants were interviewed con-
cerning 53 adolescents, with a range of 1–3 interviews per
nurse/nurse assistant (mean 1.2, SD 0.5). Thirty-six were
registered nurses and 8 were nurse assistants (non-registered
staff with 2 years of education). In the following, nurses and
nurse assistants will be referred to as nurses. The mean age
was 37 years (range 25–59), 38 were women and 6 men. The
nurses had worked in health care for an average of 14 years
(range 1–35) andwith adolescentswith cancer for an average
of 7 years (range 3 months–30 years).
Procedure
Ethical approval was obtained from the local ethics
committees at the faculties of medicine. All eligible
adolescents and their parents received written information
about the study from a coordinating nurse at each center
approximately 3 weeks after diagnosis. After a few days, the
coordinating nurse contacted the adolescent and asked him/
her if he/she was willing to participate, and asked the parents
for consent if the adolescent was �17 years. Thereafter, one
of the nurses and one of the physicians who knew the
adolescents the best, were matched and then interviewed as
close in time to the adolescent interview as possible. Data
was collected by structured telephone interviews 4–8 weeks
after the adolescent’s cancer diagnosis. All adolescents had
started chemotherapy at the time of data collection. The
adolescents received a small present in return for their
participation.
Measures
Presence, levels, and worst aspects of disease and
treatment-related distress. A structured interview-guide,
developed for the study, was used to investigate presence
Pediatr Blood Cancer DOI 10.1002/pbc
TABLE I. Demographic and Clinical Characteristics of theAdolescents (n¼ 53)
Study site
Lund 17
Umea 17
Uppsala 19
Sex
Male 36
Female 17
Age
13–14 28
15–19 25
Diagnosis
CNS-tumor 3
Ewing sarcoma 3
Leukemia 18
Lymphoma 16
Osteosarcoma 8
Other 5
Relapse
No 48
Yes 5
774 Hedstrom et al.

and/or levels of, and worst aspects of distress. The aspects
were identified through semi-structured interviews with
adolescents with cancer and nurses caring for them [11,12].
The aspects were categorized as physical concerns, personal
changes, feelings of alienation and disease, and treatment-
related worries. For 16 aspects, presence and levels were
identified through response alternatives using a six-grade
verbal scale, range ‘‘not at all’’ to ‘‘very much,’’ coded 0–5.
For four aspects presence/absence was identified through a
dichotomized yes/no alternative. Questions referred to the
time since diagnosis. Physicians and nurses answered a staff
version, which included the same items, but with questions
directed to the staff, asking them to reply what they thought
their matched adolescent had experienced since diagnosis.
For all aspects, staff had the possibility of answering ‘‘I don’t
know.’’ Finally, the nurses and physicians were asked to
identify the aspect of distress that had been the worst for the
adolescent since diagnosis. These respondents had the
possibility of reporting more than one aspect.
Presence and levels of anxiety and depression. The
hospital anxiety and depression scale (HADS) [13] was used
to investigate presence and levels of anxiety and depression.
HADS refers to the preceding week and consists of two
subscales, one assessing anxiety (HADS-A, seven items) and
one depression (HADS-D, seven items). Answers are given
on a four-grade verbal scale, coded 0–3. Subscale scores
range from 0 (no distress) to 21 (maximum distress).
Physicians and nurses answered a staff version [14], which
included the same items, but with questions directed to the
staff, asking them to reply as to how they thought their
matched adolescent had felt during the past week. TheHADS
has been found to possess adequate test-retest reliability and
sensitivity for use with adolescents [15], and has been
reported to correctly identify a majority of clinical cases of
psychiatric mood disorders among adolescents with cancer
as identified by a psychiatric evaluation [16].
Background data. Respondents were asked to report
demographic data and the coordinating nurse collected
clinical data on the adolescents from the medical records.
Data Analysis
Adolescent–staff agreement with regard to disease
and treatment-related distress. Prevalence was defined as
‘‘moderately,’’ ‘‘quite a lot,’’ or ‘‘very much’’ answers to
questions with continuous and ‘‘yes’’ answers to questions
with dichotomized response alternatives by adolescents.
Sensitivity was defined as the proportion (%) of staff being
able to detect an aspect as distressing, that is, answering
‘‘moderately,’’ ‘‘quite a lot,’’ or ‘‘very much’’ for continuous
questions, and ‘‘yes’’ to questions with dichotomized
response alternatives, when the adolescents also provided
any of these answers. Specificity was defined as the
proportion (%) of staff being able to detect an aspect as not
distressing, that is, answering ‘‘somewhat,’’ ‘‘just a little,’’ or
‘‘not at all’’ for continuous and ‘‘no’’ to questions with
dichotomized response alternatives when the adolescents
also provided any of these answers. Calculations of
sensitivity and specificity are based on an idea presented by
Brunelli et al. [1]. Overestimation was defined as staff giving
a rating more than one score above and underestimation as a
ratingmore than one score below the rating by the adolescent.
Calculations of over- and underestimation could not be
performed for questions with dichotomized response alter-
natives. Perceptions of worst aspects of distress are reported
with descriptive statistics.
Adolescent–staff agreement with regard to anxiety
and depression. For calculations of prevalence of anxiety
and depression, cut-off points indicating a potential clinical
casewere employed for scores�9 for anxiety (HADS-A) and
�7 for depression (HADS-D), as recommended for use with
adolescents [15]. Sensitivity and specificity were calculated
using these cut-off points. For calculations of correlations,
Pearson product moment correlation coefficients (PPM)
were calculated. For calculations of differences, paired, two-
tailed t-tests were used. Missing values for HADS were
substituted by the mean value of the specific respondent’s
answers to the remaining scale items, provided that six of the
seven items had been answered. This procedure was
performed for nine missing values. If more than one item
per scale was missing, that subscale was treated as missing
data in the prevalence, PPM and t-test calculations. This was
the case for one depression and one anxiety subscale for
adolescents, four depression and four anxiety subscales for
physicians, and one depression and three anxiety subscales
for nurses. Eight physicians and three nurses were not asked
to answer HADS as more than 1 week had elapsed since they
had met the adolescent.
RESULTS
Adolescent–Staff Agreement on the Presence,Levels, and Worst Aspects of Distress
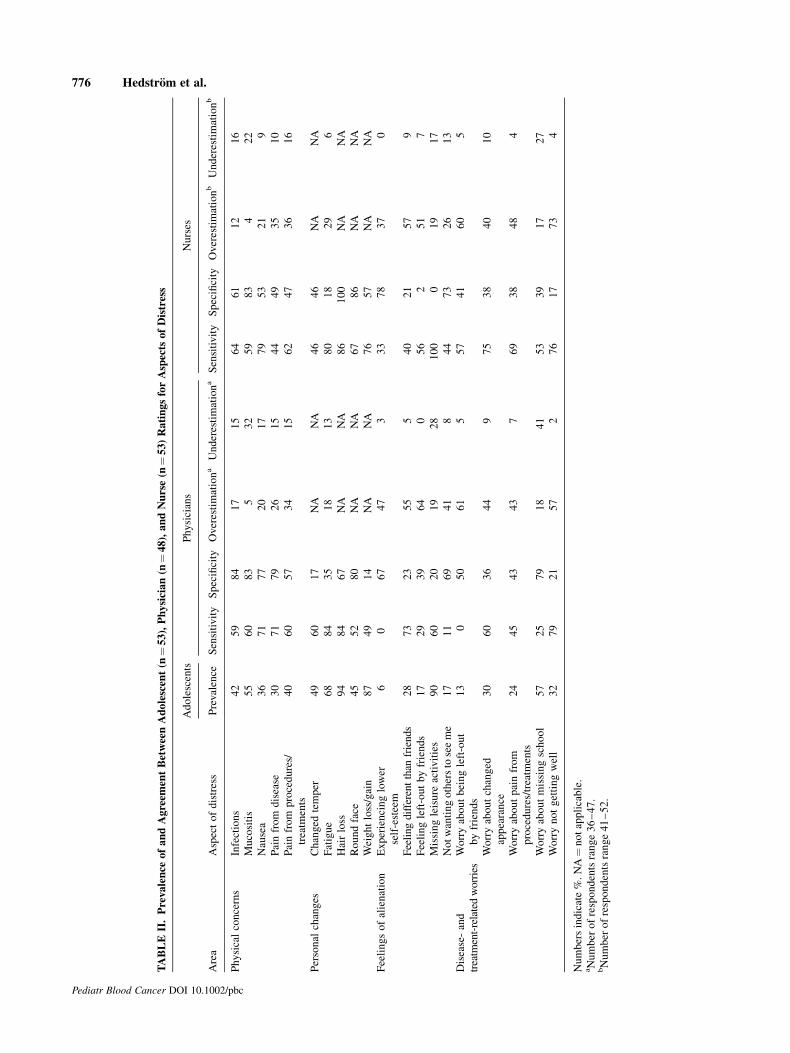
Physicians rated six aspects with a sensitivity and speci-
ficity close to or above 60%: infections, mucositis, nausea,
pain from disease, pain from procedures/treatments, and hair
loss (Table II). Nurses rated five aspects with a sensitivity and
specificity close to or above 60%: infections, mucositis,
nausea, hair loss, round face (related to steroid use), and
weight loss/gain. For most of the remaining aspects, staff
showed a higher sensitivity than specificity. Physicians under-
estimated levels of distress for more adolescents than they
overestimated it with regard tomucositis, worry about missing
school, and missing leisure activities. Nurses underestimated
levels of distressmore than they overestimated itwith regard to
mucositis, worry about missing school, and infections.
Adolescent distress items with a prevalence of >50%
were hair loss, missing leisure activities, weight loss/gain,
fatigue, worry aboutmissing school, andmucositis (Table II).
Two of these aspects were among the three for which nurses
Pediatr Blood Cancer DOI 10.1002/pbc
Distress Among Adolescents With Cancer 775
Pediatr Blood Cancer DOI 10.1002/pbc
TABLEII.Prevalence
ofandAgreem
entBetweenAdolescent(n
¼53),Physician(n
¼48),andNurse(n
¼53)RatingsforAspects
ofDistress
Area
Aspectofdistress
Adolescents
Physicians
Nurses
Prevalence
Sensitivity
Specificity
Overestimationa
Underestimationa
Sensitivity
Specificity
Overestimationb
Underestimationb
Physicalconcerns
Infections
42
59
84
17
15
64
61
12
16
Mucositis
55
60
83
532
59
83
422
Nausea
36
71
77
20
17
79
53
21
9
Painfrom
disease
30
71
79
26
15
44
49
35
10
Painfrom
procedures/
treatm
ents
40
60
57
34
15
62
47
36
16
Personal
changes
Changed
temper
49
60
17
NA
NA
46
46
NA
NA
Fatigue
68
84
35
18
13
80
18
29
6
Hairloss
94
84
67
NA
NA
86
100
NA
NA
Roundface
45
52
80
NA
NA
67
86
NA
NA
Weightloss/gain
87
49
14
NA
NA
76
57
NA
NA
Feelingsofalienation
Experiencinglower
self-esteem
60
67
47
333
78
37
0
Feelingdifferentthan
friends
28
73
23
55
540
21
57
9
Feelingleft-outbyfriends
17
29
39
64
056
251
7
Missingleisure
activities
90
60
20
19
28
100
019
17
Notwantingotherstoseeme
17
11
69
41
844
73
26
13
Disease-and
treatm
ent-relatedworries
Worryaboutbeingleft-out
byfriends
13
050
61
557
41
60
5
Worryaboutchanged
appearance
30
60
36
44
975
38
40
10
Worryaboutpainfrom
procedures/treatm
ents
24
45
43
43
769
38
48
4
Worryaboutmissingschool
57
25
79
18
41
53
39
17
27
Worrynotgettingwell
32
79
21
57
276
17
73
4
Numbersindicate%.NA¼notapplicable.
aNumber
ofrespondentsrange36–47.
bNumber
ofrespondentsrange41–52.
776 Hedstrom et al.

tended to underestimate distress, and three aspects were
among those for which physicians tended to underestimate
distress. Thus, members of staff tend to underestimate
distress caused by some of the aspects that distress most
adolescents. A similar pattern emerges for the worst aspects
of distress according to adolescents. The aspects identified as
the worst are presented in Table III. Respondents report a
variety of aspects as the worst.Worry about not getting well
wasmost oftenmentioned, especially by physicians. The two
aspects for which both nurses and physicians underestimated
distress (Table II) were among the six aspects that
adolescentsmost frequently identified as theworst:mucositis
and worry about missing school (Table III).
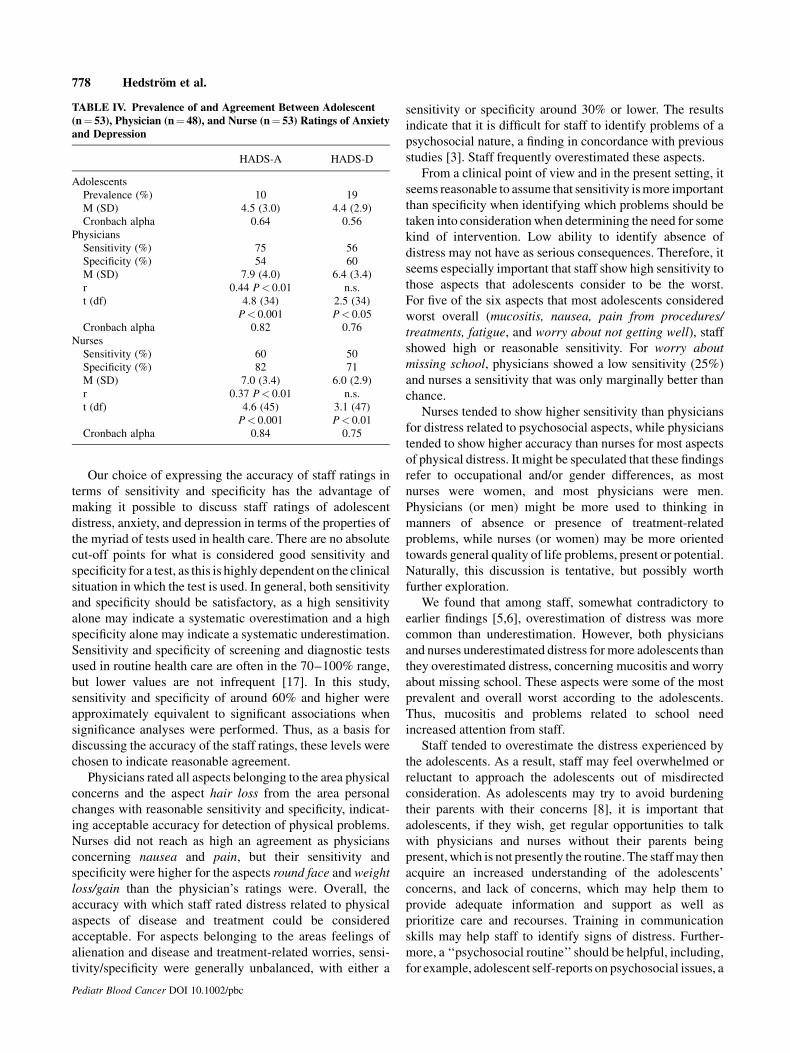
Adolescent–Staff Agreement on the Prevalenceand Levels of Anxiety and Depression
Five adolescents (10%) were identified as potential clin-
ical cases for anxiety and 10 (19%) were identified as
potential clinical cases for depression. For anxiety, physician
ratings were more accurate for the presence (75%) than for
the absence (54%) of adolescent self-reported anxiety
whereas nurses were more accurate for the absence (82%)
than for the presence (60%) of adolescent self-reported
anxiety (Table IV). Staff ratings of depression were more
accurate for the absence (60%, 71%) than for the presence
(56%, 50%) of adolescent self-reported depression. There
were statistically significant correlations between staff and
adolescents concerning level of anxiety. However, staff
reported significantly higher levels of anxiety and depression
than did the adolescents (Table IV).
DISCUSSION
As cancer in adolescents is uncommon, consists of a
multitude of diagnoses and is treated in numerousways, itwas
difficult to recruit a homogenous study group. In our study, the
adolescents were heterogeneous in terms of diagnosis, but
relatively homogenous in terms of time since diagnosis, age
group, and treatment. Five of the included adolescents had
relapses. It could be speculated that theywere better known to
the staff than the newly diagnosed adolescents were. Avisual
inspection of a separate data analysis for the relapsed
adolescents does not support this idea. For HADS, a visual
inspection of mean differences showed greater differences
between relapsed adolescents and staff than between newly
diagnosed adolescents and staff. However, it seems reason-
able to assume that adolescents with a relapse are in need of
special clinical and research attention. Another methodo-
logical aspect to consider is that participating adolescents and
staff, by necessity, were not ‘‘blinded,’’ that is, they were
informed about the aims and outlines of the study. This
awareness could speculatively tend to increase sensitivity and
overestimation. Thus, the results might not be fully
representative, which should be taken into consideration
when making conclusions for routine health care.
Pediatr Blood Cancer DOI 10.1002/pbc
TABLE III. Worst Aspects of Distress According to Adolescents (n¼ 53), Physicians (n¼ 48), and Nurses (n¼ 53)
Area Aspect of distress Adolescents Physicians Nurses
Physical concerns Infections 1 0 1
Mucositis 7 0 6
Nausea 7 1 3
Pain from disease 0 2 4
Pain from procedures/treatment 9 5 5
Other 0 0 1
Personal changes Changed temper 0 0 0
Fatigue 5 1 4
Hair loss 3 2 1
Round face 0 0 0
Weight loss/gain 1 0 0
Other 2 0 0
Feelings of alienation Experiencing lower self-esteem 0 0 0
Feeling different than friends 0 2 0
Feeling left-out by friends 2 0 1
Missing leisure activities 5 2 0
Not wanting others to see me 0 0 0
Other 1 1 4
Disease- and treatment-related worries Worry about being left-out by friends 0 0 0
Worry about changed appearance 0 0 0
Worry about pain from procedures/treatment 0 1 1
Worry about missing school 6 0 0
Worry about not getting well 11 32 23
Other 0 1 1
Don’t know 0 0 2
Numbers in columns refer to number of respondents mentioning each aspect as theworst. Respondents could report more than one aspect as theworst.
Distress Among Adolescents With Cancer 777
Our choice of expressing the accuracy of staff ratings in
terms of sensitivity and specificity has the advantage of
making it possible to discuss staff ratings of adolescent
distress, anxiety, and depression in terms of the properties of
the myriad of tests used in health care. There are no absolute
cut-off points for what is considered good sensitivity and
specificity for a test, as this is highly dependent on the clinical
situation in which the test is used. In general, both sensitivity
and specificity should be satisfactory, as a high sensitivity
alone may indicate a systematic overestimation and a high
specificity alone may indicate a systematic underestimation.
Sensitivity and specificity of screening and diagnostic tests
used in routine health care are often in the 70–100% range,
but lower values are not infrequent [17]. In this study,
sensitivity and specificity of around 60% and higher were
approximately equivalent to significant associations when
significance analyses were performed. Thus, as a basis for
discussing the accuracy of the staff ratings, these levels were
chosen to indicate reasonable agreement.
Physicians rated all aspects belonging to the area physical
concerns and the aspect hair loss from the area personal
changes with reasonable sensitivity and specificity, indicat-
ing acceptable accuracy for detection of physical problems.
Nurses did not reach as high an agreement as physicians
concerning nausea and pain, but their sensitivity and
specificity were higher for the aspects round face and weight
loss/gain than the physician’s ratings were. Overall, the
accuracy with which staff rated distress related to physical
aspects of disease and treatment could be considered
acceptable. For aspects belonging to the areas feelings of
alienation and disease and treatment-related worries, sensi-
tivity/specificity were generally unbalanced, with either a
sensitivity or specificity around 30% or lower. The results
indicate that it is difficult for staff to identify problems of a
psychosocial nature, a finding in concordance with previous
studies [3]. Staff frequently overestimated these aspects.
From a clinical point of view and in the present setting, it
seems reasonable to assume that sensitivity ismore important
than specificity when identifying which problems should be
taken into considerationwhen determining the need for some
kind of intervention. Low ability to identify absence of
distress may not have as serious consequences. Therefore, it
seems especially important that staff show high sensitivity to
those aspects that adolescents consider to be the worst.
For five of the six aspects that most adolescents considered
worst overall (mucositis, nausea, pain from procedures/
treatments, fatigue, and worry about not getting well), staff
showed high or reasonable sensitivity. For worry about
missing school, physicians showed a low sensitivity (25%)
and nurses a sensitivity that was only marginally better than
chance.
Nurses tended to show higher sensitivity than physicians
for distress related to psychosocial aspects, while physicians
tended to show higher accuracy than nurses for most aspects
of physical distress. It might be speculated that these findings
refer to occupational and/or gender differences, as most
nurses were women, and most physicians were men.
Physicians (or men) might be more used to thinking in
manners of absence or presence of treatment-related
problems, while nurses (or women) may be more oriented
towards general quality of life problems, present or potential.
Naturally, this discussion is tentative, but possibly worth
further exploration.
We found that among staff, somewhat contradictory to
earlier findings [5,6], overestimation of distress was more
common than underestimation. However, both physicians
and nurses underestimated distress for more adolescents than
they overestimated distress, concerning mucositis and worry
about missing school. These aspects were some of the most
prevalent and overall worst according to the adolescents.
Thus, mucositis and problems related to school need
increased attention from staff.
Staff tended to overestimate the distress experienced by
the adolescents. As a result, staff may feel overwhelmed or
reluctant to approach the adolescents out of misdirected
consideration. As adolescents may try to avoid burdening
their parents with their concerns [8], it is important that
adolescents, if they wish, get regular opportunities to talk
with physicians and nurses without their parents being
present, which is not presently the routine. The staffmay then
acquire an increased understanding of the adolescents’
concerns, and lack of concerns, which may help them to
provide adequate information and support as well as
prioritize care and recourses. Training in communication
skills may help staff to identify signs of distress. Further-
more, a ‘‘psychosocial routine’’ should be helpful, including,
for example, adolescent self-reports on psychosocial issues, a
Pediatr Blood Cancer DOI 10.1002/pbc
TABLE IV. Prevalence of and Agreement Between Adolescent(n¼ 53), Physician (n¼ 48), and Nurse (n¼ 53) Ratings of Anxietyand Depression
HADS-A HADS-D
Adolescents
Prevalence (%) 10 19
M (SD) 4.5 (3.0) 4.4 (2.9)
Cronbach alpha 0.64 0.56
Physicians
Sensitivity (%) 75 56
Specificity (%) 54 60
M (SD) 7.9 (4.0) 6.4 (3.4)
r 0.44 P< 0.01 n.s.
t (df) 4.8 (34)
P< 0.001
2.5 (34)
P< 0.05
Cronbach alpha 0.82 0.76
Nurses
Sensitivity (%) 60 50
Specificity (%) 82 71
M (SD) 7.0 (3.4) 6.0 (2.9)
r 0.37 P< 0.01 n.s.
t (df) 4.6 (45)
P< 0.001
3.1 (47)
P< 0.01
Cronbach alpha 0.84 0.75
778 Hedstrom et al.

routine assessment or interview by physicians or nurses, or
psychological assessments.
Worry about not getting well was the distress item most
often mentioned as the overall worst by adolescents,
physicians, and nurses. Still, the number of adolescents
mentioning the problem was low (n¼ 11) compared to
physicians (n¼ 32) and nurses (n¼ 23). This is a result that
indicates that even though many adolescents consider the
threat to their life to be very distressing, it is not as
outstanding for asmany adolescents as staff seems to believe.
Rather, adolescents’ distress seems to be more evenly
distributed among the distress areas.
The low Cronbach alpha values for the adolescent ratings
ofHADS-A andHADS-D (0.64 and 0.56, respectively)make
the interpretation of the staff assessments for HADS difficult
and tentative. As Eiser and Morse have pointed out, if the
reliability of a measure is low, agreement between raters can
never be high [18]. Both physician and nurse ratings
correlated lowly, but significantly, with adolescent ratings
on HADS-A, indicating that staff can identify some of those
adolescents who are more or less worried, even if they
overestimate the level of anxiety. For depression, however,
staff ratings did not correlate with the adolescent ratings. A
possible implication of this finding is that depression among
adolescents with cancer may go unidentified and thus
untreated.
In conclusion, staff members seem to be reasonably
accurate at identifying physical distress in adolescents
undergoing chemotherapy for newly diagnosed cancer.
However, since these adolescents frequently suffer from a
number of disease and treatment-related aspects poorly
identified by the staff, the use of staff ratings as a ‘‘test’’ to
guide specific support seems inaccurate. The accuracy of
staff ratings outside a research study might be even lower.
Thus, identification of, and action taken on, adolescent
problems in this situation needs to rely on direct commu-
nication between adolescents and staff.
ACKNOWLEDGMENT
We would like to express our sincere gratitude to the
adolescents, physicians, and nurses who agreed to share their
experiences with us.
REFERENCES
1. Brunelli C, Costantini M, Di Giulio P, et al. Quality-of-life
evaluation: When do terminal cancer patients and health-care
providers agree? J Pain Symptom Manage 1998;15:151–158.
2. Worchel FF,NolanBF,WillsonVL, et al. Assessment of depression
in children with cancer. J Pediatr Psychol 1988;13:101–112.
3. Phipps S, DunavantM, JayawardeneD, et al. Assessment of health-
related quality of life in acute in-patient settings: Use of the BASES
instrument in children undergoingbonemarrow transplantation. Int
J Cancer Suppl 1999;12:18–24.
4. Demyttenaere S, FinleyGA, JohnstonCC, et al. Pain treatment thres-
holds in children after major surgery. Clin J Pain 2001;17:173–177.
5. Billson A, Walker DA. Assessment of health status in survivors of
cancer. Arch Disease Child 1994;70:200–204.
6. Le Gales C, Costet N, Gentet JC, et al. Cross-cultural adaptation of
a health status classification system in children with cancer. First
results of the French adaptation of the Health Utilities IndexMarks
2 and 3. Int J Cancer Suppl 1999;12:112–118.
7. Eiser C, Morse R. The measurement of quality of life in children:
Past and future perspectives. JDevBehav Pediatr 2001;22:248–256.
8. Parsons SK, Barlow SE, Levy SL, et al. Health-related quality of
life in pediatric bone marrow transplant survivors: According to
whom? Int J Cancer Suppl 1999;12:46–51.
9. Chang PC, Yeh CH. Agreement between child self-report and
parent proxy-report to evaluate quality of life in children with
cancer. Psychooncology 2005;14:125–134.
10. Cleeland CS, Gonin R, Hatfield AK, et al. Pain and its treatment in
outpatientswithmetastatic cancer.NEngl JMed1994;330:592–596.
11. Hedstrom M, Haglund K, Skolin I, et al. Distressing events for
children and adolescents with cancer. Child, parent, and nurse
perceptions. J Pediatr Oncol Nurs 2003;20:120–132.
12. Hedstrom M, Skolin I, von Essen L. Distressing and positive
experiences and important aspects of care for adolescents treated
for cancer. Adolescent and nurse perceptions. Eur J Oncol Nurs
2004;8:6–17; discussion 18-19.
13. ZigmondAS, Snaith RP. The hospital anxiety and depression scale.
Acta Psychiatr Scand 1983;67:361–370.
14. von Essen L, Burstrom L, Sjoden PO. Perceptions of caring
behaviors and patient anxiety and depression in cancer patient-staff
dyads. Scand J Caring Sci 1994;8:205–212.
15. White D, Leach C, Sims R, et al. Validation of the hospital anxiety
and depression scale for usewith adolescents. Br J Psychiatry 1999;
175:452–454.
16. Berard RM, Boermeester F. Psychiatric symptomatology in
adolescents with cancer. Pediatr Hematol Oncol 1998;15:211–221.
17. Alberg AJ, Park JW, Hager BW, et al. The use of ‘‘overall
accuracy’’ to evaluate the validity of screening or diagnostic tests.
J Gen Intern Med 2004;19:460–465.
18. Eiser C, Morse R. Quality-of-life measures in chronic diseases of
childhood. Health Technol Assess 2001;5:1–157.
Pediatr Blood Cancer DOI 10.1002/pbc
Distress Among Adolescents With Cancer 779