Embed Size (px)
DESCRIPTION
ACL Injuries In the Skeletally Immature. Jason W. Folk, MD Steadman Hawkins Clinic of the Carolinas February 2012. Disclosures. Consultant Smith & Nephew Endoscopy. Objectives. - PowerPoint PPT Presentation
Citation preview
ACL Injuries In the ACL Injuries In the Skeletally ImmatureSkeletally Immature
Jason W. Folk, MDJason W. Folk, MDSteadman Hawkins Clinic of the Steadman Hawkins Clinic of the
CarolinasCarolinasFebruary 2012February 2012
Consultant Smith & Nephew Consultant Smith & Nephew EndoscopyEndoscopy
DisclosuresDisclosures
ObjectivesObjectives Describe the epidemiology, Describe the epidemiology,
pathophysiology, and treatment pathophysiology, and treatment principles of ACL injuries in skeletally principles of ACL injuries in skeletally immature patientsimmature patients
ACL Injuries: ACL Injuries: IntroductionIntroduction
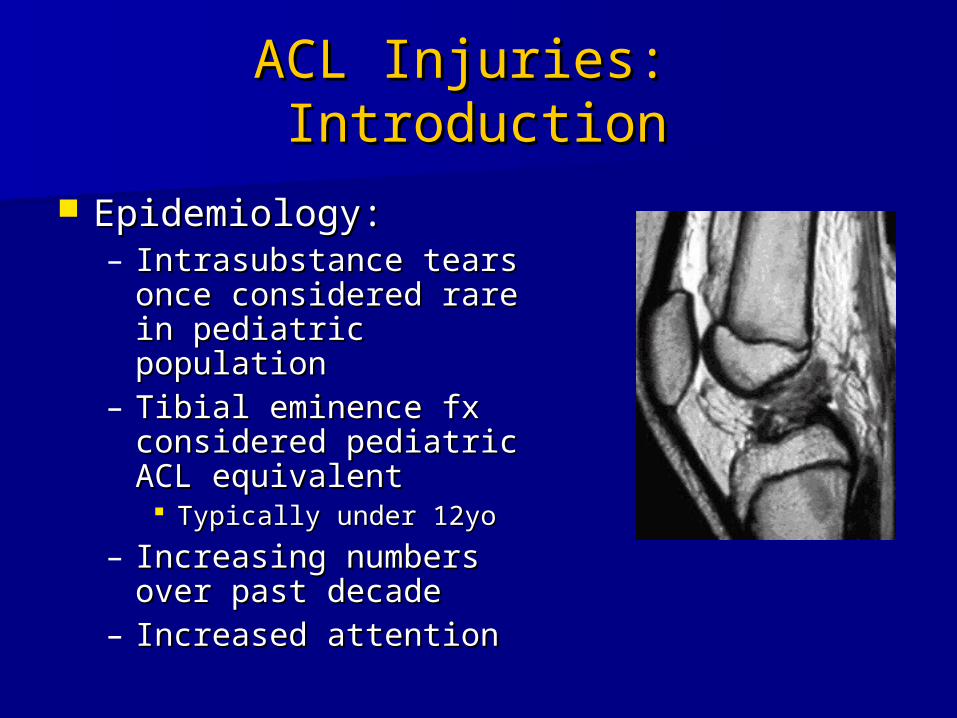
Epidemiology: Epidemiology: – Intrasubstance tears once Intrasubstance tears once
considered rare in considered rare in pediatric populationpediatric population
– Tibial eminence fx Tibial eminence fx considered pediatric ACL considered pediatric ACL equivalentequivalent Typically under 12yoTypically under 12yo
– Increasing numbers over Increasing numbers over past decadepast decade
– Increased attentionIncreased attention

55
ACL Injuries: ACL Injuries: IntroductionIntroduction
Reasons for increased Reasons for increased incidence:incidence:– Increased participation in Increased participation in
sportssports– Higher competitive levels Higher competitive levels
early onearly on– Increased awareness of Increased awareness of
injuryinjury– Decreased conditioningDecreased conditioning
ACL Injuries: ACL Injuries: IntroductionIntroduction
ACL Injuries in Soccer Players 5-18 ACL Injuries in Soccer Players 5-18 (Shea, et al. JPO 2004.)(Shea, et al. JPO 2004.)– Based on insurance data from 6 million Based on insurance data from 6 million
player-yearsplayer-years– 6.7% of total injury claims6.7% of total injury claims– 30.8% of all knee injury claims30.8% of all knee injury claims
True incidence unknownTrue incidence unknown
ACL Injuries: ACL Injuries: IntroductionIntroduction
Differences in pediatric populationDifferences in pediatric population– Often lack fully developed complex Often lack fully developed complex
motor skillsmotor skills– May have temporary decline in motor May have temporary decline in motor
and balance during pubertyand balance during puberty– Open physesOpen physes– Higher strength of ligaments vs. bone-Higher strength of ligaments vs. bone-
ligament interfaceligament interface
ACL Injuries:ACL Injuries:DiagnosisDiagnosis
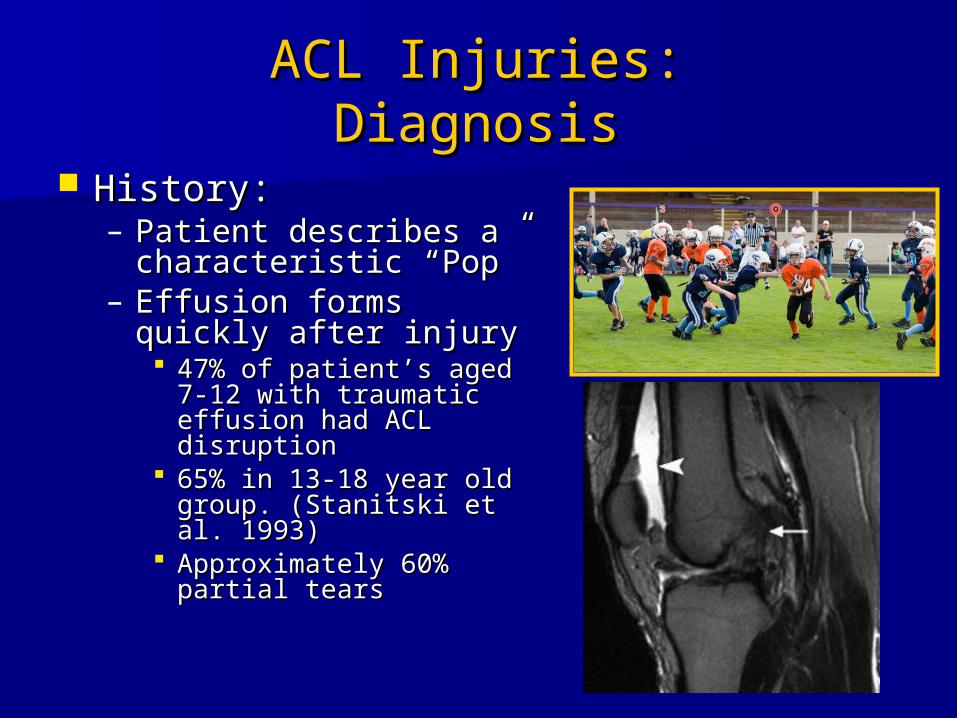
History: History: – Patient describes a Patient describes a
characteristic “Pop”characteristic “Pop”– Effusion forms quickly Effusion forms quickly
after injuryafter injury 47% of patient’s aged 7-47% of patient’s aged 7-
12 with traumatic effusion 12 with traumatic effusion had ACL disruptionhad ACL disruption
65% in 13-18 year old 65% in 13-18 year old group. (Stanitski et al. group. (Stanitski et al. 1993)1993)
Approximately 60% partial Approximately 60% partial tearstears
ACL Injuries: ACL Injuries: DiagnosisDiagnosis
Physical ExamPhysical Exam– Often more difficult in kids than adultsOften more difficult in kids than adults
Acute painAcute pain Frightened Frightened Unable to relaxUnable to relax
– Examine uninjured leg for baseline Examine uninjured leg for baseline laxity or congenital absence of ACLlaxity or congenital absence of ACL
ACL Injuries: ACL Injuries: ImagingImaging
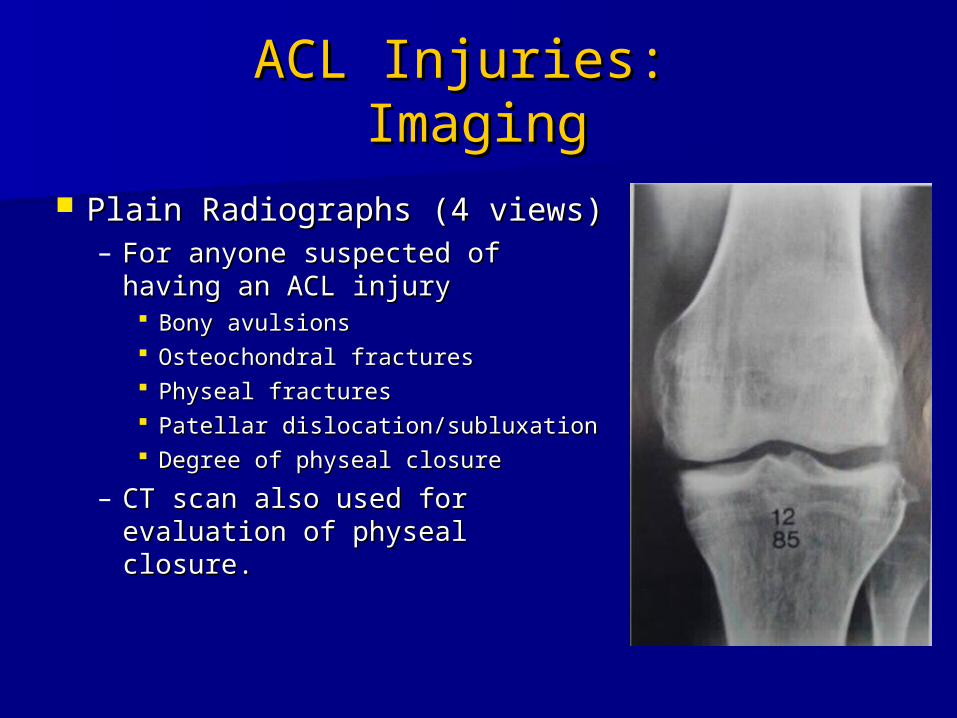
Plain Radiographs (4 views)Plain Radiographs (4 views)– For anyone suspected of For anyone suspected of
having an ACL injuryhaving an ACL injury Bony avulsionsBony avulsions Osteochondral fracturesOsteochondral fractures Physeal fracturesPhyseal fractures Patellar dislocation/subluxationPatellar dislocation/subluxation Degree of physeal closureDegree of physeal closure
– CT scan also used for CT scan also used for evaluation of physeal closure. evaluation of physeal closure.
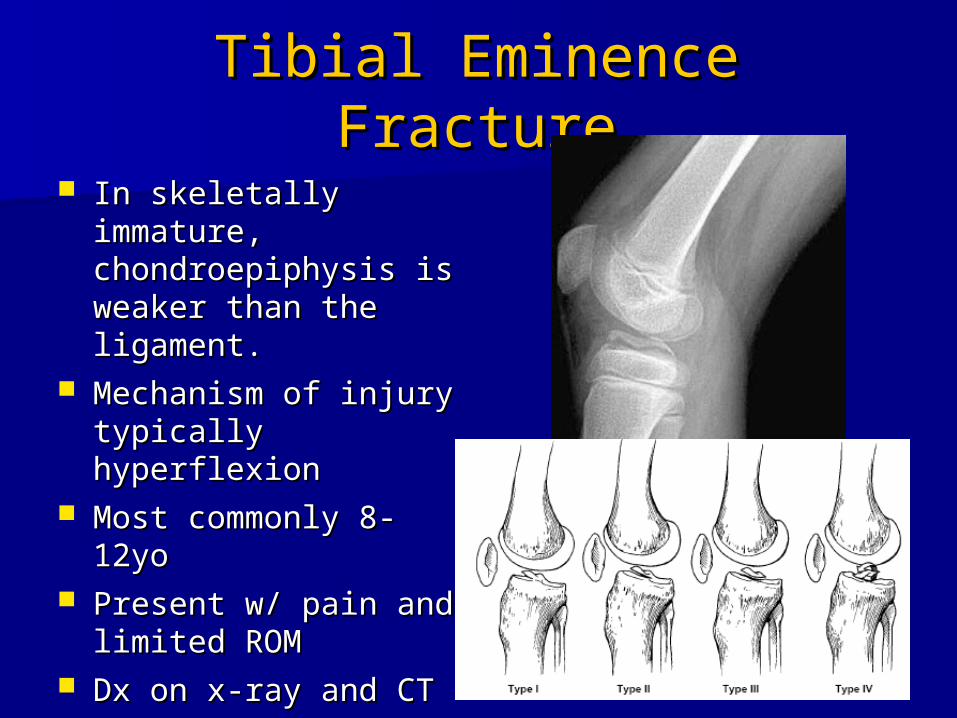
Tibial Eminence FractureTibial Eminence Fracture In skeletally immature, In skeletally immature,
chondroepiphysis is chondroepiphysis is weaker than the weaker than the ligament.ligament.
Mechanism of injury Mechanism of injury typically hyperflexiontypically hyperflexion
Most commonly 8-Most commonly 8-12yo12yo
Present w/ pain and Present w/ pain and limited ROMlimited ROM
Dx on x-ray and CTDx on x-ray and CT
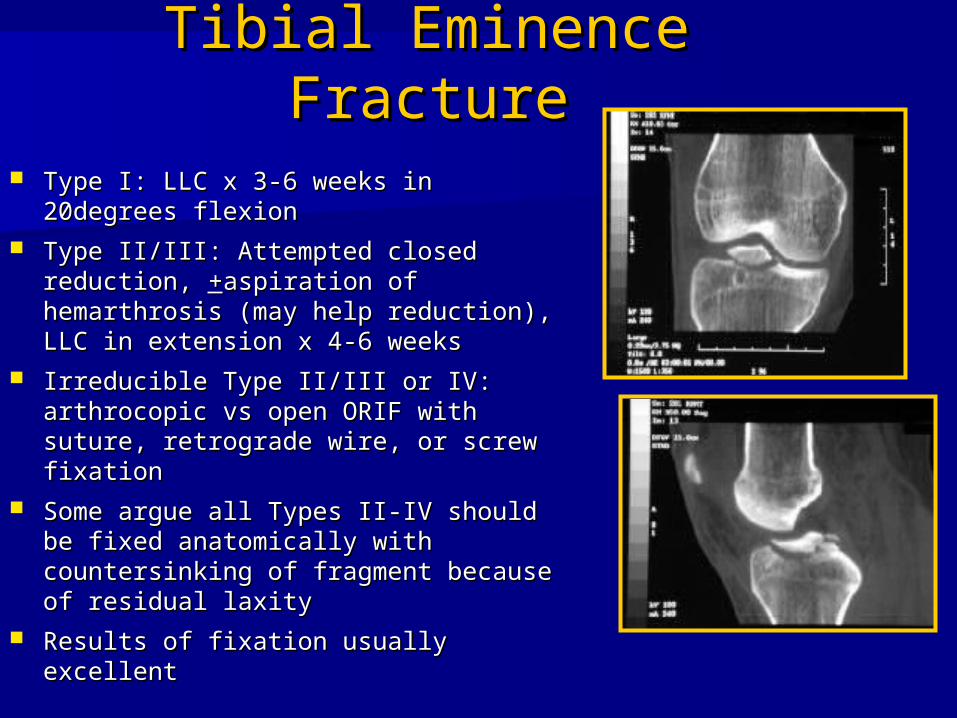
Tibial Eminence FractureTibial Eminence Fracture Type I: LLC x 3-6 weeks in 20degrees Type I: LLC x 3-6 weeks in 20degrees
flexionflexion Type II/III: Attempted closed reduction, Type II/III: Attempted closed reduction,
++aspiration of hemarthrosis (may help aspiration of hemarthrosis (may help reduction), LLC in extension x 4-6 reduction), LLC in extension x 4-6 weeksweeks
Irreducible Type II/III or IV: arthrocopic Irreducible Type II/III or IV: arthrocopic vs open ORIF with suture, retrograde vs open ORIF with suture, retrograde wire, or screw fixationwire, or screw fixation
Some argue all Types II-IV should be Some argue all Types II-IV should be fixed anatomically with countersinking fixed anatomically with countersinking of fragment because of residual laxityof fragment because of residual laxity
Results of fixation usually excellentResults of fixation usually excellent
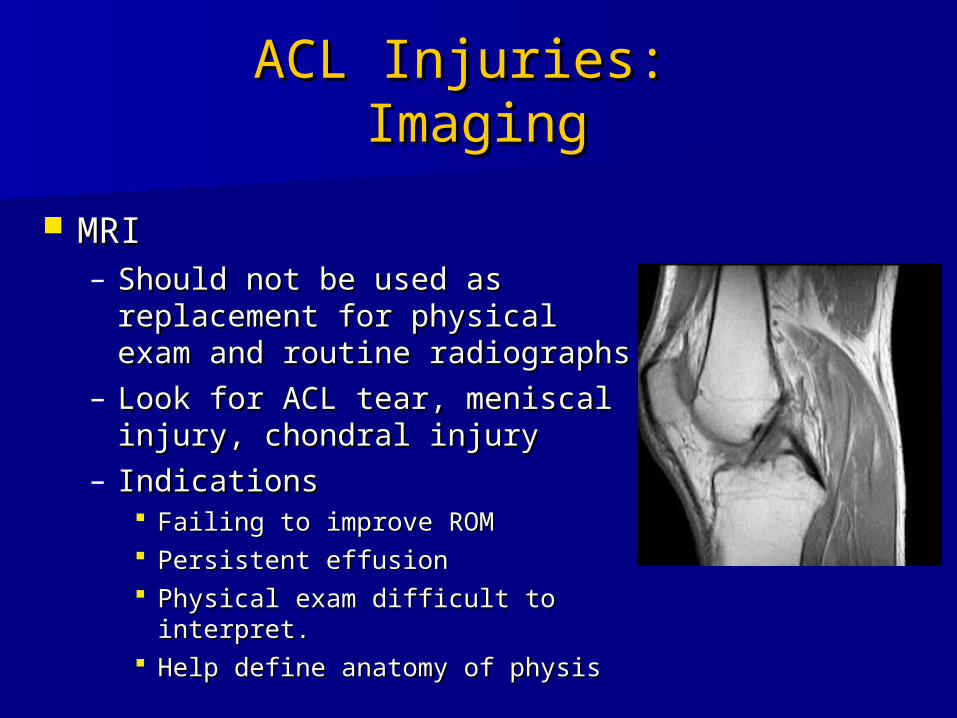
ACL Injuries: ACL Injuries: ImagingImaging
MRIMRI– Should not be used as Should not be used as
replacement for physical exam replacement for physical exam and routine radiographsand routine radiographs
– Look for ACL tear, meniscal Look for ACL tear, meniscal injury, chondral injuryinjury, chondral injury
– IndicationsIndications Failing to improve ROM Failing to improve ROM Persistent effusionPersistent effusion Physical exam difficult to interpret. Physical exam difficult to interpret. Help define anatomy of physisHelp define anatomy of physis
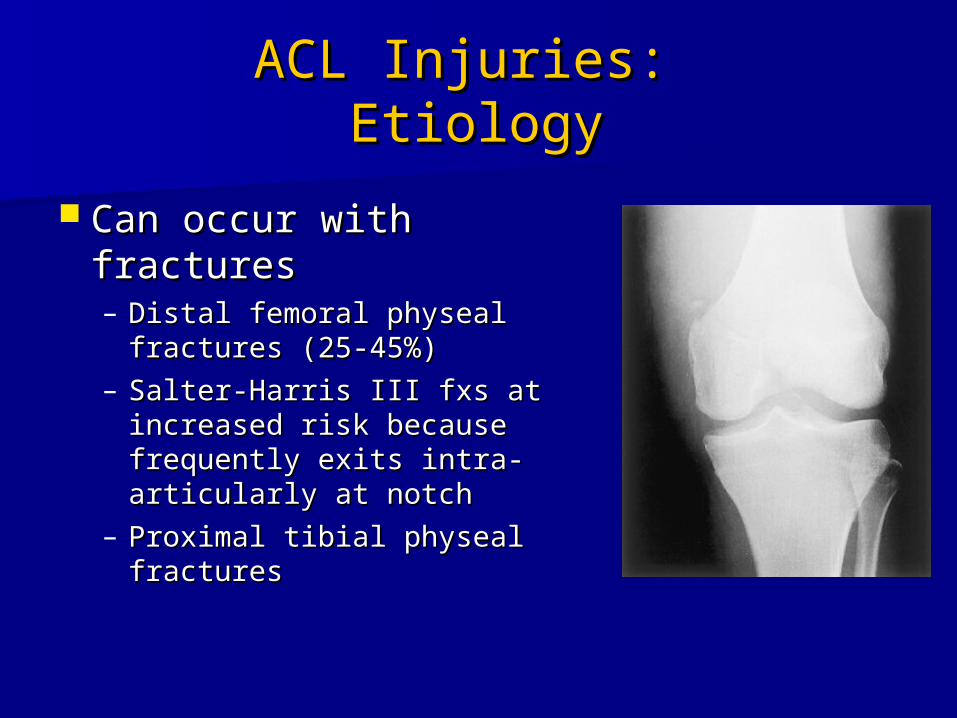
ACL Injuries: ACL Injuries: EtiologyEtiology
Can occur with fracturesCan occur with fractures– Distal femoral physeal Distal femoral physeal
fractures (25-45%)fractures (25-45%)– Salter-Harris III fxs at Salter-Harris III fxs at
increased risk because increased risk because frequently exits intra-frequently exits intra-articularly at notcharticularly at notch
– Proximal tibial physeal Proximal tibial physeal fracturesfractures
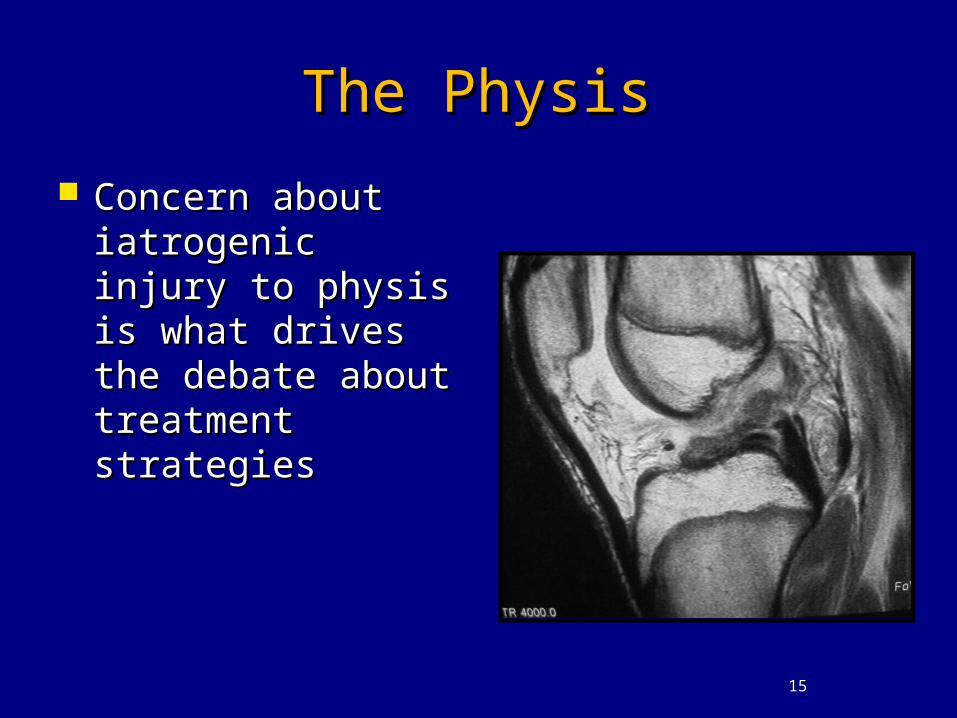
The PhysisThe Physis Concern about Concern about
iatrogenic injury to iatrogenic injury to physis is what physis is what drives the debate drives the debate about treatment about treatment strategiesstrategies
1515
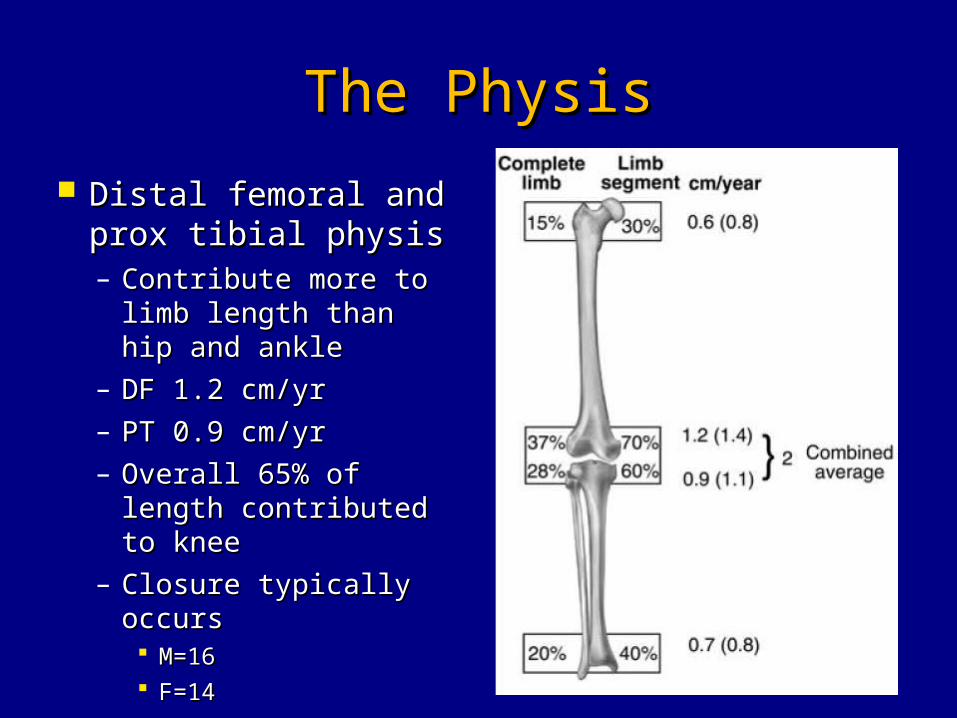
The PhysisThe Physis Distal femoral and Distal femoral and
prox tibial physisprox tibial physis– Contribute more to Contribute more to
limb length than hip limb length than hip and ankleand ankle
– DF 1.2 cm/yrDF 1.2 cm/yr– PT 0.9 cm/yrPT 0.9 cm/yr– Overall 65% of length Overall 65% of length
contributed to kneecontributed to knee– Closure typically Closure typically
occursoccurs M=16M=16 F=14F=14 1616
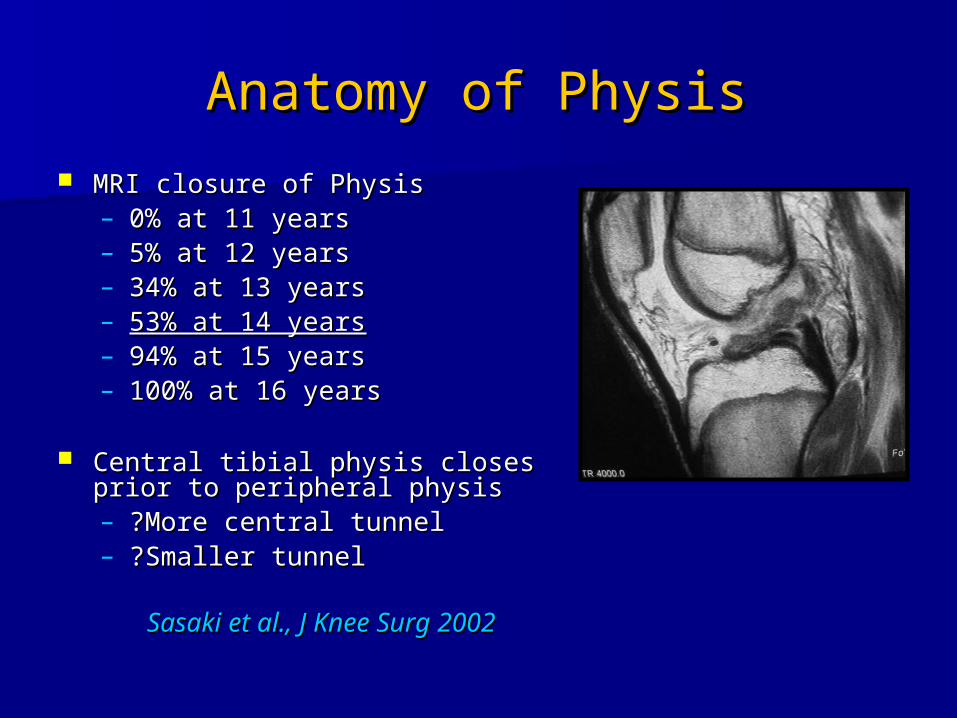
Anatomy of PhysisAnatomy of Physis MRI closure of PhysisMRI closure of Physis
– 0% at 11 years0% at 11 years– 5% at 12 years5% at 12 years– 34% at 13 years34% at 13 years– 53% at 14 years53% at 14 years– 94% at 15 years94% at 15 years– 100% at 16 years100% at 16 years
Central tibial physis closes prior to Central tibial physis closes prior to peripheral physisperipheral physis– ?More central tunnel?More central tunnel– ?Smaller tunnel?Smaller tunnel
Sasaki et al., J Knee Surg 2002Sasaki et al., J Knee Surg 2002
ACL Injuries:ACL Injuries:TreatmentTreatment
Concern for possible growth abnormality Concern for possible growth abnormality fuels debate on treatmentfuels debate on treatment– Non-operativeNon-operative– OperativeOperative
Direct RepairDirect Repair Extra-articular Extra-articular Intra-articularIntra-articular Intra/Extra articular reconstructionsIntra/Extra articular reconstructions
– Physeal sparingPhyseal sparing– Partial Transphyseal Partial Transphyseal – Complete transphysealComplete transphyseal– Trans epiphysealTrans epiphyseal
ACL InjuriesACL InjuriesNonoperative ManagementNonoperative Management
Avoids risk of physeal Avoids risk of physeal damagedamage
Sometimes used as a Sometimes used as a temporizing measure temporizing measure until skeletal maturityuntil skeletal maturity
Very difficult to Very difficult to reasonably limit young reasonably limit young patient’s activitiespatient’s activities
ACL Injuries:ACL Injuries:Nonoperative managementNonoperative management
So what if we don’t So what if we don’t treat these injuries?treat these injuries?– Angel et al. Arthroscopy Angel et al. Arthroscopy
1989 1989 27 children with 27 children with
arthroscopically arthroscopically documented ACL tearsdocumented ACL tears
22 patients at 51mo f/u22 patients at 51mo f/u None able to return to None able to return to
sports at preinjury levelsports at preinjury level
Non-op ACL Open PhysisNon-op ACL Open Physis
40 pts under 14 y/o open physis40 pts under 14 y/o open physis
16 conservative16 conservative– 6 scope for meniscal tears6 scope for meniscal tears– Only 7 return to sportsOnly 7 return to sports
All recur giving way, swelling, painAll recur giving way, swelling, pain
McCarroll et al., AJSM 1988McCarroll et al., AJSM 1988
Non-op ACL Open PhysisNon-op ACL Open Physis
18 pts ACL injury open physis18 pts ACL injury open physis Only one returned to Only one returned to
preinjury level of sportspreinjury level of sports Initial scope 13 meniscal Initial scope 13 meniscal
tearstears Later secondary meniscal Later secondary meniscal
tears in 9tears in 9 Degen changes 11 of 18 pts Degen changes 11 of 18 pts
by Xrayby Xray
Mizuta et al., JBJS Br 1995Mizuta et al., JBJS Br 1995
Non-op ACL Open PhysisNon-op ACL Open Physis
60 children with ACL tear60 children with ACL tear 23 nonop23 nonop
• Nat Hx continued instability, further Nat Hx continued instability, further meniscal and chondral damagemeniscal and chondral damage
• 25 % secondary meniscal tears25 % secondary meniscal tears• Few able to participate in sportFew able to participate in sportss
Aichroth et al., JBJS BR, 2002Aichroth et al., JBJS BR, 2002
Non-op ACL Open PhysisNon-op ACL Open Physis ? Effect of delay in ? Effect of delay in
treatmenttreatment 39 pt < 14 y/o39 pt < 14 y/o Sig increase in MMT Sig increase in MMT
with delay in treatment with delay in treatment > 6 weeks> 6 weeks• 36% chronic vs 11% in 36% chronic vs 11% in
acute Rxacute Rx No diff in rate of LMTNo diff in rate of LMT
Millett et al., Arthroscopy 2002Millett et al., Arthroscopy 2002
ACL InjuriesACL InjuriesNonoperative ManagementNonoperative Management
Graf et al: Graf et al: – 12 skeletally immature patients with ACL tears12 skeletally immature patients with ACL tears– 8 patients underwent non-op and no restriction 8 patients underwent non-op and no restriction
management. management. 7 of the 8 had new meniscal tear at follow up7 of the 8 had new meniscal tear at follow up
ACL Injury:ACL Injury:Long Term ResultsLong Term Results
Kannus et al. JBJS-B. 1988Kannus et al. JBJS-B. 1988• 8 year F/U – 4/7 Pediatric Patients that had 8 year F/U – 4/7 Pediatric Patients that had
Untreated ACL Tears showed Advancing Untreated ACL Tears showed Advancing OA radiographicallyOA radiographically
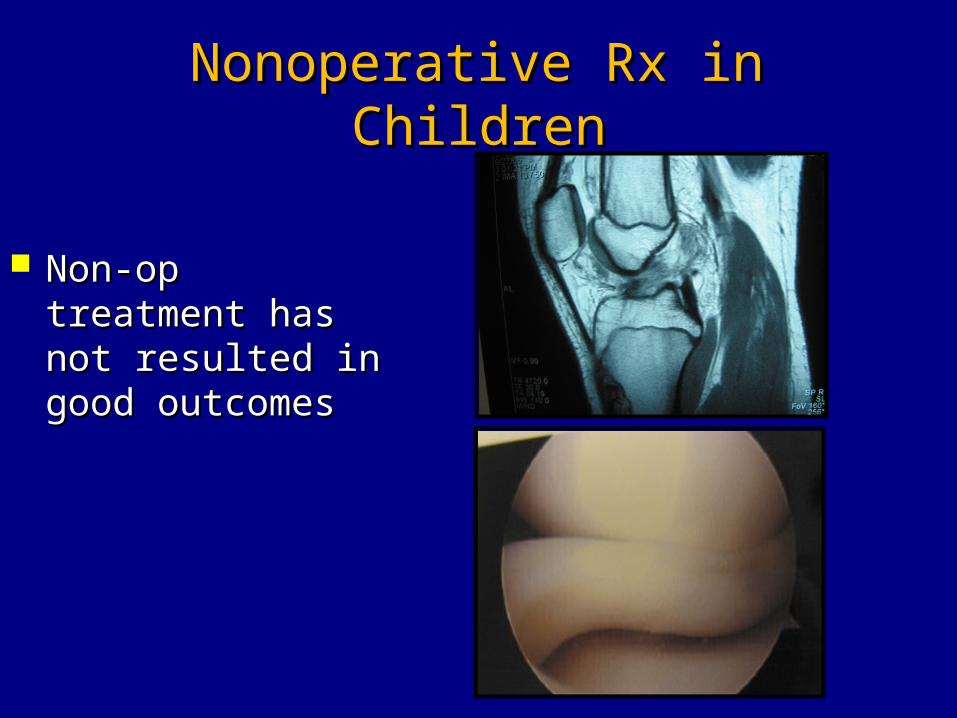
Nonoperative Rx in ChildrenNonoperative Rx in Children
Non-op treatment Non-op treatment has not resulted has not resulted in good outcomesin good outcomes
ACL Injuries:ACL Injuries:Physeal ConcernsPhyseal Concerns
Fear disruption of open Fear disruption of open physesphyses
Risk of epiphysiodesis, LLD, Risk of epiphysiodesis, LLD, angular deformityangular deformity
Caused by crossing physis Caused by crossing physis with bone plug and/or with bone plug and/or fixation devicesfixation devices
ACL Injuries:ACL Injuries:Physeal ConcernsPhyseal Concerns
History History – Campbell et al. (1959)Campbell et al. (1959)
Large holes drilled through the physis have maximal Large holes drilled through the physis have maximal retardation of growth plateretardation of growth plate
Insertion of cortical bone across physis causes arrestInsertion of cortical bone across physis causes arrest– Makel et al (1988)Makel et al (1988)
Destruction of >7% of physis causes growth arrestDestruction of >7% of physis causes growth arrest Destruction of 3% or less…no arrestDestruction of 3% or less…no arrest
– Stadelmeir et al (1995)Stadelmeir et al (1995) Soft tissue graft placed in drill hole did not cause Soft tissue graft placed in drill hole did not cause
physeal bar. physeal bar.
Factors Influencing Physeal ArrestFactors Influencing Physeal Arrest
Diameter of drill holeDiameter of drill hole Soft tissue graft within tunnelSoft tissue graft within tunnel Tension of graft across physisTension of graft across physis Tunnel location? (Central and vertical)Tunnel location? (Central and vertical)
ACL Injuries: ACL Injuries: Operative ManagmentOperative Managment
Direct Repair:Direct Repair:– A historic treatment modalityA historic treatment modality– Inflammatory changes and Inflammatory changes and
degeneration begins within 48 hours degeneration begins within 48 hours after injuryafter injury
– Metalloproteases and cytokine Metalloproteases and cytokine inflammatory factors affect healing inflammatory factors affect healing potential of direct repair potential of direct repair
– Poor resultsPoor results Delee and Curtis, CORR 1983Delee and Curtis, CORR 1983 Engebretsen, et al. Acta Orthop Scand 1988Engebretsen, et al. Acta Orthop Scand 1988
ACL Injuries:ACL Injuries:Operative ManagementOperative Management
Extra-Articular repairExtra-Articular repair– Temporizing methodTemporizing method– Non-anatomic reconstructionNon-anatomic reconstruction– Poor resultsPoor results
Dahlstedt , et al. Acta Orthop Scand Dahlstedt , et al. Acta Orthop Scand 19881988
McCarroll et al. AJSM 1998McCarroll et al. AJSM 1998 Graf, et al. Arthrsocopy 1992Graf, et al. Arthrsocopy 1992
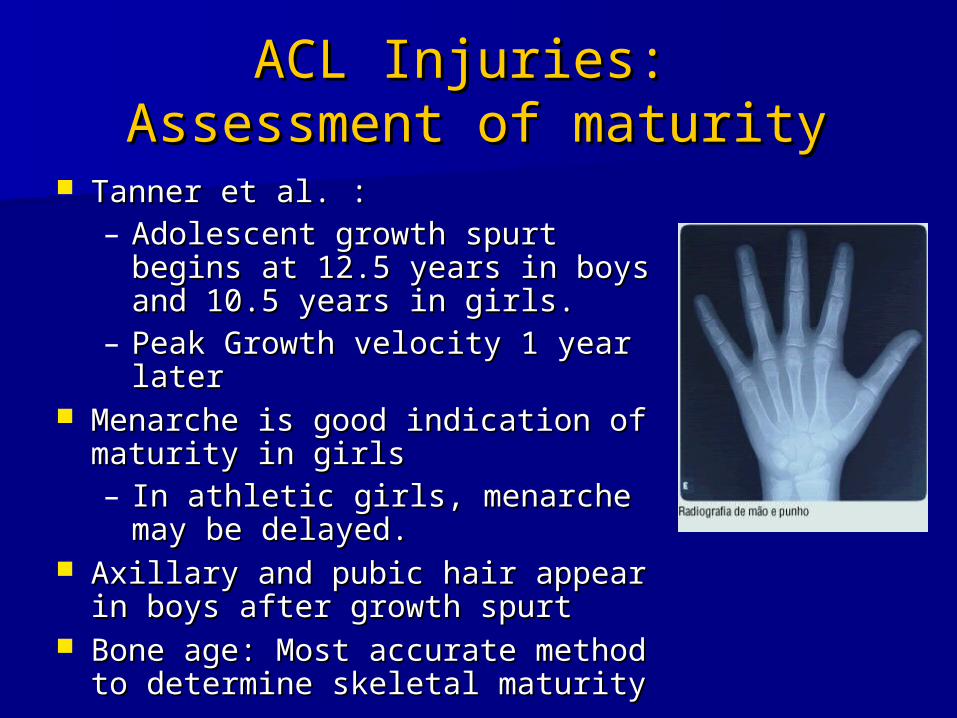
ACL Injuries: ACL Injuries: Assessment of maturityAssessment of maturity
Tanner et al. : Tanner et al. : – Adolescent growth spurt begins Adolescent growth spurt begins
at 12.5 years in boys and 10.5 at 12.5 years in boys and 10.5 years in girls. years in girls.
– Peak Growth velocity 1 year Peak Growth velocity 1 year laterlater
Menarche is good indication of Menarche is good indication of maturity in girlsmaturity in girls– In athletic girls, menarche may In athletic girls, menarche may
be delayed. be delayed. Axillary and pubic hair appear in Axillary and pubic hair appear in
boys after growth spurtboys after growth spurt Bone age: Most accurate method Bone age: Most accurate method
to determine skeletal maturity to determine skeletal maturity
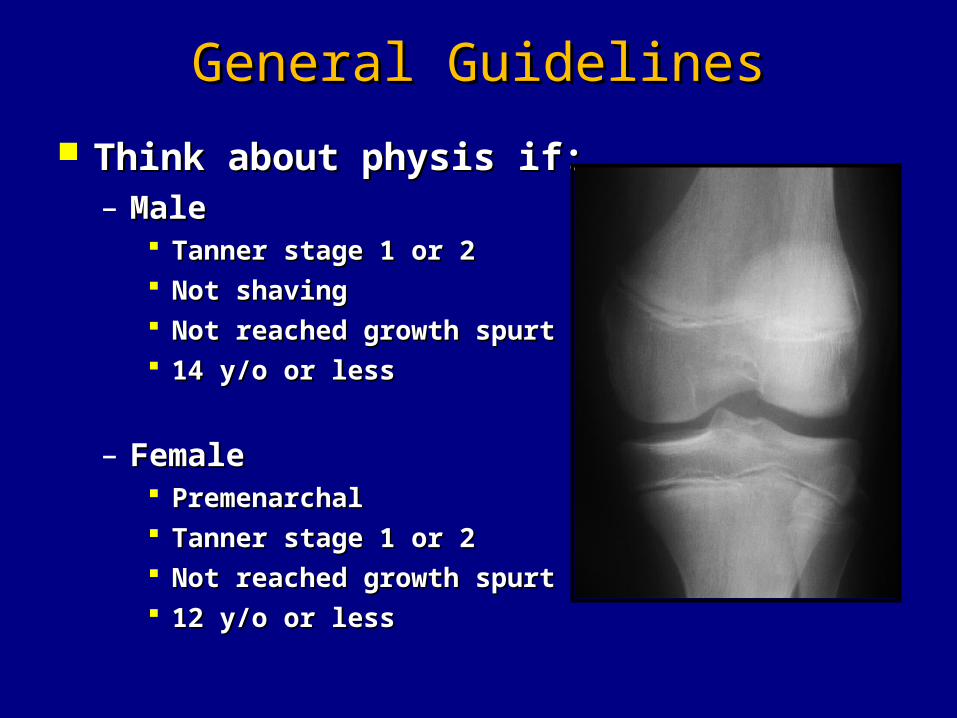
General GuidelinesGeneral Guidelines Think about physis if:Think about physis if:
– MaleMale Tanner stage 1 or 2Tanner stage 1 or 2 Not shavingNot shaving Not reached growth spurtNot reached growth spurt 14 y/o or less14 y/o or less
– FemaleFemale PremenarchalPremenarchal Tanner stage 1 or 2Tanner stage 1 or 2 Not reached growth spurtNot reached growth spurt 12 y/o or less12 y/o or less
ACL Reconstruction ACL Reconstruction TechniquesTechniques
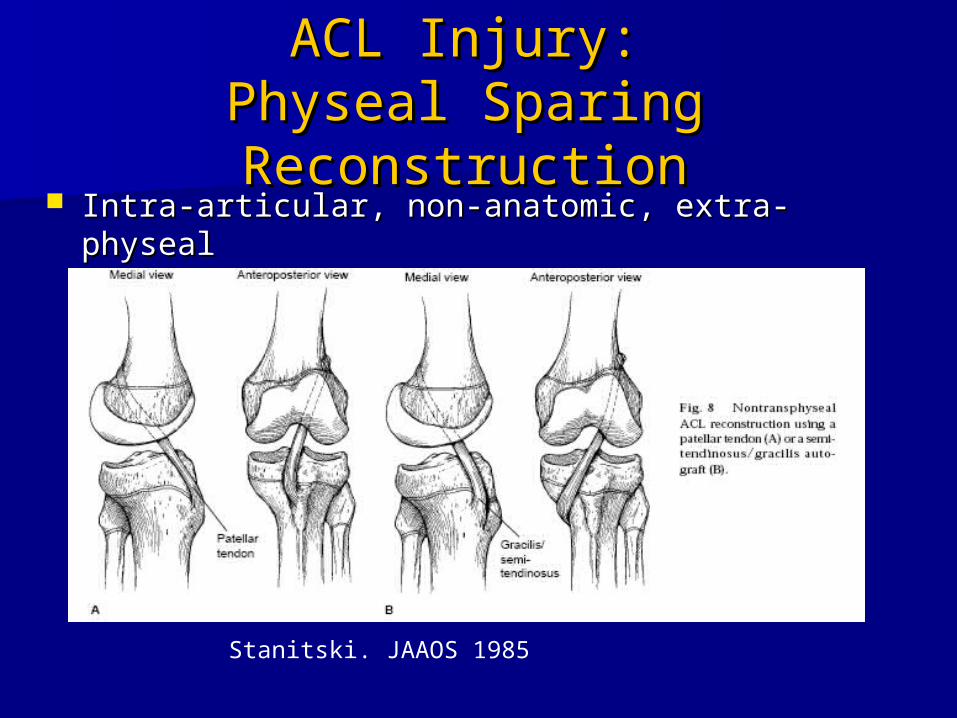
ACL Injury:ACL Injury:Physeal Sparing Physeal Sparing ReconstructionReconstruction
Intra-articular, non-anatomic, extra-physealIntra-articular, non-anatomic, extra-physeal
Stanitski. JAAOS 1985
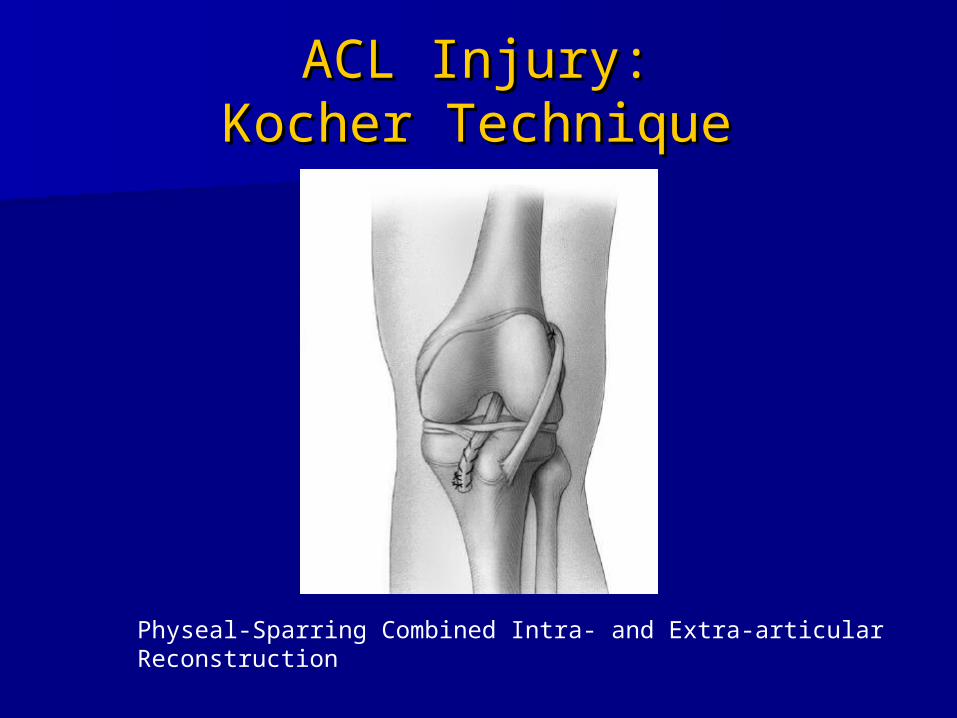
ACL Injury:ACL Injury:Kocher TechniqueKocher Technique
Physeal-Sparring Combined Intra- and Extra-articular Reconstruction
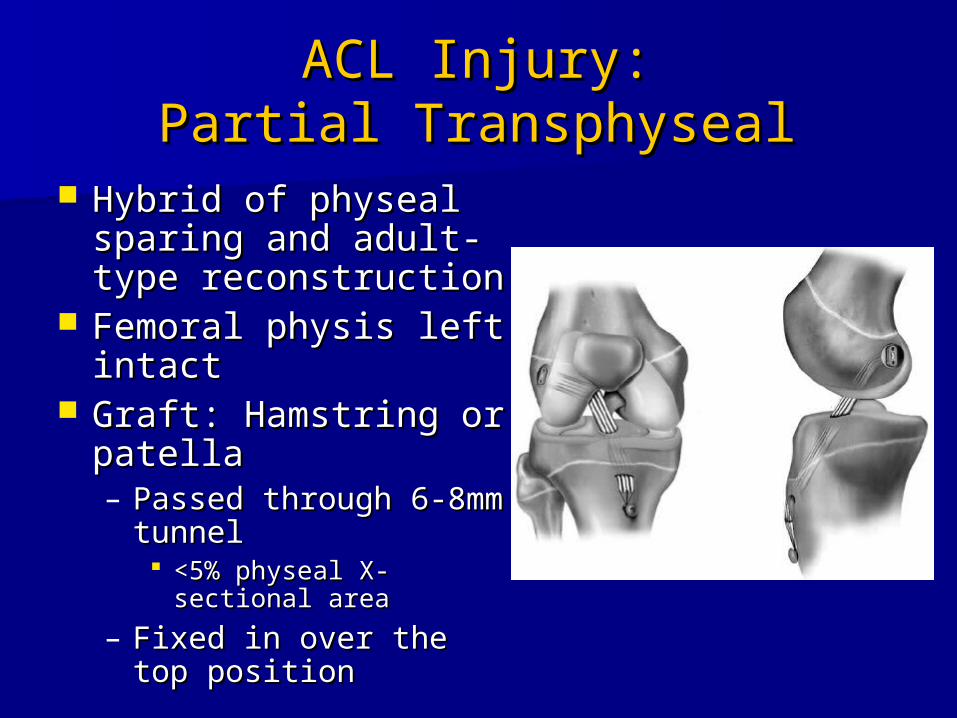
ACL Injury:ACL Injury:Partial TransphysealPartial Transphyseal
Hybrid of physeal Hybrid of physeal sparing and adult-sparing and adult-type reconstructiontype reconstruction
Femoral physis left Femoral physis left intactintact
Graft: Hamstring or Graft: Hamstring or patellapatella– Passed through 6-Passed through 6-
8mm tunnel8mm tunnel <5% physeal X-<5% physeal X-
sectional areasectional area– Fixed in over the top Fixed in over the top
positionposition
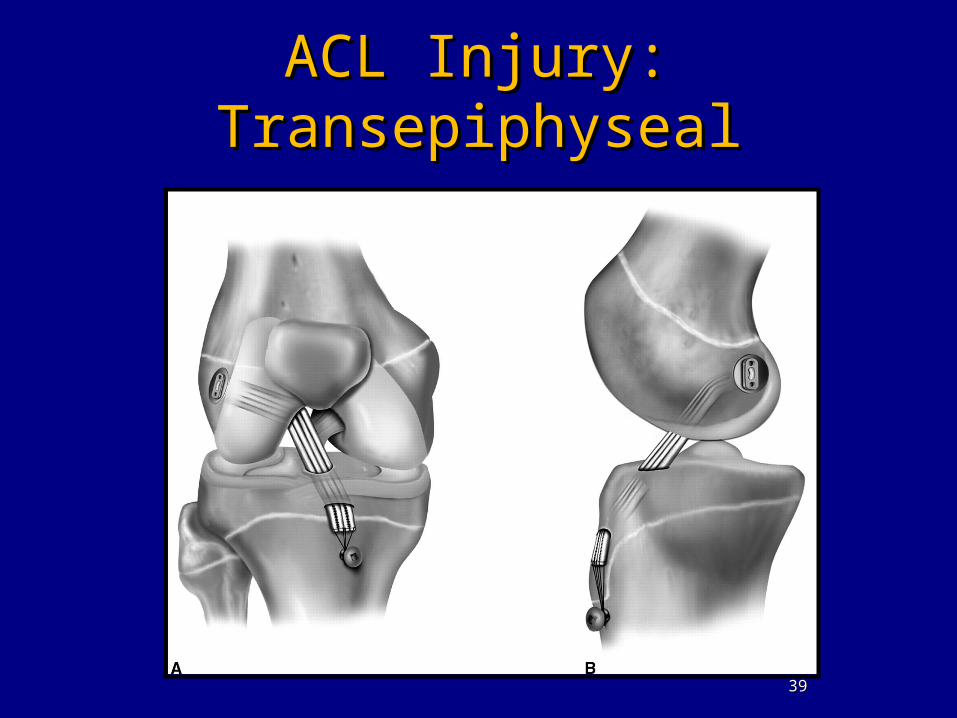
ACL Injury:ACL Injury:TransepiphysealTransepiphyseal
3939
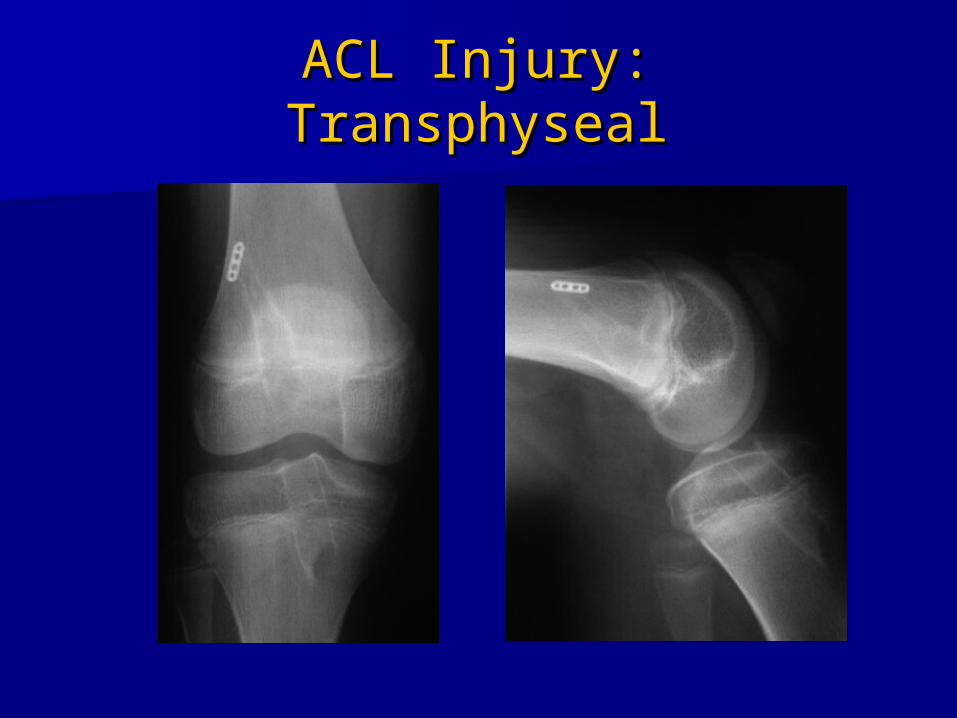
ACL Injury:ACL Injury:TransphysealTransphyseal
Thank YouThank You