Embed Size (px)
Citation preview
Active Chemotherapy for Sarcomatoid and RapidlyProgressing Renal Cell Carcinoma
David M. Nanus, M.D.1,2
Alexandria Garino, R.P.A.3
Matthew I. Milowsky, M.D.1,2
Maureen Larkin, R.N., M.S.N., F.N.P.3
Janice P. Dutcher, M.D.3
1 Department of Medicine, Weill Medical College ofCornell University, New York, New York.
2 Department of Urology, Weill Medical College ofCornell University, New York, New York.
3 Department of Medicine, Our Lady of Mercy Can-cer Center/New York Medical College, New York,New York.
Supported by the Robert H. McCooey MemorialCancer Research Fund and by the Cancer Re-search Foundation Kidney Cancer Research Fund.
The authors thank Alyssa Rosmarrin and JodiKaplan for providing nursing assistance and Ms.Heather Orkin for providing secretarial support.
Address for reprints: David M. Nanus, M.D., De-partment of Medicine, Weill Medical College ofCornell University, 525 East 68th Street, New York,NY 10021; Fax: (212) 746-0701; E-mail:[email protected]
Received January 23, 2004; revision receivedJune 17, 2004; accepted June 23, 2004.
BACKGROUND. Immunotherapy is generally ineffective in patients with sarcoma-
toid renal cell carcinoma (RCC) and in patients with rapidly progressive metastatic
or locally recurrent disease, with a median time to progression of approximately 2
months and a median survival of 4 –7 months. Gemcitabine-based regimens have
modest antitumor activity, whereas doxorubicin is often used to treat sarcomatoid
RCC. Based on the antitumor activity of doxorubicin and gemcitabine in collecting
duct carcinoma of the kidney, the authors used this combination to treat selected
patients with sarcomatoid or rapidly progressing RCC.
METHODS. Eighteen patients (11 males and 7 females; median age, 53 years; range,
31– 81 years) with RCC (56% sarcomatoid; 44% other) were treated at 2 institutions
in a collaborative study that was not institutional review board reviewed. Seven
patients received previous treatment with interferon or interleukin-2. Sites of
metastases included the lung, soft tissue, bone, liver, and brain with 88% of
patients having � 3 sites of disease. Treatment consisted of doxorubicin (50
mg/m2) and gemcitabine (1500 or 2000 mg/m2) every 2–3 weeks with granulocyte–
colony-stimulating factor support.
RESULTS. A median of 5 courses was administered (range, 2–12 cycles). Therapy
was well tolerated with no Grade 4 toxicities. Two patients had a complete re-
sponse, five had a partial response, three had a mixed response, and one had stable
disease. The median duration of response was 5 months (range, 2–21� months).
CONCLUSIONS. These data suggested that the combination of doxorubicin and
gemcitabine has antitumor activity in patients with sarcomatoid RCC or with
rapidly progressing RCC. A prospective investigation of this combination in RCC is
warranted. Cancer 2004;101:1545–51. © 2004 American Cancer Society.
KEYWORDS: chemotherapy, doxorubicin, gemcitabine, sarcomatoid renal carci-noma, kidney carcinoma.
Renal cell carcinoma (RCC) is highly resistant to chemotherapy.1 In1993, Yagoda et al.2 analyzed 72 cytotoxic chemotherapeutic
agents used singly or in a limited number of 2-drug combinations in3502 patients, and found reports of objective responses (complete[CR] and partial remissions [PR]) in only 197 (5.6%) of these patients(95% confidence interval [CI], 4.8 – 6.4%). More recent studies haveresulted in similarly low response proportions.3,4 Over the last fewyears, clinical trials using gemcitabine-containing regimens havebeen more encouraging, with major responses occurring in 5–17% ofpatients.5 Nevertheless, results using chemotherapy in this diseasehave been disappointing as indicated by the low response propor-tions and no study showing an improvement in survival. Immuno-therapy with interferon (IFN) and/or interleukin (IL)-2– based regi-mens remains the mainstay of treatment for patients with advanced
1545
© 2004 American Cancer SocietyDOI 10.1002/cncr.20541Published online 18 August 2004 in Wiley InterScience (www.interscience.wiley.com).

RCC with low, but reproducible, response rates of10 –20% and a durable response rate of � 5%.6
Sarcomatoid differentiation in RCC indicates anaggressive subtype of renal parenchymal tumors, andis associated with a poor prognosis.7,8 Some investi-gators believe that patients with metastatic RCC withsarcomatoid differentiation will not respond to immu-notherapy and should be treated with combinationchemotherapy.9 –11 Although doxorubicin-containingregimens are often administered, only rarely do pa-tients experience clinical benefit.12 In a recent Phase IItrial of doxorubicin in combination with ifosfamide inpatients with metastatic sarcomatoid RCC, no objec-tive responses occurred in 25 patients, and the mediantime to progression was only 2.2 months.13 We re-cently reported the use of doxorubicin and gemcitab-ine in a patient with collecting duct carcinoma of thekidney, a rare variant of RCC that is associated with anaggressive course and extremely poor prognosis.14 Theregimen consisted of doxorubicin (50 mg/m2) andgemcitabine (2000 mg/m2) every 2 weeks with growthfactor support and was modeled after a highly effec-tive and well tolerated regimen used to treat patientswith advanced bladder carcinoma.15 Based on thisexperience, we elected to use this regimen to treatpatients with sarcomatoid RCC, and well as patientswith rapidly progressive RCC of other histologies whomay have progressed after immunotherapy
MATERIALS AND METHODSPatient PopulationAll patients treated had histologic confirmation ofRCC, and unresectable metastatic RCC that was bidi-mensionally measurable. Patients had sarcomatoidRCC, or RCC with rapid clinical progression with ob-jective clinical progression as determined on imagingand physical examination over 1 month, and/or hadobjectively progressed after receiving immunotherapywith either IL-2 or IFN-based regimens. Patients withbrain metastases who had received radiotherapy wereeligible for therapy provided there was evidence ofprogression of systemic disease. Normal cardiac func-tion, as judged by chest radiography, an electrocardi-ography (ECG), and nuclear medicine gated cardiacscan or echocardiagram, was required. Patients whohad evidence of New York Heart Association func-tional Class III or IV heart disease or severe arrhyth-mias, including first, second, or third-degree heartblock, were not considered for treatment. The currentstudy was not a formalized clinical trial (i.e., institu-tional review board approval and signed consentforms were not obtained) and was performed collabo-ratively across two institutions. Risks and benefits of
chemotherapy were discussed in detail with each pa-tient before initiation of treatment.
Treatment Plan and Toxicity EvaluationPretreatment evaluation included a complete medicalhistory with Eastern Cooperative Oncology Group(ECOG) performance status and physical examination.Indicator lesions were measured either during a phys-ical examination or by the appropriate radiographicstudy. Baseline studies included complete bloodcount with differential, serum chemistries includingmeasurement of creatinine levels, liver function tests(including measurement of alkaline phosphatase, as-partate aminotransferase, alanine aminotransferase,bilirubin levels), chest radiograph, ECG, radionuclideleft ventriculogram or echocardiogram with ejectionfraction, and computerized tomography (CT) scans ofmetastatic disease. Bone scans were performed ifthere was clinical evidence of bone metastases or anelevated alkaline phosphatase concentration. Patientsreceived doxorubicin by intravenous (i.v.) bolus infu-sion plus gemcitabine by i.v. infusion over 1 hour. Thestarting dose of doxorubicin was 50 mg/m2. The initialdose of gemcitabine was administered at either 1500mg/m2 (Our Lady of Mercy Cancer Center [OLM]) or2000 mg/m2 (New York Presbyterian Hospital[NYPH]). Patients were instructed in the administra-tion of recombinant human granulocte– colony-stim-ulating factor and self-administered 5 �g/kg per dayby subcutaneous injection on Days 3–11 of each cycle,or until the total leukocyte was � 10,000. Dose atten-uations were at the discretion of the investigators, butgenerally included a 20 –25% reduction in the dosageof gemcitabine and/or an increase in the treatmentinterval from every 2 weeks to every 3 weeks. Toxicitywas scored using the National Cancer Institute Com-mon Toxicity Criteria, Version 2.0.
Response CriteriaTumor response evaluations were performed by phys-ical examination, chest X-ray, and/or CT scans every 3cycles (6 –9 weeks). A CR was defined as the disappear-ance of all clinical evidence of tumor by physical ex-amination, radiographic studies, or both for a mini-mum of 4 weeks. A PR was defined as a 50% decreasein the summed products of the perpendicular diame-ters of all measurable lesions for � 4 weeks, withoutthe simultaneous increase in the size of any lesion orthe appearance of any new lesion. Progression wasdefined as a � 25% increase in tumor size or theappearance of any new lesion.
1546 CANCER October 1, 2004 / Volume 101 / Number 7
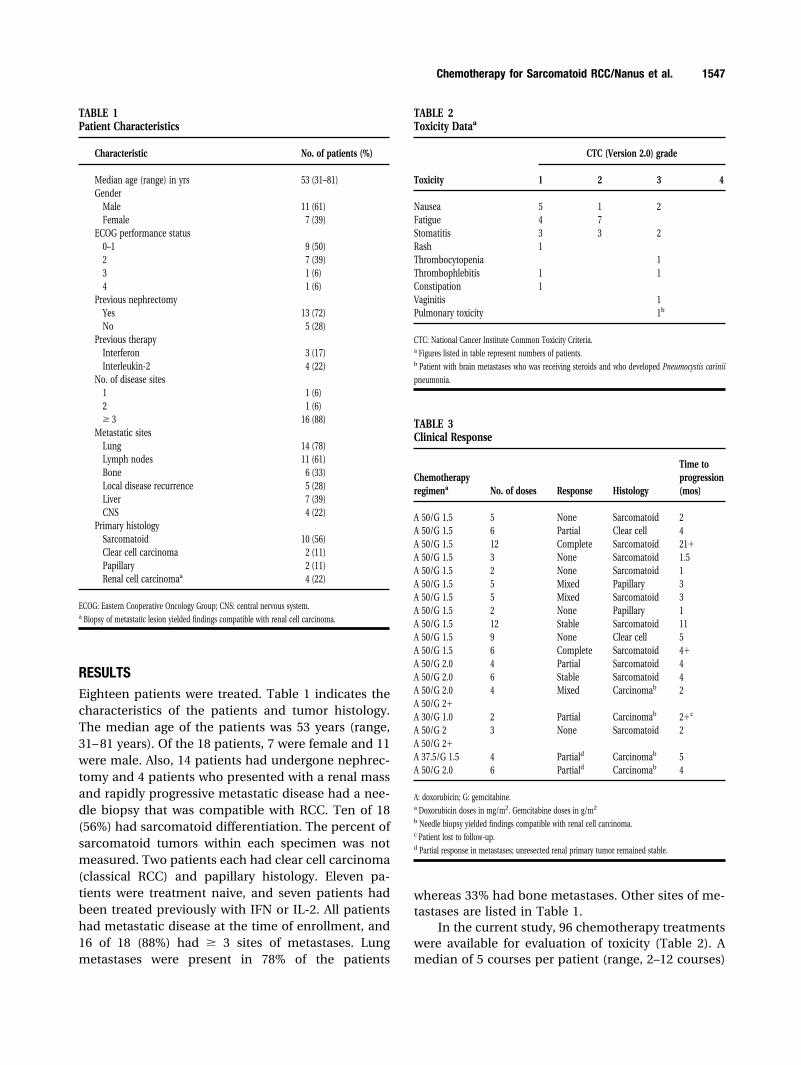
RESULTSEighteen patients were treated. Table 1 indicates thecharacteristics of the patients and tumor histology.The median age of the patients was 53 years (range,31– 81 years). Of the 18 patients, 7 were female and 11were male. Also, 14 patients had undergone nephrec-tomy and 4 patients who presented with a renal massand rapidly progressive metastatic disease had a nee-dle biopsy that was compatible with RCC. Ten of 18(56%) had sarcomatoid differentiation. The percent ofsarcomatoid tumors within each specimen was notmeasured. Two patients each had clear cell carcinoma(classical RCC) and papillary histology. Eleven pa-tients were treatment naive, and seven patients hadbeen treated previously with IFN or IL-2. All patientshad metastatic disease at the time of enrollment, and16 of 18 (88%) had � 3 sites of metastases. Lungmetastases were present in 78% of the patients
whereas 33% had bone metastases. Other sites of me-tastases are listed in Table 1.
In the current study, 96 chemotherapy treatmentswere available for evaluation of toxicity (Table 2). Amedian of 5 courses per patient (range, 2–12 courses)
TABLE 2Toxicity Dataa
Toxicity
CTC (Version 2.0) grade
1 2 3 4
Nausea 5 1 2Fatigue 4 7Stomatitis 3 3 2Rash 1Thrombocytopenia 1Thrombophlebitis 1 1Constipation 1Vaginitis 1Pulmonary toxicity 1b
CTC: National Cancer Institute Common Toxicity Criteria.a Figures listed in table represent numbers of patients.b Patient with brain metastases who was receiving steroids and who developed Pneumocystis carinii
pneumonia.
TABLE 3Clinical Response
Chemotherapyregimena No. of doses Response Histology
Time toprogression(mos)
A 50/G 1.5 5 None Sarcomatoid 2A 50/G 1.5 6 Partial Clear cell 4A 50/G 1.5 12 Complete Sarcomatoid 21�A 50/G 1.5 3 None Sarcomatoid 1.5A 50/G 1.5 2 None Sarcomatoid 1A 50/G 1.5 5 Mixed Papillary 3A 50/G 1.5 5 Mixed Sarcomatoid 3A 50/G 1.5 2 None Papillary 1A 50/G 1.5 12 Stable Sarcomatoid 11A 50/G 1.5 9 None Clear cell 5A 50/G 1.5 6 Complete Sarcomatoid 4�A 50/G 2.0 4 Partial Sarcomatoid 4A 50/G 2.0 6 Stable Sarcomatoid 4A 50/G 2.0 4 Mixed Carcinomab 2A 50/G 2�A 30/G 1.0 2 Partial Carcinomab 2�c
A 50/G 2 3 None Sarcomatoid 2A 50/G 2�A 37.5/G 1.5 4 Partiald Carcinomab 5A 50/G 2.0 6 Partiald Carcinomab 4
A: doxorubicin; G: gemcitabine.a Doxorubicin doses in mg/m2. Gemcitabine doses in g/m2
b Needle biopsy yielded findings compatible with renal cell carcinoma.c Patient lost to follow-up.d Partial response in metastases; unresected renal primary tumor remained stable.
TABLE 1Patient Characteristics
Characteristic No. of patients (%)
Median age (range) in yrs 53 (31–81)Gender
Male 11 (61)Female 7 (39)
ECOG performance status0–1 9 (50)2 7 (39)3 1 (6)4 1 (6)
Previous nephrectomyYes 13 (72)No 5 (28)
Previous therapyInterferon 3 (17)Interleukin-2 4 (22)
No. of disease sites1 1 (6)2 1 (6)� 3 16 (88)
Metastatic sitesLung 14 (78)Lymph nodes 11 (61)Bone 6 (33)Local disease recurrence 5 (28)Liver 7 (39)CNS 4 (22)
Primary histologySarcomatoid 10 (56)Clear cell carcinoma 2 (11)Papillary 2 (11)Renal cell carcinomaa 4 (22)
ECOG: Eastern Cooperative Oncology Group; CNS: central nervous system.a Biopsy of metastatic lesion yielded findings compatible with renal cell carcinoma.
Chemotherapy for Sarcomatoid RCC/Nanus et al. 1547
was administered. Therapy was generally well toler-ated with no Grade 4 toxicities. Fatigue, nausea, andmucositis were the most common side effects. Onepatient who received steroids for brain metastasesdeveloped Pneumocystis carinii pneumonia requiringhospitalization. The patient was treated with tri-methoprim/sulfamethoxazole and recovered from theinfection. Two patients required dose attenuation, 1for Grade 3 mucositis and 1 for Grade 3 fatigue. BothGrade 3 toxicities resolved after the patients receivedthe lower dose of chemotherapy.
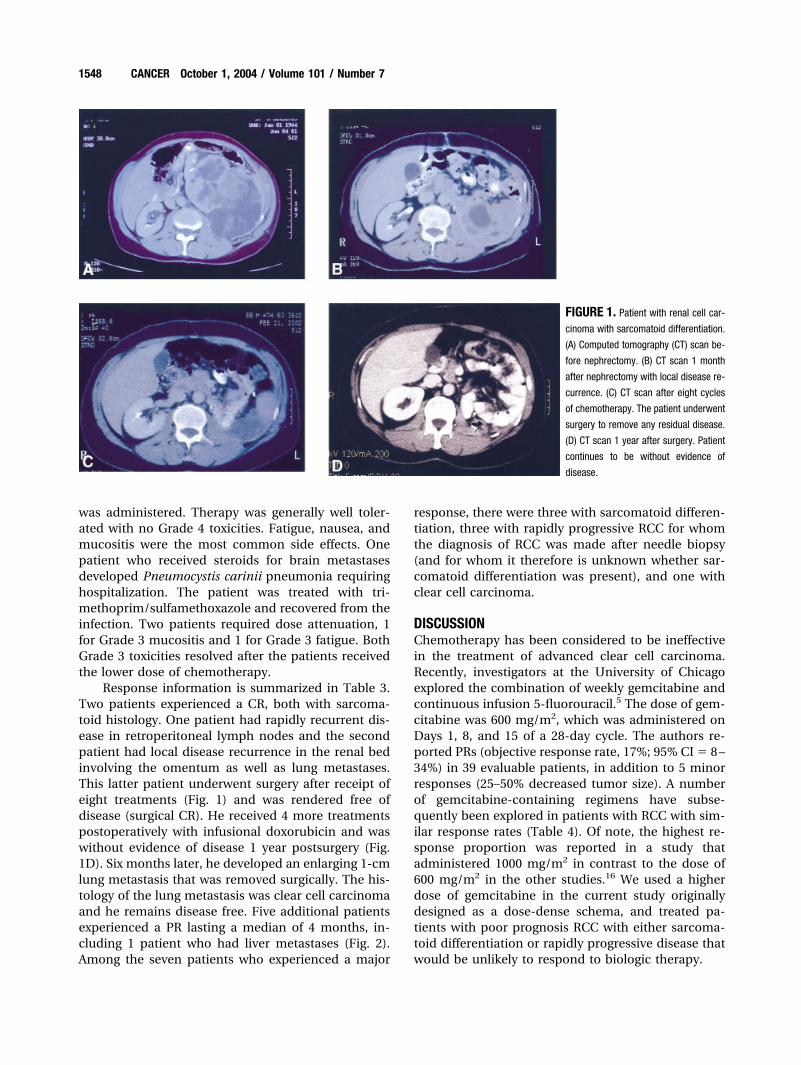
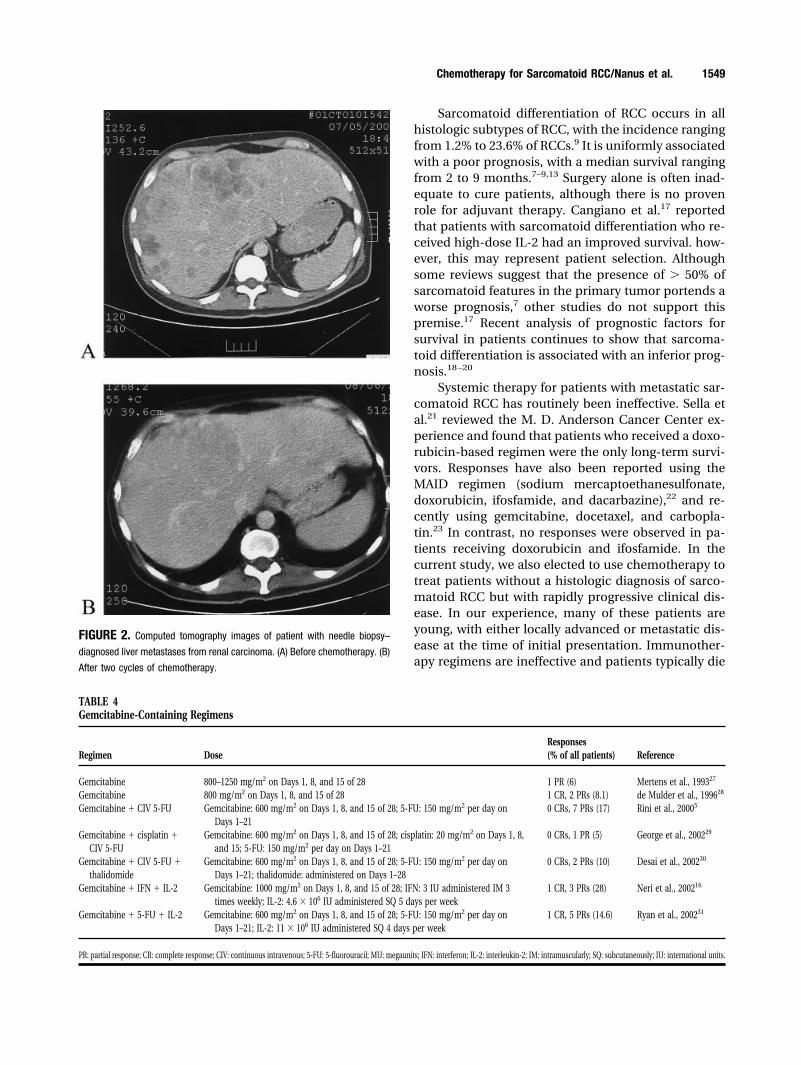
Response information is summarized in Table 3.Two patients experienced a CR, both with sarcoma-toid histology. One patient had rapidly recurrent dis-ease in retroperitoneal lymph nodes and the secondpatient had local disease recurrence in the renal bedinvolving the omentum as well as lung metastases.This latter patient underwent surgery after receipt ofeight treatments (Fig. 1) and was rendered free ofdisease (surgical CR). He received 4 more treatmentspostoperatively with infusional doxorubicin and waswithout evidence of disease 1 year postsurgery (Fig.1D). Six months later, he developed an enlarging 1-cmlung metastasis that was removed surgically. The his-tology of the lung metastasis was clear cell carcinomaand he remains disease free. Five additional patientsexperienced a PR lasting a median of 4 months, in-cluding 1 patient who had liver metastases (Fig. 2).Among the seven patients who experienced a major
response, there were three with sarcomatoid differen-tiation, three with rapidly progressive RCC for whomthe diagnosis of RCC was made after needle biopsy(and for whom it therefore is unknown whether sar-comatoid differentiation was present), and one withclear cell carcinoma.
DISCUSSIONChemotherapy has been considered to be ineffectivein the treatment of advanced clear cell carcinoma.Recently, investigators at the University of Chicagoexplored the combination of weekly gemcitabine andcontinuous infusion 5-fluorouracil.5 The dose of gem-citabine was 600 mg/m2, which was administered onDays 1, 8, and 15 of a 28-day cycle. The authors re-ported PRs (objective response rate, 17%; 95% CI � 8 –34%) in 39 evaluable patients, in addition to 5 minorresponses (25–50% decreased tumor size). A numberof gemcitabine-containing regimens have subse-quently been explored in patients with RCC with sim-ilar response rates (Table 4). Of note, the highest re-sponse proportion was reported in a study thatadministered 1000 mg/m2 in contrast to the dose of600 mg/m2 in the other studies.16 We used a higherdose of gemcitabine in the current study originallydesigned as a dose-dense schema, and treated pa-tients with poor prognosis RCC with either sarcoma-toid differentiation or rapidly progressive disease thatwould be unlikely to respond to biologic therapy.
FIGURE 1. Patient with renal cell car-
cinoma with sarcomatoid differentiation.
(A) Computed tomography (CT) scan be-
fore nephrectomy. (B) CT scan 1 month
after nephrectomy with local disease re-
currence. (C) CT scan after eight cycles
of chemotherapy. The patient underwent
surgery to remove any residual disease.
(D) CT scan 1 year after surgery. Patient
continues to be without evidence of
disease.
1548 CANCER October 1, 2004 / Volume 101 / Number 7
Sarcomatoid differentiation of RCC occurs in allhistologic subtypes of RCC, with the incidence rangingfrom 1.2% to 23.6% of RCCs.9 It is uniformly associatedwith a poor prognosis, with a median survival rangingfrom 2 to 9 months.7–9,13 Surgery alone is often inad-equate to cure patients, although there is no provenrole for adjuvant therapy. Cangiano et al.17 reportedthat patients with sarcomatoid differentiation who re-ceived high-dose IL-2 had an improved survival. how-ever, this may represent patient selection. Althoughsome reviews suggest that the presence of � 50% ofsarcomatoid features in the primary tumor portends aworse prognosis,7 other studies do not support thispremise.17 Recent analysis of prognostic factors forsurvival in patients continues to show that sarcoma-toid differentiation is associated with an inferior prog-nosis.18 –20
Systemic therapy for patients with metastatic sar-comatoid RCC has routinely been ineffective. Sella etal.21 reviewed the M. D. Anderson Cancer Center ex-perience and found that patients who received a doxo-rubicin-based regimen were the only long-term survi-vors. Responses have also been reported using theMAID regimen (sodium mercaptoethanesulfonate,doxorubicin, ifosfamide, and dacarbazine),22 and re-cently using gemcitabine, docetaxel, and carbopla-tin.23 In contrast, no responses were observed in pa-tients receiving doxorubicin and ifosfamide. In thecurrent study, we also elected to use chemotherapy totreat patients without a histologic diagnosis of sarco-matoid RCC but with rapidly progressive clinical dis-ease. In our experience, many of these patients areyoung, with either locally advanced or metastatic dis-ease at the time of initial presentation. Immunother-apy regimens are ineffective and patients typically die
FIGURE 2. Computed tomography images of patient with needle biopsy–
diagnosed liver metastases from renal carcinoma. (A) Before chemotherapy. (B)
After two cycles of chemotherapy.
TABLE 4Gemcitabine-Containing Regimens
Regimen DoseResponses(% of all patients) Reference
Gemcitabine 800–1250 mg/m2 on Days 1, 8, and 15 of 28 1 PR (6) Mertens et al., 199327
Gemcitabine 800 mg/m2 on Days 1, 8, and 15 of 28 1 CR, 2 PRs (8.1) de Mulder et al., 199628
Gemcitabine � CIV 5-FU Gemcitabine: 600 mg/m2 on Days 1, 8, and 15 of 28; 5-FU: 150 mg/m2 per day onDays 1–21
0 CRs, 7 PRs (17) Rini et al., 20005
Gemcitabine � cisplatin �CIV 5-FU
Gemcitabine: 600 mg/m2 on Days 1, 8, and 15 of 28; cisplatin: 20 mg/m2 on Days 1, 8,and 15; 5-FU: 150 mg/m2 per day on Days 1–21
0 CRs, 1 PR (5) George et al., 200229
Gemcitabine � CIV 5-FU �thalidomide
Gemcitabine: 600 mg/m2 on Days 1, 8, and 15 of 28; 5-FU: 150 mg/m2 per day onDays 1–21; thalidomide: administered on Days 1–28
0 CRs, 2 PRs (10) Desai et al., 200230
Gemcitabine � IFN � IL-2 Gemcitabine: 1000 mg/m2 on Days 1, 8, and 15 of 28; IFN: 3 IU administered IM 3times weekly; IL-2: 4.6 � 106 IU administered SQ 5 days per week
1 CR, 3 PRs (28) Neri et al., 200216
Gemcitabine � 5-FU � IL-2 Gemcitabine: 600 mg/m2 on Days 1, 8, and 15 of 28; 5-FU: 150 mg/m2 per day onDays 1–21; IL-2: 11 � 106 IU administered SQ 4 days per week
1 CR, 5 PRs (14.6) Ryan et al., 200231
PR: partial response; CR: complete response; CIV: continuous intravenous; 5-FU: 5-fluorouracil; MU: megaunits; IFN: interferon; IL-2: interleukin-2; IM: intramuscularly; SQ: subcutaneously; IU: international units.
Chemotherapy for Sarcomatoid RCC/Nanus et al. 1549

within a few months of diagnosis. As reported in thecurrent study, chemotherapy with doxorubicin andgemcitabine can reverse clinical deterioration in somepatients, and cause stabilization or regression of me-tastases. It is unclear why the combination of gem-citabine and doxorubicin appeared to be more ef-fective in our study than that observed in previousregimens with either drug alone. This may resultfrom the high dose of gemcitabine in the currentregimen compared with that used in the Phase IIsingle-agent studies for patients with RCC, or thatthe combination of an anthracylcine and gemcitab-ine results in improved efficacy, as has been sug-gested by other clinical trials in a variety of malig-nancies using this combination.15,24 –26
In summary, RCC is correctly considered a che-motherapy-resistant tumor with most patients withclear cell carcinoma resistant to cytotoxic agents.However, we suggest that in certain instances, such aspatients with sarcomatoid RCC or patients with rap-idly progressing tumors (i.e., 25–50% objective pro-gression over 1–2 months), combination chemother-apy should be considered for therapy. A proposedclinical ECOG trial will formally study this regimen inpatients with RCC with sarcomatoid differentiationusing a dose of 1500 mg/m2 of gemcitabine and 50mg/m2 of doxorubicin every 2 weeks with growth fac-tor support. Clearly, molecular studies are needed tomore accurately characterize RCCs to identify whichpatients will specifically benefit from this approach, aswell as which patients will benefit from immunother-apy or other newer therapies.
REFERENCES1. Milowsky MI, Nanus DM. Chemotherapeutic strategies for
renal cell carcinoma. Urol Clin North Am. 2003;30:601– 609.2. Yagoda A, Petrylak D, Thompson S. Cytotoxic chemotherapy
for advanced renal cell carcinoma. Urol Clin North Am.1993;20:303–321.
3. Amato RJ. Chemotherapy for renal cell carcinoma. SeminOncol. 2000;27:177–186.
4. Motzer RJ, Russo P. Systemic therapy for renal cell carci-noma. J Urol. 2000;163:408 – 417.
5. Rini BI, Vogelzang NJ, Dumas MC, Wade JL III, Taber DA,Stadler WM. Phase II trial of weekly intravenous gemcitab-ine with continuous infusion fluorouracil in patients withmetastatic renal cell cancer. J Clin Oncol. 2000;18:2419 –2426.
6. Bleumer I, Oosterwijk E, De Mulder P, Mulders PF. Immu-notherapy for renal cell carcinoma. Eur Urol. 2003;44:65–75.
7. Peralta-Venturina M, Moch H, Amin M, et al. Sarcomatoiddifferentiation in renal cell carcinoma: a study of 101 cases.Am J Surg Pathol. 2001;25:275–284.
8. Cheville JC, Lohse CM, Zincke H, Weaver AL, Blute ML.Comparisons of outcome and prognostic features amonghistologic subtypes of renal cell carcinoma. Am J SurgPathol. 2003;27:612– 624.
9. Mian BM, Bhadkamkar N, Slaton JW, et al. Prognostic fac-
tors and survival of patients with sarcomatoid renal cellcarcinoma. J Urol. 2002;167:65–70.
10. Culine S, Bekradda M, Terrier-Lacombe MJ, Droz JP. Treat-ment of sarcomatoid renal cell carcinoma: is there a role forchemotherapy? Eur Urol. 1995;27:138 –141.
11. Bangalore N, Bhargava P, Hawkins MJ, et al. Sustained re-sponse of sarcomatoid renal-cell carcinoma to MAID che-motherapy: case report and review of the literature. AnnOncol. 2001;12:271–274.
12. Amato RJ. Therapy for patients with uncommon histologicvarieties of renal cell carcinoma. In: Bukowski RM, NovickAC, editors. Renal cell carcinoma: molecular biology, immu-nology, and clinical management. Totowa, NJ: HumanaPress, 2000:397– 405.
13. Escudier B, Droz JP, Rolland F, et al. Doxorubicin and ifos-famide in patients with metastatic sarcomatoid renal cellcarcinoma: a phase II study of the Genitourinary Group ofthe French Federation of Cancer Centers. J Urol. 2002;168:959 –961.
14. Milowsky MI, Rosmarin A, Tickoo SK, Papanicolaou N, Na-nus DM. Active chemotherapy for collecting duct carcinomaof the kidney: a case report and review of the literature.Cancer. 2002;94:111–116.
15. Dodd PM, McCaffrey JA, Hilton S, et al. Phase I evaluation ofsequential doxorubicin, gemcitabine then ifosfamide, pac-litaxel, cisplatin for patients with unresectable or metastatictransitional-cell carcinoma of the urothelial tract. J ClinOncol. 2000;18:840 – 846.
16. Neri B, Doni L, Gemelli MT, et al. Phase II trial of weeklyintravenous gemcitabine administration with interferon andinterleukin-2 immunotherapy for metastatic renal cell can-cer. J Urol. 2002;168:956 –958.
17. Cangiano T, Liao J, Naitoh J, Dorey F, Figlin R, Belldegrun A.Sarcomatoid renal cell carcinoma: biologic behavior, prog-nosis, and response to combined surgical resection andimmunotherapy. J Clin Oncol. 1999;17:523–528.
18. Grabowski M, Huzarski T, Lubinski J, Sikorski A. Survival inpatients with rare subtypes of renal cell carcinoma. BJU Int.2002;89:599 – 600.
19. Leibovich BC, Han KR, Bui MH, et al. Scoring algorithm topredict survival after nephrectomy and immunotherapy inpatients with metastatic renal cell carcinoma: a stratificationtool for prospective clinical trials. Cancer. 2003;98:2566–2575.
20. Stadler WM, Huo D, George C, et al. Prognostic factors forsurvival with gemcitabine plus 5-fluorouracil based regimensfor metastatic renal cancer. J Urol. 2003;170:1141–1145.
21. Sella A, Logothetis CJ, Ro JY, Swanson DA, Samuels ML.Sarcomatoid renal cell carcinoma. A treatable entity. Cancer.1987;60:1313–1318.
22. Bangalore N, Bhargava P, Hawkins MJ, Bhargava P. Sus-tained response of sarcomatoid renal-cell carcinoma toMAID chemotherapy: case report and review of the litera-ture. Ann Oncol. 2001;12:271–274.
23. Hoshi S, Satoh M, Ohyama C, et al. Active chemotherapy forbone metastasis in sarcomatoid renal cell carcinoma. IntJ Clin Oncol. 2003;8:113–117.
24. Neri B, Cini G, Doni L, et al. Weekly gemcitabine plusepirubicin as effective chemotherapy for advanced pancre-atic cancer: a multicenter phase II study. Br J Cancer. 2002;87:497–501.
25. Neri B, Doni L, Fulignati C, et al. Gemcitabine plus epi-doxorubicin as first-line chemotherapy for bladder cancer inadvanced or metastatic stage: a phase II [sic]. Anticancer Res.2002;22:2981–2984.
1550 CANCER October 1, 2004 / Volume 101 / Number 7

26. Jassem J. Gemcitabine and anthracyclines in breast cancer.Semin Oncol. 2003;30:11–14.
27. Mertens WC, Eisenhauer EA, Moore M, et al. Gemcitabine inadvanced renal cell carcinoma. A phase II study of theNational Cancer Institute of Canada Clinical Trials Group.Ann Oncol. 1993;4:331–332.
28. de Mulder PH, Weissbach L, Jakse G, Osieka R, Blatter J. Gem-citabine: a phase II study in patients with advanced renalcancer. Cancer Chemother Pharmacol. 1996;37:491–495.
29. George CM, Vogelzang NJ, Rini BI, Geoffroy FJ, Kollipara P,Stadler WM. A phase II trial of weekly intravenous gemcit-abine and cisplatin with continuous infusion fluorouracil in
patients with metastatic renal cell carcinoma. Ann Oncol.2002;13:116 –120.
30. Desai AA, Vogelzang NJ, Rini BI, Ansari R, Krauss S, StadlerWM. A high rate of venous thromboembolism in a multi-institutional phase II trial of weekly intravenous gemcitab-ine with continuous infusion fluorouracil and daily thalid-omide in patients with metastatic renal cell carcinoma.Cancer. 2002;95:1629 –1636.
31. Ryan CW, Vogelzang NJ, Stadler WM. A phase II trial ofintravenous gemcitabine and 5-fluorouracil with subcuta-neous interleukin-2 and interferon-� in patients with met-astatic renal cell carcinoma. Cancer. 2002;94:2602–2609.
Chemotherapy for Sarcomatoid RCC/Nanus et al. 1551