Embed Size (px)
Citation preview
Please see Prescribing Information for RADICAVA®, also available at radicavahcp.com.
Helping Provide Access to RADICAVA® (edaravone)
RESOURCE GUIDEActor portrayals.

Please see Prescribing Information for RADICAVA® (edaravone), also available at radicavahcp.com.
Searchlight Support® Care CoordinatorsKnowledgeable navigators of the treatment process.
The access program is ready with personalized support and resources for patients, caregivers, and healthcare providers
• Benefit verification• Limited Prior Authorization assistance• Understanding health plan options• Navigating exceptions and appeals information• Out-of-pocket cost support• Patient site of care coordination• General information about:
– Reimbursement support– Coding and billing
Our Care Team is dedicated to helping navigate product access challenges
Actor portrayals.
2
Please see Prescribing Information for RADICAVA® (edaravone), also available at radicavahcp.com.
Starting patients on RADICAVA® (edaravone) ����������������������������������������������������4
We can help with access to treatment for patients
• Benefit investigation and verification of benefits• Limited Prior Authorization (PA) support*• Assistance with understanding the health plan exceptions
and appeals process
Identifying options to help patients afford treatment �������������������������������������������8
Learn about the out-of-pocket cost support options available to patients
• Out-of-pocket Assistance Program for eligible, commercially insured patients
• Information about government health plan coverage• Other affordability options
Locating resources for the ALS community ����������������������������������������������������������12
Online ALS Care Locator helps find infusion sites of care for patients who receive RADICAVA®
• Uses patient preferences to locate sites of care, including home infusion services
• Designed to help locate other resources for ALS community
Helping your office with product access challengesPrior Authorization | Navigating Exceptions and Appeals Information | Coding and Billing Information
* Searchlight Support® does not fill out any information that requires the medical judgment of the prescriber and only the prescriber can determine whether to pursue a Prior Authorization.
A comprehensive approach to access, affordability, and treatment support
3
Please see Prescribing Information for RADICAVA® (edaravone), also available at radicavahcp.com.
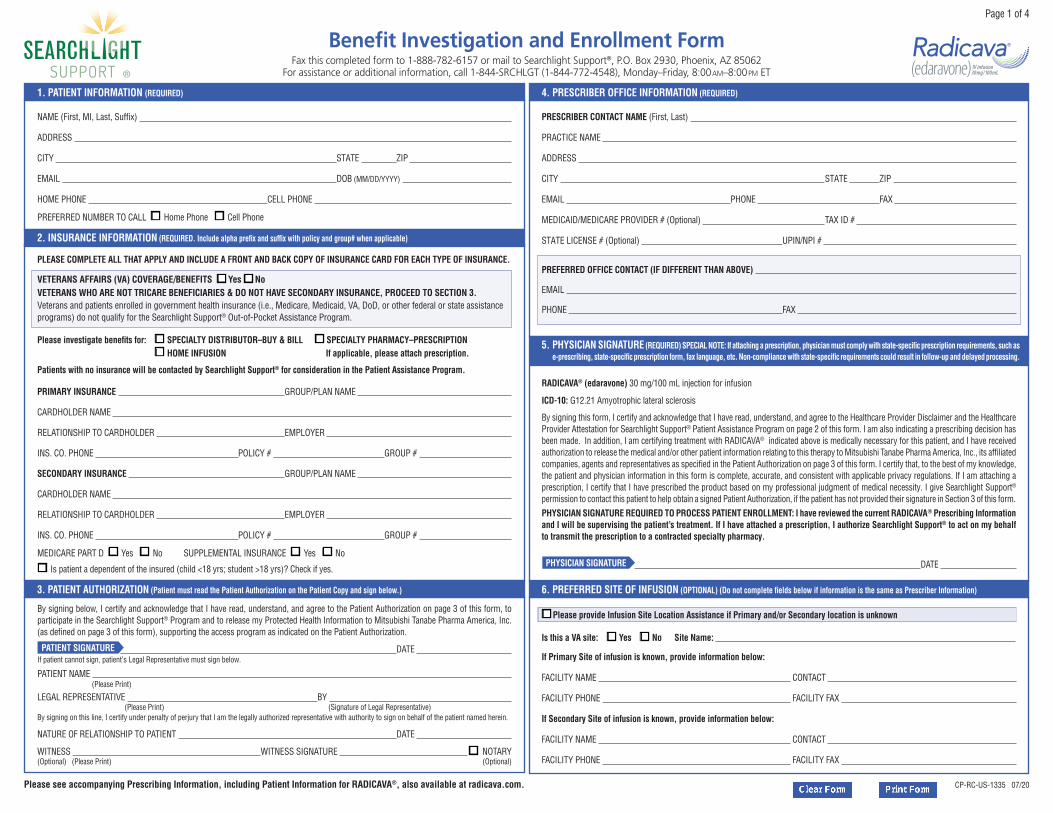
Starting patients on RADICAVA®
(edaravone)
Begin with the Benefit Investigation and Enrollment Form, and submit to Searchlight Support®
• A patient or their Legal Representative signature is required in Section 3
• The prescriber signature is required in Section 5*
• Indicate the preferred site of infusion in Section 6, if known
A completed Benefit Investigation and Enrollment Form connects your office and your patients with personalized support.†
RADICAVA® (edaravone) 30 mg/100 mL injection for infusion
ICD-10: G12.21 Amyotrophic lateral sclerosis
By signing this form, I certify and acknowledge that I have read, understand, and agree to the Healthcare Provider Disclaimer and the Healthcare Provider Attestation for Searchlight Support® Patient Assistance Program on page 2 of this form. I am also indicating a prescribing decision has been made. In addition, I am certifying treatment with RADICAVA® indicated above is medically necessary for this patient, and I have received authorization to release the medical and/or other patient information relating to this therapy to Mitsubishi Tanabe Pharma America, Inc., its affiliated companies, agents and representatives as specified in the Patient Authorization on page 3 of this form. I certify that, to the best of my knowledge, the patient and physician information in this form is complete, accurate, and consistent with applicable privacy regulations. If I am attaching a prescription, I certify that I have prescribed the product based on my professional judgment of medical necessity. I give Searchlight Support® permission to contact this patient to help obtain a signed Patient Authorization, if the patient has not provided their signature in Section 3 of this form.PHYSICIAN SIGNATURE REQUIRED TO PROCESS PATIENT ENROLLMENT: I have reviewed the current RADICAVA® Prescribing Information and I will be supervising the patient’s treatment. If I have attached a prescription, I authorize Searchlight Support® to act on my behalf to transmit the prescription to a contracted specialty pharmacy.
PHYSICIAN SIGNATURE DATE
By signing below, I certify and acknowledge that I have read, understand, and agree to the Patient Authorization on page 3 of this form, to participate in the Searchlight Support® Program and to release my Protected Health Information to Mitsubishi Tanabe Pharma America, Inc. (as defined on page 3 of this form), supporting the access program as indicated on the Patient Authorization.
PATIENT SIGNATURE DATE If patient cannot sign, patient’s Legal Representative must sign below.
PATIENT NAME (Please Print)
LEGAL REPRESENTATIVE BY (Please Print) (Signature of Legal Representative)By signing on this line, I certify under penalty of perjury that I am the legally authorized representative with authority to sign on behalf of the patient named herein.
NATURE OF RELATIONSHIP TO PATIENT DATE
WITNESS WITNESS SIGNATURE q NOTARY (Optional) (Please Print) (Optional)
Benefit Investigation and Enrollment FormFax this completed form to 1-888-782-6157 or mail to Searchlight Support®, P.O. Box 2930, Phoenix, AZ 85062
For assistance or additional information, call 1-844-SRCHLGT (1-844-772-4548), Monday–Friday, 8:00am–8:00pm ET
Page 1 of 4
NAME (First, MI, Last, Suffix)
ADDRESS
CITY STATE ZIP
EMAIL DOB (MM/DD/YYYY)
HOME PHONE CELL PHONE
PREFERRED NUMBER TO CALL q Home Phone q Cell Phone
1. PATIENT INFORMATION (REQUIRED)
Please see accompanying Prescribing Information, including Patient Information for RADICAVA®, also available at radicava.com. CP-RC-US-1335 07/20
PLEASE COMPLETE ALL THAT APPLY AND INCLUDE A FRONT AND BACK COPY OF INSURANCE CARD FOR EACH TYPE OF INSURANCE.
VETERANS AFFAIRS (VA) COVERAGE/BENEFITS q Yes q No VETERANS WHO ARE NOT TRICARE BENEFICIARIES & DO NOT HAVE SECONDARY INSURANCE, PROCEED TO SECTION 3. Veterans and patients enrolled in government health insurance (i.e., Medicare, Medicaid, VA, DoD, or other federal or state assistance programs) do not qualify for the Searchlight Support® Out-of-Pocket Assistance Program.
Please investigate benefits for: q SPECIALTY DISTRIBUTOR–BUY & BILL q SPECIALTY PHARMACY–PRESCRIPTION
q HOME INFUSION If applicable, please attach prescription.
Patients with no insurance will be contacted by Searchlight Support® for consideration in the Patient Assistance Program.
PRIMARY INSURANCE GROUP/PLAN NAME
CARDHOLDER NAME
RELATIONSHIP TO CARDHOLDER EMPLOYER
INS. CO. PHONE POLICY # GROUP #
SECONDARY INSURANCE GROUP/PLAN NAME
CARDHOLDER NAME
RELATIONSHIP TO CARDHOLDER EMPLOYER
INS. CO. PHONE POLICY # GROUP #
MEDICARE PART D q Yes q No SUPPLEMENTAL INSURANCE q Yes q No
q Is patient a dependent of the insured (child <18 yrs; student >18 yrs)? Check if yes.
2. INSURANCE INFORMATION (REQUIRED. Include alpha prefix and suffix with policy and group# when applicable)
5. PHYSICIAN SIGNATURE (REQUIRED) SPECIAL NOTE: If attaching a prescription, physician must comply with state-specific prescription requirements, such as e-prescribing, state-specific prescription form, fax language, etc. Non-compliance with state-specific requirements could result in follow-up and delayed processing.
PRESCRIBER CONTACT NAME (First, Last)
PRACTICE NAME
ADDRESS
CITY STATE ZIP
EMAIL PHONE FAX
MEDICAID/MEDICARE PROVIDER # (Optional) TAX ID #
STATE LICENSE # (Optional) UPIN/NPI #
PREFERRED OFFICE CONTACT (IF DIFFERENT THAN ABOVE)
PHONE FAX
4. PRESCRIBER OFFICE INFORMATION (REQUIRED)
3. PATIENT AUTHORIZATION (Patient must read the Patient Authorization on the Patient Copy and sign below.)
q Please provide Infusion Site Location Assistance if Primary and/or Secondary location is unknown
Is this a VA site: q Yes q No Site Name:
If Primary Site of infusion is known, provide information below:
FACILITY NAME CONTACT
FACILITY PHONE FACILITY FAX
If Secondary Site of infusion is known, provide information below:
FACILITY NAME CONTACT
FACILITY PHONE FACILITY FAX
6. PREFERRED SITE OF INFUSION (OPTIONAL) (Do not complete fields below if information is the same as Prescriber Information)
* A valid prescriber signature is required to allow Searchlight Support® to contact the patient. Let your patient know that Searchlight Support® will be contacting them.
† Searchlight Support® cannot enroll patients in Searchlight Support® services without Patient Authorization, which can be found on the Benefit Investigation and Enrollment Form, or a separate signed Patient Authorization Form for RADICAVA® on file. In addition, a Searchlight Support® Benefit Investigation and Enrollment Form must be submitted for each patient for whom treatment with RADICAVA® is requested.
Patient insurance benefit investigation is provided as a service by RxC Acquisition Company d.b.a. RxCrossroads by McKesson under contract for Mitsubishi Tanabe Pharma America, Inc. (“Mitsubishi Tanabe Pharma America”). RxCrossroads by McKesson provides assistance in determining whether treatment can be covered by the payer based on the payer’s health plan guidelines and the patient information you provided as authorized by the patient on the Benefit Investigation and Enrollment Form, following your determination of medical necessity.
Verification of insurance coverage is ultimately the responsibility of the provider. Since reimbursement by payers is subject to many factors, RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America do not represent or guarantee that payer reimbursement or any other payment or reimbursement of any kind will be made. RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America do not reimburse for claims denied by payers. Information provided as a result of the benefit investigation is provided for general reference and informational purposes only. RxCrossroads by McKesson makes every effort to be accurate in the information provided; however, no representations or warranties are expressed or implied by RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America regarding the accuracy or reliability of the information. RxCrossroads by McKesson or Mitsubishi Tanabe Pharma America, or its agents or employees shall not be liable legally, financially, or otherwise, for damages of any kind as a result of or related to these services. Providers and other users of this information resulting from benefit investigation services accept full responsibility for use of the service.
Mitsubishi Tanabe Pharma America does not assume responsibility for, nor does it guarantee the availability, scope, or quality of the services offered including reimbursement support, prescription fulfillment coordination, and other services under Searchlight Support®. Providers, not Mitsubishi Tanabe Pharma America, are responsible for the services they provide. The Searchlight Support® services have no value apart from the product.
See Options to Submit on next page
4
Please see Prescribing Information for RADICAVA® (edaravone), also available at radicavahcp.com.
Two ways to submit a Benefit Investigation and Enrollment Form to Searchlight Support®*
RADICAVA® (edaravone) 30 mg/100 mL injection for infusion
ICD-10: G12.21 Amyotrophic lateral sclerosis
By signing this form, I certify and acknowledge that I have read, understand, and agree to the Healthcare Provider Disclaimer and the Healthcare Provider Attestation for Searchlight Support® Patient Assistance Program on page 2 of this form. I am also indicating a prescribing decision has been made. In addition, I am certifying treatment with RADICAVA® indicated above is medically necessary for this patient, and I have received
the patient and physician information in this form is complete, accurate, and consistent with applicable privacy regulations. If I am attaching a prescription, I certify that I have prescribed the product based on my professional judgment of medical necessity. I give Searchlight Support® permission to contact this patient to help obtain a signed Patient Authorization, if the patient has not provided their signature in Section 3 of this form.PHYSICIAN SIGNATURE REQUIRED TO PROCESS PATIENT ENROLLMENT: I have reviewed the current RADICAVA® Prescribing Information and I will be supervising the patient’s treatment. If I have attached a prescription, I authorize Searchlight Support® to act on my behalf to transmit the prescription to a contracted specialty pharmacy.
PHYSICIAN SIGNATURE DATE
By signing below, I certify and acknowledge that I have read, understand, and agree to the Patient Authorization on page 3 of this form, to participate in the Searchlight Support® Program and to release my Protected Health Information to Mitsubishi Tanabe Pharma America, Inc.
am as indicated on the Patient Authorization.
PATIENT SIGNATURE DATE If patient cannot sign, patient’s Legal Representative must sign below.
PATIENT NAME (Please Print)
LEGAL REPRESENTATIVE BY (Please Print) (Signature of Legal Representative)By signing on this line, I certify under penalty of perjury that I am the legally authorized representative with authority to sign on behalf of the patient named herein.
NATURE OF RELATIONSHIP TO PATIENT DATE
WITNESS WITNESS SIGNATURE NOTARY (Optional) (Please Print) (Optional)
Benefit Investigation and Enrollment FormFax this completed form to 1-888-782-6157 or mail to Searchlight Support®, P.O. Box 2930, Phoenix, AZ 85062
For assistance or additional information, call 1-844-SRCHLGT (1-844-772-4548), Monday–Friday, 8:00AM–8:00PM ET
Page 1 of 4
ADDRESS
CITY STATE ZIP
EMAIL DOB (MM/DD/YYYY)
HOME PHONE CELL PHONE
PREFERRED NUMBER TO CALL Home Phone Cell Phone
1. PATIENT INFORMATION (REQUIRED)
Please see accompanying Prescribing Information, including Patient Information for RADICAVA®, also available at radicava.com. CP-RC-US-1327 08/20
PLEASE COMPLETE ALL THAT APPLY AND INCLUDE A FRONT AND BACK COPY OF INSURANCE CARD FOR EACH TYPE OF INSURANCE.
VETERANS AFFAIRS (VA) COVERAGE/BENEFITS Yes No VETERANS WHO ARE NOT TRICARE BENEFICIARIES & DO NOT HAVE SECONDARY INSURANCE, PROCEED TO SECTION 3. Veterans and patients enrolled in government health insurance (i.e., Medicare, Medicaid, VA, DoD, or other federal or state assistance programs) do not qualify for the Searchlight Support® Out-of-Pocket Assistance Program.
SPECIALTY DISTRIBUTOR–BUY & BILL SPECIALTY PHARMACY–PRESCRIPTION
HOME INFUSION If applicable, please attach prescription.
Patients with no insurance will be contacted by Searchlight Support® for consideration in the Patient Assistance Program.
PRIMARY INSURANCE GROUP/PLAN NAME
CARDHOLDER NAME
RELATIONSHIP TO CARDHOLDER EMPLOYER
INS. CO. PHONE POLICY # GROUP #
SECONDARY INSURANCE GROUP/PLAN NAME
CARDHOLDER NAME
RELATIONSHIP TO CARDHOLDER EMPLOYER
INS. CO. PHONE POLICY # GROUP #
MEDICARE PART D Yes No SUPPLEMENTAL INSURANCE Yes No
Is patient a dependent of the insured (child <18 yrs; student >18 yrs)? Check if yes.
2. INSURANCE INFORMATION when applicable)
5. PHYSICIAN SIGNATURE
PRESCRIBER CONTACT NAME (First, Last)
PRACTICE NAME
ADDRESS
CITY STATE ZIP
EMAIL PHONE FAX
MEDICAID/MEDICARE PROVIDER # (Optional) TAX ID #
STATE LICENSE # (Optional) UPIN/NPI #
PREFERRED OFFICE CONTACT (IF DIFFERENT THAN ABOVE)
PHONE FAX
4. PRESCRIBER OFFICE INFORMATION (REQUIRED)
3. PATIENT AUTHORIZATION (Patient must read the Patient Authorization on the Patient Copy and sign below.)
Please provide Infusion Site Location Assistance if Primary and/or Secondary location is unknown
Is this a VA site: Yes No Site Name:
If Primary Site of infusion is known, provide information below:
FACILITY NAME CONTACT
FACILITY PHONE FACILITY FAX
If Secondary Site of infusion is known, provide information below:
FACILITY NAME CONTACT
FACILITY PHONE FACILITY FAX
6. PREFERRED SITE OF INFUSION ame as Prescriber Information)
Sign
Sign
Sign
NOTE: As a reminder, all covered entities are obligated under the Health Insurance Portability and Accountability Act of 1996 (HIPAA) to have a business associate agreement (BAA) in place with any service provider that handles protected health information (PHI) on their behalf. This includes, among others, electronic data transmission services such as DocuSign® and electronic fax services. Please refer to each service provider’s website for more information regarding BAAs and PHI.
* Mitsubishi Tanabe Pharma America, Inc. (“MTPA”) is not affiliated with DocuSign® or any electronic fax service providers (collectively, “service providers”). No fees or remuneration of any kind have been or will be exchanged with any healthcare provider for use of these service providers. Mention of these service providers does not constitute a referral, recommendation, endorsement of a particular service provider, and similarly, the absence of a service provider’s name should not be construed as a negative comment from MTPA about that service provider. MTPA, as well as its employees or agents, shall not be held liable for any damages or harm resulting from any use or reliance on these service providers, and MTPA may modify its policy regarding these service providers at any time without notice.
Patient authorization is required. If not provided in the Benefit Investigation and Enrollment Form, Searchlight Support® will contact the patient about the need to obtain a signed Patient Authorization Form.
Online via DocuSign® PowerForm with electronic signature capability
• Access the DocuSign® PowerForm at radicavahcp.com
• Follow the onscreen instructions to complete, sign, and submit
• Use the “paper clip” attachment feature to include a prescription and patient insurance documentation with your submission
If you have access to a printer
• Download and save the editable form at radicavahcp.com
• Complete and sign form
• Print, sign, scan, or photograph. Submit form using:
Mail: PO Box 2930, Phoenix, AZ 85062Fax or Electronic Fax: 1-888-782-6157
Benefit Investigation and Enrollment FormFax this completed form to 1-888-782-6157 or mail to Searchlight Support®, P.O. Box 2930, Phoenix, AZ 85062
For assistance or additional information, call 1-844-SRCHLGT (1-844-772-4548), Monday–Friday, 8:00am–8:00pm ET
Page 1 of 4
NAME (First, MI, Last, Suffix)
ADDRESS
CITY STATE ZIP
EMAIL DOB (MM/DD/YYYY)
HOME PHONE CELL PHONE
PREFERRED NUMBER TO CALL q Home Phone q Cell Phone
1. PATIENT INFORMATION (REQUIRED)
Please see accompanying Prescribing Information, including Patient Information, for RADICAVA®, also available at radicava.com.
PLEASE COMPLETE ALL THAT APPLY AND INCLUDE A FRONT AND BACK COPY OF INSURANCE CARD FOR EACH TYPE OF INSURANCE.
Please investigate benefits for: q SPECIALTY DISTRIBUTOR–BUY & BILL q SPECIALTY PHARMACY–PRESCRIPTION
q HOME INFUSION If applicable, please attach prescription.
Patients with no insurance will be contacted by Searchlight Support® for consideration in the Patient Assistance Program.
PRIMARY INSURANCE GROUP/PLAN NAME
CARDHOLDER NAME
RELATIONSHIP TO CARDHOLDER EMPLOYER
INS. CO. PHONE POLICY # GROUP #
SECONDARY INSURANCE GROUP/PLAN NAME
CARDHOLDER NAME
RELATIONSHIP TO CARDHOLDER EMPLOYER
INS. CO. PHONE POLICY # GROUP #
MEDICARE PART D q Yes q No SUPPLEMENTAL INSURANCE q Yes q No
q Is patient a dependent of the insured (child <18 yrs; student >18 yrs)? Check if yes.
2. INSURANCE INFORMATION (REQUIRED. Include alpha prefix and suffix with policy and group# when applicable)
5. PHYSICIAN SIGNATURE (REQUIRED) SPECIAL NOTE: If attaching a prescription, physician must comply with state-specific prescription requirements, such as e-prescribing, state-specific prescription form, fax language, etc. Non-compliance with state-specific requirements could result in follow-up and delayed processing.
RADICAVA® (edaravone) 30 mg/100 mL injection for infusion
ICD-10: G12.21 Amyotrophic lateral sclerosis
By signing this form, I certify and acknowledge that I have read, understand, and agree to the Healthcare Provider Disclaimer and the Healthcare Provider Attestation for Searchlight Support® Patient Assistance Program on page 2 of this form. I am also indicating a prescribing decision has been made. In addition, I am certifying treatment with RADICAVA® indicated above is medically necessary for this patient, and I have received authorization to release the medical and/or other patient information relating to this therapy to Mitsubishi Tanabe Pharma America, Inc., its affiliated companies, agents and representatives as specified in the Patient Authorization on page 3 of this form. I certify that, to the best of my knowledge, the patient and physician information in this form is complete, accurate, and consistent with applicable privacy regulations. If I am attaching a prescription, I certify that I have prescribed the product based on my professional judgment of medical necessity. I give Searchlight Support® permission to contact this patient to help obtain a signed Patient Authorization, if the patient has not provided their signature in Section 3 of this form.PHYSICIAN SIGNATURE REQUIRED TO PROCESS PATIENT ENROLLMENT: I have reviewed the current RADICAVA® Prescribing Information and I will be supervising the patient’s treatment. If I have attached a prescription, I authorize Searchlight Support® to act on my behalf to transmit the prescription to a contracted specialty pharmacy.
PHYSICIAN SIGNATURE DATE
q Please provide Infusion Site Location Assistance if Primary and/or Secondary location is unknown
If Primary Site of infusion is known, provide information below:
FACILITY NAME CONTACT
FACILITY PHONE FACILITY FAX
If Secondary Site of infusion is known, provide information below:
FACILITY NAME CONTACT
FACILITY PHONE FACILITY FAX
6. PREFERRED SITE OF INFUSION (OPTIONAL) (Do not complete fields below if information is the same as Prescriber Information)
PRESCRIBER CONTACT NAME (First, Last)
PRACTICE NAME
ADDRESS
CITY STATE ZIP
PHONE FAX
MEDICAID/MEDICARE PROVIDER # STATE LICENSE # UPIN/NPI #
PREFERRED OFFICE CONTACT (IF DIFFERENT THAN ABOVE)
PHONE FAX
4. PRESCRIBER OFFICE INFORMATION (REQUIRED)
By signing below, I certify and acknowledge that I have read, understand, and agree to the Patient Authorization on page 3 of this form, to participate in the Searchlight Support® Program and to release my Protected Health Information to Mitsubishi Tanabe Pharma America, Inc. (as defined on page 3 of this form), supporting the access program as indicated on the Patient Authorization.
PATIENT SIGNATURE DATE If patient cannot sign, patient’s Legal Representative must sign below.
PATIENT NAME (Please Print)
LEGAL REPRESENTATIVE BY (Please Print) (Signature of Legal Representative)By signing on this line, I certify under penalty of perjury that I am the legally authorized representative with authority to sign on behalf of the patient named herein.
NATURE OF RELATIONSHIP TO PATIENT DATE
WITNESS WITNESS SIGNATURE q NOTARY (Optional) (Please Print) (Optional)
3. PATIENT AUTHORIZATION (Patient must read the Patient Authorization on the Patient Copy and sign below.)
Sign
See options for submitting a signed Patient Authorization Form on next page
5
Please see Prescribing Information for RADICAVA® (edaravone), also available at radicavahcp.com.
Options for submitting a signed Patient Authorization Form
If you are unable to obtain a signature from a patient or their Legal Representative on the Benefit Investigation and Enrollment Form, they may submit a signed Patient Authorization Form.*
1. A patient or their Legal Representative may access a link to the DocuSign® PowerForm available at radicava.com and submit with electronic signature.
2. Searchlight Support® can email a link to the DocuSign® Patient Authorization Form to the patient.
3. You can advise your patient or their Legal Representative to download, complete, and sign the Patient Authorization Form available at radicava.com, and submit by electronic fax, conventional fax, or USPS mail.
4. Searchlight Support® will mail your patient or their Legal Representative a copy of the Patient Authorization Form to return by electronic fax, conventional fax, or USPS mail.
Mail: PO Box 2930, Phoenix, AZ 85062Fax or Electronic Fax: 1-888-782-6157
RADICAVA, the RADICAVA logo, and the corporate symbol of Mitsubishi Tanabe Pharma America are registered trademarks of Mitsubishi Tanabe Pharma Corporation. Searchlight Support is a registered trademark of Mitsubishi Tanabe Pharma America, Inc. For US audiences only.Mitsubishi Tanabe Pharma America, Inc.525 Washington Boulevard, Suite 400Jersey City, NJ 07310© 2020 Mitsubishi Tanabe Pharma America, Inc. All rights reserved. CP-RC-US-1342 04/20
Please see accompanying Prescribing Information, including Patient Information, for Radicava®, also available at radicava.com.
Patient Authorization Form for RADICAVA® (edaravone) (continued)
This Authorization will remain in effect for 5 years from the date of my signature, or until I am no longer participating in Searchlight Support® services, whichever is sooner. A copy of this Authorization will be as valid as the original. I may cancel this Authorization at any time in writing by mailing a letter to Searchlight Support®, P.O. Box 2930, Phoenix, AZ 85062. I can also cancel my Authorization by informing my Healthcare Providers and Insurers in writing that I do not want them to share any information with Mitsubishi Tanabe Pharma America. Cancelling this authorization will not affect the ability of Mitsubishi Tanabe Pharma America to use and disclose Protected Health Information that it has received prior to receipt of the cancellation of my Authorization. My Authorization will also end if Searchlight Support® is discontinued. Furthermore, I understand that I have the right to see or copy the Protected Health Information my Healthcare Providers or Insurers have given to Mitsubishi Tanabe Pharma America.
Patient Name: Date of Birth (mm/dd/yyyy):
Patient Address:
City: State: ZIP Code:
I have read this Form and understand that signing this Authorization is voluntary. By signing below, I acknowledge that I have read, understood and accept all of the above.
Patient Signature: Date:
PATIENT ACKNOWLEDGMENTMy signature above on this Patient Authorization Form (the “Form”) for RADICAVA® serves as confirmation of the following:
• If I am eligible to participate in the Searchlight Support® Patient Assistance Program (the “Program”), I agree to notify Searchlight Support® if my insurance situation changes, and I understand that upon obtaining health insurance, I will no longer be eligible to participate in the Program and that Searchlight Support® Patient Assistance Program medication will no longer be dispensed to me.
• My eligibility to receive assistance in the Program will be reviewed every 12 months and may change if I no longer meet the current program eligibility requirements. For program eligibility requirements, terms and conditions, I can refer to the Searchlight Support® Patient Assistance Program brochure.
• Additionally, I acknowledge and agree that I will not seek credit for or otherwise submit any claim for reimbursement to any third-party payer for the RADICAVA® medication provided at no charge by the Program and that I will not seek to have free medication or any associated costs counted towards my Medicare Part D True out-of-pocket (TrOOP) costs for prescription drugs.
• I understand and agree that the Program covers only the cost of RADICAVA® and not the cost of any infusion services or Healthcare Provider visits, which are my sole responsibility.
• I understand that Searchlight Support® has the right to verify my eligibility, including the right to audit any information I provide, and to contact me to confirm receipt of medications.
• I also understand that the Program may be revised, changed or terminated at any time without notice.
If patient cannot sign, patient’s Legal Representative must sign below:
Legal Representative: By: (Please Print) (Signature of Legal Representative)
By signing on this line, I certify under penalty of perjury that I am the legally authorized representative with authority to sign on behalf of the patient named herein.
Nature of Relationship to Patient: Date:
Witness: Witness Signature: Notary (Optional) (Please Print) (Optional)
Fax completed form to 888-782-6157 or mail to Searchlight Support®, P.O. Box 2930, Phoenix, AZ 85062
* Mitsubishi Tanabe Pharma America, Inc. (“MTPA”) is not affiliated with DocuSign® or any electronic fax service providers (collectively, “service providers”). No fees or remuneration of any kind have been or will be exchanged with any healthcare provider for use of these service providers. Mention of these service providers does not constitute a referral, recommendation, endorsement of a particular service provider, and similarly, the absence of a service provider’s name should not be construed as a negative comment from MTPA about that service provider. MTPA, as well as its employees or agents, shall not be held liable for any damages or harm resulting from any use or reliance on these service providers, and MTPA may modify its policy regarding these service providers at any time without notice.
6
Please see Prescribing Information for RADICAVA® (edaravone), also available at radicavahcp.com.
Available support with a completed and signed Benefit Investigation and Enrollment Form
Summary of support:
• Verify insurance benefits within 2 business days
- Advise if a Prior Authorization (PA) is required
- Send a concise benefit summary to your office and your patient
• Limited support for PA and exceptions and appeals process*
- Research patient’s health plan for PA requirements and forms
- Monitor status of the PA submission
- Notify your office within 3 weeks prior to PA expiration
• Provide streamlined product acquisition options
- Via Buy & Bill (through a Limited Distribution Network) or
- Specialty pharmacy, including assignment of medical benefit
Support for your patients:
A Searchlight Support® Care Coordinator will provide care coordination and call patients to explain insurance benefits and out-of-pocket cost support options with follow-up calls, as needed.
Summary of support
* Searchlight Support® does not fill out any information that requires the medical judgment of the prescriber and only the prescriber can determine whether to pursue a Prior Authorization. Determination of Prior Authorization is at the sole discretion of the health plan. Searchlight Support® and Mitsubishi Tanabe Pharma America, Inc., do not assume responsibility for, nor do they guarantee the approval of a Prior Authorization request.
7
Please see Prescribing Information for RADICAVA® (edaravone), also available at radicavahcp.com.
Identifying options to help patients afford treatment
The Benefit Investigation and Enrollment Form activates the Searchlight Support® Out-of-Pocket Assistance Program
Eligible patients with commercial insurance coverage for treatment with RADICAVA® (edaravone) are automatically enrolled in the Program.
Patients may also enroll by completing the Out-of-Pocket Assistance Program Enrollment Form, available at radicava.com.
For your patients:
• Savings on their deductible, co-pay, and co-insurance costs for their medication and infusion costs for RADICAVA®†
• Automatic re-enrollment for the next calendar year, if eligible
For your office:
• Processes for submitting a request for co-pay assistance, by electronic or paper submission
• Support with information and answers to questions about the Program by calling 1-844-772-4548
* The Searchlight Support® Out-of-Pocket Assistance Program is for eligible patients who have commercial insurance that covers a portion of the medication and administration costs for RADICAVA®. Other restrictions apply. See full Eligibility Requirements & Terms and Conditions at radicavahcp.com.
† Persons residing in Massachusetts, Michigan, Minnesota, and Rhode Island are eligible for out-of-pocket assistance for the cost of the drug only and are not eligible for other types of cost support for administration of the medication.
Searchlight Support® Out-of-Pocket Assistance Program
Restrictions apply� $20,000 maximum program benefit per calendar year per eligibility criteria� See full Eligibility Requirements & Terms and Conditions for details�
PER INFUSION*ELIGIBLE PATIENTS PAY AS LITTLE AS $0$0
8
Please see Prescribing Information for RADICAVA® (edaravone), also available at radicavahcp.com.
How the Program works
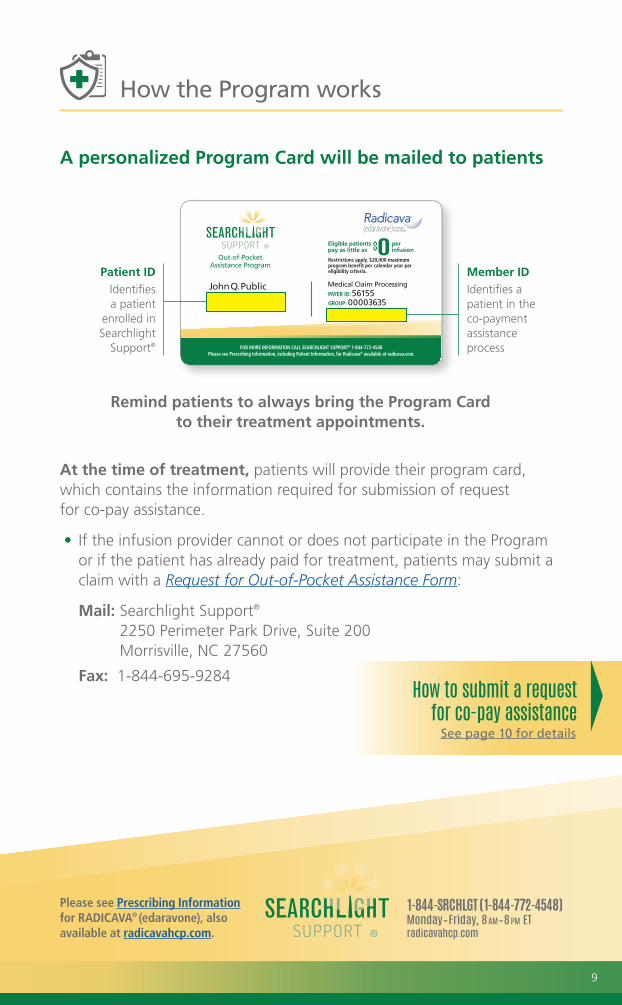
A personalized Program Card will be mailed to patients
Remind patients to always bring the Program Card to their treatment appointments.
At the time of treatment, patients will provide their program card, which contains the information required for submission of request for co-pay assistance.
• If the infusion provider cannot or does not participate in the Program or if the patient has already paid for treatment, patients may submit a claim with a Request for Out-of-Pocket Assistance Form:
Mail: Searchlight Support® 2250 Perimeter Park Drive, Suite 200 Morrisville, NC 27560
Fax: 1-844-695-9284
Patient IDIdentifies a patient
enrolled in Searchlight
Support®
Member IDIdentifies a patient in the co-payment assistance process
How to submit a request for co-pay assistance See page 10 for details
9
Please see Prescribing Information for RADICAVA® (edaravone), also available at radicavahcp.com.
How the Program works (continued)
How to submit a request for co-pay assistance
Send a claim for medication and infusion costs to the patient’s primary health plan. Then, complete a secondary claim request for co-pay assistance and submit it to the Program.
ELECTRONIC SUBMISSION
Submit a standard electronic claim to Interactive Medical Systems using Payer ID 56155, Group 00003635, and the patient’s Member ID as a secondary payer.
MAIL OR FAX SUBMISSION
Submit a medical claim form (CMS-1500 or UB-04) and a copy of the primary health plan Explanation of Benefits (EOB).
Fax: 1-919-562-0021
Mail: P.O. Box 1349, Wake Forest, NC 27588
For help processing a request for co-pay assistance, call 1-844-772-4548.
OUT-OF-POCKET ASSISTANCE PROGRAMHelping Provide Patients with Affordable Access to RADICAVA® (edaravone)
Please see accompanying Prescribing Information for RADICAVA®, also available at radicava.com.
Actor portrayals.
Claim requirements, and instructions for submitting a request for co-pay assistance under the patient’s pharmacy benefit, are available in the Out-of-Pocket Assistance Program Brochure for HCPs at radicavahcp.com, or ask your Mitsubishi Tanabe Pharma America (MTPA) representative.
10
Please see Prescribing Information for RADICAVA® (edaravone), also available at radicavahcp.com.
Other options for cost support
Support for patients who are eligible for government-funded insurance
We can provide information about government health plan options for RADICAVA® (edaravone), including:
• Veterans Administration l TRICARE l DoD
- RADICAVA® is on the VA National Formulary, subject to National Prior Authorization criteria
• Medicare l Social Security Disability Insurance l Medicaid
Resources for patients who are uninsured
We can also provide information about the Searchlight Support® Patient Assistance Program (PAP):
• The PAP can help patients in financial need who are uninsured
• Patients who meet program requirements may be able to receive RADICAVA® at no charge for up to two years*
Restrictions apply. See Eligibility Requirements & Terms and Conditions at radicavahcp.com.
* Only product provided at no charge. The Patient Assistance Program covers only the cost of RADICAVA® and not the cost of any infusion services or healthcare provider visits, which are the sole responsibility of the patient.
Call Searchlight Support® for more information or visit radicavahcp.com
Please see accompanying Prescribing Information, including Patient Information for RADICAVA®, also available at radicava.com.
UNDERSTANDING GOVERNMENT HEALTH PLAN OPTIONS
Know your options for 2019-2020
Actor portrayals.
Please see accompanying Prescribing Information, including Patient Information for RADICAVA®, also available at radicava.com.
PATIENT ASSISTANCE PROGRAM
If you are in financial need and have no insurance
Actor portrayals.
11
Please see Prescribing Information for RADICAVA® (edaravone), also available at radicavahcp.com.
Locating resources for the ALS community
ALS Care Locator—available at radicava.com/carelocator This search tool was designed for the ALS community to help locate ALS care providers, specifically healthcare providers (HCPs) who treat ALS and infusion centers.
How to enroll
You can enroll your practice or infusion service in the ALS Care Locator. Visit ALSCareDirectory.com for more information.* When you enroll, your site of care and profile information will be publicly available at radicava.com.
The ALS Care Locator is an informational resource only regarding available treatment providers. The providers listed in the directory are under no obligation to provide treatment.
The ALS Care Locator can help you:• Search for infusion providers capable of administering
RADICAVA® (edaravone), including home infusion, based on your patient’s preferences:- Type of Facility, Location, Insurance Accepted, including Medicare- Languages spoken, Hours of operation, Amenities
• Find neurologists and other HCPs who treat ALS
* The ALS Care Locator is a directory with a number of functions, including a directory of providers that treat ALS and which have opted-in to participate in the directory. This submission information is updated on a monthly basis.Providers listed in the directory are not affiliated with Mitsubishi Tanabe Pharma America, Inc. and do not pay to be on this list. No fees or remuneration of any kind have been or will be exchanged for participation in the ALS Care Locator. Inclusion of a provider in the ALS Care Locator does not constitute a referral, recommendation, endorsement, or verification of credentials, qualifications, or abilities of the provider listed. Similarly, the absence of a provider’s name and information should not be construed as a negative comment from Mitsubishi Tanabe Pharma America, Inc. about the provider’s credentials, qualifications, or abilities.Mitsubishi Tanabe Pharma America, Inc., as well as its employees or agents, shall not be held liable for any damages or harm resulting from any use or reliance on information contained in the ALS Care Locator; and may modify, amend, remove, or cancel the ALS Care Locator at any time without notice.
12
Please see full Indication and Important Safety Information on page 16, and Prescribing Information for RADICAVA® (edaravone), also available at radicavahcp.com.
Locating resources for the ALS community (continued)
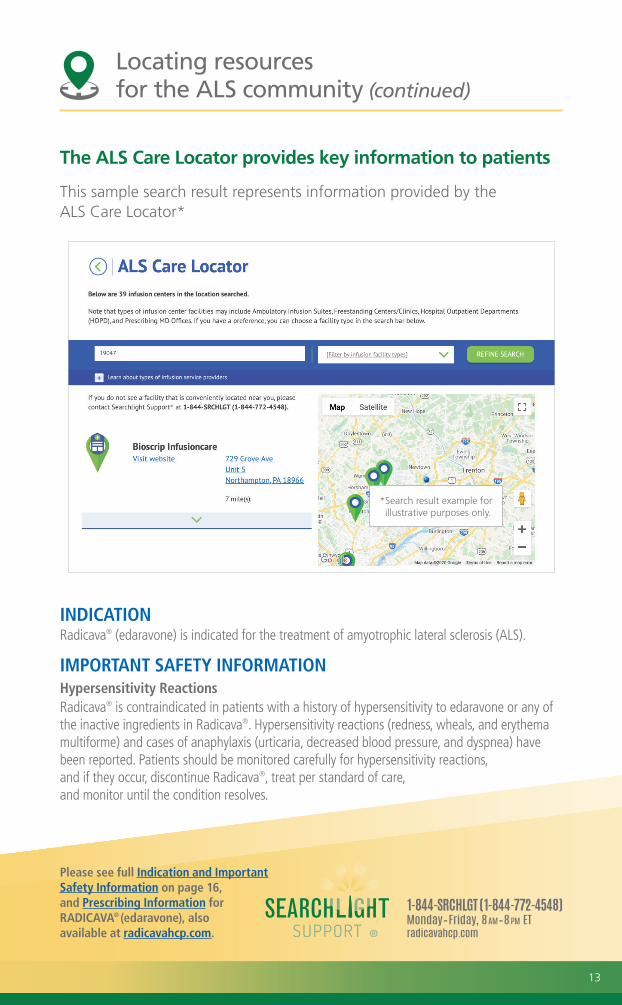
The ALS Care Locator provides key information to patients
This sample search result represents information provided by the ALS Care Locator*
INDICATIONRadicava® (edaravone) is indicated for the treatment of amyotrophic lateral sclerosis (ALS).
IMPORTANT SAFETY INFORMATIONHypersensitivity ReactionsRadicava® is contraindicated in patients with a history of hypersensitivity to edaravone or any of the inactive ingredients in Radicava®. Hypersensitivity reactions (redness, wheals, and erythema multiforme) and cases of anaphylaxis (urticaria, decreased blood pressure, and dyspnea) have been reported. Patients should be monitored carefully for hypersensitivity reactions, and if they occur, discontinue Radicava®, treat per standard of care, and monitor until the condition resolves.
* Search result example for illustrative purposes only.
13
Please see Prescribing Information for RADICAVA® (edaravone), also available at radicavahcp.com.
Helping your office and your patients navigate treatment challenges
Searchlight Support® offers a range of resources to assist you, your office staff, and your patients.
Limited Exceptions and Appeals Assistance*
If your patient is denied coverage, Searchlight Support® provides helpful information regarding the steps typically required to:
• Request coverage under a health plan’s exceptions process
• Use the appeals process if an exception request is denied
Coding and Billing Information
The Searchlight Support® Coding and Billing Guide provides general coding and billing information for RADICAVA® (edaravone)†
Ask your MTPA Manager of Patient Access representative for a copy of these resources.
* Searchlight Support® does not fill out any information that requires the medical judgment of the prescriber and only the prescriber can determine whether to pursue a Prior Authorization. Determination of Prior Authorization is at the sole discretion of the health plan. Searchlight Support® and Mitsubishi Tanabe Pharma America, Inc., do not assume responsibility for, nor do they guarantee the approval of a Prior Authorization request.
† Each healthcare provider is ultimately responsible for determining the appropriate codes, coverage, and payment for individual patients. Searchlight Support® does not guarantee third-party coverage or payment for RADICAVA® or reimburse for denied claims. Providers should contact their third-party payers for specific information on coding and billing requirements. You may also contact Searchlight Support® for coding and billing information for RADICAVA®. Call 1-844-SRCHLGT (1-844-772-4548), Monday–Friday, 8 AM–8 PM ET, or visit radicavahcp.com.
Appeals
What is an appeal?An appeal is a process used to challenge a plan’s coverage determination:
• Patients have the right to an appeal when an exception request has not been granted
Who can initiate an appeal?An appeal of a health plan’s coverage determination can be initiated by:
• The healthcare provider
• The patient
• An individual designated by the patient (such as a caregiver or relative)- The health plan may require a HIPAA waiver or authorization form signed by the patient- CMS requires a completed “Appointment of Representative” form (CMS Form 1696). Visit the Medicare section at cms.gov for additional information
The Appeals ProcessIn most cases, the appeal process is progressive, with sequential steps leading to higher levels of appeals. It is important to remember that all steps must be followed in order. Failure to complete the requirements at one level of the appeals process usually prevents patients from moving to the next level of appeal. The appeals process ends when the request has been granted or all levels of appeal have been exhausted.
Most health plans have similar rules regarding appeals:
1 Requests typically must be made in writing
2 Supporting statement from the prescribing healthcare provider must accompany the appeal
3 Expedited processes are available if there is a threat to the patient’s life or health
4 The steps of the appeals process must be followed in order
5 The timelines of each step must be met by all parties
Once the need for an appeal is identified, patients, their representative, or their healthcare provider should contact their health insurance company for specific information
on the exceptions and appeals process and requirements under their health plan.
Remember that Medicaid and commercial health plans may have a different process.
4
CONSIDERATIONS FOR THEEXCEPTIONS AND APPEALS PROCESS*
Please see accompanying Prescribing Information for RADICAVA®, also available at radicavahcp.com
Helpful information regarding the steps typically required in order to:• Request coverage under a health plan’s exception process• Use the appeals process if an exception request is denied
* Once the need for an exception is identified, patients, their representative, or their healthcare provider should contact their health insurance company for specific information on the exceptions and appeals process and requirements under their health plan.
Actor portrayal.
For your office
Requesting an Exception from Your Health PlanA General Overview
Have you been notified that your medication is not covered by your health plan or that you need to meet other requirements before obtaining it?
You can call your health plan and request an “exception” for coverage of your medication. Here are steps you may follow:
Prepare for the call
• Have your Group# and the BIN# on the front of your health insurance card ready. If there is no Group# on your card, you can use your Member ID#.
• Locate the Customer Service 800# on the back of your health insurance card.
Make the call
• Call the Customer Service 800# and ask to speak with the “Exceptions and Appeals Representative,” if there is one. Be sure to say that you are calling about your Medical Benefits.
• Ask the representative to give you information about your health plan’s “Exceptions and Appeals Process,” any required forms, and what you need to do to request an exception.
Work with your doctor’s office
• Obtain the information needed for submission of an exception request.
• Follow the health plan’s policy guidelines and observe their timeline.
Use the Checklist on Side 2 to help make sure you follow your health plan’s requirements for an exception request.
1
2
3
Know your numbers
Call this number
For illustration purposes only–your card may look different
Actor portrayal.
For your patients
Coding Information and Sample CMS-1500 and UB-04 Claim Forms for RADICAVA® (edaravone)
CODING AND BILLING GUIDE
Please see Indication and Important Safety Information on back cover and accompanying Prescribing Information for RADICAVA®, located in the pocket of this brochure, also available at radicava.com
Actor portrayal. 2020 EDITION
For your office
14
Please see Prescribing Information for RADICAVA® (edaravone), also available at radicavahcp.com.
Tools to help patients access treatment
Please use these forms, also available at radicavahcp.com:
Order Form for Buy & Bill
DOWNLOAD & PRINT
Benefit Investigation and Enrollment Form
COMPLETE, SIGN AND SUBMIT ONLINE
OR DOWNLOAD & PRINT
Sample Benefit Summary
ACCESS HERE & PRINT
Patient Authorization
Form
PATIENTS CAN COMPLETE, SIGN
AND SUBMIT ONLINE OR DOWNLOAD
Sample Letter of Medical Necessity
(for reference only)
DOWNLOAD & PRINT
Dedicated to helping provide access to RADICAVA® (edaravone) for people with ALS, and those who care for them.
15
INDICATION
Radicava® (edaravone) is indicated for the treatment of amyotrophic lateral sclerosis (ALS).
IMPORTANT SAFETY INFORMATIONHypersensitivity ReactionsRadicava® is contraindicated in patients with a history of hypersensitivity to edaravone or any of the inactive ingredients in Radicava®. Hypersensitivity reactions (redness, wheals, and erythema multiforme) and cases of anaphylaxis (urticaria, decreased blood pressure, and dyspnea) have been reported. Patients should be monitored carefully for hypersensitivity reactions, and if they occur, discontinue Radicava®, treat per standard of care, and monitor until the condition resolves.
Sulfite Allergic ReactionsRadicava® contains sodium bisulfite, and may cause allergic type reactions, including anaphylactic symptoms and life-threatening or less severe asthmatic episodes in susceptible people. The overall prevalence of sulfite sensitivity in the general population is unknown, but occurs more frequently in asthmatic people.
Most Common Adverse ReactionsMost common adverse reactions (at least 10% and greater than placebo) are contusion, gait disturbance, and headache.
PregnancyBased on animal data, Radicava® may cause fetal harm.
Geriatric UseNo overall differences in safety or effectiveness were observed between patients 65 years of age and older and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
To report suspected adverse reactions or product complaints, contact Mitsubishi Tanabe Pharma America, Inc. at 1-888-292-0058. You may also report suspected adverse reactions to the FDA at 1-800-FDA-1088, or www.fda.gov/medwatch.
RADICAVA, the RADICAVA logo, and the corporate symbol of Mitsubishi Tanabe Pharma America are registered trademarks of Mitsubishi Tanabe Pharma Corporation. Searchlight Support is a registered trademark of Mitsubishi Tanabe Pharma America, Inc.All other company names, product names, trade/service marks or other trade names are the property of their respective owners.For US audiences only.Mitsubishi Tanabe Pharma America, Inc.525 Washington Boulevard, Suite 400Jersey City, NJ 07310© 2020 Mitsubishi Tanabe Pharma America, Inc. All rights reserved. CP-RC-US-1258 08/20
Please see Prescribing Information for RADICAVA®, also available at radicavahcp.com.
RADICAVA® (edaravone) 30 mg/100 mL injection for infusion
ICD-10: G12.21 Amyotrophic lateral sclerosis
By signing this form, I certify and acknowledge that I have read, understand, and agree to the Healthcare Provider Disclaimer and the Healthcare Provider Attestation for Searchlight Support® Patient Assistance Program on page 2 of this form. I am also indicating a prescribing decision has been made. In addition, I am certifying treatment with RADICAVA® indicated above is medically necessary for this patient, and I have received authorization to release the medical and/or other patient information relating to this therapy to Mitsubishi Tanabe Pharma America, Inc., its affiliated companies, agents and representatives as specified in the Patient Authorization on page 3 of this form. I certify that, to the best of my knowledge, the patient and physician information in this form is complete, accurate, and consistent with applicable privacy regulations. If I am attaching a prescription, I certify that I have prescribed the product based on my professional judgment of medical necessity. I give Searchlight Support® permission to contact this patient to help obtain a signed Patient Authorization, if the patient has not provided their signature in Section 3 of this form.PHYSICIAN SIGNATURE REQUIRED TO PROCESS PATIENT ENROLLMENT: I have reviewed the current RADICAVA® Prescribing Information and I will be supervising the patient’s treatment. If I have attached a prescription, I authorize Searchlight Support® to act on my behalf to transmit the prescription to a contracted specialty pharmacy.
PHYSICIAN SIGNATURE DATE
By signing below, I certify and acknowledge that I have read, understand, and agree to the Patient Authorization on page 3 of this form, to participate in the Searchlight Support® Program and to release my Protected Health Information to Mitsubishi Tanabe Pharma America, Inc. (as defined on page 3 of this form), supporting the access program as indicated on the Patient Authorization.
PATIENT SIGNATURE DATE If patient cannot sign, patient’s Legal Representative must sign below.
PATIENT NAME (Please Print)
LEGAL REPRESENTATIVE BY (Please Print) (Signature of Legal Representative)By signing on this line, I certify under penalty of perjury that I am the legally authorized representative with authority to sign on behalf of the patient named herein.
NATURE OF RELATIONSHIP TO PATIENT DATE
WITNESS WITNESS SIGNATURE NOTARY (Optional) (Please Print) (Optional)
Benefit Investigation and Enrollment FormFax this completed form to 1-888-782-6157 or mail to Searchlight Support®, P.O. Box 2930, Phoenix, AZ 85062
For assistance or additional information, call 1-844-SRCHLGT (1-844-772-4548), Monday–Friday, 8:00am–8:00pm ET
Page 1 of 4
NAME (First, MI, Last, Suffix)
ADDRESS
CITY STATE ZIP
EMAIL DOB (MM/DD/YYYY)
HOME PHONE CELL PHONE
PREFERRED NUMBER TO CALL Home Phone Cell Phone
1. PATIENT INFORMATION (REQUIRED)
Please see accompanying Prescribing Information, including Patient Information for RADICAVA®, also available at radicava.com. CP-RC-US-1335 07/20
PLEASE COMPLETE ALL THAT APPLY AND INCLUDE A FRONT AND BACK COPY OF INSURANCE CARD FOR EACH TYPE OF INSURANCE.
VETERANS AFFAIRS (VA) COVERAGE/BENEFITS Yes No VETERANS WHO ARE NOT TRICARE BENEFICIARIES & DO NOT HAVE SECONDARY INSURANCE, PROCEED TO SECTION 3. Veterans and patients enrolled in government health insurance (i.e., Medicare, Medicaid, VA, DoD, or other federal or state assistance programs) do not qualify for the Searchlight Support® Out-of-Pocket Assistance Program.
Please investigate benefits for: SPECIALTY DISTRIBUTOR–BUY & BILL SPECIALTY PHARMACY–PRESCRIPTIONHOME INFUSION If applicable, please attach prescription.
Patients with no insurance will be contacted by Searchlight Support® for consideration in the Patient Assistance Program.
PRIMARY INSURANCE GROUP/PLAN NAME
CARDHOLDER NAME
RELATIONSHIP TO CARDHOLDER EMPLOYER
INS. CO. PHONE POLICY # GROUP #
SECONDARY INSURANCE GROUP/PLAN NAME
CARDHOLDER NAME
RELATIONSHIP TO CARDHOLDER EMPLOYER
INS. CO. PHONE POLICY # GROUP #
MEDICARE PART D Yes No SUPPLEMENTAL INSURANCE Yes No
Is patient a dependent of the insured (child <18 yrs; student >18 yrs)? Check if yes.
2. INSURANCE INFORMATION (REQUIRED. Include alpha prefix and suffix with policy and group# when applicable)
5. PHYSICIAN SIGNATURE (REQUIRED) SPECIAL NOTE: If attaching a prescription, physician must comply with state-specific prescription requirements, such as e-prescribing, state-specific prescription form, fax language, etc. Non-compliance with state-specific requirements could result in follow-up and delayed processing.
PRESCRIBER CONTACT NAME (First, Last)
PRACTICE NAME
ADDRESS
CITY STATE ZIP
EMAIL PHONE FAX
MEDICAID/MEDICARE PROVIDER # (Optional) TAX ID #
STATE LICENSE # (Optional) UPIN/NPI #
PREFERRED OFFICE CONTACT (IF DIFFERENT THAN ABOVE)
PHONE FAX
4. PRESCRIBER OFFICE INFORMATION (REQUIRED)
3. PATIENT AUTHORIZATION (Patient must read the Patient Authorization on the Patient Copy and sign below.)
Please provide Infusion Site Location Assistance if Primary and/or Secondary location is unknown
Is this a VA site: Yes No Site Name:
If Primary Site of infusion is known, provide information below:
FACILITY NAME CONTACT
FACILITY PHONE FACILITY FAX
If Secondary Site of infusion is known, provide information below:
FACILITY NAME CONTACT
FACILITY PHONE FACILITY FAX
6. PREFERRED SITE OF INFUSION (OPTIONAL) (Do not complete fields below if information is the same as Prescriber Information)
Page 2 of 4
Healthcare Provider Disclaimer
By providing your information and information about your patient on the front of this Benefit Investigation and Enrollment Form, you are requesting to participate in Searchlight Support® and its programs. The information you provide will only be used by Mitsubishi Tanabe Pharma America, Inc. (“Mitsubishi Tanabe Pharma America”), our affiliates, and our service providers involved in managing and delivering these services and programs. You may withdraw your request for these services at any time by calling 1-844-772-4548. You agree to be contacted by Mitsubishi Tanabe Pharma America at Searchlight Support® by mail, fax, email or telephone for the purposes of managing and delivering these services and programs. Our Privacy Policy, available at mt-pharma-america.com/privacy-policy, governs the use of the information you provide. By providing the information on this form and submitting this form, you indicate that you have read, understand, and agree to these terms and agree to receive program-related communications from Searchlight Support® and its service providers, including RxC Acquisition Company d.b.a. RxCrossroads by McKesson and TrialCard, Inc. (TrialCard). Please contact Searchlight Support® at 1-844-772-4548 if you wish to change your communication preferences.
Patient insurance benefit investigation is provided as a service by RxCrossroads by McKesson under contract for Mitsubishi Tanabe Pharma America. RxCrossroads by McKesson provides assistance in determining whether treatment can be covered by the payer based on the payer’s health plan guidelines and the patient information you provided as authorized by the patient on the Benefit Investigation and Enrollment Form, following your determination of medical necessity. Patient out-of-pocket cost support through the Searchlight Support® Out-of-Pocket Assistance Program is provided to eligible patients as a service by TrialCard under contract for Mitsubishi Tanabe Pharma America.
Verification of insurance coverage is ultimately the responsibility of the provider. Since reimbursement by payers is subject to many factors, RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America do not represent or guarantee that payer reimbursement or any other payment or reimbursement of any kind will be made. RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America do not reimburse for claims denied by payers. Information provided as a result of the benefit investigation is provided for general reference and informational purposes only. RxCrossroads by McKesson makes every effort to be accurate in the information provided; however, no representations or warranties are expressed or implied by RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America regarding the accuracy or reliability of the information. RxCrossroads by McKesson or Mitsubishi Tanabe Pharma America, or its agents or employees shall not be liable legally, financially, or otherwise, for damages of any kind as a result of or related to these services. Providers and other users of this information resulting from benefit investigation services accept full responsibility for use of the service.
Mitsubishi Tanabe Pharma America does not assume responsibility for, nor does it guarantee the availability, scope, or quality of the services offered including reimbursement support, prescription fulfillment coordination, and other services under Searchlight Support®. Providers, not Mitsubishi Tanabe Pharma America, are responsible for the services they provide. The Searchlight Support® services have no value apart from the product.
Healthcare Provider Attestation for Searchlight Support® Patient Assistance Program
If the patient identified on page 1 of this form is determined to be eligible to participate in the Searchlight Support® Patient Assistance Program (the “Program”), I confirm that to the best of my knowledge, the patient does not have health insurance of any type, for example, but not limited to, an HMO, Private Insurance, State Pharmacy Program, Medicare, Medicaid, or Veterans Assistance. By signing page 1 of this form, I attest that I do not and will not bill, charge, seek credit for or otherwise submit any claim for reimbursement to any third-party payer or the patient for the Product the patient receives at no charge through the Program. I understand that the Program does not include the cost of any associated services such as administration of product or healthcare provider visits. I also understand it is my responsibility to promptly inform the Program of any information that changes from what is being submitted on page 1 of this Searchlight Support® Benefit Investigation and Enrollment Form for RADICAVA® (edaravone).
Please see accompanying Prescribing Information, including Patient Information for RADICAVA®, also available at radicava.com.
Patient Copy
Provider Instructions1. Instruct the patient to read this page and sign the Authorization in Section 3 on page 1 of the Benefit Investigation and Enrollment Form for RADICAVA® (edaravone).2. Give the patient this page, a copy of page 1 of the Searchlight Support® Benefit Investigation and Enrollment Form, and a copy of the Patient Acknowledgement.
PATIENT AUTHORIZATIONMy signature on page 1 of the Benefit Investigation and Enrollment Form (the “Form”) for RADICAVA® serves as confirmation that I authorize each of my physicians and pharmacists, including any specialty pharmacy and/or home infusion provider which receives my prescription for RADICAVA® and other healthcare providers (together, “Healthcare Providers”) and each of my health insurers (together, “Insurers”) to use and disclose my Protected Health Information, including, but not limited to, medical records and history, information related to my medical condition and treatment, my health insurance coverage, my name, address, telephone number, Social Security number, insurance plan and/or group numbers (together, “Protected Health Information”) to Mitsubishi Tanabe Pharma America, Inc., its affiliated companies, agents and representatives (together, “Mitsubishi Tanabe Pharma America”), including providers of alternate sources of funding for prescription drug costs, and other service providers supporting access and assistance programs for Healthcare Providers and patients (Searchlight Support®) for the purposes described below.I specifically authorize Mitsubishi Tanabe Pharma America to receive, use, and disclose my Protected Health Information for the following purposes: (i) to enroll me in, and contact me and/or the person legally authorized to sign on my behalf, about Searchlight Support® programs, including potential enrollment in the Searchlight Support® Out-of-Pocket Assistance Program if I am an eligible, commercially insured patient with insurance coverage for RADICAVA®, or Searchlight Support® Patient Assistance Program, if I have no insurance and meet eligibility requirements; (ii) to provide me and/or the person legally authorized to sign on my behalf with educational materials, information, and services related to RADICAVA®; (iii) to verify, investigate, assist with, and coordinate my coverage for RADICAVA® with my Insurers; (iv) to coordinate prescription fulfillment, including triaging my information and my prescription to a specialty pharmacy and/or home infusion provider; (v) to assist with analyses related to the quality, efficacy, and safety of RADICAVA®, and patient access to and treatment compliance with RADICAVA®; (vi) to send me marketing information related to my condition, my treatment, or related products or services that might be of interest to me; (vii) to contact me occasionally to obtain my feedback for market research purposes about my treatment, my condition, or my experience with RADICAVA®, Mitsubishi Tanabe Pharma America and/or Searchlight Support®; and (viii) to contact me about other products and services offered by Mitsubishi Tanabe Pharma America. Mitsubishi Tanabe Pharma America may use my Protected Health Information to contact me for any purpose described in this Authorization by mail, email, phone calls, voice messages, interactive voice recordings that may include use of autodialers or artificial or prerecorded voice messages, and SMS text messages (data rates may apply). Marketing communications will include information about how I can opt-out of receiving future communications. I understand that my participation in the Searchlight Support® Program will not be affected if I opt-out.I understand that pharmacies that ship my medication may be paid to share this information with Searchlight Support® in order to help provide the offerings requested for me. I also understand that my Protected Health Information will not be used or disclosed by Mitsubishi Tanabe Pharma America for any other purpose than described in this Form without my authorization unless permitted by law or unless information that specifically identifies me is removed so that the information is “de-identified.” I understand that Mitsubishi Tanabe Pharma America will make every effort to keep my information private. I understand that information used or disclosed under this Authorization may be re-disclosed by the recipient and may no longer be protected by federal or state law. For additional information on how Mitsubishi Tanabe Pharma America collects, uses, and discloses personal information, I can visit mt-pharma-america.com/privacy-policy.I understand that I am not required to sign the front of the Benefit Investigation and Enrollment Form for RADICAVA®. My decision whether to sign will not change the way my Healthcare Providers or Insurers treat me. If I do not sign the Authorization in Section 3 on page 1 of this Form, or cancel (revoke) my Authorization later, I understand that this means I will not be able to participate or receive assistance from Searchlight Support®.This Authorization will remain in effect for 5 years from the date of my signature, or until I am no longer participating in Searchlight Support® services, whichever is sooner. A copy of this Authorization will be as valid as the original. I may cancel this Authorization at any time in writing by mailing a letter to Searchlight Support®, P.O. Box 2930, Phoenix, AZ 85062. I can also cancel my Authorization by informing my Healthcare Providers and Insurers in writing that I do not want them to share any information with Mitsubishi Tanabe Pharma America. Cancelling this authorization will not affect the ability of Mitsubishi Tanabe Pharma America to use and disclose Protected Health Information that it has received prior to receipt of the cancellation of my Authorization. My Authorization will also end if Searchlight Support® is discontinued. Furthermore, I understand that I have the right to see or copy the Protected Health Information my Healthcare Providers or Insurers have given to Mitsubishi Tanabe Pharma America.
Page 3 of 4
Please see accompanying Prescribing Information, including Patient Information for RADICAVA®, also available at radicava.com.
PATIENT ACKNOWLEDGMENT
My signature on page 1 of the Benefit Investigation and Enrollment Form (the “Form”) for RADICAVA® (edaravone) serves as confirmation of the following:
• If I am eligible to participate in the Searchlight Support® Patient Assistance Program (the “Program”), I agree to notify Searchlight Support® if my insurance situation changes, and I understand that upon obtaining health insurance, I will no longer be eligible to participate in the Program and that Searchlight Support® Patient Assistance Program medication will no longer be dispensed to me.
• My eligibility to receive assistance in the Program will be reviewed every 12 months and may change if I no longer meet the current program eligibility requirements. For program eligibility requirements, terms and conditions, I can refer to the Searchlight Support® Patient Assistance Program brochure.
• Additionally, I acknowledge and agree that I will not seek credit for or otherwise submit any claim for reimbursement to any third-party payer for the RADICAVA® medication provided at no charge by the Program and that I will not seek to have free medication or any associated costs counted towards my Medicare Part D True out-of-pocket (TrOOP) costs for prescription drugs.
• I understand and agree that the Program covers only the cost of RADICAVA® and not the cost of any infusion services or Healthcare Provider visits, which are my sole responsibility.
• I understand that Searchlight Support® has the right to verify my eligibility, including the right to audit any information provided on page 1 and to contact me to confirm receipt of medications.
• I also understand that the Program may be revised, changed or terminated at any time without notice.
Page 4 of 4
RADICAVA, the RADICAVA logo, and the corporate symbol of Mitsubishi Tanabe Pharma America are registered trademarks of Mitsubishi Tanabe Pharma Corporation. Searchlight Support is a registered trademark of Mitsubishi Tanabe Pharma America, Inc.For US audiences only.Mitsubishi Tanabe Pharma America, Inc.525 Washington Boulevard, Suite 400Jersey City, NJ 07310© 2020 Mitsubishi Tanabe Pharma America, Inc. All rights reserved. CP-RC-US-1335 07/20
Please see accompanying Prescribing Information, including Patient Information for RADICAVA®, also available at radicava.com.

Please see accompanying Prescribing Information, including Patient Information, for Radicava®, also available at radicava.com.
Patient Authorization Form for RADICAVA® (edaravone)
Instructions:
•• If patient has not already signed a Searchlight Support® Benefit Investigation and Enrollment Form for RADICAVA® (edaravone), patient must read this Patient Authorization and sign on the next page to authorize Searchlight Support® services.
•• Patient should retain a copy of this form for their records.
My signature on this Patient Authorization Form (the “Form”) for RADICAVA® serves as confirmation that I authorize each of my physicians and pharmacists, including any specialty pharmacy and/or home infusion provider which receives my prescription for RADICAVA® and other healthcare providers (together, “Healthcare Providers”) and each of my health insurers (together, “Insurers”) to use and disclose my Protected Health Information, including, but not limited to, medical records and history, information related to my medical condition and treatment, my health insurance coverage, my name, address, telephone number, Social Security number, insurance plan and/or group numbers (together, “Protected Health Information”) to Mitsubishi Tanabe Pharma America, Inc., its affiliated companies, agents and representatives (together, “Mitsubishi Tanabe Pharma America”), including providers of alternate sources of funding for prescription drug costs, and other service providers supporting access and assistance programs for Healthcare Providers and patients (Searchlight Support®) for the purposes described below.
I specifically authorize Mitsubishi Tanabe Pharma America to receive, use, and disclose my Protected Health Information for the following purposes: (i) to enroll me in, and contact me and/or the person legally authorized to sign on my behalf, about Searchlight Support® programs, including potential enrollment in the Searchlight Support® Out-of-Pocket Assistance Program if I am an eligible, commercially insured patient with insurance coverage for RADICAVA®, or Searchlight Support® Patient Assistance Program, if I have no insurance and meet eligibility requirements; (ii) to provide me and/or the person legally authorized to sign on my behalf with educational materials, information, and services related to RADICAVA®; (iii) to verify, investigate, assist with, and coordinate my coverage for RADICAVA® with my Insurers; (iv) to coordinate prescription fulfillment, including triaging my information and my prescription to a specialty pharmacy and/or home infusion provider; (v) to assist with analyses related to the quality, efficacy, and safety of RADICAVA®, and patient access to and treatment compliance with RADICAVA®; (vi) to send me marketing information related to my condition, my treatment, or related products or services that might be of interest to me; (vii) to contact me occasionally to obtain my feedback for market research purposes about my treatment, my condition, or my experience with RADICAVA®, Mitsubishi Tanabe Pharma America and/or Searchlight Support®; and (viii) to contact me about other products and services offered by Mitsubishi Tanabe Pharma America. Mitsubishi Tanabe Pharma America may use my Protected Health Information to contact me for any purpose described in this Authorization by mail, email, phone calls, voice messages, interactive voice recordings that may include use of autodialers or artificial or prerecorded voice messages, and SMS text messages (data rates may apply). Marketing communications will include information about how I can opt-out of receiving future communications. I understand that my participation in the Searchlight Support® Program will not be affected if I opt-out.
I understand that pharmacies that ship my medication may be paid to share this information with Searchlight Support® in order to help provide the offerings requested for me. I also understand that my Protected Health Information will not be used or disclosed by Mitsubishi Tanabe Pharma America for any other purpose than described in this Form without my authorization unless permitted by law or unless information that specifically identifies me is removed so that the information is “de-identified.” I understand that Mitsubishi Tanabe Pharma America will make every effort to keep my information private. I understand that information used or disclosed under this Authorization may be re-disclosed by the recipient and may no longer be protected by federal or state law. For additional information on how Mitsubishi Tanabe Pharma America collects, uses, and discloses personal information, I can visit mt-pharma-america.com/privacy-policy.
I understand that I am not required to sign this Patient Authorization Form for RADICAVA®. My decision whether to sign will not change the way my Healthcare Providers or Insurers treat me. If I do not sign below, or cancel (revoke) my Authorization later, I understand that this means I will not be able to participate or receive assistance from Searchlight Support®.
RADICAVA, the RADICAVA logo, and the corporate symbol of Mitsubishi Tanabe Pharma America are registered trademarks of Mitsubishi Tanabe Pharma Corporation. Searchlight Support is a registered trademark of Mitsubishi Tanabe Pharma America, Inc. For US audiences only.Mitsubishi Tanabe Pharma America, Inc.525 Washington Boulevard, Suite 400Jersey City, NJ 07310© 2020 Mitsubishi Tanabe Pharma America, Inc. All rights reserved. CP-RC-US-1342 04/20
Please see accompanying Prescribing Information, including Patient Information, for Radicava®, also available at radicava.com.
Patient Authorization Form for RADICAVA® (edaravone) (continued)
This Authorization will remain in effect for 5 years from the date of my signature, or until I am no longer participating in Searchlight Support® services, whichever is sooner. A copy of this Authorization will be as valid as the original. I may cancel this Authorization at any time in writing by mailing a letter to Searchlight Support®, P.O. Box 2930, Phoenix, AZ 85062. I can also cancel my Authorization by informing my Healthcare Providers and Insurers in writing that I do not want them to share any information with Mitsubishi Tanabe Pharma America. Cancelling this authorization will not affect the ability of Mitsubishi Tanabe Pharma America to use and disclose Protected Health Information that it has received prior to receipt of the cancellation of my Authorization. My Authorization will also end if Searchlight Support® is discontinued. Furthermore, I understand that I have the right to see or copy the Protected Health Information my Healthcare Providers or Insurers have given to Mitsubishi Tanabe Pharma America.
Patient Name: Date of Birth (mm/dd/yyyy):
Patient Address:
City: State: ZIP Code:
I have read this Form and understand that signing this Authorization is voluntary. By signing below, I acknowledge that I have read, understood and accept all of the above.
Patient Signature: Date:
PATIENT ACKNOWLEDGMENTMy signature above on this Patient Authorization Form (the “Form”) for RADICAVA® serves as confirmation of the following:
•• If I am eligible to participate in the Searchlight Support® Patient Assistance Program (the “Program”), I agree to notify Searchlight Support® if my insurance situation changes, and I understand that upon obtaining health insurance, I will no longer be eligible to participate in the Program and that Searchlight Support® Patient Assistance Program medication will no longer be dispensed to me.
•• My eligibility to receive assistance in the Program will be reviewed every 12 months and may change if I no longer meet the current program eligibility requirements. For program eligibility requirements, terms and conditions, I can refer to the Searchlight Support® Patient Assistance Program brochure.
•• Additionally, I acknowledge and agree that I will not seek credit for or otherwise submit any claim for reimbursement to any third-party payer for the RADICAVA® medication provided at no charge by the Program and that I will not seek to have free medication or any associated costs counted towards my Medicare Part D True out-of-pocket (TrOOP) costs for prescription drugs.
•• I understand and agree that the Program covers only the cost of RADICAVA® and not the cost of any infusion services or Healthcare Provider visits, which are my sole responsibility.
•• I understand that Searchlight Support® has the right to verify my eligibility, including the right to audit any information I provide, and to contact me to confirm receipt of medications.
•• I also understand that the Program may be revised, changed or terminated at any time without notice.
If patient cannot sign, patient’s Legal Representative must sign below:
Legal Representative: By: (Please Print) (Signature of Legal Representative)
By signing on this line, I certify under penalty of perjury that I am the legally authorized representative with authority to sign on behalf of the patient named herein.
Nature of Relationship to Patient: Date:
Witness: Witness Signature: Notary (Optional) (Please Print) (Optional)
Fax completed form to 888-782-6157 or mail to Searchlight Support®, P.O. Box 2930, Phoenix, AZ 85062
1
Sample Letter of Medical Necessity for RADICAVA® (edaravone)
This letter provides an example of the types of information that may be included when responding to a
request from a patient's insurance company to provide a Letter of Medical Necessity for RADICAVA®. Use
of the information in this letter does not guarantee that the health plan will provide reimbursement for
RADICAVA®, and it is not intended to be a substitute for, or to influence, the independent medical
judgment of the physician.
Helpful tips
• You may consider including a letter of medical necessity (like the example on page 2 of this document) with your prior authorization (PA) request to emphasize the medical necessity for RADICAVA® or in addition to your appeal letter, as needed
• Letters of medical necessity should be signed by the physician only
• Be sure to include an appropriate International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) that matches your patient’s diagnosis
• When you download this document, make certain to delete pages 1 and 3 of this document Example Checklist Summary
Example chart notes − Date of initial diagnosis
− ALSFRS-R score − FVC score − Brief description of the patients’ recent symptoms and conditions, including current motor function − Previous therapies the patient has undergone for the symptoms associated with
their condition, and patient’s response to these therapies A PDF of the Prescribing Information for RADICAVA®
INDICATION
Radicava® (edaravone) is indicated for the treatment of amyotrophic lateral sclerosis (ALS). IMPORTANT SAFETY INFORMATION Hypersensitivity Reactions Radicava® is contraindicated in patients with a history of hypersensitivity to edaravone or any of the inactive ingredients in Radicava®. Hypersensitivity reactions (redness, wheals, and erythema multiforme) and cases of anaphylaxis (urticaria, decreased blood pressure, and dyspnea) have been reported. Patients should be monitored carefully for hypersensitivity reactions, and if they occur, discontinue Radicava®, treat per standard of care, and monitor until the condition resolves. Please see Indication and full Important Safety Information on last page and Prescribing Information for RADICAVA®, also available at radicava.com.
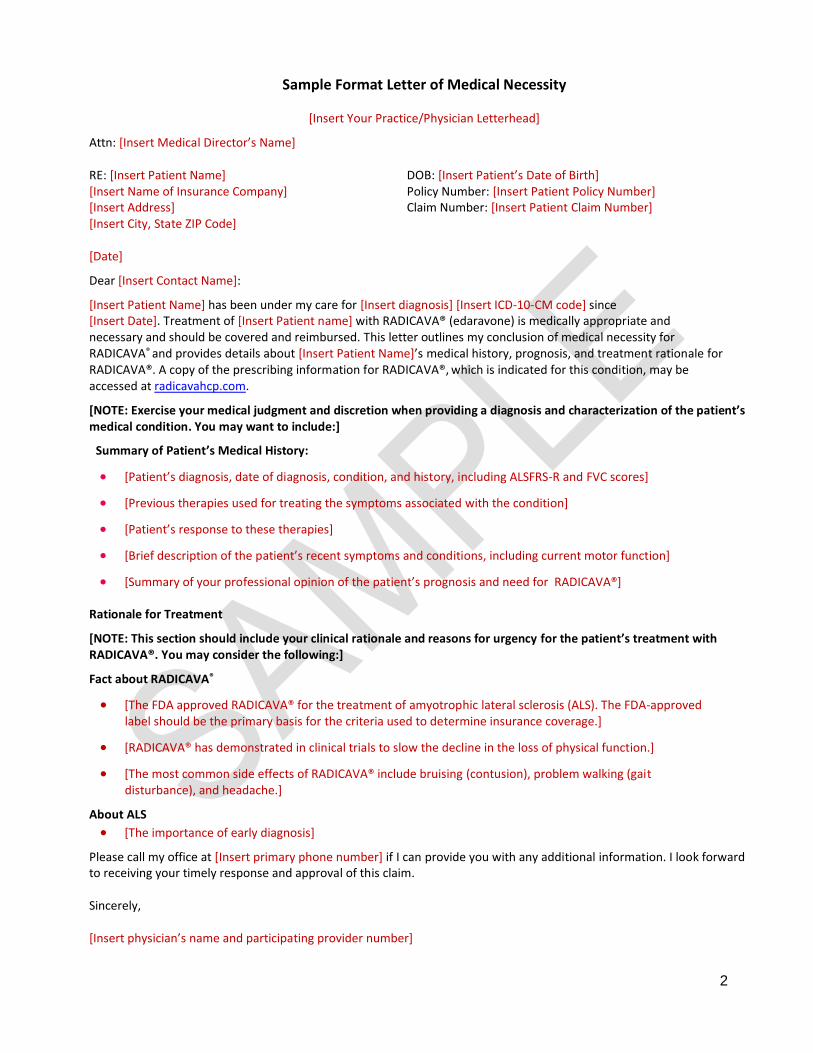
2
Sample Format Letter of Medical Necessity
[Insert Your Practice/Physician Letterhead]
Attn: [Insert Medical Director’s Name] RE: [Insert Patient Name] DOB: [Insert Patient’s Date of Birth] [Insert Name of Insurance Company] Policy Number: [Insert Patient Policy Number] [Insert Address] Claim Number: [Insert Patient Claim Number] [Insert City, State ZIP Code] [Date]
Dear [Insert Contact Name]:
[Insert Patient Name] has been under my care for [Insert diagnosis] [Insert ICD-10-CM code] since [Insert Date]. Treatment of [Insert Patient name] with RADICAVA® (edaravone) is medically appropriate and necessary and should be covered and reimbursed. This letter outlines my conclusion of medical necessity for RADICAVA® and provides details about [Insert Patient Name]’s medical history, prognosis, and treatment rationale for RADICAVA®. A copy of the prescribing information for RADICAVA®, which is indicated for this condition, may be accessed at radicavahcp.com.
[NOTE: Exercise your medical judgment and discretion when providing a diagnosis and characterization of the patient’s medical condition. You may want to include:]
Summary of Patient’s Medical History:
• [Patient’s diagnosis, date of diagnosis, condition, and history, including ALSFRS-R and FVC scores]
• [Previous therapies used for treating the symptoms associated with the condition]
• [Patient’s response to these therapies]
• [Brief description of the patient’s recent symptoms and conditions, including current motor function]
• [Summary of your professional opinion of the patient’s prognosis and need for RADICAVA®]
Rationale for Treatment
[NOTE: This section should include your clinical rationale and reasons for urgency for the patient’s treatment with RADICAVA®. You may consider the following:]
Fact about RADICAVA®
• [The FDA approved RADICAVA® for the treatment of amyotrophic lateral sclerosis (ALS). The FDA-approved label should be the primary basis for the criteria used to determine insurance coverage.]
• [RADICAVA® has demonstrated in clinical trials to slow the decline in the loss of physical function.]
• [The most common side effects of RADICAVA® include bruising (contusion), problem walking (gait disturbance), and headache.]
About ALS
• [The importance of early diagnosis]
Please call my office at [Insert primary phone number] if I can provide you with any additional information. I look forward to receiving your timely response and approval of this claim. Sincerely, [Insert physician’s name and participating provider number]
3
RADICAVA® (edaravone) INDICATION AND IMPORTANT SAFETY INFORMATION INDICATION
Radicava® (edaravone) is indicated for the treatment of amyotrophic lateral sclerosis (ALS). IMPORTANT SAFETY INFORMATION
Hypersensitivity Reactions Radicava® is contraindicated in patients with a history of hypersensitivity to edaravone or any of the inactive ingredients in Radicava®. Hypersensitivity reactions (redness, wheals, and erythema multiforme) and cases of anaphylaxis (urticaria, decreased blood pressure, and dyspnea) have been reported. Patients should be monitored carefully for hypersensitivity reactions, and if they occur, discontinue Radicava®, treat per standard of care, and monitor until the condition resolves. Sulfite Allergic Reactions Radicava® contains sodium bisulfite, and may cause allergic type reactions, including anaphylactic symptoms and life-threatening or less severe asthmatic episodes in susceptible people. The overall prevalence of sulfite sensitivity in the general population is unknown, but occurs more frequently in asthmatic people. Most Common Adverse Reactions Most common adverse reactions (at least 10% and greater than placebo) are contusion, gait disturbance, and headache. Pregnancy Based on animal data, Radicava® may cause fetal harm. Geriatric Use No overall differences in safety or effectiveness were observed between patients 65 years of age and older and younger patients, but greater sensitivity of some older individuals cannot be ruled out. To report suspected adverse reactions or product complaints, contact Mitsubishi Tanabe Pharma America, Inc. at 1-888-292-0058. You may also report suspected adverse reactions to the FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. Please see Prescribing Information for RADICAVA®, also available at radicava.com. RADICAVA is a registered trademark of Mitsubishi Tanabe Pharma Corporation. For US audiences only. Mitsubishi Tanabe Pharma America, Inc. 525 Washington Boulevard, Suite 400 Jersey City, NJ 07310
© 2020 Mitsubishi Tanabe Pharma America, Inc. All rights reserved. CP-RC-US-1135 04/20
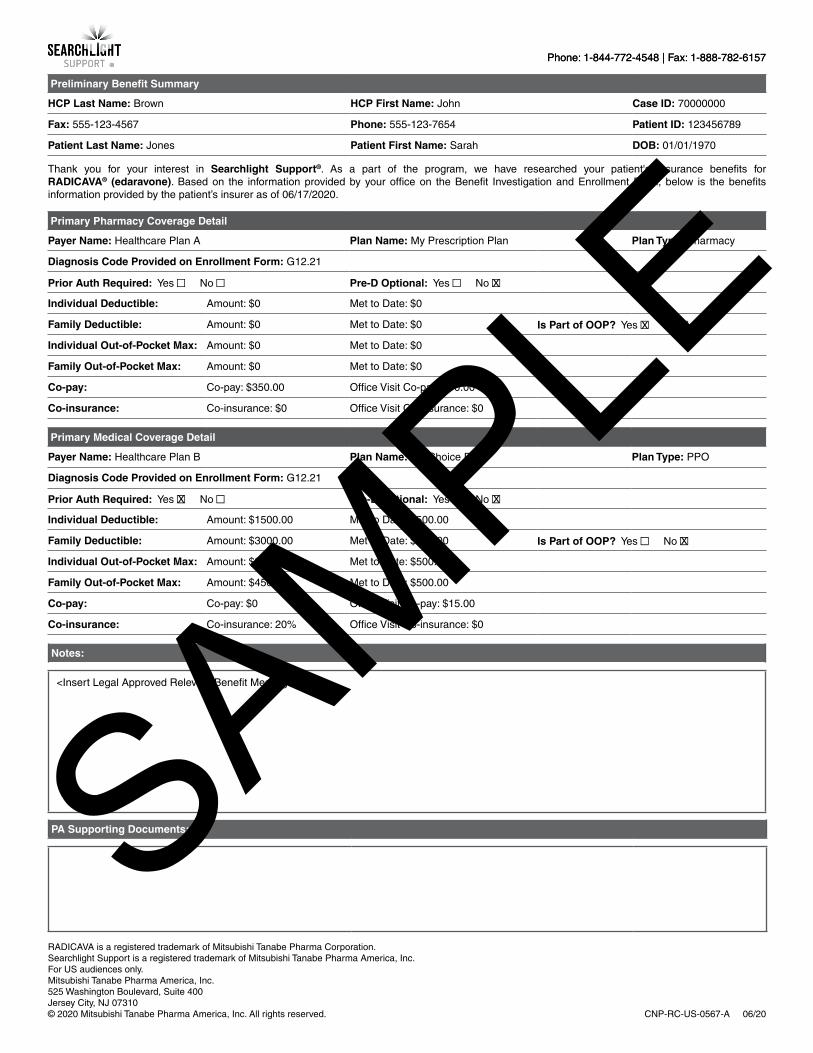
Phone: 1-844-772-4548 | Fax: 1-888-782-6157Phone: 1-844-772-4548 | Fax: 1-888-782-6157
Preliminary Benefit Summary
HCP Last Name: Brown HCP First Name: John Case ID: 70000000
Fax: 555-123-4567 Phone: 555-123-7654 Patient ID: 123456789
Patient Last Name: Jones Patient First Name: Sarah DOB: 01/01/1970
Thank you for your interest in Searchlight Support®. As a part of the program, we have researched your patient's insurance benefits for RADICAVA® (edaravone). Based on the information provided by your office on the Benefit Investigation and Enrollment Form, below is the benefits information provided by the patient’s insurer as of 06/17/2020.
Primary Pharmacy Coverage Detail
Payer Name: Healthcare Plan A Plan Name: My Prescription Plan Plan Type: Pharmacy
Diagnosis Code Provided on Enrollment Form: G12.21
Prior Auth Required: Yes ■ No ■ Pre-D Optional: Yes ■ No ■
Individual Deductible: Amount: $0 Met to Date: $0
Family Deductible: Amount: $0 Met to Date: $0 Is Part of OOP? Yes ■ No ■
Individual Out-of-Pocket Max: Amount: $0 Met to Date: $0
Family Out-of-Pocket Max: Amount: $0 Met to Date: $0
Co-pay: Co-pay: $350.00 Office Visit Co-pay: $10.00
Co-insurance: Co-insurance: $0 Office Visit Co-insurance: $0
Primary Medical Coverage Detail
Payer Name: Healthcare Plan B Plan Name: My Choice Plan Plan Type: PPO
Diagnosis Code Provided on Enrollment Form: G12.21
Prior Auth Required: Yes ■ No ■ Pre-D Optional: Yes ■ No ■
Individual Deductible: Amount: $1500.00 Met to Date: $500.00
Family Deductible: Amount: $3000.00 Met to Date: $500.00 Is Part of OOP? Yes ■ No ■
Individual Out-of-Pocket Max: Amount: $3500.00 Met to Date: $500.00
Family Out-of-Pocket Max: Amount: $4500.00 Met to Date: $500.00
Co-pay: Co-pay: $0 Office Visit Co-pay: $15.00
Co-insurance: Co-insurance: 20% Office Visit Co-insurance: $0
PA Supporting Documents:
Notes:
<Insert Legal Approved Relevant Benefit Messages>
RADICAVA is a registered trademark of Mitsubishi Tanabe Pharma Corporation. Searchlight Support is a registered trademark of Mitsubishi Tanabe Pharma America, Inc. For US audiences only. Mitsubishi Tanabe Pharma America, Inc. 525 Washington Boulevard, Suite 400 Jersey City, NJ 07310 © 2020 Mitsubishi Tanabe Pharma America, Inc. All rights reserved. CNP-RC-US-0567-A 06/20
X
X X
X
X
SAMPLE
Phone: 1-844-772-4548 | Fax: 1-888-782-6157Phone: 1-844-772-4548 | Fax: 1-888-782-6157
RADICAVA is a registered trademark of Mitsubishi Tanabe Pharma Corporation. Searchlight Support is a registered trademark of Mitsubishi Tanabe Pharma America, Inc. For US audiences only. Mitsubishi Tanabe Pharma America, Inc. 525 Washington Boulevard, Suite 400 Jersey City, NJ 07310 © 2020 Mitsubishi Tanabe Pharma America, Inc. All rights reserved. CNP-RC-US-0567-A 06/20
Patient insurance benefit investigation is provided as a service by RxC Acquisition Company d.b.a. RxCrossroads by McKesson under contract for Mitsubishi Tanabe Pharma America, Inc. (“Mitsubishi Tanabe Pharma America”). RxCrossroads by McKesson provides assistance in determining whether treatment can be covered by the payer based on the payer’s health plan guidelines and the patient information you provided as authorized by the patient on the Benefit Investigation and Enrollment Form, following your determination of medical necessity. Verification of insurance coverage is ultimately the responsibility of the provider. Since reimbursement by payers is subject to many factors, RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America do not represent or guarantee that payer reimbursement or any other payment or reimbursement of any kind will be made. Information provided as a result of the benefit investigation is provided for general reference and informational purposes only. RxCrossroads by McKesson makes every effort to be accurate in the information provided; however, no representations or warranties are expressed or implied by RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America regarding the accuracy or reliability of the information. RxCrossroads by McKesson or Mitsubishi Tanabe Pharma America, or its agents or employees shall not be liable legally, financially, or otherwise, for damages of any kind as a result of or related to these services. Providers and other users of this information resulting from benefit investigation services accept full responsibility for use of the service. Mitsubishi Tanabe Pharma America does not assume responsibility for, nor does it guarantee the availability, scope, or quality of the services offered including reimbursement support, prescription fulfillment coordination, and other services under Searchlight Support®. Providers, not Mitsubishi Tanabe Pharma America, are responsible for the services they provide. The Searchlight Support® services have no value apart from the product. Please see Prescribing Information for RADICAVA® (edaravone), available at radicava.com. Confidentiality Notice: The information contained in this facsimile may be confidential and legally privileged. It is intended only for use of the individual named. If you are not the intended recipient, you are hereby notified that the disclosure, copying, distribution, or taking of any action in regards to the contents of this fax–except its direct delivery to the intended recipient–is strictly prohibited. If you have received this fax in error, please notify the sender immediately and destroy this cover sheet along with its contents, and delete from your system, if applicable.
SAMPLE
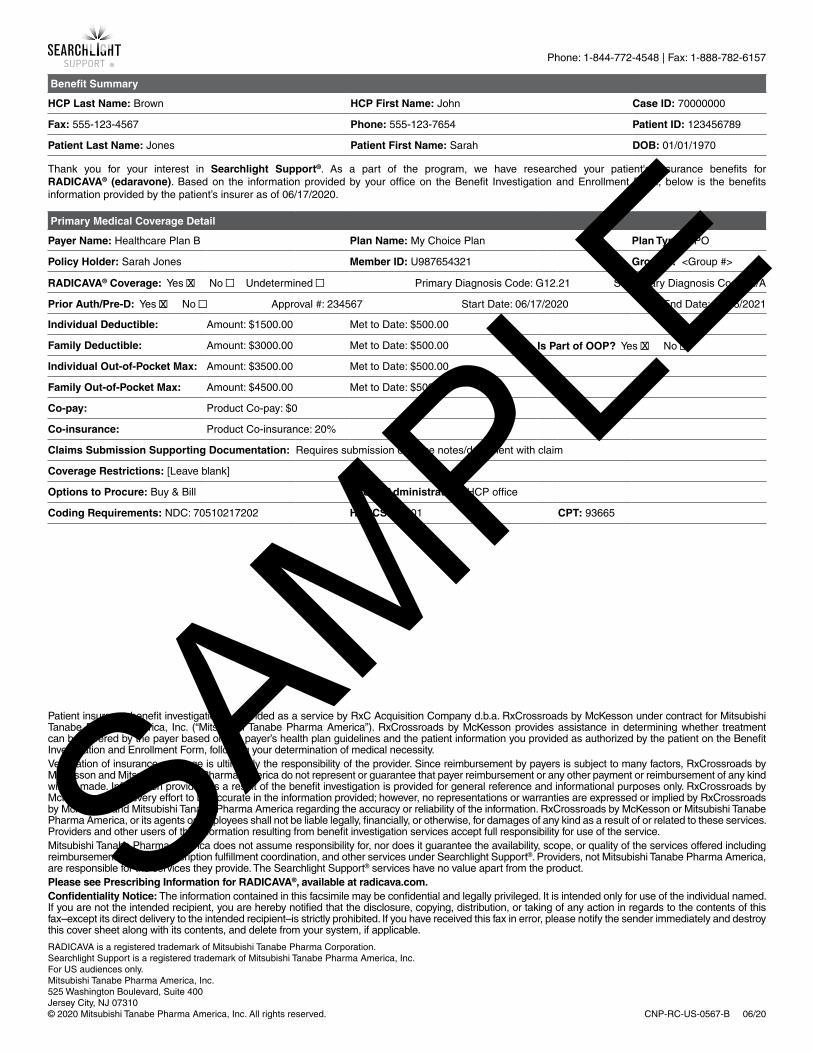
Phone: 1-844-772-4548 | Fax: 1-888-782-6157
Patient insurance benefit investigation is provided as a service by RxC Acquisition Company d.b.a. RxCrossroads by McKesson under contract for Mitsubishi Tanabe Pharma America, Inc. (“Mitsubishi Tanabe Pharma America”). RxCrossroads by McKesson provides assistance in determining whether treatment can be covered by the payer based on the payer’s health plan guidelines and the patient information you provided as authorized by the patient on the Benefit Investigation and Enrollment Form, following your determination of medical necessity. Verification of insurance coverage is ultimately the responsibility of the provider. Since reimbursement by payers is subject to many factors, RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America do not represent or guarantee that payer reimbursement or any other payment or reimbursement of any kind will be made. Information provided as a result of the benefit investigation is provided for general reference and informational purposes only. RxCrossroads by McKesson makes every effort to be accurate in the information provided; however, no representations or warranties are expressed or implied by RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America regarding the accuracy or reliability of the information. RxCrossroads by McKesson or Mitsubishi Tanabe Pharma America, or its agents or employees shall not be liable legally, financially, or otherwise, for damages of any kind as a result of or related to these services. Providers and other users of this information resulting from benefit investigation services accept full responsibility for use of the service. Mitsubishi Tanabe Pharma America does not assume responsibility for, nor does it guarantee the availability, scope, or quality of the services offered including reimbursement support, prescription fulfillment coordination, and other services under Searchlight Support®. Providers, not Mitsubishi Tanabe Pharma America, are responsible for the services they provide. The Searchlight Support® services have no value apart from the product. Please see Prescribing Information for RADICAVA®, available at radicava.com. Confidentiality Notice: The information contained in this facsimile may be confidential and legally privileged. It is intended only for use of the individual named. If you are not the intended recipient, you are hereby notified that the disclosure, copying, distribution, or taking of any action in regards to the contents of this fax–except its direct delivery to the intended recipient–is strictly prohibited. If you have received this fax in error, please notify the sender immediately and destroy this cover sheet along with its contents, and delete from your system, if applicable.
RADICAVA is a registered trademark of Mitsubishi Tanabe Pharma Corporation. Searchlight Support is a registered trademark of Mitsubishi Tanabe Pharma America, Inc. For US audiences only. Mitsubishi Tanabe Pharma America, Inc. 525 Washington Boulevard, Suite 400 Jersey City, NJ 07310 © 2020 Mitsubishi Tanabe Pharma America, Inc. All rights reserved. CNP-RC-US-0567-B 06/20
Benefit Summary
HCP Last Name: Brown HCP First Name: John Case ID: 70000000
Fax: 555-123-4567 Phone: 555-123-7654 Patient ID: 123456789
Patient Last Name: Jones Patient First Name: Sarah DOB: 01/01/1970
Thank you for your interest in Searchlight Support®. As a part of the program, we have researched your patient's insurance benefits for RADICAVA® (edaravone). Based on the information provided by your office on the Benefit Investigation and Enrollment Form, below is the benefits information provided by the patient’s insurer as of 06/17/2020.
Primary Medical Coverage Detail
Payer Name: Healthcare Plan B Plan Name: My Choice Plan Plan Type: PPO
Policy Holder: Sarah Jones Member ID: U987654321 Group #: <Group #>
RADICAVA® Coverage: Yes ■ No ■ Undetermined ■ Primary Diagnosis Code: G12.21 Secondary Diagnosis Code: N/A
Prior Auth/Pre-D: Yes ■ No ■ Approval #: 234567 Start Date: 06/17/2020 End Date: 06/16/2021
Individual Deductible: Amount: $1500.00 Met to Date: $500.00
Family Deductible: Amount: $3000.00 Met to Date: $500.00 Is Part of OOP? Yes ■ No ■
Individual Out-of-Pocket Max: Amount: $3500.00 Met to Date: $500.00
Family Out-of-Pocket Max: Amount: $4500.00 Met to Date: $500.00
Co-pay: Product Co-pay: $0
Co-insurance: Product Co-insurance: 20%
Claims Submission Supporting Documentation: Requires submission of office notes/document with claim
Coverage Restrictions: [Leave blank]
Options to Procure: Buy & Bill Site of Administration: HCP office
Coding Requirements: NDC: 70510217202 HCPCS: J1301 CPT: 93665
X
X
X
SAMPLE
Phone: 1-844-772-4548 | Fax: 1-888-782-6157
Patient insurance benefit investigation is provided as a service by RxC Acquisition Company d.b.a. RxCrossroads by McKesson under contract for Mitsubishi Tanabe Pharma America, Inc. (“Mitsubishi Tanabe Pharma America”). RxCrossroads by McKesson provides assistance in determining whether treatment can be covered by the payer based on the payer’s health plan guidelines and the patient information you provided as authorized by the patient on the Benefit Investigation and Enrollment Form, following your determination of medical necessity. Verification of insurance coverage is ultimately the responsibility of the provider. Since reimbursement by payers is subject to many factors, RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America do not represent or guarantee that payer reimbursement or any other payment or reimbursement of any kind will be made. Information provided as a result of the benefit investigation is provided for general reference and informational purposes only. RxCrossroads by McKesson makes every effort to be accurate in the information provided; however, no representations or warranties are expressed or implied by RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America regarding the accuracy or reliability of the information. RxCrossroads by McKesson or Mitsubishi Tanabe Pharma America, or its agents or employees shall not be liable legally, financially, or otherwise, for damages of any kind as a result of or related to these services. Providers and other users of this information resulting from benefit investigation services accept full responsibility for use of the service. Mitsubishi Tanabe Pharma America does not assume responsibility for, nor does it guarantee the availability, scope, or quality of the services offered including reimbursement support, prescription fulfillment coordination, and other services under Searchlight Support®. Providers, not Mitsubishi Tanabe Pharma America, are responsible for the services they provide. The Searchlight Support® services have no value apart from the product. Please see Prescribing Information for RADICAVA®, available at radicava.com. Confidentiality Notice: The information contained in this facsimile may be confidential and legally privileged. It is intended only for use of the individual named. If you are not the intended recipient, you are hereby notified that the disclosure, copying, distribution, or taking of any action in regards to the contents of this fax–except its direct delivery to the intended recipient–is strictly prohibited. If you have received this fax in error, please notify the sender immediately and destroy this cover sheet along with its contents, and delete from your system, if applicable.
RADICAVA is a registered trademark of Mitsubishi Tanabe Pharma Corporation. Searchlight Support is a registered trademark of Mitsubishi Tanabe Pharma America, Inc. For US audiences only. Mitsubishi Tanabe Pharma America, Inc. 525 Washington Boulevard, Suite 400 Jersey City, NJ 07310 © 2020 Mitsubishi Tanabe Pharma America, Inc. All rights reserved. CNP-RC-US-0567-B 06/20
Secondary Medical Coverage Detail
Payer Name: N/A Plan Name: N/A Plan Type: N/A
Policy Holder: N/A Member ID: N/A Group #: N/A
RADICAVA® (edaravone) Coverage: Yes ■ No ■ Undetermined ■ Primary Diagnosis Code: N/A Secondary Diagnosis Code: N/A
Prior Auth/Pre-D: Yes ■ No ■ Approval #: N/A Start Date: N/A End Date: N/A
Individual Deductible: Amount: N/A Met to Date: N/A
Family Deductible: Amount: N/A Met to Date: N/A Is Part of OOP? Yes ■ No ■
Individual Out-of-Pocket Max: Amount: N/A Met to Date: N/A
Family Out-of-Pocket Max: Amount: N/A Met to Date: N/A
Co-pay: Product Co-pay: N/A
Co-insurance: Product Co-insurance: N/A
Claims Submission Supporting Documentation: N/A
Coverage Restrictions: N/A
Options to Procure: N/A Site of Administration: N/A
Coding Requirements: NDC: N/A HCPCS: N/A CPT: N/A
Tertiary Medical Coverage Detail
Payer Name: N/A Plan Name: N/A Plan Type: N/A
Policy Holder: N/A Member ID: N/A Group #: N/A
RADICAVA® Coverage: Yes ■ No ■ Undetermined ■ Primary Diagnosis Code: N/A Secondary Diagnosis Code: N/A
Prior Auth/Pre-D: Yes ■ No ■ Approval #: N/A Start Date: N/A End Date: N/A
Individual Deductible: Amount: N/A Met to Date: N/A
Family Deductible: Amount: N/A Met to Date: N/A Is Part of OOP? Yes ■ No ■
Individual Out-of-Pocket Max: Amount: N/A Met to Date: N/A
Family Out-of-Pocket Max: Amount: N/A Met to Date: N/A
Co-pay: Product Co-pay: N/A
Co-insurance: Product Co-insurance: N/A
Claims Submission Supporting Documentation: N/A
Coverage Restrictions: N/A
Options to Procure: N/A Site of Administration: N/A
Coding Requirements: NDC: N/A HCPCS: N/A CPT: N/A
SAMPLE
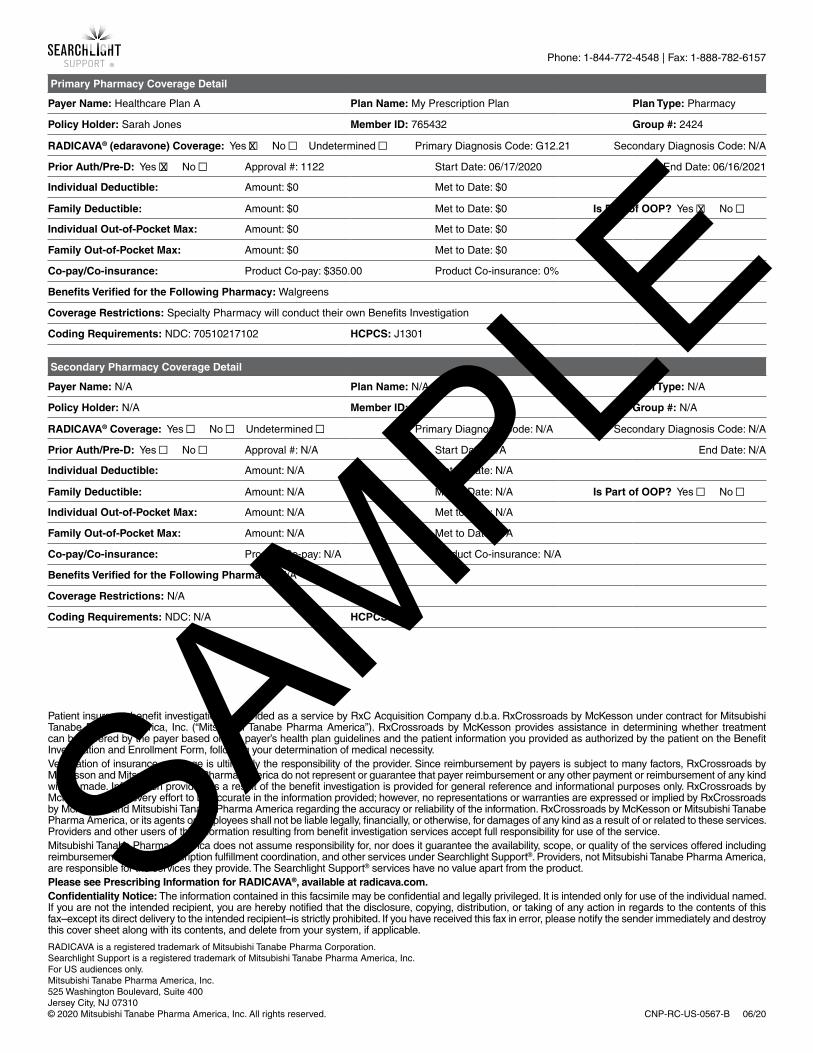
Phone: 1-844-772-4548 | Fax: 1-888-782-6157
Patient insurance benefit investigation is provided as a service by RxC Acquisition Company d.b.a. RxCrossroads by McKesson under contract for Mitsubishi Tanabe Pharma America, Inc. (“Mitsubishi Tanabe Pharma America”). RxCrossroads by McKesson provides assistance in determining whether treatment can be covered by the payer based on the payer’s health plan guidelines and the patient information you provided as authorized by the patient on the Benefit Investigation and Enrollment Form, following your determination of medical necessity. Verification of insurance coverage is ultimately the responsibility of the provider. Since reimbursement by payers is subject to many factors, RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America do not represent or guarantee that payer reimbursement or any other payment or reimbursement of any kind will be made. Information provided as a result of the benefit investigation is provided for general reference and informational purposes only. RxCrossroads by McKesson makes every effort to be accurate in the information provided; however, no representations or warranties are expressed or implied by RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America regarding the accuracy or reliability of the information. RxCrossroads by McKesson or Mitsubishi Tanabe Pharma America, or its agents or employees shall not be liable legally, financially, or otherwise, for damages of any kind as a result of or related to these services. Providers and other users of this information resulting from benefit investigation services accept full responsibility for use of the service. Mitsubishi Tanabe Pharma America does not assume responsibility for, nor does it guarantee the availability, scope, or quality of the services offered including reimbursement support, prescription fulfillment coordination, and other services under Searchlight Support®. Providers, not Mitsubishi Tanabe Pharma America, are responsible for the services they provide. The Searchlight Support® services have no value apart from the product. Please see Prescribing Information for RADICAVA®, available at radicava.com. Confidentiality Notice: The information contained in this facsimile may be confidential and legally privileged. It is intended only for use of the individual named. If you are not the intended recipient, you are hereby notified that the disclosure, copying, distribution, or taking of any action in regards to the contents of this fax–except its direct delivery to the intended recipient–is strictly prohibited. If you have received this fax in error, please notify the sender immediately and destroy this cover sheet along with its contents, and delete from your system, if applicable.
RADICAVA is a registered trademark of Mitsubishi Tanabe Pharma Corporation. Searchlight Support is a registered trademark of Mitsubishi Tanabe Pharma America, Inc. For US audiences only. Mitsubishi Tanabe Pharma America, Inc. 525 Washington Boulevard, Suite 400 Jersey City, NJ 07310 © 2020 Mitsubishi Tanabe Pharma America, Inc. All rights reserved. CNP-RC-US-0567-B 06/20
Primary Pharmacy Coverage Detail
Payer Name: Healthcare Plan A Plan Name: My Prescription Plan Plan Type: Pharmacy
Policy Holder: Sarah Jones Member ID: 765432 Group #: 2424
RADICAVA® (edaravone) Coverage: Yes ■ No ■ Undetermined ■ Primary Diagnosis Code: G12.21 Secondary Diagnosis Code: N/A
Prior Auth/Pre-D: Yes ■ No ■ Approval #: 1122 Start Date: 06/17/2020 End Date: 06/16/2021
Individual Deductible: Amount: $0 Met to Date: $0
Family Deductible: Amount: $0 Met to Date: $0 Is Part of OOP? Yes ■ No ■
Individual Out-of-Pocket Max: Amount: $0 Met to Date: $0
Family Out-of-Pocket Max: Amount: $0 Met to Date: $0
Co-pay/Co-insurance: Product Co-pay: $350.00 Product Co-insurance: 0%
Benefits Verified for the Following Pharmacy: Walgreens
Coverage Restrictions: Specialty Pharmacy will conduct their own Benefits Investigation
Coding Requirements: NDC: 70510217102 HCPCS: J1301
Secondary Pharmacy Coverage Detail
Payer Name: N/A Plan Name: N/A Plan Type: N/A
Policy Holder: N/A Member ID: N/A Group #: N/A
RADICAVA® Coverage: Yes ■ No ■ Undetermined ■ Primary Diagnosis Code: N/A Secondary Diagnosis Code: N/A
Prior Auth/Pre-D: Yes ■ No ■ Approval #: N/A Start Date: N/A End Date: N/A
Individual Deductible: Amount: N/A Met to Date: N/A
Family Deductible: Amount: N/A Met to Date: N/A Is Part of OOP? Yes ■ No ■
Individual Out-of-Pocket Max: Amount: N/A Met to Date: N/A
Family Out-of-Pocket Max: Amount: N/A Met to Date: N/A
Co-pay/Co-insurance: Product Co-pay: N/A Product Co-insurance: N/A
Benefits Verified for the Following Pharmacy: N/A
Coverage Restrictions: N/A
Coding Requirements: NDC: N/A HCPCS: N/A
X
X
X
SAMPLE
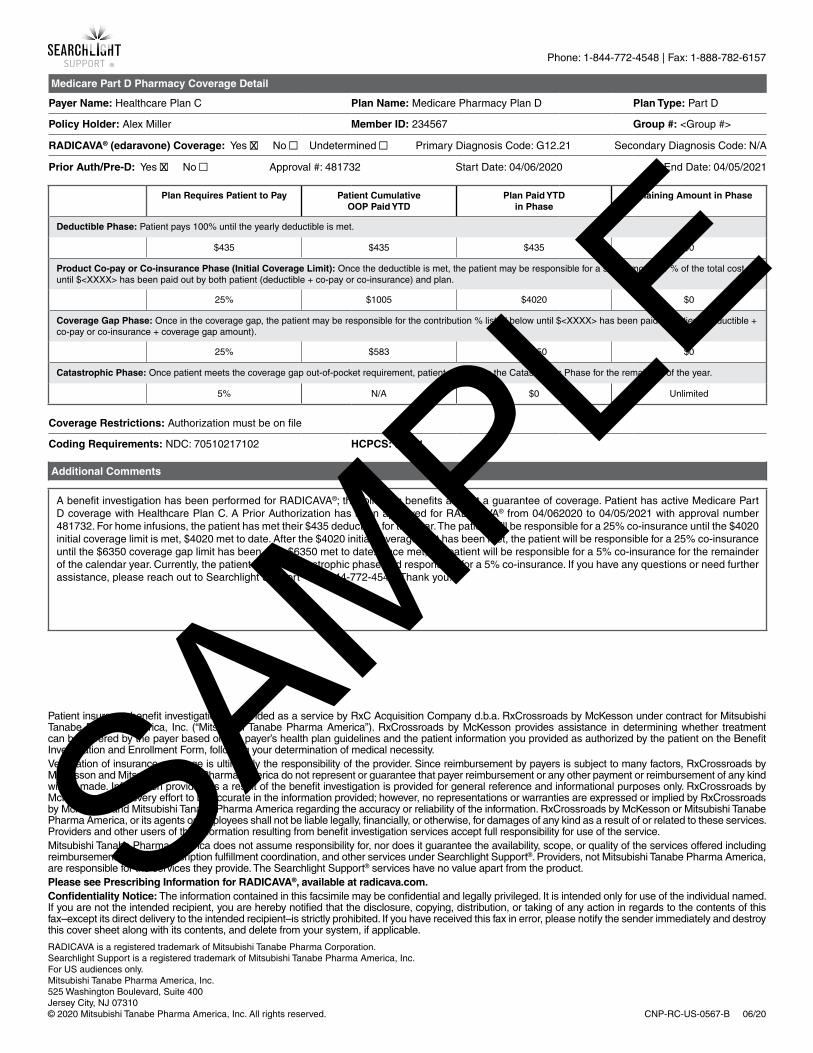
Phone: 1-844-772-4548 | Fax: 1-888-782-6157
Patient insurance benefit investigation is provided as a service by RxC Acquisition Company d.b.a. RxCrossroads by McKesson under contract for Mitsubishi Tanabe Pharma America, Inc. (“Mitsubishi Tanabe Pharma America”). RxCrossroads by McKesson provides assistance in determining whether treatment can be covered by the payer based on the payer’s health plan guidelines and the patient information you provided as authorized by the patient on the Benefit Investigation and Enrollment Form, following your determination of medical necessity. Verification of insurance coverage is ultimately the responsibility of the provider. Since reimbursement by payers is subject to many factors, RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America do not represent or guarantee that payer reimbursement or any other payment or reimbursement of any kind will be made. Information provided as a result of the benefit investigation is provided for general reference and informational purposes only. RxCrossroads by McKesson makes every effort to be accurate in the information provided; however, no representations or warranties are expressed or implied by RxCrossroads by McKesson and Mitsubishi Tanabe Pharma America regarding the accuracy or reliability of the information. RxCrossroads by McKesson or Mitsubishi Tanabe Pharma America, or its agents or employees shall not be liable legally, financially, or otherwise, for damages of any kind as a result of or related to these services. Providers and other users of this information resulting from benefit investigation services accept full responsibility for use of the service. Mitsubishi Tanabe Pharma America does not assume responsibility for, nor does it guarantee the availability, scope, or quality of the services offered including reimbursement support, prescription fulfillment coordination, and other services under Searchlight Support®. Providers, not Mitsubishi Tanabe Pharma America, are responsible for the services they provide. The Searchlight Support® services have no value apart from the product. Please see Prescribing Information for RADICAVA®, available at radicava.com. Confidentiality Notice: The information contained in this facsimile may be confidential and legally privileged. It is intended only for use of the individual named. If you are not the intended recipient, you are hereby notified that the disclosure, copying, distribution, or taking of any action in regards to the contents of this fax–except its direct delivery to the intended recipient–is strictly prohibited. If you have received this fax in error, please notify the sender immediately and destroy this cover sheet along with its contents, and delete from your system, if applicable.
RADICAVA is a registered trademark of Mitsubishi Tanabe Pharma Corporation. Searchlight Support is a registered trademark of Mitsubishi Tanabe Pharma America, Inc. For US audiences only. Mitsubishi Tanabe Pharma America, Inc. 525 Washington Boulevard, Suite 400 Jersey City, NJ 07310 © 2020 Mitsubishi Tanabe Pharma America, Inc. All rights reserved. CNP-RC-US-0567-B 06/20
Medicare Part D Pharmacy Coverage Detail
Payer Name: Healthcare Plan C Plan Name: Medicare Pharmacy Plan D Plan Type: Part D
Policy Holder: Alex Miller Member ID: 234567 Group #: <Group #>
RADICAVA® (edaravone) Coverage: Yes ■ No ■ Undetermined ■ Primary Diagnosis Code: G12.21 Secondary Diagnosis Code: N/A
Prior Auth/Pre-D: Yes ■ No ■ Approval #: 481732 Start Date: 04/06/2020 End Date: 04/05/2021
Plan Requires Patient to Pay Patient CumulativeOOP Paid YTD
Plan Paid YTDin Phase
Remaining Amount in Phase
Deductible Phase: Patient pays 100% until the yearly deductible is met.
$435 $435 $435 $0
Product Co-pay or Co-insurance Phase (Initial Coverage Limit): Once the deductible is met, the patient may be responsible for a set $ amount or % of the total cost until $<XXXX> has been paid out by both patient (deductible + co-pay or co-insurance) and plan.
25% $1005 $4020 $0
Coverage Gap Phase: Once in the coverage gap, the patient may be responsible for the contribution % listed below until $<XXXX> has been paid by patient (deductible + co-pay or co-insurance + coverage gap amount).
25% $583 $6350 $0
Catastrophic Phase: Once patient meets the coverage gap out-of-pocket requirement, patient remains in the Catastrophic Phase for the remainder of the year.
5% N/A $0 Unlimited
Coverage Restrictions: Authorization must be on file
Coding Requirements: NDC: 70510217102 HCPCS: J1301
Additional Comments
A benefit investigation has been performed for RADICAVA®; the following benefits are not a guarantee of coverage. Patient has active Medicare Part D coverage with Healthcare Plan C. A Prior Authorization has been approved for RADICAVA® from 04/062020 to 04/05/2021 with approval number 481732. For home infusions, the patient has met their $435 deductible for the year. The patient will be responsible for a 25% co-insurance until the $4020 initial coverage limit is met, $4020 met to date. After the $4020 initial coverage limit has been met, the patient will be responsible for a 25% co-insurance until the $6350 coverage gap limit has been met, $6350 met to date. Once met, the patient will be responsible for a 5% co-insurance for the remainder of the calendar year. Currently, the patient is in the catastrophic phase and responsible for a 5% co-insurance. If you have any questions or need further assistance, please reach out to Searchlight Support® at 1-844-772-4548. Thank you.
X
X
SAMPLE
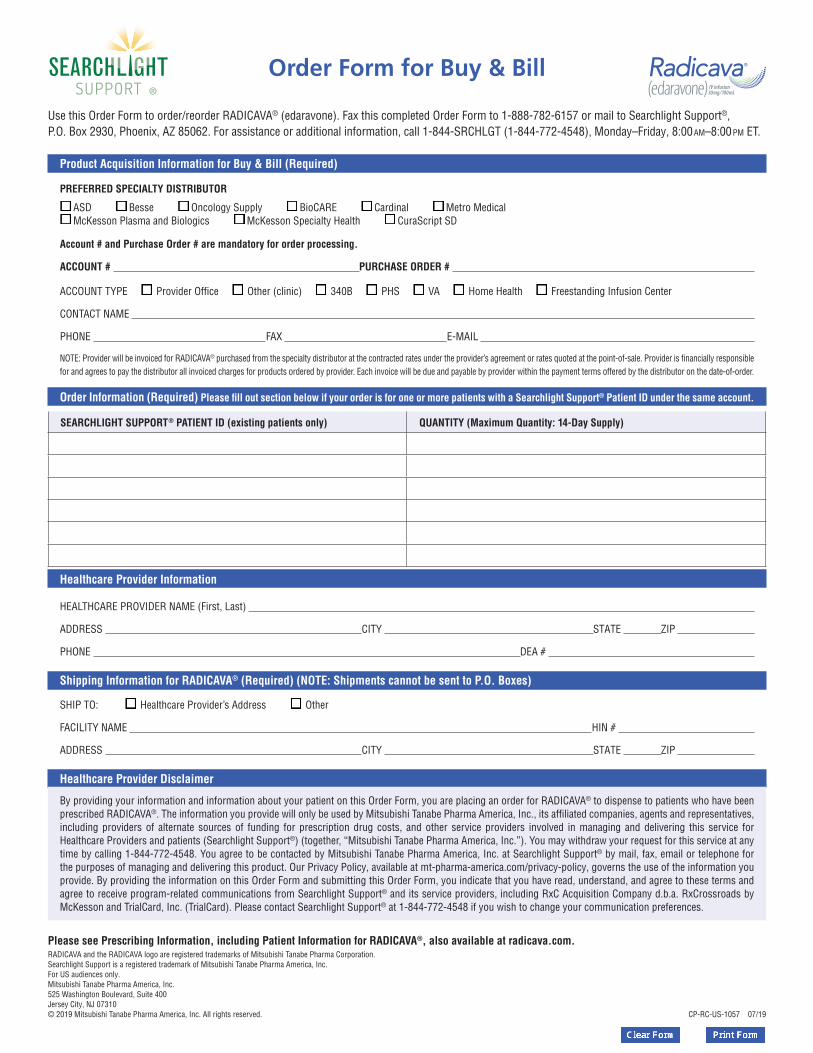
Product Acquisition Information for Buy & Bill (Required)
PREFERRED SPECIALTY DISTRIBUTOR
ASD Besse Oncology Supply BioCARE Cardinal Metro Medical McKesson Plasma and Biologics McKesson Specialty Health CuraScript SD
Account # and Purchase Order # are mandatory for order processing.
ACCOUNT # PURCHASE ORDER #
ACCOUNT TYPE Provider Office Other (clinic) 340B PHS VA Home Health Freestanding Infusion Center
CONTACT NAME
PHONE FAX E-MAIL
NOTE: Provider will be invoiced for RADICAVA® purchased from the specialty distributor at the contracted rates under the provider’s agreement or rates quoted at the point-of-sale. Provider is financially responsible for and agrees to pay the distributor all invoiced charges for products ordered by provider. Each invoice will be due and payable by provider within the payment terms offered by the distributor on the date-of-order.
Order Information (Required) Please fill out section below if your order is for one or more patients with a Searchlight Support® Patient ID under the same account.
Healthcare Provider Information
HEALTHCARE PROVIDER NAME (First, Last)
ADDRESS CITY STATE ZIP
PHONE DEA #
Shipping Information for RADICAVA® (Required) (NOTE: Shipments cannot be sent to P.O. Boxes)
SHIP TO: Healthcare Provider’s Address Other
FACILITY NAME HIN #
ADDRESS CITY STATE ZIP
Healthcare Provider Disclaimer
By providing your information and information about your patient on this Order Form, you are placing an order for RADICAVA® to dispense to patients who have been prescribed RADICAVA®. The information you provide will only be used by Mitsubishi Tanabe Pharma America, Inc., its affiliated companies, agents and representatives, including providers of alternate sources of funding for prescription drug costs, and other service providers involved in managing and delivering this service for Healthcare Providers and patients (Searchlight Support®) (together, “Mitsubishi Tanabe Pharma America, Inc.”). You may withdraw your request for this service at any time by calling 1-844-772-4548. You agree to be contacted by Mitsubishi Tanabe Pharma America, Inc. at Searchlight Support® by mail, fax, email or telephone for the purposes of managing and delivering this product. Our Privacy Policy, available at mt-pharma-america.com/privacy-policy, governs the use of the information you provide. By providing the information on this Order Form and submitting this Order Form, you indicate that you have read, understand, and agree to these terms and agree to receive program-related communications from Searchlight Support® and its service providers, including RxC Acquisition Company d.b.a. RxCrossroads by McKesson and TrialCard, Inc. (TrialCard). Please contact Searchlight Support® at 1-844-772-4548 if you wish to change your communication preferences.
Use this Order Form to order/reorder RADICAVA® (edaravone). Fax this completed Order Form to 1-888-782-6157 or mail to Searchlight Support®, P.O. Box 2930, Phoenix, AZ 85062. For assistance or additional information, call 1-844-SRCHLGT (1-844-772-4548), Monday–Friday, 8:00am–8:00pm ET.
SEARCHLIGHT SUPPORT® PATIENT ID (existing patients only) QUANTITY (Maximum Quantity: 14-Day Supply)
Please see Prescribing Information, including Patient Information for RADICAVA®, also available at radicava.com.RADICAVA and the RADICAVA logo are registered trademarks of Mitsubishi Tanabe Pharma Corporation. Searchlight Support is a registered trademark of Mitsubishi Tanabe Pharma America, Inc.For US audiences only.Mitsubishi Tanabe Pharma America, Inc.525 Washington Boulevard, Suite 400Jersey City, NJ 07310© 2019 Mitsubishi Tanabe Pharma America, Inc. All rights reserved. CP-RC-US-1057 07/19
Order Form for Buy & Bill





























