-
PENATALAKSANAAN PASIEN DENGAN KELUHAN CHEST ( CARDIAC )
PAINWahyu Widjanarko
-
SUSPECTED CARDIAC PAIN :Clinical characteristics predictive of
AMI in ED px with chest pain :
Description of pain Prob.MI (%)Pressure, tightness, crushing
24Burning, Indigestion 23Ache 13 Sharp, Stabbing 5Pleuritic
7Radiation 19Reproducibility 5 6Combination 0
-
HOW TO MANAGE Px with CHEST PAIN Suspected cardiac painECGNo ECG
ST Normal ECG,CKMB,troponinIschaemic,CKMB/troponin ECG ST / LBBBAMI
guidelineSuspected ACSConfirmid ACS
-
Normal ECG/CKMB/Troponin at 12 hrs consider DischargeAdmit
CCU,ECG monitor,Aspirin/LMWH/-blockerStress testStable for 48
h,high risk features -Recurrent symptoms/ECG changes/other
indication of high riskCoroner AngiographyRisk stratificationLow
intermediate high
Discharge
Revascularisation/medical tx
-
ACUT CORONARY SYNDROME ( ACS ) DEFINISI : Segala bentuk gejala
klinisyang sesuai dengan kondisi iskemia miokard akut
Patogenese dan Presentasi klinis sama, berbeda dalam derajat
berat ringannya
-
ACUTE CORONARY SYNDROME
No ST Elevation ST ElevationUnstable AnginaNon-STEMINon-Q wave
MIQ wave MIBraunwald et al. JACC 2000;36:970-1062
-
Iskemia Jantung Demand O2 meningkat pada:Exercise, makan,
stress
Supply O2 berkurang akibat sumbatan (obstruksi) pembuluh darah
jantung seperti pada: aterosklerosis vasokonstriksi (spasme) bekuan
darah (thrombus)
Setelah lewat suatu batas waktu, jaringan iskemik akan mati
(nekrosis), dan akhirnya digantikan oleh jaringan parut yang
non-fungsional Infark Miokard
-
Tahapan Terbentuknya Aterosklerosis
Kerusakan endotelium pembuluh arteri
Trombosit/platelet melekat pada daerah yang rusak, diikuti
proliferasi endotel, pembentukan kapsul fibrosis dan penumpukan
kolesterol
Plak membesar, menutupi lumen arteri dan inti jaringan lemak
bertambah besar
-
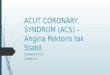
Oklusi sebagianPlak(inti kaya lemak,kapsul fibrosa)Plak pecah
Kumpulan agregasi platelet, thrombosisOklusi sebagianOklusi
komplitLysis and repairNo symptomsRapid progression of
atherosclerosisUnstable anginaNon Q wave MIAngina,ECG
changes,Troponin releaseQ wave MINon Q-wave MIAngina,ECG
changes,Troponin releasetrombolisistrombosisCollateralsMonosit,
macrofag, inflamasiPlak tidak stabil pada ACS
-
APTS/NSTEMI Diagnosa berdasarkan riwayat penyakit, EKG 12 lead,
cardiac enzymes (CK, CK-MB, LDH) atau petanda lain di plasma
(troponin I atau T)
1. Klinis sama: 1. Angina saat istirahat terus menerus > 15
mnt 2. Angina pertama kali (CCS class III ) 3. Angina yang
meningkat ( makin lama, sering dan mudah tercetus )
2. EKG dan petanda biokimia kerusakan miokard berbeda
-
EKG : Segmen ST depresi ST elevasi transient spontan hilang dg
atau tanpa nitrat Gelombang T inversi Riwayat infark miokard LBBB
Perubahan yang tidak spesific Normal
-
ENZIM dan PETANDA JANTUNG : Conventional cardiac enzyms ( CK,
CK-MB, LDH ) bisa normal atau meningkat Troponin T ( > 0,1 ug/l
) atau Troponin I ( > 0,4 ug/l ) merupakan petanda spesifik
terjadinya kerusakan miokard High risk px Evaluasi troponin normal
atau tidak terdeteksi dalam 12 jam Low risk px
-
3. STRATIFIKASI RESIKO :Resiko tinggi : - Usia > 65 th -
Nyeri saat istirahat > 15 - Perubahan segmen ST dinamis - ST
depresi transient - Angina tdk stabil paska infark - Comorbid : DM
- Troponin T/I - Fungsi Vki - Aritmia mayor
-
PenatalaksanaanPengobatan darurat / immediate treatment:Oksigen,
morfin, nitrogliserinMenghilangkan nyeri, mencegah terjadinya MI
dan kematian akibat perluasan thrombus
Reperfusi segera:Thrombolitic agents (aspirin,
heparin)Mechanical reperfusion (PCI, CABG)
-
PenatalaksanaanANTI ISKEMIKMengoptimalisasi keseimbangan antara
kebutuhan dan supply oksigen pada miokardiumANTI TROMBOTIKMengatasi
proses perjalanan penyakit yakni pada pembentukan trombus
-
Antiiskemik Beta blockerTerapi tunggal pada unstable angina,
kombinasi dengan nitrat untuk mencegah recurrent iskemiaMengurangi
kebutuhan oksigen, menurunkan HR dan tekanan darahKontraindikasi
pada jenis angina vasospastik
-
Antiiskemik - Calcium channel blockerBaik untuk vasodilator pada
angina
Tidak ada bukti manfaatnya pada pencegahan infark miokard.
Memberikan hasil yang baik dalam jangka pendek pada episode
iskemik.
-
Antiiskemik - Nitrat
VasodilatorMengurangi konsumsi oksigenEfektif menurunkan jumlah
episode iskemiaSediaan sublingual, spray, IV (dosis disesuaikan
dengan gejala klinis dan EKG)
-
Jenis Antitrombotik Obat anti platelet/antitrombosis aspirin,
clopidogrel / ticlopidine, anti Gp IIb/IIIaMencegah haemostasis
primer
Antikoagulanheparin, LMWHMencegah perluasan trombus
TrombolitikstreptokinaseMenghancurkan trombus
-
Antitrombotik pada Unstable Angina
AspirinHeparinLMWH
-
AspirinAgregasi platelet = titik awal pembentukan
trombusMenghambat enzim platelet (cyclooxygenase) , mengganggu
sintesa aktivator platelet (thromboxane A2)Dosis: 75mg/hari 325 mg
q.i.d.Unstable angina akut diberikan secepat mungkin, dosis awal
150-325 mg
-
Heparin (UFH)
Mencegah pembentukan dan perluasan trombus (anti Xa dan IIa)
Manfaatnya sulit dibuktikan dari studi klinis.
-
Keunggulan Potensial LMWHBioavailabilitas total dengan pemberian
per SK Waktu paruh panjang Tidak ada ikatan endotelInteraksi dengan
platelet minimalIkatan protein plasma minimalSensitivitas terhadap
PF4 rendahPemberian per SKlebih mudah penggunaannyaEfek
antikoagulan stabil dan dapat diprediksi
Lebih aman tanpa kontrol biologis
-
Studi klinis penggunaan LMWHpada ACSFRISCDalteparin dibanding
plasebo (1996)FRISC IIDalteparin dibanding plasebo (1999)
FRICDalteparin dibanding UFH (1996)
ESSENCEEnoxaparin dibanding UFH (1997)TIMI 11BEnoxaparin
dibanding UFH (1998)
FRAXISNadroparin dibanding UFH (1998)
-
STEMI Dx 2 dari 3 kriteria ( WHO ) : 1. Nyeri dada iskemi yang
khas2. Evolusi EKG ( serial )3. Peningkatan yang diikuti penurunan
kadar enzim-2 jantung (CK-MB dan Troponin secara serial)
Strategi dan penanganan dini Early open artery dengan terapi
reperfusi : TROMBOLITIK atau PTCA PRIMER
-
2. Penanganan di ICVCU : Tindakan Umum : - Bed rest - Monitoring
Farmakoterapi : - Oksigen 2 4 l/mnt - Aspirin - - blocker - Nitrat
- ACEI
-
*Aterosklerosis adalah patologi dasar yang berhubungan dengan
ACS dan penyakit utama arteri koroner.Ruptur plag mengaktivasi
jalur ekstrinsik pada mekanisme pembekuan darah.Fibrin dihubungkan
pada stabilisasi pembekuan darah platelet berhenti yang segera
membentuk mengikuti luka endotelialBersama-sama : platelet, fibrin,
dan sel darah merah membentuk trombus intra-koroner yang berperan
pada UA / non-Q-wave MI (NQMI) dan AMI
**9b- Beta-blockers
These are effective in both symptomatic and prophylactic
treatment of myocardial infarction.
Beta-blockers are known to be moderate vasoconstrictors : they
must therefore be systematically associated with a nitrate and
preference should be given to cardioselective agents.
They are contra-indicated in vasospastic angina.
*10c- calcium-channel blockers
There is no evidence that calcium-channel blockers alone are of
benefit in the prevention of myocardial infarction.
However, in the short term, they do give good results in the
treatment of symptomatic or non-symptomatic ischemic episodes.
In cases where there is cause to suspect a vasospastic element,
the association of calcium-channel blockers is quite justified.
*8a- organic nitrates
Nitrates are vasodilators which reduce oxygen consumption.They
are widely used (based on empirical findings) and are extremely
effective for reducing the number of ischemic episodes during the
first few hours after initiation of intravenous treatment.
They are used in moderate doses to start (1 mg per hour in
continuous infusion) which are thereafter increased by progressive
stages according to the clinical response.
*3Reminder :Antithrombotics include 3 classes of drugs :-
antiplatelet drugs (aspirin, Ticlid[ticlopidine], ReoPro)-
anticoagulants (unfractionated heparin, LMWH, Antivitamin K)-
thrombolytics (streptokinase, Actilyse)
*1Antithromboticsin unstable angina
A. AspirinLewis, Cairns, RISC Studies
B. Unfractionated heparinThroux, RISC, ATACS Studies
C - Low Molecular Weight Heparins1. Potential advantages of
LMWH2. Clinical studiesFraxiparin : Garfinkel StudyFragmin : FRISC,
FRIC StudiesLovenox : TIMI 11A, ESSENCE Studies
*5A. Aspirin
Platelet aggregation on a ruptured atherosclerotic plaque is the
starting point for the formation of an intracoronary
thrombus.Antiplatelet drugs are consequently an essential element
in the treatment of unstable angina.Sufficient evidence exists to
prove their efficacy. The advantages of aspirin have been
demonstrated in all the studies in this field, regardless of the
duration of observation and the dosage used. (see Table : Lewis,
Cairns, RISC Studies).
Globally :aspirin reduces by half the occurence of myocardial
infarction and cardiac death.The doses of aspirin generally
administered are between 100 and 350 mg per day, but lower doses
have also been assessed (75 mg). Other antiplatelet drugs, such as
ticlopidine (TICLID) have also been proved to be effective and can
be used in patients unable to tolerate aspirin. Potent new
antiplatelet drugs, fibrinogen platelet receptor inhibitors (anti
GP IIb/IIIa) are currently being evaluated in the treatment of
unstable angina.
*7B. Unfractionated heparin
Standard or unfractionated heparin inhibits the production of
thrombin (anti Xa action) and also neutralises its effects (anti
IIa action).Its essential role is that of preventing the extension
of thrombi, without dissolving any already formed thrombi.Its use
in the treatment of unstable angina is therefore rational, even
though its efficacy has been difficult to demonstrate in clinical
trials.
*14C - Low Molecular Weight Heparins
1. Potential advantages of LMWH
The efficacy of low molecular weight heparins has been widely
demonstrated to be at least equal to that of unfractionated heparin
for the prophylaxis and treatment of venous thrombosis. They have
evident advantages in terms of convenience and simplicity of
use.
However, studies aiming at evaluating the use of low molecular
weight heparins in arterial pathology are relatively limited.
Nevertheless, they ought to be considered "a priori" to be at least
as effective as unfractionated heparin in the treatment of arterial
thrombosis and immediate prevention of their recurrence.Compared
with unfractionated heparin, they present potential advantages
which can be of major importance in the acute phase of arterial
accidents, coronary episodes in particular.
In these situations, rapid onset of effective anticoagulation is
essential.
*