Embed Size (px)
Citation preview

International Journal of Cardiology xxx (2014) xxx–xxx
IJCA-19163; No of Pages 7
Contents lists available at ScienceDirect
International Journal of Cardiology
j ourna l homepage: www.e lsev ie r .com/ locate / i j ca rd
Acute decompensated heart failure patients admitted to critical careunits: Insights from ASCEND-HF
Sean van Diepen a,b,⁎,1, Mohua Podder b, Adrian F. Hernandez c, Cynthia M.Westerhout b, Paul W. Armstong b,d,John J.V. McMurray e, Zubin J. Eapen c, Robert M. Califf c, Randall C. Starling f,Christopher M. O'Connor c, Justin A. Ezekowitz b,d,1
a Divisions of Critical Care and Cardiology, University of Alberta, Edmonton, Alberta, Canadab Canadian Vigour Center, Edmonton, Alberta, Canadac Duke Clinical Research Institute, Duke University Medical Center, Durham, NC, USAd Division of Cardiology, University of Alberta, Edmonton, Alberta, Canadae Western Infirmary, University of Glasgow, Glasgow, Scotland, United Kingdomf Cleveland Clinic, OH, USA
⁎ Corresponding author at: 2C2 Cardiology Walter MAlberta Hospital, 8440-11 St. Edmonton, Alberta T6G 2B7
E-mail address: [email protected] (S. van Diepen).1 SVD and JAE take responsibility for all aspects of the r
of the data presented and their discussed interpretation.
http://dx.doi.org/10.1016/j.ijcard.2014.11.0070167-5273/© 2014 Elsevier Ireland Ltd. All rights reserved
Please cite this article as: S. van Diepen, et alHF, Int J Cardiol (2014), http://dx.doi.org/10
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 20 September 2014Accepted 3 November 2014Available online xxxxKeywords:Heart failureCritical careCoronary care unitIntensive care unitOutcomes
Background: Little is known about global patterns of critical care unit (CCU) care and the relationship with out-comes in patients with acute decompensated heart failure (ADHF). Whether a ward or a CCU admission is asso-ciated with better outcomes is unclear.Methods: Patients in the Acute Study of Clinical Effectiveness of Nesiritide in Decompensated Heart Failure (AS-CEND-HF) trial were initially hospitalized in a ward or CCU (coronary or intensive care unit). Sites were geo-graphically classified: Asia-Pacific (AP), Central Europe (CE), Latin America (LA), North America (NA), andWestern-Europe (WE). The primary outcome of 30-day all-cause mortality or all-cause hospital readmissionwas adjusted using a two-stage multivariable logistic regression model with a generalized estimated equationthat took sites within each country as a nested random factor.Results:Overall, 1944 (38.2%) patients were admitted to a CCU and 3150 (61.8%) to a ward, and this varied by re-
gion: 50.6% AP, 63.3% CE, 60.7% WE, 22.1% LA, and 28.6% NA. The 30-day death or readmission rate was 15.2% inward patients and 17.0% in CCU patients (risk-adjusted Odds Ratio [OR] 1.44: 95% CI, 1.14–1.82). ComparedwithCCU patients in NA (24.1% 30-day event rate), the primary outcomes were: AP (10.4%, Odds Ratio [OR] 0.63; 95%confidence Interval [CI], 0.35 to 1.15), CE (10.4%, OR 0.56: 95% CI, 0.31 to 1.02), LA (22.4%, OR 0.60: 95% CI, 0.11 to3.32), andWE (11.2%, OR 0.63, 95% CI, 0.25 to 1.56). No regional differences in 30-day mortality were observed;however, 30-day readmission rates were highest in NA sites.Conclusions:Management of patients with ADHF varies significantly, and after adjustment, CCU care was associ-ated with higher risk of early mortality, not explained by international differences. These findings may help toimprove the early decisions regarding risk stratification of patients hospitalized with ADHF.© 2014 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
The growing prevalence of heart failure in the general populationhas coincided with an increase in hospital and critical care unit (CCU)HF admissions [1–3]. A reported 12–51% of European and 19–25% ofUnited States patients hospitalized with acute decompensate heart fail-ure (ADHF) are admitted to a CCU, yet no evidence-based guidance ex-ists on which patients are best suited for a CCU [4–7]. Importantly,
acKenzie Center, University of, Canada.
eliability and freedom from bias
.
., Acute decompensated heart
.1016/j.ijcard.2014.11.007
higher unadjusted mortality rates among ADHF patients admitted toCCU have been reported; however, little is known about the global pat-terns of care, resource utilization, and the clinical outcomes in this highrisk subset of patients after adjustment for key clinical information [4].
Hospitalization for ADHF is a well-recognized adverse prognosticmarker and the mortality among patients who survive to hospital dis-charge is up to 30% at 1 year [1,8]. Similarly, among patients admittedto medical and surgical intensive care units with diverse admission di-agnoses, post-discharge mortality rates are high and critical illness re-duces long-term survival [9–12]. Whether a CCU or ward admissionfor ADHF modifies survival remains unclear given the heterogeneity ofpatient, system and provider differences globally.
Accordingly, in the Acute Study of Clinical Effectiveness of Nesiritidein Decompensated Heart Failure (ASCEND-HF) trial we examined:
failure patients admitted to critical care units: Insights from ASCEND-

2 S. van Diepen et al. / International Journal of Cardiology xxx (2014) xxx–xxx
(1) global patterns in care, resource utilization, and associated clinicaloutcomes among hospitalized ADHF patients and (2) the short and in-termediate term prognosis associated with CCU and hospital wardADHF admissions.
2. Methods
The ASCEND-HF trial (ClinicalTrials.gov number NCT00475852) methods and resultshave been previously described [13,14]. Briefly, this was an international, multi-center,double-blind, randomized trial of nesiritide vs. placebo in patients hospitalized for acutedecompensated heart failure (ADHF). Patients ≥18 years were eligible for enrollment iftheywere hospitalizedwith ADHFwithin 24h or diagnosedwith ADHFwithin 48hof hos-pitalization for another reason. Key exclusion criteria included patients with a risk of hy-potension (systolic blood pressure b100 mm Hg or b110 mm Hg with intravenousvasodilators), systolic blood pressure N180 mm Hg, acute coronary syndromes, recent oranticipated inotropic therapy, dopamine ≥5 μg/kg/min, severe pulmonary disease, andrenal replacement therapy. The institutional review board of each participating site ap-proved the study and all study participants provided written informed consent.
2.1. Critical care study population and regional categorization
Case report formswere used to identify patient covariates, in-hospital treatments, andprocedures. Additional information captured included the number of days and type of unitthroughout the index hospitalization. Patients admitted to intensive care or coronary careunits for at least 1 night after randomization were considered to have CCU admission. Pa-tients with hospital admissions only to a general ward, emergency department, and/orstep-down unit were categorized as ward admissions. In order to eliminate any site-specific CCU bias mandated by a trial site for the use of nesiritide, only patients admittedto institutions with study patients admitted to both ward and CCU were included in thisstudy. Study siteswere categorized into 5 geographic regions according to previously pub-lished ASCEND-HF categorizations: Asia-Pacific, Central Europe, Latin America, NorthAmerica, and Western-Europe [15]. The primary analysis compared in-hospital pharma-ceutical andmechanical device therapies, and compared clinical outcomes across interna-tional study regions among patients admitted to a CCUwith ADHF. The secondary analysiscompared outcomes between ADHF patients with CCU and ward admissions.
2.2. Outcomes
The primary outcome of interest was 30 day all-cause mortality or all-cause hospitalreadmission. Other outcomes included 30 day all-causemortality, 30-day all-cause hospi-tal readmission, 30-day ADHF readmission, and 31–180 all-cause mortality.
2.3. Statistical methods
Patient characteristics, demographics, laboratory values, medical treatments and out-comes for the selected cohort of 5094 patients were described by CCU and ward admis-sions. Median and interquartile ranges were presented for continuous variables; andcounts with proportions were presented for discrete variables. The Wilcoxon rank sumand chi-square tests were applied to test the differences between the prospective studygroups for continuous and discrete variables, respectively. The Fisher's exact test was ap-plied to categorical variables with a cell count of ≤5.
To maintain stability of the statistical model, countries with b20 critical care or totalpatients were removed. A total of 4587 patients (1854 CCU and 2733ward)were includedin themodeling. Regional 30 day outcomes in CCU patients, using North America as a ref-erence region, were analyzed using a two-stage multivariable logistic regression modelwith a generalized estimated equation (GEE), taking sites within each country as a nestedrandom factor [16,17]. The exchangeable correlation structurewas applied as theworkingcorrelation matrix for each of the GEE models. Outcomes between CCU versus ward pa-tients were similarly evaluated using a GEE model. A Frailty Cox Proportional HazardsModel taking sites with each country as a nested random factor was used to evaluate31–180 day mortality [18].
In order to mitigate potential bias related to the admission to a CCU, models compar-ing CCU versus ward patients included propensity scores of belonging to either group asinverse probability weights (see Appendix 1 for propensity model covariates andweighting) [19,20]. In addition, tomitigate the potential lead time bias (due to differencesin lengths of hospital stay among CCU and ward patients) with 30 day readmission, thesecondary analysis was landmarked to include patients who survived to 7 days after hos-pital admission. The list of adjusting covariates for all the abovemodels included previous-ly developed and validated ASCEND-HF risk model covariates in addition to a set ofclinically relevant baseline and at-discharge variables (see Appendix 2) [21]. Results forall 30 daymodels were presented as adjusted Odds Ratios (OR) and 95% confidence inter-vals (CI); and 31–180 daymodels through adjustedhazard ratios (HR) and 95% confidenceintervals (CI). Statistical significance was pre-determined as 2-sided α = 0.05.
3. Results
In the ASCEND-HF trial, 5094 (72.7%) patients were admitted to 224hospitals where study participants were admitted to either ward or
Please cite this article as: S. van Diepen, et al., Acute decompensated heartHF, Int J Cardiol (2014), http://dx.doi.org/10.1016/j.ijcard.2014.11.007
CCUs; 1815 (25.9%) patients at 173 sites were not enrolled in siteswith both CCUandward admissions and excluded from further analysis.Among the5094patients, 1944 (38.2%) patientswere admitted to a CCUfor at least one night, and 3150 (61.8%) were not. The percentage of pa-tients hospitalizedwith ADHF admitted to a CCUvaried by region: 50.6%in Asia-Pacific, 63.3% in Central European, 60.7% in Western European,22.1% in Latin American, and 28.6% in North American patients(p b 0.001 across regions). Differences in baseline characteristics be-tween participants with and without a CCU admission are provided inTable 1. Patients admitted to CCUs were more frequently male, white,had fewer medical co-morbidities, and a higher heart rate, respiratoryrate, blood urea nitrogen, troponin T, and lower serum sodium.
Regional differences in baseline characteristics of patients spendingat least one night in a CCU are presented in Appendix 3. Patients admit-ted toWestern European CCUs were older, more frequently female, andmore frequently had a history of a myocardial infarction or cancer.North American patientsmore frequently had a history of hypertension,hyperlipidemia, prior coronary revascularization, smoking, or chronicrespiratory disease. Central European patients had the highest medianbody mass index and rate of coronary artery disease. Asia-Pacific pa-tients had the highest median baseline heart rates, the lowest left ven-tricular ejection fractions, and the highest incidence of diabetes.
3.1. Global treatment differences in critical care patients
Differences in in-hospital treatment patterns were observed acrossregions (Table 2). Patients admitted to CCUs in Western Europe morefrequently received bolus intravenous loop diuretics within the first6 h of randomization, while Asian-Pacific patients most frequently re-ceived infusions of intravenous loop diuretics. In-hospital treatmentwith β-blockers was highest in North America, and aldosterone antago-nists and either angiotensin converting enzyme inhibitors or angioten-sin receptor blockers were highest in Central Europe. Digitalis use washighest in Asian-Pacific and Central European sites, and hydralazineuse was most prevalent in North America. The use of inotropes, vasodi-lators, and vasopressors was highest in Latin-America.
Invasive and non-invasive procedure rates differed across regions(Table 2). Approximately 11% of all Asian-Pacific, Latin American, andNorth American patients underwent mechanical ventilation. The useof non-invasive mechanical ventilation and intra-aortic balloon pumpcounter-pulsation was highest in North America while the applicationof ultrafiltration and dialysis was most common in Latin America.North American study participants admitted to CCUs were the mostlikely to undergo coronary angiography, cardiac surgery, and non-cardiac surgery, and have either an implantable cardioverter defibrilla-tor or cardiac resynchronization therapy. The application of non-invasive cardiac imaging was highest in Central Europe while non-invasive stress testingwas highest in North American study sites. Differ-ences in in-hospitalmedical therapies,mechanical therapies, and proce-dures between participants with and without a CCU admission arepresented in Appendix 4.
Total hospital and CCU length of stay (LOS) varied significantlyacross regions. Central Europeanpatients had the longestmedianhospi-tal LOS (10 nights) while Asia-Pacific patients had the shortest medianLOS (6 nights). Median CCU LOS was shortest among Asia-Pacific pa-tients (2 nights) and longest among Central European patients (5nights, Table 2).
3.2. Clinical outcomes
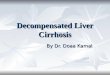
The overall primary outcome (30-day all-cause death or readmis-sion) occurred in 14.9% of patients in ASCEND-HF; the rate was 15.2%inward patients and 17.0% in CCU patients. In CCU patients, the primaryoutcome occurred in 24.1% of North American, 22.4% of Latin American,12.2% of Western European, 11.2% of Asian-Pacific, and 10.4% of CentralEuropean patients (p b 0.001 across groups; Fig. 1). There was no
failure patients admitted to critical care units: Insights from ASCEND-

Table 1Baseline characteristics among patients with and without a critical care unit admission.
Variable Ward admission(n = 3150)
Critical care unit admission(n = 1944)
p-Value
Age, years 66 (55–76) 67 (56.5–76) 0.067Female, n (%) 1140 (36.2) 619 (31.8) 0.001Race, n (%)
Asian 585 (18.6) 601 (30.9) b0.001Black or African American 786 (25.0) 171 (8.8)White 1575 (50.0) 1127 (58.0)Other 204 (6.5) 45 (2.3)
Body mass index, kg/m2 28.4 (24.2–33.6) 27.1 (23.3–32.2) b0.001Past medical history, n (%)
Hypertension 2394 (76.0) 1340 (68.9) b0.001Diabetes 1397 (44.3) 872 (44.9) 0.724Current or prior smoker 1219 (38.7) 682 (35.1) 0.004Hyperlipidemia 1529 (48.5) 742 (38.2) b0.001Coronary artery disease 1587 (50.4) 996 (51.2) 0.620Prior myocardial infarction 1030 (32.7) 696 (35.8) 0.056Prior PCI 553 (17.6) 323 (16.6) 0.290Prior CABG 634 (20.1) 352 (18.1) 0.076Peripheral arterial disease 369 (11.7) 182 (9.4) 0.009Cerebrovascular disease 432 (13.7) 201 (10.3) b0.001Chronic respiratory disease 618 (19.6) 288 (14.8) b0.001Cancer within 5 years 133 (4.2) 73 (3.8) 0.411Depression 301 (9.6) 153 (7.9) 0.040
Presenting features, n (%)Dyspnea with minimal activity 1371 (43.5) 742 (38.2) b0.001Orthopnea 2460 (78.2) 1491 (76.8) 0.230Pulmonary congestion 2622 (83.3) 1704 (87.6) b0.001S3 gallop 734 (23.3) 401 (20.6) 0.025Elevated JVP 1934 (61.5) 1005 (51.7) b0.001Peripheral edema 2464 (78.2) 1389 (71.4) b0.001Mitral valve regurgitation murmur 910 (28.9) 496 (25.5) 0.009Presenting vitals, median (IQR)Heart rate, per minute 80 (70–92) 84 (72–98) b0.001Respiratory rate, per minute 22 (20–24) 24 (21–26) b0.001Systolic blood pressure, mm Hg 123 (110–140) 122 (110–140) 0.241Diastolic blood pressure, mm Hg 74 (66–84) 75 (65–83) 0.073
Laboratory values at randomization, median (IQR)Hemoglobin, g/L 126 (113–139) 127 (113–140) 0.571Sodium, mmol/L 139 (137–141) 138 (135–141) b0.001Creatinine, umol/L 108 (88–141) 110 (89.1–141.4) 0.303BUN, mmol/L 8.2 (5.9–12.4) 9.3 (6.7–14.3) b0.001Troponin I, ng/mL 0.05 (0.03–0.10) 0.05 (0.03–0.10) 0.744Tropnin T, ng/mL 0.02 (0.01–0.04) 0.03 (0.01–0.05) 0.001BNP, pg/mL 1039 (597–1925) 1056 (632–2017) 0.224NT-proBNP, pg/mL 4548 (2178–9166) 4868 (2181–9841) 0.238Left ventricular ejection fraction, median (IQR), % 30 (20–38) 29 (20–36) 0.191
RegionAsia-Pacific 576 (49.4) 590 (50.6) b0.001Central Europe 189 (36.7) 326 (63.3)Western Europe 90 (39.3) 139 (60.7)Latin America 268 (77.9) 76 (22.1)North America 2027 (71.4) 813 (28.6)
Length of stay, median (IQR), nightsCritical care unit Excluded 3.0 (2.0–6.0) –
Step down unit 4.0 (2.0–6.0) 3.0 (1.0–6.0) b0.001Ward 4.0 (2.0–8.0) 4.0 (2.0–8.0) 0.864Total hospital 7.0 (4.0–10.0) 8.0 (5.0–12.0 b0.001
Abbreviations: BUN, blood urea nitrogen; CABG, coronary artery bypass grafting; IQR, interquartile range; JVP, jugular venous pressure; and PCI, percutaneous coronary intervention.
3S. van Diepen et al. / International Journal of Cardiology xxx (2014) xxx–xxx
significant difference in 30-day all-cause mortality between regions.All-cause readmission and all cause ADHF readmission at 30 daysamong CCU patients were highest among North American (19.7% and10.4%) and lowest among Central European (5.0% and 2.2%) patients(unadjusted-p b 0.001 across groups for all-cause and ADHFreadmissions). The unadjusted all-cause mortality at 7 days was 1.1%in North American, 0% in Latin American, 0.8% of Western European,2.7% of Asian-Pacific, and 1.2% of Central European patients (p =0.150 across groups). All-cause mortality between 31 and 180 dayswas highest in Latin American (20.3%) and lowest in Asian-Pacific(7.4%) study sites (unadjusted-p = 0.003 across groups).
To account for differences in patients, sites, countries and regions,multivariable adjustment was performed. In CCU patients, after
Please cite this article as: S. van Diepen, et al., Acute decompensated heartHF, Int J Cardiol (2014), http://dx.doi.org/10.1016/j.ijcard.2014.11.007
multivariable adjustment using GEE regression, taking study site withineach country as a nesting factor, nodifference in the primary outcomeof30-day all-cause mortality or readmission was observed between re-gions when compared with North America (Table 3). Similarly, therewere no differences in 30-day mortality or 31–180 day mortality.After adjustment, the 30-day all-cause and ADHF readmission riskswere lower in the Asia-Pacific and Central Europe regions comparedwith North America.
3.3. Critical care outcomes
Among patients hospitalizedwith ADHFwho survived 7 days, a CCUadmission was independently associated with a higher risk of 30-day
failure patients admitted to critical care units: Insights from ASCEND-

Table 2Post-randomization differences in pharmacotherapy, mechanical therapies, and procedures by region of patients admitted to a critical care unit.
Post-randomization treatment Asia-Pacificn = 590
Central Europen = 326
Western Europen = 139
Latin American = 76
North American = 813
p-Value
Diuretics 0–6 h, n (%)IV loop bolus 247 (41.9) 96 (29.5) 104 (74.8) 46 (60.5) 463 (57.0) b0.001IV loop infusion 54 (9.2) 3 (0.9) 0 0 5 (0.6) b0.001Oral loop 1 (0.2) 0 4 (2.9) 1 (1.3) 36 (4.4) b0.001All thiazide 22 (3.7) 2 (0.6) 1 (0.7) 0 19 (2.3) 0.011
Diuretics 6–24 h, n (%)IV loop bolus 420 (71.2) 265 (81.3) 126 (90.7) 61 (80.3) 667 (82.0) b0.001IV loop infusion 81 (13.7) 16 (4.9) 1 (0.7) 0 9 (1.1) b0.001Oral loop 1 (0.2) 0 5 (3.6) 1 (1.3) 43 (5.3) b0.001All thiazide 54 (0.2) 18 (5.5) 2 (1.4) 1 (1.3) 48 (5.9) 0.002
Heart failure medicines at discharge, n (%)β-Blockers 301 (51.0) 250 (76.7) 95 (68.4) 45 (59.2) 661 (81.3) b0.001ACE/ARB inhibitors 437 (74.1) 270 (82.8) 96 (69.1) 48 (63.2) 556 (68.4) b0.001Aldosterone antagonists 238 (40.3) 215 (66.0) 52 (37.4) 44 (57.9) 257 (31.6) b0.001Digitalis 271 (45.9) 129 (39.6) 34 (24.5) 22 (29.0) 225 (27.7) b0.001Hydralazine 17 (2.9) 1 (0.3) 0 9 (11.8) 132 (16.2) b0.001
Intravenous vasoactive medications, n (%)Inotropes 128 (21.7) 47 (14.4) 20 (14.4) 22 (29.0) 147 (18.1) 0.006Vasodilators 14 (2.4) 0 1 (0.7) 4 (5.3) 15 (1.9) 0.009Vasopressors 15 (2.5) 5 (1.5) 3 (2.2) 5 (6.6) 46 (5.7) 0.002
Mechanical therapies, n (%)Mechanical ventilation 67 (11.4) 7 (2.2) 4 (2.9) 8 (10.5) 58 (7.1) b0.001NIMV 42 (7.1) 6 (1.8) 4 (2.9) 2 (2.6) 81 (10.0) b0.001Intra-aortic balloon pump 3 (0.5) 0 0 0 15 (1.9) 0.009Renal dialysis 6 (1.0) 0 2 (1.4) 3 (4.0) 17 (2.1) 0.023Ultrafiltration 10 (1.7) 3 (0.9) 2 (1.4) 3 (4.0) 30 (3.7) 0.026
Invasive proceduresCoronary catheterization 34 (5.8) 13 (4.0) 21 (15.1) 10 (13.2) 160 (19.7) b0.001PCI 9 (1.5) 8 (2.5) 4 (2.9) 4 (5.3) 9 (1.1) 0.049Pacemaker 5 (0.9) 0 0 1 (1.3) 5 (0.6) 0.370CRT or ICD 12 (2.0) 3 (0.9) 2 (1.4) 5 (6.6) 53 (6.5) b0.001Non-cardiac surgery 2 (0.3) 0 0 1 (1.3) 11 (1.4) 0.050Any cardiovascular surgery 17 (2.9) 4 (1.2) 2 (1.4) 2 (2.6) 42 (5.2) 0.006CABG 8 (1.4) 1 (0.3) 1 (0.7) 1 (1.3) 21 (2.6) 0.058Heart transplant 1 (0.2) 0 0 0 2 (0.2) 0.863Left ventricular assist device 2 (0.3) 0 0 1 (1.3) 8 (1.0) 0.167
Non-invasive proceduresAny cardiac imaging 57 (9.7) 172 (52.8) 64 (46.0) 29 (38.2) 362 (44.5) b0.001Stress test 88 (14.9) 10 (3.1) 7 (5.0) 7 (9.2) 110 (13.5) b0.001
Length of stay, median (IQR), nightsCritical care unit 2.0 (1.0–3.0) 5.0 (3.0–9.0) 4.0 (2.0–7.0) 3.0 (2.0–6.0) 4.0 (3.0–7.0) b0.001Step down unit 2.0 (2.0–3.0) 3.0 (0.0–7.0) 6.0 (3.0–8.0) 1.0 (0.5–2.5) 4.0 (1.0–8.0) b0.001Ward 4.0 (2.0–7.0) 7.0 (4.0–12.0) 4.0 (3.0–8.5) 3.0 (2.0–7.0) 2.0 (0.5–6.0) b0.001Total hospital 6.0 (5.0–10.0) 10.0 (8.0–15.0) 9.0 (6.0–12.0) 8.0 (6.0–14.5) 7.0 (5.0–12.0) b0.001
Abbreviations: ACE, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; CABG, coronary artery bypass grafting; CRT, cardiac resynchronization therapy; ICD, im-plantable cardioverter defibrillator; IV, intravenous; NIMV, non-invasive mechanical ventilation; and PCI, percutaneous coronary intervention.
Fig. 1.Unadjusted clinical outcomes in critical care unit patient by region. There are significant international differences in the unadjusted 30-day primary composite outcome and 30 dayre-admission.
4 S. van Diepen et al. / International Journal of Cardiology xxx (2014) xxx–xxx
Please cite this article as: S. van Diepen, et al., Acute decompensated heart failure patients admitted to critical care units: Insights from ASCEND-HF, Int J Cardiol (2014), http://dx.doi.org/10.1016/j.ijcard.2014.11.007

Table 3Adjusted regional outcomes of patients with heart failure admitted to critical care units.
Outcome Region Adjusted OR (95% CI)a,b
All-cause 30-day mortality orreadmission
Asia-Pacific 0.64 (0.34–1.17)Central Europe 0.57 (0.31–1.03)Latin America 0.61 (0.11–3.25)Western Europe 0.63 (0.25–1.56)
30-day all-cause mortality Asia-Pacific 0.67 (0.29–1.54)Central Europe 0.82 (0.39–1.76)Western Europe 0.90 (0.19–4.14)Latin America 1.11 (0.29–4.34)
30-day all-cause readmission Asia-Pacific 0.45 (0.22–0.91)Central Europe 0.38 (0.16–0.86)Western Europe 0.57 (0.12–2.67)Latin America 0.47 (0.12–1.80)
30-day HF readmission Asia-Pacific 0.35 (0.13–0.98)Central Europe 0.28 (0.13–0.61)Western Europe 0.35 (0.06–1.93)Latin America 0.90 (0.23–3.44)
31 to 180-day death Asia-Pacific 0.71 (0.28–1.83)Central Europe 1.02 (0.35–2.97)Western Europe 0.33 (0.05–2.16)Latin America 2.14 (0.28–16.13)
a Compared to North American sites.b Adjusted outcomes of 30-day all-cause mortality or readmission, mortality, all-cause
readmission, ADHF readmission analyzed using a generalized estimating equation regres-sion adjusting for individual variables and taking sides as nesting factor adjusted31–180 day mortality analyzed using a Frailty Cox Proportional Hazards Model.
5S. van Diepen et al. / International Journal of Cardiology xxx (2014) xxx–xxx
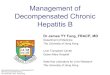
all-cause mortality or readmission (17.0% vs. 15.2%; OR 1.44; 95% CI,1.14–1.82; p = 0.002), and 31–180 day all-cause mortality (10.6% vs.8.1%; HR 1.37; 95% CI, 1.01–1.86; p = 0.0.043) compared with a wardadmission. The 30-day mortality was non-significantly higher (5.4% vs2.8%; OR 1.60; 95% CI, 0.97–2.64; p = 0.068) in patients admitted to aCCU. A KaplanMeier curve for cumulative 180 daymortality is providedin Fig. 2. There were no global regional differences in the prognosis as-sociated with a CCU versus a ward admission (interaction-p = 0.696for 30-day primary outcome).
Fig. 2. Kaplan Meier curve for cumulative incidence of all-cause-deaths in heart failure patientsmortality was higher in hospitalized critical care unit patients than ward patients.
Please cite this article as: S. van Diepen, et al., Acute decompensated heartHF, Int J Cardiol (2014), http://dx.doi.org/10.1016/j.ijcard.2014.11.007
4. Discussion
In this analysis of the largest international dataset to date of patientshospitalizedwith ADHF, several novel findings emerge. First, worldwidedifferences in the in-hospital pharmacologic treatment and the applica-tion of mechanical technologies and cardiac procedures were observedamong ADHF patients admitted to CCUs. Second, there were no signifi-cant differences in the 30-day incidence of all cause death or hospital re-admission, or death alone; however, 30-day all-cause and ADHFreadmission rates were highest in North American study centers.Third, a CCU admission for ADHFwas independently associatedwith ad-verse short and intermediate term outcomes compared with patientsadmitted to a hospital ward with ADHF.
Contemporary analyses have reported patterns of heart failure careand adherence to evidence basedmedical therapy; however these anal-yses have been largely limited to national and continental registries andsurveys of non-critical patients hospitalized with heart failure. TheEuroHeart Failure Survey Programme has reported heterogeneity in na-tional β-blocker and angiotensin converting enzyme inhibitor (ACE)prescription rates as well as variations in the use of cardiac imagingand coronary angiography among European patients hospitalized withADHF [22,23]. In the United States, inter-hospital differences in the ad-herence to guidelines recommended treatments, aswell as the associat-ed outcomes, have been reported [24–26]. On an international scale,considerably less is known about ADHF practice patterns. The ASCENDHF trial has described global differences in care quality, but these met-ricswere limited to the appropriate use of medications, implantable de-fibrillators, and blood pressure control at the time of hospital dischargeand did not describe the in-hospital treatment variations in CCU ADHFpatients [27]. The EVEREST (efficacy of vasopressin antagonism inheart failure: outcome study with tolvaptan) has described differencesin ADHF pharmacotherapy at the time hospital discharge between theAmericas and Europe, while the URGENT Dyspnea study described dif-ferences in the emergency department treatment of ADHF betweenthe United States and Europe [28,29].
The present study builds on previous research by describing regionaldifferences in international in-hospital treatment practice patterns in a
with and without a critical care admission. The cumulative incidence of 180 day all-cause
failure patients admitted to critical care units: Insights from ASCEND-

6 S. van Diepen et al. / International Journal of Cardiology xxx (2014) xxx–xxx
higher risk subset of ADHF patients admitted to CCUs.We observed sig-nificant variations in the in-hospital early diuresis regimens, heart fail-ure pharmacotherapies, intravenous vasoactive therapies, mechanicaltechnologies, cardiac procedures, and cardiac imaging across study re-gions. In addition, the utilization of evidence based heart failure thera-pies at the time of discharge also differed across study regions. Giventhat the lack of adherence to heart failure pharmacotherapy at thetime of hospital discharge has been reported to be significantly associat-ed with reduced patient mortality and readmission, this represents op-portunities for quality improvement [24,25]. We recognize, however,that individual patient indications and contraindications to therapieswere not captured in this study and the findings can only serve tobroadly inform regional areas for improved adherence to clinicalpractice guidelines such as early intravenous diuresis, cardiacresynchronization therapy, and discharge heart failure pharmacothera-py [30–33]. This analysis may also help identify international regionsthat may overuse therapies and technologies whose benefit is lessclear or potentially harmful such as diuretic infusions, intra-aortic bal-loon pumps, inotropic support, and ultrafiltration with cardio-renalsyndrome [34–37]. Finally, in an era of constrained health care funding,a nearly five-fold regional difference in coronary angiography and stresstesting rateswith relatively low overall percutaneous coronary revascu-larization or cardiac surgery rates was observed. These findings poten-tially provide opportunities for resource consolidation and cost savings.
Despite wide variations in treatment practices, no regional interna-tional differences in 30-day all cause death or readmission, or deathalone were observed. This finding differs from an analysis reportingthat compared to North America, South American heart failure patientshad a highermortality and eastern European patients had lower cardio-vascular death and ADHF hospitalization rates at 1 year [28]. This study,however, included all patients hospitalized with ADHF and was unableto adjust for differences in-hospital treatment and measures of patientacuity. We hypothesize that that the lack of an observed differences inshort term outcomes despite wide practice variation may suggest thatpatient variables may be the principal determinant of prognosis in thishigher risk subset of ADHF patients. We did, however, observe a signif-icant global region difference in 30-day all cause and ADHF readmissionwhere North American patients had the highest readmission risk. TheEplerenone Post-Acute Myocardial Infarction Heart Failure Efficacyand Survival Study (EPHESUS) reported thatNorthAmerican, comparedto Europeanpatients, had a significantly higher risk of all cause readmis-sion over 16 months and the EuroHeart Failure Survey Programme re-ported 12 week readmission rates that varied between 3 and 54% [23,38]. A previous ASCEND publication reported that international 30-day readmissions varied between 2.5% and 15% and were inversely as-sociated with hospital length of stay [39]. This analysis extends ourknowledge of readmission disparities to critical care ADHF patients.
Finally, this study furthers our understanding of how a CCU admis-sion serves as an adverse prognostic marker in new patient population.Though critical care admissions are known to portend reduced survivalin medical and surgical patients, previous studies examining ADHF pa-tients with a CCU versus ward admission are limited by unadjusteddata. This is the first international study to report that CCU admissionshave a significantly higher short and intermediate term risk ofmortalityand readmission compared to patients admitted to a hospital wardwithADHF [9,10,12,40,41]. This finding presents future opportunities to im-prove the risk stratification and prognostic assessment of patients hos-pitalized with ADHF through the incorporation of level of care oracuity measures.
4.1. Limitations
The limitations of this analysis merit consideration. First, theASCEND-HF trial excluded patients with hemodynamic instability atthe time of randomization. Second, uniform international definitionsof coronary care and intensive care unit are lacking and some
Please cite this article as: S. van Diepen, et al., Acute decompensated heartHF, Int J Cardiol (2014), http://dx.doi.org/10.1016/j.ijcard.2014.11.007
institutions have amalgamated units; thus, all CCU admissions werecombined and more detailed unit-based analyses were not possible.However, combining coronary and medical intensive care unit patientsadmitted with ADHF has been previously reported and may provide abroader view of critical care ADHF management [42]. Third, therewere noCCUadmission criteria in this trial and admission unit decisionswere at the discretion of the local physicians, hence the use of propen-sity matching, and only including sites that had patients in both wardand CCU.
5. Conclusions
Among patients with ADHF admitted to CCUs, we observed signifi-cant international variations in the in-hospital pharmacologic treat-ment, the application of mechanical technologies and the use ofcardiac procedures. No differences in regional 30 day short or interme-diate term mortality rates were observed; however, North Americansites had higher 30-day readmission rates. A critical care admission forADHFwas also an independent negative prognostic marker. These find-ings may help to broadly inform regional areas for improved adherenceto clinical practice guidelines and may improve the risk stratification ofpatients hospitalized with ADHF.
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.ijcard.2014.11.007.
Conflicts of interest
SVD, MP, CMW, and JJVM, none to report. AFH: research grants:Bristol-Myers-Squibb, Janssen, Novartis, and Portola Pharmaceuticals;Honoraria: Amgen, Bristol-Myers-Squibb, Janssen, and Novartis. PWA:advisor/consultant: Eli Lilly; research grants: Boehringer IngelheimPharmaceuticals, Inc. and Sanofi; unrestricted educational grants:AstraZeneca Pharmaceuticals LP and Eli Lilly. ZJE: advisory board:Novartis and Cytokinetics; honoraria: Janssen. RMC's are publicallyavailable at https://www.dcri.org/about-us/conflict-of-interest/Califf-COI_2-3-2014.pdf. RCS: consulting fees/honoraria: Thoratec andHeartWare. CMO: consulting fees/honoraria: Amgen and ActelionPharmaceuticals Ltd.; ownership/partnership/principal: Biscardia, LLC;research grants: Otsuka, Astellas, Gilead, BG Medicine, Roche Diagnos-tics, Critical Diagnostics, and ResMed. JAE: consulting fees/honoraria:Servier, Abbott Labs, Pfizer, Astra-Zeneca, and Bristol-Myers Squibb; re-search/research grants: Amgen. ASCEND-HF was supported by Scios.
Author contributions
SVD and JAE: conception and design, analysis and interpretation,drafting of the article, and final approval of the manuscript; MP andCMW: analysis and interpretation, drafting of the article, and final ap-proval; AFH: conception and design, acquisition of data, revisions forcritically important intellectual content, and final approval; and PWA,JJVM, ZJE, RMC, RCS, and COC: acquisition and interpretation of data, re-visions for critically important intellectual content, and final approval.
Acknowledgment of grant support
ASCEND-HF was supported by Scios.
References
[1] J.A. Ezekowitz, P. Kaul, J.A. Bakal, H. Quan, F.A. McAlister, Trends in heart failure care:has the incident diagnosis of heart failure shifted from the hospital to the emergen-cy department and outpatient clinics? Eur. J. Heart Fail. 13 (2011) 142–147.
[2] J. Fang, G.A. Mensah, J.B. Croft, N.L. Keenan, Heart failure-related hospitalization inthe U.S., 1979 to 2004, J. Am. Coll. Cardiol. 52 (2008) 428–434.
[3] J.N. Katz, A.T. Turer, R.C. Becker, Cardiology and the critical care crisis: a perspective,J. Am. Coll. Cardiol. 49 (2007) 1279–1282.
[4] K.F. Adams Jr., G.C. Fonarow, C.L. Emerman, et al., Characteristics and outcomes ofpatients hospitalized for heart failure in the United States: rationale, design, and
failure patients admitted to critical care units: Insights from ASCEND-

7S. van Diepen et al. / International Journal of Cardiology xxx (2014) xxx–xxx
preliminary observations from the first 100,000 cases in the Acute DecompensatedHeart Failure National Registry (ADHERE), Am. Heart J. 149 (2005) 209–216.
[5] C.W. Yancy, M. Lopatin, L.W. Stevenson, T. De Marco, G.C. Fonarow, Clinical presen-tation, management, and in-hospital outcomes of patients admitted with acute de-compensated heart failure with preserved systolic function: a report from the AcuteDecompensated Heart Failure National Registry (ADHERE) Database, J. Am. Coll.Cardiol. 47 (2006) 76–84.
[6] E.D. Nicol, B. Fittall, M. Roughton, J.G.F. Cleland, H. Dargie, M.R. Cowie, NHS heartfailure survey: a survey of acute heart failure admissions in England, Wales andNorthern Ireland, Heart 94 (2008) 172–177.
[7] M.S. Nieminen, D. Brutsaert, K. Dickstein, et al., EuroHeart Failure Survey II (EHFS II):a survey on hospitalized acute heart failure patients: description of population, Eur.Heart J. 27 (2006) 2725–2736.
[8] C.M. O'Connor, W.T. Abraham, N.M. Albert, et al., Predictors of mortality after dis-charge in patients hospitalized with heart failure: an analysis from the OrganizedProgram to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure(OPTIMIZE-HF), Am. Heart J. 156 (2008) 662–673.
[9] H. Wunsch, C. Guerra, A.E. Barnato, D.C. Angus, G. Li, W.T. Linde-Zwirble, Three-yearoutcomes for medicare beneficiaries who survive intensive care, JAMA 303 (2010)849–856.
[10] J.M. Eddleston, P. White, E. Guthrie, Survival, morbidity, and quality of life after dis-charge from intensive care, Crit. Care Med. 28 (2000) 2293–2299.
[11] S.A. Nasraway, G.J. Button, W.M. Rand, T. Hudson-Jinks, M. Gustafson, Survivors ofcatastrophic illness: outcome after direct transfer from intensive care to extendedcare facilities, Crit. Care Med. 28 (2000) 19–25.
[12] D. Somme, J.-M. Maillet, M. Gisselbrecht, A. Novara, C. Ract, J.-Y. Fagon, Critically illold and the oldest-old patients in intensive care: short- and long-term outcomes, In-tensive Care Med. 29 (2003) 2137–2143.
[13] A.F. Hernandez, C.M. O'Connor, R.C. Starling, et al., Rationale and design of the AcuteStudy of Clinical Effectiveness of Nesiritide in Decompensated Heart Failure Trial(ASCEND-HF), Am. Heart J. 157 (2009) 271–277.
[14] C.M. O'Connor, R.C. Starling, A.F. Hernandez, et al., Effect of nesiritide in patientswith acute decompensated heart failure, N. Engl. J. Med. 365 (2011) 32–43.
[15] R.J. Mentz, A.F. Hernandez, A. Stebbins, et al., Predictors of early dyspnoea relief inacute heart failure and the association with 30-day outcomes: findings fromASCEND-HF, Eur. J. Heart Fail. 15 (2013) 456–464.
[16] K. Liang, S. Zeger, Longitudinal data analysis using generalized linear models,Biometrika 73 (1986) 13–22.
[17] W. Pan, Akaike's information criterion in generalized estimating equations, Biomet-rics 57 (2001) 120–125.
[18] P. Allison, Survival Analysis Using SAS: A Practical Guide, SAS press, 2010.[19] P.C. Austin, Balance diagnostics for comparing the distribution of baseline covariates
between treatment groups in propensity-score matched samples, Stat. Med. 28(2009) 3083–3107.
[20] S.R. Cole, M.A. Hernan, Adjusted survival curves with inverse probability weights,Comput. Methods Prog. Biomed. 75 (2004) 45–49.
[21] R.C. Starling, A.F. Hernandez, P.W. Armstrong, et al., Clinical outcomes at 180 days inthe ASCEND-HF Trial: double-blind, placebo-controlled, multicenter acute study ofclinical effectiveness of nesiritide in subjects with decompensated heart failure, J.Card. Fail. 17 (2011) 971.
[22] M. Komajda, F. Follath, K. Swedberg, et al., The EuroHeart Failure Survey programme—a survey on the quality of care among patients with heart failure in Europe. Part 2:treatment, Eur. Heart J. 24 (2003) 464–474.
[23] J.G.F. Cleland, K. Swedberg, F. Follath, et al., The EuroHeart Failure Survey pro-gramme—a survey on the quality of care among patients with heart failure inEurope, Eur. Heart J. 24 (2003) 442–463.
[24] G.C. Fonarow, W.T. Abraham, N.M. Albert, et al., Association between performancemeasures and clinical outcomes for patients hospitalized with heart failure, JAMA297 (2007) 61–70.
Please cite this article as: S. van Diepen, et al., Acute decompensated heartHF, Int J Cardiol (2014), http://dx.doi.org/10.1016/j.ijcard.2014.11.007
[25] G.C. Fonarow, W.T. Abraham, N.M. Albert, et al., Carvedilol use at discharge in pa-tients hospitalized for heart failure is associated with improved survival: an analysisfrom Organized Program to Initiate Lifesaving Treatment in Hospitalized Patientswith Heart Failure (OPTIMIZE-HF), Am. Heart J. 153 (82) (2007) e1–e11.
[26] G.C. Fonarow, C.W. Yancy, J. Heywood, Adherence to heart failure quality-of-care in-dicators in US hospitals: analysis of the adhere registry, Arch. Intern. Med. 165(2005) 1469–1477.
[27] J.G. Howlett, J.A. Ezekowitz, M. Podder, et al., Global variation in quality of careamong patients hospitalized with acute heart failure in an international trial: find-ings from the acute study clinical effectiveness of nesiritide in decompensatedheart failure trial (ASCEND-HF), Circ. Cardiovasc. Qual. Outcomes 6 (2013) 534–542.
[28] J.E.A. Blair, F. Zannad, M.A. Konstam, et al., Continental differences in clinical charac-teristics, management, and outcomes in patients hospitalized with worsening heartfailure results from the EVEREST (Efficacy of Vasopressin Antagonism in Heart Fail-ure: Outcome Study with Tolvaptan) program, J. Am. Coll. Cardiol. 52 (2008)1640–1648.
[29] S.P. Collins, P.S. Pang, C.J. Lindsell, et al., International variations in the clinical, diag-nostic, and treatment characteristics of emergency department patients with acuteheart failure syndromes, Eur. J. Heart Fail. 12 (2010) 1253–1260.
[30] R.O. Bonow, S. Bennett, D.E. Casey, et al., ACC/AHA clinical performancemeasures foradults with chronic heart failure, Circulation 112 (2005) 1853–1887.
[31] R.S. McKelvie, G.W.Moe, J.A. Ezekowitz, et al., The 2012 Canadian Cardiovascular So-ciety heart failure management guidelines update: focus on acute and chronic heartfailure, Can. J. Cardiol. 29 (2013) 168–181.
[32] J.J.V. McMurray, S. Adamopoulos, S.D. Anker, et al., ESC guidelines for the diagnosisand treatment of acute and chronic heart failure 2012: The Task Force for the Diag-nosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Soci-ety of Cardiology, Eur. Heart J. 33 (2012) 1787–1847.
[33] C.W. Yancy, M. Jessup, B. Bozkurt, et al., 2013 ACCF/AHA guideline for the manage-ment of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, Circulation 128(2013) e240–e327.
[34] G.M. Felker, K.L. Lee, D.A. Bull, et al., Diuretic strategies in patients with acute de-compensated heart failure, N. Engl. J. Med. 364 (2011) 797–805.
[35] H. Thiele, U. Zeymer, F.-J. Neumann, et al., Intraaortic balloon support for myocardialinfarction with cardiogenic shock, N. Engl. J. Med. 367 (2012) 1287–1296.
[36] M. Packer, W. Colucci, L. Fisher, et al., Effect of levosimendan on the short-term clin-ical course of patients with acutely decompensated heart failure, J. Am. Coll. Cardiol.Heart Fail. 1 (2013) 103–111.
[37] B.A. Bart, S.R. Goldsmith, K.L. Lee, et al., Ultrafiltration in decompensated heart fail-ure with cardiorenal syndrome, N. Engl. J. Med. 367 (2012) 2296–2304.
[38] B. Pitt, F. Zannad, M. Gheorghiade, et al., Transatlantic similarities and differences inmajor natural history endpoints of heart failure after acute myocardial infarction: apropensity-matched study of the EPHESUS trial, Int. J. Cardiol. 143 (2010) 309–316.
[39] Z.J. Eapen, S.D. Reed, Y. Li, et al., Do countries or hospitals with longer hospital staysfor acute heart failure have lower readmission rates?: findings from ASCEND-HF,Circ. Heart Fail. 6 (2013) 727–732.
[40] O. Chioncel, A.P. Ambrosy, D. Filipescu, et al., Patterns of intensive care unit admis-sions in patients hospitalized for heart failure: insights from the RO-AHFS registry,J. Cardiovasc. Med. (2014), http://dx.doi.org/10.2459/JCM.
[41] F. Follath, M.B. Yilmaz, Delgado, et al., Clinical presentation, management and out-comes in the acute heart failure global survey of standard treatment, IntensiveCare Med. 37 (2011) 619–626.
[42] K.C. Safavi, K. Dharmarajan, N. Kim, et al., Variation exists in rates of admission to in-tensive care units for heart failure patients across hospitals in the United States, Cir-culation 127 (2013) 923–929.
failure patients admitted to critical care units: Insights from ASCEND-