Embed Size (px)
Citation preview
Tiirki,l, Neiirosiirgery 11: 111 - 116, 2001 Yiiceer: Aciite Epiriiiml Aliscess oL tlie CerI'irnI Spiiie
Acute Epidural Abscess of the Cervical SpineCaused By Staphylococcus Aureus: Report Of Two Cases
Staphylococcus A ureus EtkenH
Iki Olgu
Akut ServikalSunumu
Epidural Abse:
NURULLAH YÜCEER, M. NURI ARDA
Dokuz Eylül University School of Medicine, Department of Neurosurgery (NY) (M NA), Izmir
Received : 27.12.1999 <::> Accepted : 25.5.2000
Abstract: This report describes two cases of spinal epiduralabscess. At presentation, both patients complained ofcervical pain and weakness in the arms and legs. Theirneurological examinations revealed quadriplegia andtetraparesis, respectively. In both cases, the definitivediagnosis was established preoperatively with magneticresonance imaging. Surgical treatment in both patientsinvolved laminectomy through a posterior approach forabscess drainage. In both cases, the causative microorganism\Vas Staphylococcus aureus. The patients received an S-weekcourse of intravenous vancomycin treatment, and both werefollowed postoperatively with monthly magnetic resonanceimaging scans. Their neurological examinations werenormal at 6 months postsurgery.
Key words: Spinal epidural abscess, infection, incidence,magnetic resonance imaging, therapy
INTRODUCTION
Spinal epidural abscess (SEA) is very rare,occmring at a reported frequency of 0.2-1.96per 10,000hospital admissions (2,9,10,16,17,19,20,22).Despite theprogress in imaging, surgical techniques, andantimicrobial therapy, this lesion is stili associated withhigh morbidity and mortality. The mortality ratesreported in recent series range from 18% to 31%(2,10,12,13). On the positive side, however, the
Özet: Bu çalisma, spinal epidural abseli iki olguyuiçermektedir. Basvuni aninda, iki olguda boyun agrisi ilekol ve bacaklarinda kuvvetsizlikten sikayetçiydi.Nörolojik muayeneleri sirasiyla, quadripleji vetetrapareziyi gösterdi. Her iki olguda da ameliyat öncesikesin tani, manyetik rezonans görüntüleme yardimiylayapildi. Her iki hastanin da cerrahi tedavisinde, abscdrenaj! için posterior yaklasimla laminektomi uygulandi.Iki olguda da etken mikroorganizma Staphylococcusaureus'du. Hastalar S-hafta süreyle intravenözvancomyein tedavisi aldi, ve ameliyat sonrasi aylik olarakmanyetik rezonans görüntüleme incelemeleriyle takipedildiler. Cerrahi tedaviden 6 ay sonra yapilan nörolojikmuayeneleri normaldi.
Anahtar kelimeler: Enfeksiyon, insidens, manyetikrezonans görüntüleme, spinal epidural abse, tedavi
advances in diagnostic tools, surgery and therapy haveled to better prognosis for SEA patients.
Studies have shown that SEA is associated with
a number of predisposing factors and conditions,including diabetes meJlitus, intraven'ous drug use,steroid injection for sciatica, paraspinal abscess,ceJlulitis, malignancy, endocarditis, pneumonia,discography procedure, trauma, duodenolumbarfistula, chronic steroid use, and human
111

Tiirkisli Neurosiirgery 11: 111 - 116, 2001
immunodeficiencyvirus (HM, and the lesion mayaisoarise as a surgical complication (3,4,8,10,11,13,15,16,20,22,24).
In this report, we deseribe two cases of cervicalepidural abscess associate d with paraspinal abscess.In both instances, the causal organism wasStaphylococcus aureus, and both patients presentedwith acute tetraparesis. The important pointshighlighted by these cases are as follows: (1) Uppercervical epidural abscess is very rare, and treatment ofaffected patients who present with acut~ tetraparesisor quadriplegia is always complicated, even inindividuals with lower cervical abscess; (2) Magneticresonance imaging (MRI) is the best tool for diagnosingSEA; (3) treatment should involve immediate surgicaldecompression and abscess drainage, combined withappropriate antibiotic therapy. We successfully treatedboth our patients with earlyand uncomplicatedsurgical abscess drainage, in addition to antimicrobialtherapy.
CASE REPORTS
CASE 1.
A 72-year-old male presented with the complaintsof neck pain and weakness in all four limbs that hadstarted 20 days earlier. His medical history wasunremarkable. On physical examination, the patientexhibited respiratory distress and urinary dysfunction.On admission, a neurological examination revealedquadriplegia with no deep tendon reflexes but positiveBabinski reflex bilaterally. Laboratory tests revealedleukocytosis (13,OOO/mm3) and elevated erythrocytesedimentation rate (ESR) (110 mm/hr). The patient alsohad an intermittent fever, averaging 38.5UC.The patientwas tested positive for anti-HIV antibodies. Aposteroanterior lung x-ray demonstrated bilateralpneumonic infiltration. Cervical x-rays showed basilarimpression, atlantooccipital fusion and spondylosis.Cervical computerized tomography (CT)demonstrated a lesion compressing the anterior aspectof the cervical spinal cord at CL-C3. MRI revealed ahypointense parapharyngeal mass and a hypointenselesion at CL-C3 (Figure 1).
The preoperative diagnosis was acute epiduralabscess of the upper cervical spine. Emergency surgerywas planned. The procedure involved a right C2-C3hemipartial laminectomy through a posterior cervicalapproach, and was done with the patient in proneposition. Upon exposing the site of interest, we founda purulent collection extending from CL to C3 alongthe anterior margin of the spinal epidural space. Thepurulent material was not enclosed in a capsule, but
112
Yiiceer: Aciile Epidiiml Absc!!ss of Ilie CalJiml SpiiiL'
Figure 1: A Tl-weighted sagittal MR image captured afterintravenous gadolinium injection shows anepidural abscess located adjacent to the anterioraspect of the spinal cord and extending from CLto C3. Note the marked compressian of theanterior spinal cord at this site, as well as thepresence of a prevertebral abscess.
appeared to have accumulated freely in the epiduralspace. There was no dural tear, nor any evidence ofcerebrospinal fluid leakage.
We took a swab of the material and culture iso
lated S. aureus. Starting immediately postoperatively,we administered an 8-week course of intravenous
vancomycin at a rate of 2 g/ day (4 x 500 mg infusionsdaily). The patienf s quadriplegia began to resolve soo naf ter the surgery. On completing the full course of antimicrobial therapy, his ESR was 28 mm/hr. CervicalMR! at 2 months postsurgery revealed that the lesionsite was gradually returning to normal (Figure 2A,2B).The patient was discharged af ter 60 days of hospitalization with persistent quadriparesis (right side 3/5;left side 2/5), but he was free of cervical pain. Threemonths af ter discharge, the muscle power in all hislimbs W)lS graded 4/5. At 6 months postsurgery, hisneurological examination was normal.
CASE 2:
A 60-year-old woman presented with thecomplaints of neck pain and left brachialgia of 15 daysduration. She also had an upper respiratory tractinfection. Her medical history included 5 years of spinaland lower extremity pain, which was managed wellwith antiinf1ammatory and analgesic agents. A
Tiirkish Neiirosiirgery 11: 111 - 116, 2001 Yiiceer: ACi/le Epidiiral Abscess vf Ihe Cai>ica! Spiiie
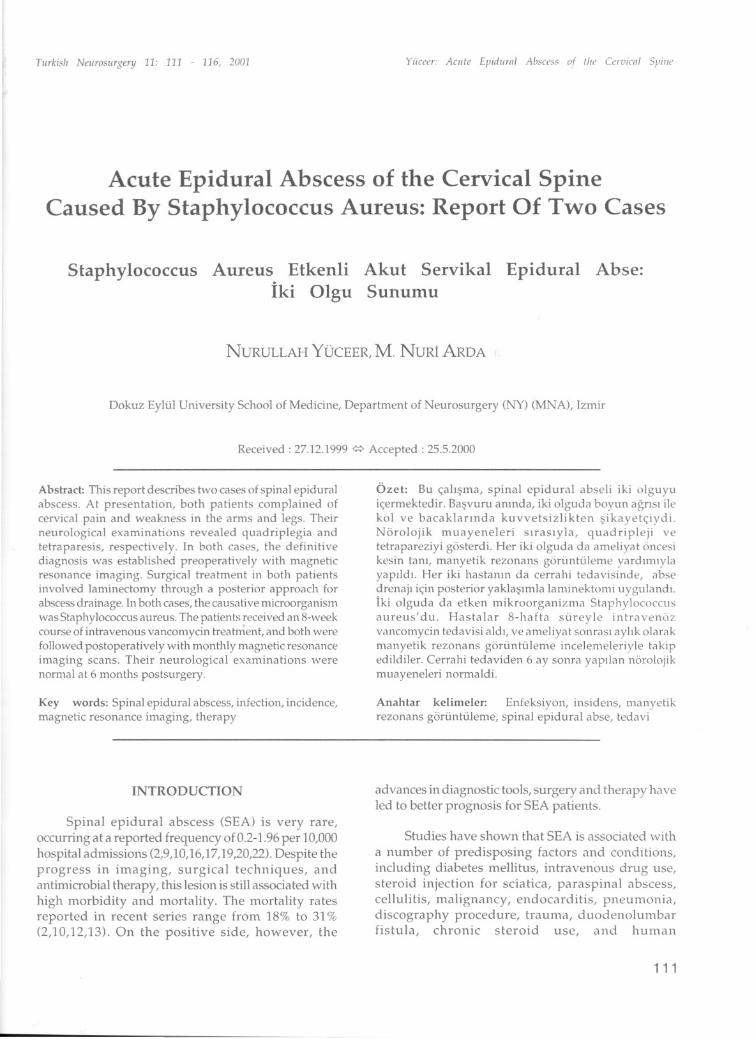
Figure 2: A and B. Gadolinium-enhanced Tl-weighted sagittal MR images of the lesion in Figure 1 at 2months after the operation show that the patienfs SEA had significantly decreased in size.
neurological examination revealed weakness of botharms (grade 3/5 muscle power) and both legs (grade0/5 muscle power). Laboratory findings showedleukocytosis (17,000/mm3) and elevated ESR (170mm/hr). The patient also had an intermittent fever,averaging 39.0°C. Plain radiographs and cervical CTshowed spondylosis in the cervical spine. When thepatient deteriorated significantly within hours of ourinitial assessment, we ordered immediate spinal MR!.Gadolinium-enhanced images revealed an SEAassociated with a prevertebral abscess at C6-C7(Figure3A,3B).
We carried out emergency surgery through aposterior approach. After performing a left C6-C7hemipartial laminectomy, we evacuated 10 ml ofpurulent material from the epidural space. Thepatient' s postoperative course was uneventful. Cultureof the material identified S. aureus. We administered
intravenous vancomycin at a dose of 2 g/ day (4 x 500mg infusions daily) for 8 weeks. After the antimicrobialtherapy, the patient's ESR was 22 mm/hr. As followup to the antibiotic treatment, she was referred forinpatient rehabilitabon. Three months after the
operation, MR! showed that the pathologic findingswere resolving (Figure 4A,4B).Over the next 6 months,the patient made a full recovery from her initialcomplete paraplegia.
DISCUSSION
Various organisms are known to cause SEA(6,7,12).The most com mon of these are streptococcusspecies and S. aureus, which was isolated from bothour cases (7,16,20,22,23,24,25).Many factors are knownto influence outcome in patients who develop thislesion, including the severity of acute or chronic clinicalsigns and symptoms, the location and extent of theabscess, the degree of spinal cord compression, patientage and medical condition, the surgical or medicaltreatment applied, and surgical findings of pus versusgranulation tissue. Of these, the most importantelements are clinical presentation and the surgical andmedical therapy that is administered.
Clinical signs and symptoms of SEA can appearwithin days or weeks of the formation of an abscessfocus in the epidural space. Some SEA patientsdeteriorate rapidIy, within a matter of hours or days,
113
Tiirkish Neuros/irgery 11: 111 - 116, 2001 Yiieeer: ACIlif Epidiiral A/Jsecs, of ilic Cerl'icnl Sl'iiic
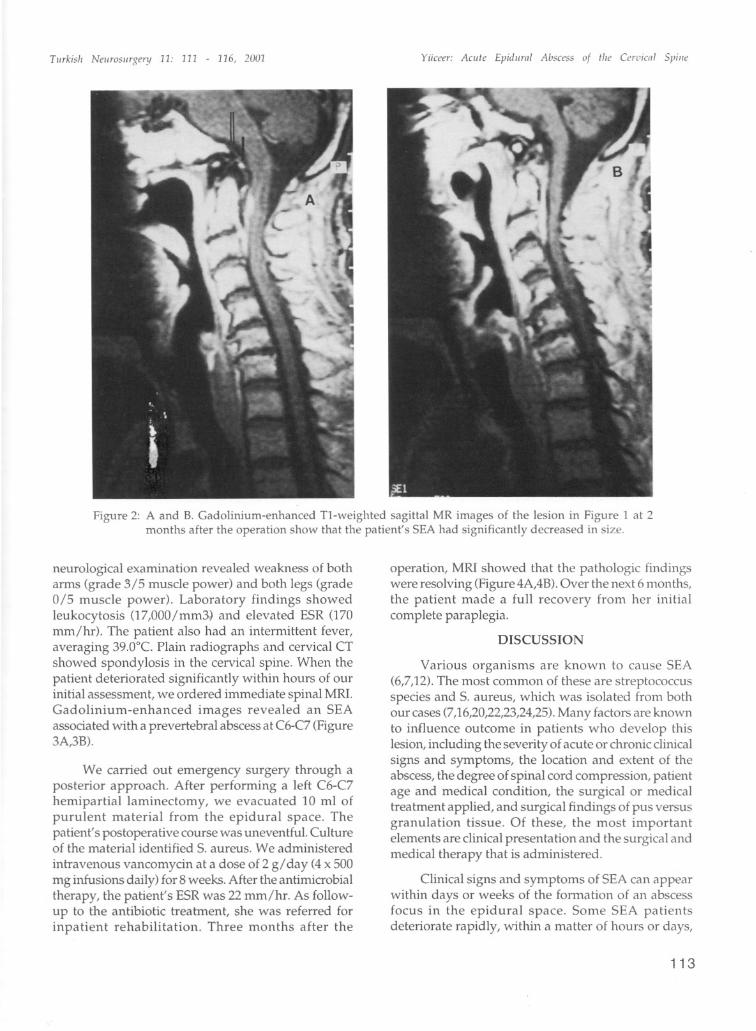
Figure 3: A and B.Contrast-enhanced Tl-weighted sagitta! MR iinages demonstrate an epidura! abscess at C6-7.
as our cases demonstrated. The typical presentingproblems are pain localized near the site of infectionand intermittent fever. Involvement of adjacent nerveroots may produce radicular pain. When an abscesscompresses the spinal cord or causes cauda equina,the patient exhibits sensory and motor deficits distalto the affected site, as well as impaired sphinctercontrol. Our patients exhibited most of these problems.The compression effect of the abscess may impact oneor more vertebral segments.
it is extremely unusual to find a spinal abscess inthe upper cervical region 00,13,25). Interestingly, therehave been rare findings of infection extending the entirelength of the spinal canal from the sacral to the uppercervical levels (25). Cmling and coJleagues (5)described onlyone patient with uppercervical epiduralabscess in a total of 29 cases of SEA. it is significant tonote that both cases we deseribe in this report presentedto our elinic within the past year. The patients hadquadriplegia and tetraparesis, respectively, and theirSEAs extended from CL to C3 and from C6 to C7,
respectively.
Regarding diagnosis, spinal x-ray films areindicated in the work-up of these cases, but there are
114
usuaiiy no abnormal findings unless the patient has aparavertebral abscess or adjacent osteomyelitic lesions.CT and MRI are both valuable tools for evaIuatingparaspinal and epidural spinal abscesses. CT mayreveal intraspinal gas formation (4,14); however, MRlis superior for demonstrating the extent and degree ofepidural involvement and the compressiye effect onthe cord and roots 0,4,16,20,22). MRl is also better thanCT for differentiation between SEA and the lesions of
transverse myelitis and spinal cord infarction (lO). T1weighted MRI wiii demonstrate a hypo- or isointenseepidural mass. Vertebral osteomyelitic lesions arecharacterized by reduced signal intensity. T2-weightedMRI shows a high-intensity epidural mass that of tenenhances with gadoJinium injection. MR images ofepidural abscess may show a dense and homogeneousor a nonhomogeneous mass, and the re may be a thinmargin of enhancement at the periphery of the lesi on(l6,18,20,21,22). We diagnosed both of our SEA casesusingMRl.
The treatment indicated for SEA is surgicaldrainage combined with parenteral antibiotics. Inpatients with severe and progressive neurologicaldeficits, emergency drainage of the abscess should be
TI/rkis/i Neiirosl/rgay 11: 111 - 116, 2001 Yiicra: ACi/k Epidl/ml Absass of tli" ("r,'iCilI Spiii"
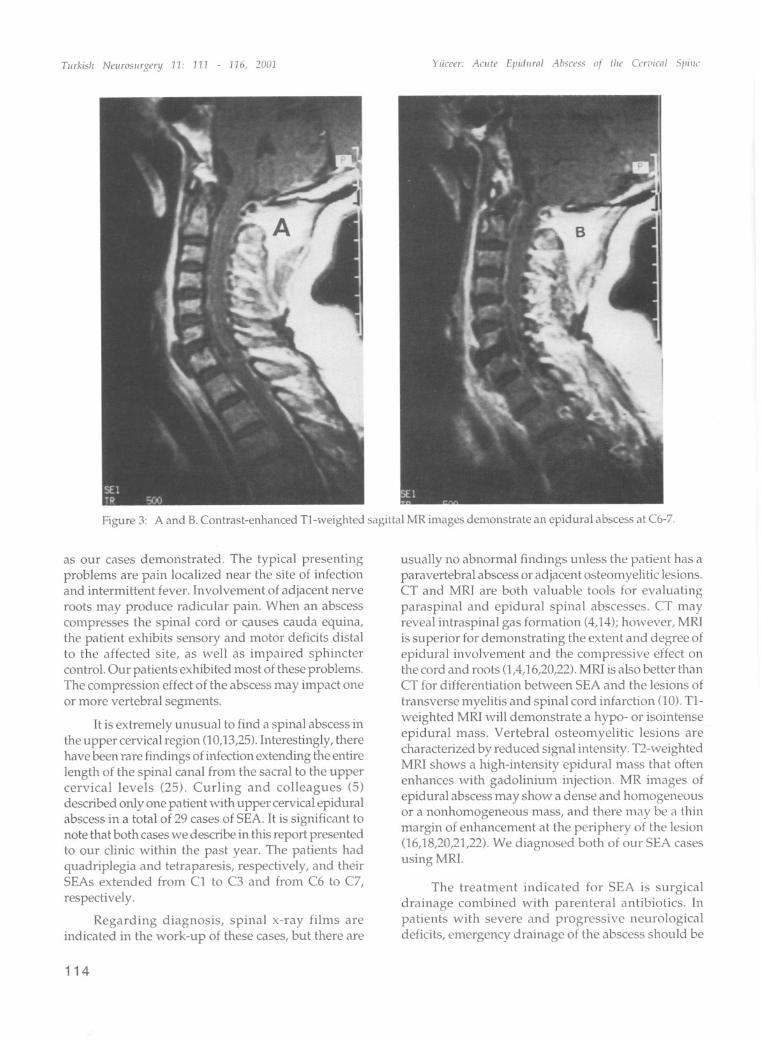
Figure 4: A and B. Contrast- enhanced Tl-weighted MR images of the lesion in Figure 3 at 3 months af terthe operation show that the patient's SEA had decreased in size.
performed via the most convenient and appropriateroute. This procedure confirms the diagnosis andsimuItaneously treats the problem, but care must betaken to prevent spinal instability. Our patientsexhibited acute and severe neurological deteriorationwithin 24 hours of presentation, and developed severequadriplegia and tetraparesis, respectively. Both of thepatients had been referred to our department fromanother clinic, and we immediately performed surgicaldrainage and initiated effective antibiotic therapy.
In both cases, neurological status began toimprove in the early postoperative stages. Weprescribed an extended course of antibiotic therapyaf ter surgery for penetration of the deep tissues andclear the infected site. Six months after their operations,both patients had normal neurologic examinations.Parenteral antibiotics should be administered as soon
as the diagnosis of spinal abscess is established. Theintravenous route for antibiotic therapy should be usedfor two months(5,10).
Medical treatment alone is indicated for selected
patients who have no neurological deficits or who arein very poor health. In these individuals, the high risk
of morbidity and mortality associated with surgery andanesthesia may outweigh the benefits of surgicaltreatment. Obviously, a correct microbiologicaldiagnosis is essential in these cases, and this can usuallybe achieved through blood culture or from a closedpercutaneous biopsy of a paravertebral abscess(17,20,22,25). However, it is important that aneurological team closely monitors high-riskindividuals who are treated conservatively because19% to 23% of these patients will exhibit neurologicaldeterioration despite appropriate antibiotic treatment(10,13,20,22). Tacconi et aL. (25) administered
conservative treatment to 2 high-risk individuals in agroup of 10 patients with SEA. One of the two was avery elderly ambulant patient whose neurologicaldeficits were stabilized. The other was a young patientwith few neurological signs for whom conservativetreatment was prescribed to circumvent extensivelaminectomy.
In conclusion, patients in whom SEA is suspectedrequire careful clinical evaiuatian, with detailedhistory-taking and thorough physical and neurologicexaminations. When this type of lesion is suspected
115
Tiirkisli Neiirosiirgery 11: 111 - 116, 2001
preoperatively, antibiotics should be started beforesurgery, as was done in our cases. Individuals withsevere neurologic deficits rarely improve, even whensurgical intervention takes place within 6-12 hrs of theonset of paralysis; however, a few series have indicatedthat there is potential for some recovery when a patientis treated within 36 hrs of paralysis (5,9). This risk ofpermanent deficit underlines the need for earlier ratherthan later surgical decompression, whet1ier or not thedisease progression is acute. it is essential thatappropriate antibiotic therapy should be continued for8 weeks af ter surgery in order to fully eradicate thedeep focus of infection. The patients in this report wereoperated on within 24 hrs of the on set of quadriplegiaand tetraparesis and postoperative antibiotic treatmentwas administered for 8 weeks. Both showed gradualimprovement over a 6-month period.
Correspondence: M. Nuri ArdaDepartment of Neurosurgery,Dokuz Eylül University School ofMedicine,InciraHi, izmir,TR-35340 TurkeyTel: + 90 (232) 259 5959Fax: + 90 (232) 278 8802
REFERENCES
1. Angtuaco EL,McConnell JR, Chadduck WM, FlaniganS: MR imaging of spinal epidural sepsis. AJR 149:12491253,1987
2. Baker AS, Ojemann RG, Swartz MN, Richardson EP:Spinal epidural abscess. N Engl J Med 293:463-468,1975
3. Chan ST, Leung S: Spinal epidural abscess followingsteroid injection for sciatica: Case report. Spine 14:106108, 1989
4. Chen JY,Chen Wl, Huang TJ, Shih CH: Spinal epiduralabscess complicating cervical spine fracture withhypopharyngeal perforation. A case report. Spine17:971-974,1992
5. Curling 00 Jr, Gower DJ, McWhorter JM: Changingconcepts in spinal epidural abscess: A report of 29cases. Neurosurgery 27:185-192, 1990
6. Elian D, Hassin D, Tomer A, Bank H, Eisenstein Z:Spinal epidural abscess: an unusual complication ofbacterial endocarditis. Infection. 12:258-259, 1984
7. Hancock D: A study of 49 patients with acute spinalextradural abscess. Paraplegia 70:285-288, 1973
8. Harston PK: Spinal epidural abscess as a complicationof duodenolumbar fistula: A case report. Spine 17:593596,1992
Yiiceer: Aci/le Epidimil Abscess of Ilie Cer,'ica! Spiiie
9. Heusner AP: Nontuberculous spinal epidural infections.N Engl J Med 239:845-854, 1948
10. Hlavin MC, Kaminski Hl, Ross JS, Ganz E: Spinalepidural abscess: Aten-year perspective. Neurosurgery27:177-184, 1990
11. Junila J, Niinimaki T, Tervonen O: Epidural abscess afterlumbardiscography. A casereport. Spine 22:2191-2193,1997
12. Kaufmann DE,KaplanJG, Litmann N: Infectious agents inspinal epidural abscess. Neurology 1980;30:848-850,1980
13. Khanna RK,Malik GM, Rock JP, Rosenblum ML: Spinalepidural abscess: Evaluation of factors influencingoutcome. Neurosurgery 39:958-964, 1996
14. Kirzner H, Oh YK,Lee SH: Intraspinal air: A CT findingof epidural abscess. AJR 151:1217-1218, 1988
15. Korovessis P, Sidiropoulos P, Piperos G, Karagiannis A:Spinal epidural abscess complicated closed vertebralfracture. A case report and review of literature. Spine18:671-674,1993
16. Mackenzie AR, Laing RB, Smith CC, Kaar GF, SmithFW: Spinal epidural abscess: the importance of earlydiagnosis and treahnent. J Neurol Neurosurg Psychiatry65:209-212, 1998
17. Nussbaum ES, Rigamonti D, Standiford H, NumaguchiY, Wolf AL, Robinson WL: Spinal epidural abscess: Areport of 40 cases and review. Surg Neurol 38:225-231,1992
18. Post MJ, Sze G, Quencer RM, Eismont FJ, Green BA,Gahbauer H: Gadolinium-enhanced MR in spinalinfection. J Comput Assist Tomogr 14:721-729,1990
19. Redekop JG, Del Maestro FR: Diagnosis andmanagement of spinal epidural abscess. Can J NeurolSci 19:180-187,1992
20. Rigamonti D, Liem L,Sampath P, Knoller N, NamaguchiY,Schreibman OL,Sloan MA, Wolf A, Zeidman S:Spinalepidural abscess: contemporary trends in etiology,evaIuation, and management. Surg Neurol 52:189-196,1999
21. Sadato N, Numaguchi Y, Rigamonti D, Kodama T,Nussbaum E, Rothman M: Spinal epidural abscess withgadolinium-enhanced MR!. Serial follow-up studies andclinical correlations. Neuroradiology 36:44-48, 1994
22. Sampath P, Rigamonti D: Spinal epidural abscess: areview of epidemiology, diagnosis, and treatment. JSpinal Disord 12:89-93, 1999
23. Schmutzhard E, Aichner F, Dierckx RA, GerstenbrandF, Willeit J: New perspectives in acute spinal epiduralabscess: illustrated by two case reports. Acta Neurochir80:105-108,1986
24. Spiegelmann R, Findler G, Faibel M, Ram Z, Schacked I,Sahar A:Postoperative spinal epidural empyema: clinicaland computed tomography features. Spine 16:1146-1149,1991
25. Taccani L,Johnston FG, Symon L:Spinal epidural abscess:Review of 10cases. Ada Neurochir 138:520-523,1996
Thoracic spinal cord is the most commonly involved
area for intramedullanj spinal cord abscess.
116





![Epidural steroid injections: our experience and a review of the ......Infectious Epidural abscess, Discitis, Osteomyelitis [38-45] Intravascular injection Intravenous or Intraarterial](https://img.pdfslide.net/doc/110x75/60df39605510cf3a1862f983/epidural-steroid-injections-our-experience-and-a-review-of-the-infectious.jpg)






















