Embed Size (px)
Citation preview

~ .
ELSEVIER Brain & Development 1994; 16:16-22
Special Article
Acute hemiplegia syndrome in childhood Takehiko Okuno, MD
Three types of clinical features at the onset are well known to be characteristic of acute hemiplegia syndrome (AHS). Type 1 comprises status epilepticus of hemiconvulsions with fever. Representative diseases of this type are the infectious diseases of the central nervous system, acute encephalopathy and cerebral vascular diseases. Type 2 comprises status epilepticus of hemiconvulsions without fever. Cerebral vascular diseases and epilepsy are the major ones of this type. Type 3 comprises hemiplegia or hemiparesis of sudden onset without fever or convulsions. Most patients with this type had cerebral vascular diseases, about half of which were moyamoya disease in Japan. Recent progress in neuroimaging studies has allowed considerable elucidation of the etiology of AHS. Gadolinium- enhanced MRI showed minimal lesions such as capsular infarction more clearly than plain MRI. Acetazolamide test 99mTc-HMPAO SPECT imaging is one of the useful assisted diagnostic techniques for moyamoya disease, because it reveals the reserve capacity of the collaterals. [123I]IMP SPECT is useful for the diagnosis and follow-up of acute disseminated encephalomyelitis (ADEM), as the images of the lesions coincide well with the MRI ones. 99mTc-HMPAO SPECT in a case with alternating hemiplegia revealed normoperfusion in the ictai periods. Four cases of AHS are reported here.
Key words: Acute hemiplegia syndrome; Lacunar infarction; Moyamoya disease; Acute disseminated en- cephalomyelitis; Alternating hemiplegia in an infant
1. INTRODUCTION
Acute hemiplegia syndrome (AHS) in childhood is often found in infants under 2 years of age, although the etiology varies [1-5]. Hemiconvulsions develop with or without fever. Hemiplegia or transient ischemic attacks (TIA) occur abruptly in cases of cerebral infarc- tion or moyamoya disease. Recent progress in imaging studies has allowed considerable elucidation of the etiology of AHS. [~23I]IMP-SPECT (single photon emission computed tomography) is useful for the de- tection of cerebral ischemia, because of its sensitivity, non-invasiveness, and accurate reflection of the cere-
Department of Pediatrics, Tenri Hospital, Tenri, Nara, Japan
Received 7 August 1993; accepted 5 October 1993
This paper was presented as an invited lecture at the 35th annual meeting of the Japanese Society of Child Neurology, Kyoto, 17-19 June 1993.
Correspondence address: Dr. Okuno, Department of Pediatrics, Tenri, Nara 632, Japan. Fax: (81) (7436) 21 903.
0387-7604/94/$07.00 © 1994 Elsevier Science B.V. All rights reserved SSDI 0387-7604(93)E0100-W
bral blood flow distribution [6]. A post-hemiconvulsive type of hemiplegia has been described as the hemicon- vulsion-hemiplegia-epilepsy (HHE) syndrome [7]. It has been reported that the epileptic seizures occurred 8 years after the onset in one long-term follow-up case [8].
Alternating hemiplegia in infants was first reported in 1971 by Verret and Steele [9]. Kr~igeloh and Aicardi emphasized the differences between this syndrome and the common types of hemiplegia or basilar migraine which have been discussed in previous reports [10-12].
Four cases of AHS are reported here.
2. CLASSIFICATION OF AHS
Among the 100 patients with acute hemiplegia syn- drome in childhood that we have studied, there were 42 cases of type 1, i.e. status epilepticus of hemiconvul- sions with fever; those of type 2, i.e. status epilepticus of hemiconvulsions without fever, numbered 12, and those of type 3 without fever or convulsions 46 [13]. About one-third with type 1 AHS had infectious dis-

7". Okuno /Brain & Development 1994; 16:16-22 17
eases of the central nervous system, including acute encephalopathy, cerebral vascular diseases and an un- known etiology. About half of the type 2 cases had had cerebral vascular diseases, and the other half epilepsy and an unknown etiology. Type 3 cases had hemiplegia or hemiparesis of sudden onset without fever or con- vulsions. Most patients with this type had cerebral vascular diseases, about half of which was diagnosed as moyamoya disease. This classification is assumed to be useful, as the type of onset is characteristic of the etiology.
girl had left hemiparesis and was admitted to this hospital.
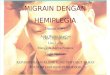
On T2-weighted MRI, an oval high intensity area was noted in the right putamen (Fig. 1, left). T 1- weighted MRI showed a low intensity area in the same region, and ring-like enhancement around this area and at its center were seen with gadolinium (Fig. 1, right).
She was diagnosed as having a capsular infarction and the hemiparesis improved within a few weeks.
3. CAPSULAR INFARCTION
Although capsular infarction was essentially un- known in children until the introduction of cranial computed tomography, it is not an infrequent occur- rence [14]. Regli et al. reported that gadolinium-en- hanced magnetic resonance imaging (MRI) of small deep (lacunar) cerebral infarcts led to improvement in the evaluation of the clinicotopographic correlation [15]. In our case, gadolinium-enhanced magnetic reso- nance imaging revealed the region of the lacunar in- farction more clearly than CT.
3.1. Case 1: a 3-year-old girl
The patient had had a common cold for 10 days. After taking a nap, her mother found her limping and speaking unclearly, and consulted Tenri Hospital. The
4. MOYAMOYA DISEASE
A decrease in cerebrovascular reactivity to acetazo- lamide has been reported in patients with occlusion of the internal carotid artery or cerebral ischemic syn- drome [16,17], and a significant increase in the cerebral blood flow (CBF) was observed post-neurosurgical op- eration [16]. Pre- and post-acetazolamide test 99rnTc- H M P A O (99mTc-hexamethylpropylenamine oxime) SPECT imaging is one of the useful assisted diagnostic techniques for moyamoya disease. The decrease in CBF post-acetazolamide administration implies a poor reserve capacity of the dilated collaterals in moyamoya disease.
4.1. Case 2: a 2-year 7-month-old boy
One month before admission, the patient developed left hemiparesis after head injury. CT showed a low
Fig. 1. MRI in Case 1. On T2-weighted MRI, an oval high intensity area was notedin the right putamen (left). Tl-weighted MRI showed aiow intensity area in the same region, and ring-like enhancement around this area and at its center were seen with gadolinium (right).

18 T. Okuno /Brain & Development 1994; 16." 16-22

T. Okuno /Brain & Development 1994; 16:16-22 19
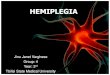
Fig. 3. MRI in Case 3. A high-intensity area in the bilateral cerebellum, thalamus, midbrain and pallidum (arrowheads) was shown. This area of high intensity was more pronounced on the right than on the left side.
intensi ty area in the right occipital lobe. Two days before hand, he exper ienced left hemipares is for a few minu tes after crying. He was admi t t ed to Tenr i Hospi- tal, because his consciousness became turb id after cry- ing.
M R I showed a high in tensi ty area on T2-weighted imaging. M R I showed flow void areas on Tl -weighted imaging in the bi la teral basal ganglia. O n 99mTc- H M P A O SPECT, an ischemic region of cerebral CB F was revealed in the right hemishpere (Fig. 2, left). C B F in the right hemishpere was decreased after venous inject ion of acetazolamide (Fig. 2, right).
Cerebra l angiography (CAG) showed stenosis of the bi la teral in te rna l carotid arteries and moyamoya arter- ies in the basal ganglia.
5. ACUTE DISSEMINATED E N C E P H A L O M Y E L I T I S (ADEM)
CT scanning shows the reversible hypodense areas in the cerebral white mat ter , basal ganglia and mid- bra in in A D E M [18-20].
Fig. 2. 99mTc-HMPAO SPECT in Case 2. On 99raTc-HMPAO SPECT, an ischemic region of CBF was shown in the right hemisphere (left). CBF in the right hemishpere was decreased after venous injection of acetazolamide (right).
Fig. 4. [123I]IMP SPEC'T in Case 3. Decreased blood flow was noted in the bilateral thalamus and occipital lobes, and the cerebellum, midbrain and pons.
Fig. 5. Comparison of the first (left, R/L = 932/977 = 95.4) and second ictal 99mTc-HMPAO SPECT scans (right, R/L = 794/832 = 95.4) in Case 4. Comparison of the first and second ictal 99mTc-HMPAO SPECT scans did not reveal a significant difference.

20 T. Okuno / Brain & Development 1994; 16:16-22
MRI revealed high-intensity in T 2 images coincident with the neurological abnormalities in ADEM [21-23]. Kesselring et al. reported that serial MRI was useful for distinguishing between multiple sclerosis (MS) and ADEM, because follow-up MRI at intervals of 2 weeks-18 months demonstrates partial resolution of the abnormalities, although some persistent lesions and new MRI lesions were found at follow-up in 1 case after an interval of 2 weeks [23].
[123I]IMP SPECT is useful for the diagnosis and follow-up of ADEM, as the images of the lesions coincide well with the MRI ones.
5.1. Case 3: a 5-year-old girl
The patient was born after a normal full-term preg- nancy and uncomplicated delivery. Her birth weight was 3,100 g. About 20 days prior to admission, she developed an episode of fever, headache and vomiting, and so was referred to a regional hospital. CSF showed pleocytosis and a negative culture, without increased protein or IgG. The patient was diagnosed as having aseptic meningitis and so was admitted for approxi- mately 2 weeks.
Her mother noted that she watched television from a very close distance and was ataxic from a few days after discharge. She consulted an ophthalmologist, who noted a decrease in visual activity: right, 0.1; left, 0.05. She also developed a dull facial expression and was noted to wander aimlessly. She was admitted to our hospital with drowsiness and left hemiparesis.
MRI 2 weeks after the onset showed a high-intensity area involving the bilateral cerebellum, thalamus, mid- brain, and pallidum (Fig. 3). This area of high intensity was more pronounced on the right than on the left side. CSF examination revealed 23 cel ls /ml, 37 mg pro te in /d l , and normal IgG and myelin basic protein levels.
EEG showed 7 Hz 0 waves mixed with 8 Hz a waves. Brainstem auditory evoked potentials (BAEP), visual evoked potentials (VEP), and somatosensory evoked potentials (SEP) were all normal. Blood chem- istry was normal. Lactate and pyruvate were normal. Viral CF in serum and HI antibody titers were not significantly increased.
The patient was diagnosed as having ADEM and thus treated with 2 m g / k g / d a y of prednisolone for 2 weeks beginning 17 days after the onset. As the symp- toms and signs disappeared rapidly, the steroid was gradually tapered and discontinued 5 weeks after the beginning of the treatment.
CT showed findings similar to the MRI ones at 3 weeks after the onset. The abnormal findings were found to have been resolved on MRI approximately 3 months after the onset.[lz3I]IMP SPECT 4 weeks after the onset gave images of lesions resulting from de-
creased blood flow in the bilateral thalamus and occipi- tal lobes, and the cerebellum, midbrain and pons (Fig. 4). These findings almost coincided with those on MRI.
6. ALTERNATIVE HEMIPLEGIA IN INFANTS (AHI)
Increased CBF has been reported during the epilep- tic seizures, and hypoperfusion was found in patients with epilepsy interictally. We have reported the similar- ity of the regional CBF (rCBF) in AHI on SPECT to that in epilepsy. Decreased or normal interictal rCBF has been detected by [123I]IMP-SPECT and increased ictal rCBF has been detected by 99mTc-HMPAO SPECT in AHI [24,25].
A regional decrease in cerebral tracer uptake was observed in 16 patients with common migraine by Schlake et al. [26]. In 10 of their 15 cases with hemi- plegic symptoms during the migraine attacks, the areas of decreased tracer uptake on SPECT with 99mTc-
HMPAO showed a topographic relationship to the neurological deficits.
Several groups observed hypoperfusion of rCBF on PET (positron emmision tomography) or [I23I]IMP SPECT in the interictal periods in AHI [27,28]. In a nation wide investigation on AHI, rCBF hypoperfusion was observed in 6 of the 8 examined in Japan [29]. There has only been one previous report of rCBF measured by [123I]IMP SPECT during actual alternat- ing hemiplegic episodes, decreased rCBF being re- ported [30].
Some alternating hemiplegic infants have epileptic seizures and exhibit epileptic discharges on EEG. Han- son and Chodos proposed that the same mechanism as that operating in epilepsy is involved [31].
A S P E C T study revealed hypoperfusion of rCBF in patients with focal epilepsy [32,33]. A high uptake region caused by epileptic seizure discharges was re- vealed on ictal measurements [33-35]. The normal rCBF findings in alternating hemiplegic infants may not be compatible with those found in migraine or epileptic disorders, but not all the patients showed hypoperfusion during migraine [26], and hyperperfu- sion was detected on ictal measurement in patients with epilepsy [32-35].
6.1. Case 4: a 2-year-old girl
The patient was born after a normal pregnancy and delivery at 41 weeks of gestation, with a birth weight of 3,615 g. She had no family history of migraine. Her development was normal. At the age of 11 months, right hemiplegia occurred, followed by left hemiplegia about a week after the onset. She was treated with carbamazepine and the attacks developed again at the age of 1 year and 8 months.

T. Okuno /Brain & Development 1994; 16." 16-22 21
On admission, her consciousness was clear. Physical findings were normal. No paresis was found. The deep tendon reflexes were normal. No pathological reflex was noted. Laboratory findings. Serum electrolytes and chemicals were normal. Serum lactate, pyruvate and ammonia, and serum and urinary amino acids were normal. Uri- nary 5-HIAA was normal during the attacks. BAEP, VEP and SEP were normal. CT scanning, MRI, CAG and VAG (vertical angiography) showed no abnormali- ties. She was diagnosed as having AHI.
Ictal 99mTc-HMPAO SPECT during the left hemi- plegia revealed almost symmetric uptake. Comparison of the first and second ictal SPECT scans did not reveal a significant difference, although there seemed to be slight asymmetry between the left and right temporal lobes (Fig. 5).
ACKNOWLEDGEMENTS I wish to thank the doctors of the Pedi- atric Neurology Group, Department of Pediatrics, School of Medicine, Kyoto University, Kyoto, and those at the Departments of Pediatrics and Radiology, Tenri Hospital, Tenri. I also wish to thank Drs Naoki Matoba and Yoshiharu Yonekura of the Radiology De- partment, School of Medicine, Kyoto University, Kyoto, for their helpful comments and kind preparation of the radiologic records. 1 also thank Dr. Haruki Mikawa, Hononary Professor at Kyoto Uni- versity, and now the director of the Hospital of Kansai Electric Power Co., for his supervision.
7. REFERENCES
1. Bickerstaff ER. Aetiology of acute hemiplegia in childhood. Br Med J 1964; 2: 82-7.
2. Carter S, Gold AP. Acute infantile hemiplegia. Pediatr Clin North Am 1967; 14: 851-64.
3. Solomon GE, Hilal SK, Gold AP, et al., Natural history of acute hemiplegia of childhood. Brain 1970; 93: 107-20.
4. Isler W. Acute hemiplegias and hemisyndromes in childhood. London: Spastics International Medical Publications, 1971.
5. Gold AP, Carter S. Acute hemiplegia of infancy and childhood. Pediatr Clin North Am 1976; 23: 413-33.
6. Shirasaka Y, Ito M, Okuno T, Fujii T, Mikawa H. Sequential [123I]IMP-SPECT in acute infantile hemiplegia. Peditr Neurol 1989; 5: 306-10.
7. Gastaut H, Pinsard N, Gastaut JL, Regis H, Michel B. Acute hemiplegia in children. Adv Neurol 1979; 25: 329-37.
8. Kataoka H, Okuno T, Mikawa H, Hojo H. Cranial computed tomographic and electroencephalographic abnormalities in chil- dren with post-hemiconvulsive hemiplegia. Eur Neurol 1988; 28: 279-84.
9. Verret S, Steele JC. Alternating hemiplegia in childhood: a report of eight patients with complicated migraine beginning in infancy. Pediatrics 1971; 47: 675-80.
10. Kr~igeloh I, Aicardi J. Alternating hemiplegia in infants: Report of five cases. Dev Med Child Neurol 1980; 22: 784-91.
11. Hosking GP, Cavanagh NPC, Wilson J. Alternating hemiplegia: complicated migraine of infancy. Arch Dis Child 1978; 53: 656-9.
12. Dittrich J, Havlova M, Nevsimalova S. Paroxysmal hemiparesis in childhood. Dev Med Child Neurol 1979; 21: 800-7.
13. Okuno T, Takao T, Itoh M, Konishi Y, Nakano S, Mikawa H. Acute hemiplegia in childhood (in Japanese). CTKenkyu (Tokyo) 1983; 5: 223-30.
14. Okuno T, Takao T, Ito M, Konishi Y, Mikawa H, Nakano Y. Infarction of the internal capsule in children. J Comput Assist Tomogr 1980; 4: 770-4.
15. Regli L, Regli F, Maeder P, Bogousslavsky J. Magnetic reso- nance imaging with gadolinium contrast agent in small deep (lacunar) cerebral infarcts. Arch Neurol 1993; 50: 175-80.
16. Vorstrup S, Brun B, Lassen NA. Evaluation of the cerebral vasodilatory capacity by the acetazolamide test before EC-IC bypass surgery in patients with occlusion of the internal carotid artery. Stroke 1986; 17: 1291-8.
17. Matsuda H, Higashi S, Asli IN, Eftekhari M, Esmaili J, Seki H, et al., Evaluation of cerebral collateral circulationby Tech- netium-99m HM-PAO brain SPECT during the Matas test: Report of three cases. J Nucl Med 1988; 29: 1724-9.
18. Okuno T, Takao T, Ito M, Mikawa H, Nakano Y. Contrast enhanced hypodense areas in a case of acute disseminated encephalitis following influenza A virus. Computerized Radiol 1982; 6: 215-7.
19. Okuno T, Fuseya Y, Ito M, Konishi Y, Nakano Y. Reversible multiple hypodense areas in the white matter diagnosed as acute disseminated encephalomyelitis. J Comput Assist Tomogr. 1981; 5: 119-21.
20. Lukes SA, Norman D. Computed tomography in acute dissemi- nated encephalomyelitis. Ann Neurol 1983; 13: 567-72.
21. Ormerod I, Bronstein A, Rudge P, Johnson G, Macmanus D, Halliday AM, et al., Magnetic resonance imaging in clinically isolated lesions of the brain stem. J Neurol Neurosurg Psychiatr 1986; 49: 737-43.
22. Atlas SW, Grossman RI, Goldberg HI, Hackney DB, Bilaniuk LT, Zimmerman RA. MR diagnosis of acute disseminated en- cephalomyelitis. J Comput Assist Tomogr 1986; 10: 798-801.
23. Kesselring J, Miller DH, Robb SA, Kendall BE, Moseley IF, Kingsley D, et al., Acute disseminated encephalomyelitis: MRI findings and the distinction from multiple sclerosis. Brain 1990; 113: 291-302.
24. Shirasaka Y, lto M, Okuno T, Mikawa H, Yamori Y. Epileptic seizures difficult to differentiate from alternating hemiplegia in infants: A case report. Brain Dev (Tokyo) 1990; 12: 521-4.
25. Kanazawa O, Shirasaka Y, Hattori H, Okuno T, Mikawa H. Ictal 99mTc-HMPAO SPECT in alternating hemiplegia. Pediatr Neu- rol 1991; 7: 121-4.
26. Schlake HP, Bottger IG, Grotemeyer KH, Husstedt IW, Vollet B, Schober O, et al., Single photon emission computed tomogra- phy with technetium-99m hexamethyl propylenamino oxime in the pain-free interval of migraine and cluster headache. Eur Neurol 1990; 30: 153-6.
27. Nakamura Y, Nagano T, Mizuguchi M, Mizuno Y, Tamagawa K, Komiya K, et al., Alternating hemiplegia in infants: a case report (in Japanese). No To Hattatsu (Tokyo) 1986; 18: 406-12.
28. Sakuragawa N, Matsuo T, Kihira S, Matsuzaka T, Matsui A, Arima M, et al., Alternating hemiplegia in infancy: two case reports and reduced regional cerebral blood flow on 11CO2 dynamic positron emission tomography. Brain Dev (Tokyo) 1985; 7: 207.
29. Sakuragawa N, Arima M, Matsumoto S. Nationwide investiga- tion of actual conditions of alternating hemiplegia of children in Japan (in Japanese). Nippon Shonika Gakkai Zasshi (Tokyo) 1988; 92: 892-8.
30. Hattori H, Hashizuka S, Matsuoka O, Murata R, Ueda T. Alternating hemiplegia in infants: a case report with abnormal findings on ABR (auditory brain stem response) and SPECT (single photon emission CT) (in Japanese). Shonika Rinsho (Tokyo) 1989; 42: 77-82.
31. Hanson PA, Chodos R. Hemiparetic seizures. Neurology 1978; 28: 920-3.
32. Bonte FJ, Stokely EM, Devons MD, Horman RW. Single photon tomographic study of regional cerebral blood flow in epilepsy. Acta Neurol 1983; 40: 267-70.

22 T. Okuno / Brain & Development 1994; 16:16-22
33. Dietrich ME, Bergen D, Smith MC, Fariello R, Ali M. Correla- tion of abnormalities of interictal n-isopropyl-p-iodoampheta- mine single-photon emission tomography with focus of seizure onset in complex partial seizure disorders. Epilepsia 1991; 32: 187-94.
34. Ryding E, Rosen I, Elrnqvist D, Ingvar DH. SPECT measure-
ments with 99mTc-HMPAO in focal epilepsy. J Cereb Blood Flow Metab 1988; 8: $95-100.
35. Stefan H, Bauer J, Feistel H, Schulemann H, Neubauer U, Wenzel B, et al., Regional cerebral blood flow during focal seizures of temporal and frontocentral onset. Ann Neurol 1990; 27: 162-6.