Embed Size (px)
Citation preview
BRIEF COMMUNICATIONS
Acute treatment of torsades de pointes with amiodarone: Proarrhythmic and antiarrhythmic association of QT prolongation
Andrew C. Rankin, MD, Stuart D. Pringle, MB, ChB, and Stuart M. Cobbe, MD. Glasgow, Scotland
The polymorphic ventricular tachycardia known as "tor- sades de pointes" is associated with syndromes of QT in- terval prolongation, which may be congenital 1 or secondary to drugs, or electrolyte abnormalities. 2 Antiarrhythmic drugs that cause prolongation of the QT interval, such as quinidine, disopyramide, sotalol, and amiodarone, are par- ticularly incriminated. It has therefore been recommended that they should be avoided in the short-term treatment of torsades de pointes. 2 The antiarrhythmic action of such drugs, however, is also associated with prolongation of the QT interval. 3, 4 The clinical significance of a long QT inter- val, whether proarrhythmic or antiarrhythmic, remains uncertain. 5 We present a patient with QT interval prolon- gation and torsades de pointes of multifactorial etiology
From the University Department of Medical Cardiology, Royal Infirmary. Reprint requests: Dr Andrew C. Rankin, Department of Medical Cardiol- ogy, Royal Infirmary, 10 Alexandra Parade, Glasgow, G31 2ER, Scotland. 4 / 4 / 1 6 7 2 8
(sotalol, hypokalemia, and hypomagnesemia 2, 6, 7) who was successfully treated over the short term with intravenous amiodarone, despite resultant further QT interval prolon- gation.
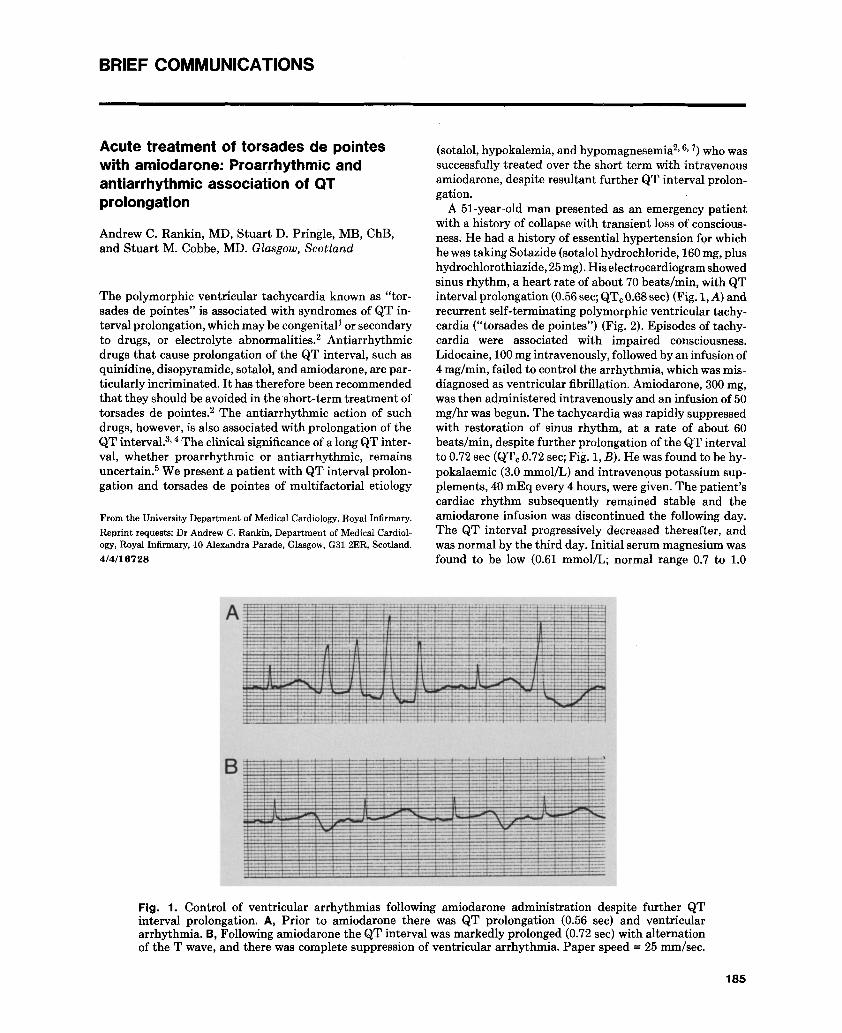
A 51-year-old man presented as an emergency patient with a history of collapse with transient loss of conscious- ness. He had a history of essential hypertension for which he was taking Sotazide (sotalol hydrochloride, 160 mg, plus hydrochlorothiazide, 25 mg). His electrocardiogram showed sinus rhythm, a heart rate of about 70 beats/min, with QT interval prolongation (0.56 sec; QTe 0.68 sec) (Fig. 1, A) and recurrent self-terminating polymorphic ventricular tachy- cardia ("torsades de pointes") (Fig. 2). Episodes of tachy- cardia were associated with impaired consciousness. Lidocaine, 100 mg intravenously, followed by an infusion of 4 mg/min, failed to control the arrhythmia, which was mis- diagnosed as ventricular fibrillation. Amiodarone, 300 mg, was then administered intravenously and an infusion of 50 mg/hr was begun. The tachycardia was rapidly suppressed with restoration of sinus rhythm, at a rate of about 60 beats/min, despite further prolongation of the QT interval to 0.72 sec (QTr 0.72 sec; Fig. 1, B). He was found to be hy- pokalaemic (3.0 mmol/L) and intravenous potassium sup- plements, 40 mEq every 4 hours, were given. The patient's cardiac rhythm subsequently remained stable and the amiodarone infusion was discontinued the following day. The QT interval progressively decreased thereafter, and was normal by the third day. Initial serum magnesium was found to be low (0.61 mmol/L; normal range 0.7 to 1.0
Fig. 1. Control of ventricular arrhythmias following amiodarone administration despite further QT interval prolongation. A, Prior to amiodarone there was QT prolongation (0.56 sec) and ventricular arrhythmia. B, Following amiodarone the QT interval was markedly prolonged (0.72 sec) with alternation of the T wave, and there was complete suppression of ventricular arrhythmia. Paper speed = 25 mm/see.
185

January 1990
1 86 Brief Communications American Heart Journal
1S
Fig. 2. T•rsadesdep•intes .Aself- terminat ingepis•de•fp•lym•rphictachycardia•ini t iatedbya`` late•• ventricular premature beat, occurred on the downslope of the T wave. Paper speed = 25 mm/sec.
mmol/L) but became normal after 2 days without t reat- ment. Alcohol excess was denied by the pa t ien t at the t ime of admission, but i t later emerged tha t he had been drink- ing heavily during the preceding week. Echocardiography and exercise test ing were normal. Blood pressure remained normal and ant ihyper tensive therapy was not recom- menced.
The association between QT prolongation and torsades de pointes is well established, 1, 2 but the quant i ta t ive rela- t ionship is less clear. 5 No critical QT durat ion has been identif ied and not all clinical syndromes with long QT ex- hibi t the arrhythmia, indicat ing tha t i t is not s imply the length of the QT interval t ha t is arrhythmogenic. Disper- sion and not just prolongation of repolarization is necessary for the development of the arrhythmia. 5 Successful short- term t rea tment of torsades de pointes is directed not only at shortening the QT interval bu t at unifying repolariza- tion, as can be achieved by pacing. 2 Shor t - term drug t reat- ment of torsades de pointes is less predictable. Lidocaine will suppress the a r rhy thmia in less than half of cases. 7, 8 Class l a drugs, which may cause further QT prolongation, are rarely effective and may exacerbate the arrhythmia. 2; s Similarly, the class I I I drug bre ty l ium has been repor ted as relat ively ineffective 7 or proarrhythmic. 8 Amiodarone, an- other class I I I drug, may cause prolongation of the QT in- terval and torsades de pointes, s, 9 Proarrhythmia , however, is uncommon with amiodarone and QT prolongation is more often associated with ant ia r rhythmic therapeut ic efficacy) Combinat ions of drugs tha t prolong the QT interval have been advised against because of concern about increased arrhythmogenic potential . 2, 7 This might have been expected in the present case, as the use of ami- odarone to t rea t sotalol- induced torsades de pointes was associated with marked prolongation of the QT interval. The opposite occurred, however, with suppression of the ventr icular arrhythmias.
The efficacy of amiodarone may be due s imply to suppression of ventr icular ectopy, which often precedes torsades de pointes, 7 or may depend on its correcting dis- persion of repolarization, 5 by prolonging action potent ial durat ion throughout the h e a r t ) ~ A previous s tudy s of drug-induced polymorphic ventr icular tachycardia (which included but was not l imited to torsades de pointes) repor ted one case of successful shor t - term t rea tment with intravenous amiodarone, but without details of its effects on the QT interval. These same investigators also found amiodarone to be useful as al ternat ive long-term antiar- rhythmic therapy, often in spite of QT interval prolonga-
tion. However, there is insufficient evidence to recommend amiodarone as the shor t - term t rea tment of choice for tor- sades de pointes, which remains a t r ia l or ventricular pacing,2, 7 but we present this case to i l lustrate the arrhyth- mic and ant iar rhythmic associations of QT prolongation.
REFERENCES 1. Schwartz PJ. Idiopathic long QT syndromes: progress and
questions. AM HEART J 1985;109:399. 2. Stratmann HG, Kennedy HL. Torsades de pointes associated
with drugs and toxins: recognition and management. AM HEART J 1987;113:1470.
3. Roden DM, Woosley RL. QT prolongation and arrhythmia suppression. AM HEART J 1985;109:411.
4. Torres V, Tepper D, Flowers D, Wynn J, Lam S, Keefe D, Mi- ura D, Somberg JC. QT prolongation and the antiarrhythmic efficacy of amiodarone. J Am Coll Cardiol 1986;7:]42.
5. Surawicz B, Knoebel SB. Long QT: good, bad or indifferent? J Am Coll Cardiol 1984;4:398.
6. McKibbon JK, Pocock WA, Barlow JB, Scott Millar RN, Obel IWP. Sotalol, hypokalaemia, syncope, and torsades de pointes. Br Heart J 1984;51:157.
7. Kay GN, Plumb V J, Arciniegas JG, Henthorn RW, Waldo AL. Torsades de pointes: the long-short initiating sequence and other clinical features: observations in 32 patients. J Am Coll Cardiol 1983;2:806.
8. Nguyen PT, Scheinmann MM, Seger J. Polymorphous ven- tricular tachycardia: clinical characterization, therapy, and the QT interval. Circulation 1986;74:340.
9. Sclarovsky S, Lewin RF, Kracoff 0, Strasberg B, Arditti A, Agmon J. Amiodarone-induced polymorphous ventricular ta- chycardia. AM HEART J 1982;105:6.
10. Yabek SM, Kato R, Singh BN. Effects of amiodarone and its metabolite, desethylamiodarone, on the electrophysiologic properties of isolated cardiac muscle. J Cardiovasc Pharmacol 1986;8:197.
Pulmonic ba l loon va lvu lop lasty in adul ts
Warren Sherman, MD, a Ronnie Hershman, MD, a Dimitrios Alexopoulos, MD, a Marc Cohen, MD, a Jay Midwall, MD, c Joshua Kieval, MD, c and Richard Golinko, MD. b New York, N.Y., and Atlantis and Miami, Fla.
From the Divisions of aCardiology and bpediatric Cardiology, Mount Sinai Hospital, New York; and e John F. Kennedy Medical Center, Atlantis; and the University of Miami, School of Medicine. Reprint requests: Warren Sherman, MD, Division of Cardiology, Box 1030, Mount Sinai Hospital, New York, NY 10029. 4/4/16723