Embed Size (px)
Citation preview

Adaptation and Validation of the Voice Handicap
Index in Latvian
*Baiba Trinite and †Janis Sokolovs, *Liepaja, and yRiga, Latvia
Summary: Objectives. To establish psychometric indicators of the Voice Handicap Index (VHI) (Latvian version)
AccepFrom t
and the yAddre
ResearchE-mail: bJourna0892-1� 201http://d
and their relationship to the psychometric indicators of the original items.Study Design. Parallel group design.Methods. The VHI was translated and adapted to Latvian. The translated version of the VHI (Lat-VHI) wascompleted by 54 patients with voice disorders and by 73 subjects without voice disorders forming the control group.A test-retest group included 54 subjects without voice problems, able to complete the questionnaire twice. The test-retest stability, internal consistency of items of the Lat-VHI, and content and convergent validity of the Latvian versionof the VHI were analyzed.Results. The interclass correlation coefficient ratio of all scales indicated statistically significant (P < 0.001) test-retestreliability for the Lat-VHI. High internal consistency was observed among the Lat-VHI total scale (a¼ .96), functional(a ¼ .92), physical (a ¼ .86), and emotional scale (a ¼ .91) in the patient group. The Pearson moment correlation co-efficient indicates a high correlation among the Lat-VHI total scale and subscales (r > 0.94), as well as a high correlationamong subscales (r > 0.81) in the patient group. Convergent validity of the Lat-VHI was determined by comparing theLat-VHI results with the Voice Disorder Severity scale results. Statistically significant correlation (r¼ 0.78, P < 0.001)was discovered in the patient group.Conclusions. The Latvian version of the VHI is a psychometrically validated instrument whose indicators correspondto the psychometric indicators of the original sample.Key Words: Voice–Subjective evaluation–Voice Handicap Index–Quality of life.
INTRODUCTION
A self-assessment of voice by the patient is very important inclinical practice. The objective evaluation of voice functiongives information about quality of voice, functional, and struc-tural integrity of the larynx but does not allow the investigationof the handicapping effect of voice disorders. It is the patientwho has to live with his/her voice that provides this informa-tion.1 The purpose of subjective self-evaluation was to deter-mine the deviance of voice quality and the severity ofdisability or handicap in daily professional and social life andthe possible emotional repercussions of the dysphonia.2 Oneof the most used self-assessment methods of impact of voicedisorders is the Voice Handicap Index (VHI). The VHI wasdeveloped in 1997.3 The VHI comprised 30 statements dividedinto three subscales—10 physical, 10 emotional, and 10 func-tional statements. Respondents use a five-point Likert scale toevaluate the extent to which each of these statements relate totheir individual experience. The minimum total acquired pointsis 0 and the maximum is 120 points. Allocated time for fillingout the VHI is 5–10 minutes. The VHI is adapted and validatedin many languages: German,4 Chinese,5 Mandarin Chinese,6
French,7 Portuguese,8 Polish,9 Dutch,10 Hebrew,11 Spanish,12
Swedish,13 Brazilian Portuguese,14 Greek,15 Italian,16
Arabic,17 Hindi,18 and others. To date, no statistically validand reliable instruments for measuring voice disorder handicap
ted for publication January 15, 2014.he *Speech and Voice Research Laboratory, Liepaja University, Liepaja, Latvia;Department of Otorhinolaryngology, Riga Stradins University, Riga, Latvia.ss correspondence and reprint requests to Baiba Trinite, Speech and VoiceLaboratory, Liepaja University, Liela iela 14, Liepaja, LV 3411, [email protected] of Voice, Vol. -, No. -, pp. 1-6997/$36.004 The Voice Foundationx.doi.org/10.1016/j.jvoice.2014.01.008
exist in Latvian. The purpose of the study was to establish aLatvian version of the VHI and evaluate the psychometricindices of the original items in the English VHI to the sameitems translated into Latvian.
MATERIAL AND METHODS
The development of the VHI Latvian version included transla-tion of the VHI into Latvian, administration of the VHI in a newcultural environment to persons with healthy voices and tovoice patients, and empirical and statistical validation of thetranslated material.
VHI translation and protocol form development was as fol-lows: (1) translation was performed by three highly qualifiedLatvian-English language practitioners, (2) symmetrical trans-lation method was adopted, using the two-way translationapproach, (3) emphasis was placed on the semantic compati-bility of the items, (4) local cultural peculiarities were takeninto consideration, (5) Voice Disorder Severity scale3 wasincluded into the VHI form for validation of convergence, (6)the translated material was tested in a small pilot study (fivemales, five females, three of them with voice pathology, andseven with healthy voices) after which the formulation ofsome items was changed.
The test-retest reliability was evaluated with interclass corre-lation coefficients (ICC). The mean of the differences (d) be-tween the test and retest, and the standard deviation of thedifferences (SDdiff) were calculated.
19 The 95% limits of agree-ment (LOA) were calculated as d±2SDdiff . The Bland and Alt-man20 method was used for calculation of LOA. The correlationbetween the subscales of the Lat-VHI was analyzed using Pear-son product-moment correlation.3,6 The reliability wasconsidered as high if 0.8� r� 1.21 The items of the VHI scaleshave more than two responses; therefore, Cronbach alpha
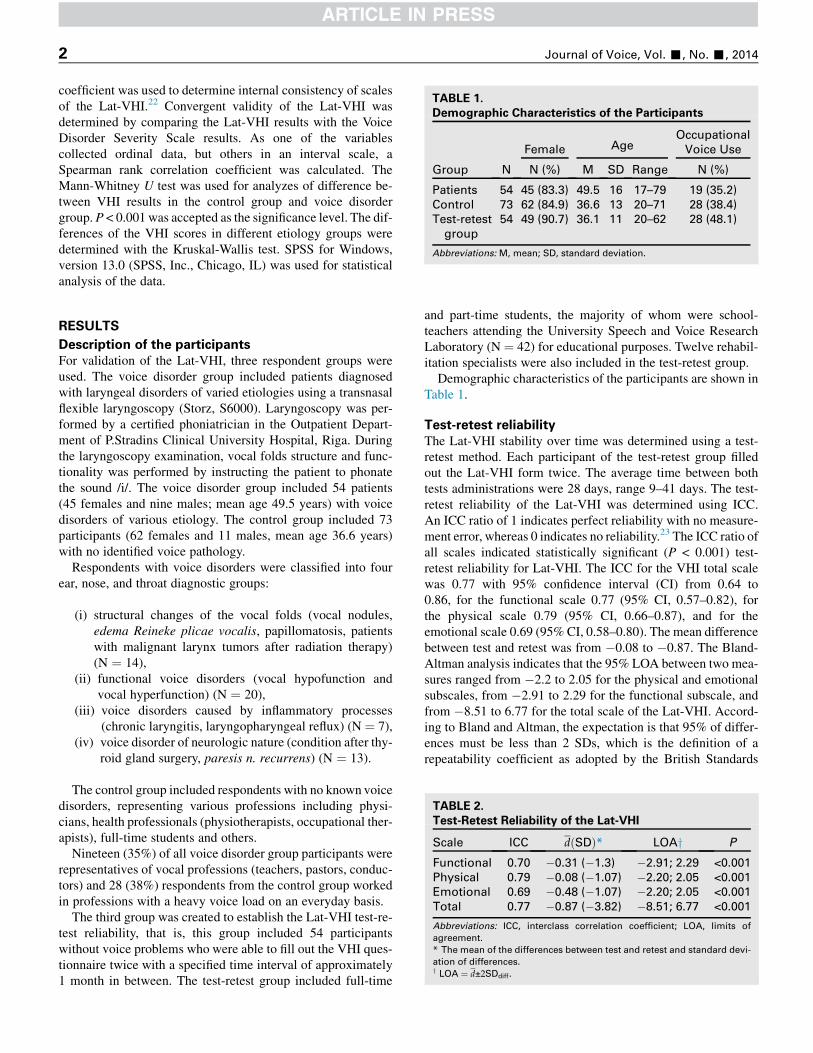
TABLE 1.
Demographic Characteristics of the Participants
Group N
Female AgeOccupational
Voice Use
N (%) M SD Range N (%)
Patients 54 45 (83.3) 49.5 16 17–79 19 (35.2)
Control 73 62 (84.9) 36.6 13 20–71 28 (38.4)
Test-retest
group
54 49 (90.7) 36.1 11 20–62 28 (48.1)
Abbreviations: M, mean; SD, standard deviation.
Journal of Voice, Vol. -, No. -, 20142
coefficient was used to determine internal consistency of scalesof the Lat-VHI.22 Convergent validity of the Lat-VHI wasdetermined by comparing the Lat-VHI results with the VoiceDisorder Severity Scale results. As one of the variablescollected ordinal data, but others in an interval scale, aSpearman rank correlation coefficient was calculated. TheMann-Whitney U test was used for analyzes of difference be-tween VHI results in the control group and voice disordergroup. P < 0.001 was accepted as the significance level. The dif-ferences of the VHI scores in different etiology groups weredetermined with the Kruskal-Wallis test. SPSS for Windows,version 13.0 (SPSS, Inc., Chicago, IL) was used for statisticalanalysis of the data.
TABLE 2.
Test-Retest Reliability of the Lat-VHI
Scale ICC dðSDÞ* LOAy P
Functional 0.70 �0.31 (�1.3) �2.91; 2.29 <0.001
Physical 0.79 �0.08 (�1.07) �2.20; 2.05 <0.001
Emotional 0.69 �0.48 (�1.07) �2.20; 2.05 <0.001
Total 0.77 �0.87 (�3.82) �8.51; 6.77 <0.001
Abbreviations: ICC, interclass correlation coefficient; LOA, limits of
agreement.
* The mean of the differences between test and retest and standard devi-
ation of differences.y LOA ¼ d±2SDdiff.
RESULTS
Description of the participants
For validation of the Lat-VHI, three respondent groups wereused. The voice disorder group included patients diagnosedwith laryngeal disorders of varied etiologies using a transnasalflexible laryngoscopy (Storz, S6000). Laryngoscopy was per-formed by a certified phoniatrician in the Outpatient Depart-ment of P.Stradins Clinical University Hospital, Riga. Duringthe laryngoscopy examination, vocal folds structure and func-tionality was performed by instructing the patient to phonatethe sound /i/. The voice disorder group included 54 patients(45 females and nine males; mean age 49.5 years) with voicedisorders of various etiology. The control group included 73participants (62 females and 11 males, mean age 36.6 years)with no identified voice pathology.
Respondents with voice disorders were classified into fourear, nose, and throat diagnostic groups:
(i) structural changes of the vocal folds (vocal nodules,edema Reineke plicae vocalis, papillomatosis, patientswith malignant larynx tumors after radiation therapy)(N ¼ 14),
(ii) functional voice disorders (vocal hypofunction andvocal hyperfunction) (N ¼ 20),
(iii) voice disorders caused by inflammatory processes(chronic laryngitis, laryngopharyngeal reflux) (N ¼ 7),
(iv) voice disorder of neurologic nature (condition after thy-roid gland surgery, paresis n. recurrens) (N ¼ 13).
The control group included respondents with no known voicedisorders, representing various professions including physi-cians, health professionals (physiotherapists, occupational ther-apists), full-time students and others.
Nineteen (35%) of all voice disorder group participants wererepresentatives of vocal professions (teachers, pastors, conduc-tors) and 28 (38%) respondents from the control group workedin professions with a heavy voice load on an everyday basis.
The third group was created to establish the Lat-VHI test-re-test reliability, that is, this group included 54 participantswithout voice problems who were able to fill out the VHI ques-tionnaire twice with a specified time interval of approximately1 month in between. The test-retest group included full-time
and part-time students, the majority of whom were school-teachers attending the University Speech and Voice ResearchLaboratory (N ¼ 42) for educational purposes. Twelve rehabil-itation specialists were also included in the test-retest group.Demographic characteristics of the participants are shown in
Table 1.
Test-retest reliability
The Lat-VHI stability over time was determined using a test-retest method. Each participant of the test-retest group filledout the Lat-VHI form twice. The average time between bothtests administrations were 28 days, range 9–41 days. The test-retest reliability of the Lat-VHI was determined using ICC.An ICC ratio of 1 indicates perfect reliability with no measure-ment error, whereas 0 indicates no reliability.23 The ICC ratio ofall scales indicated statistically significant (P < 0.001) test-retest reliability for Lat-VHI. The ICC for the VHI total scalewas 0.77 with 95% confidence interval (CI) from 0.64 to0.86, for the functional scale 0.77 (95% CI, 0.57–0.82), forthe physical scale 0.79 (95% CI, 0.66–0.87), and for theemotional scale 0.69 (95% CI, 0.58–0.80). The mean differencebetween test and retest was from �0.08 to �0.87. The Bland-Altman analysis indicates that the 95% LOA between two mea-sures ranged from �2.2 to 2.05 for the physical and emotionalsubscales, from �2.91 to 2.29 for the functional subscale, andfrom �8.51 to 6.77 for the total scale of the Lat-VHI. Accord-ing to Bland and Altman, the expectation is that 95% of differ-ences must be less than 2 SDs, which is the definition of arepeatability coefficient as adopted by the British Standards
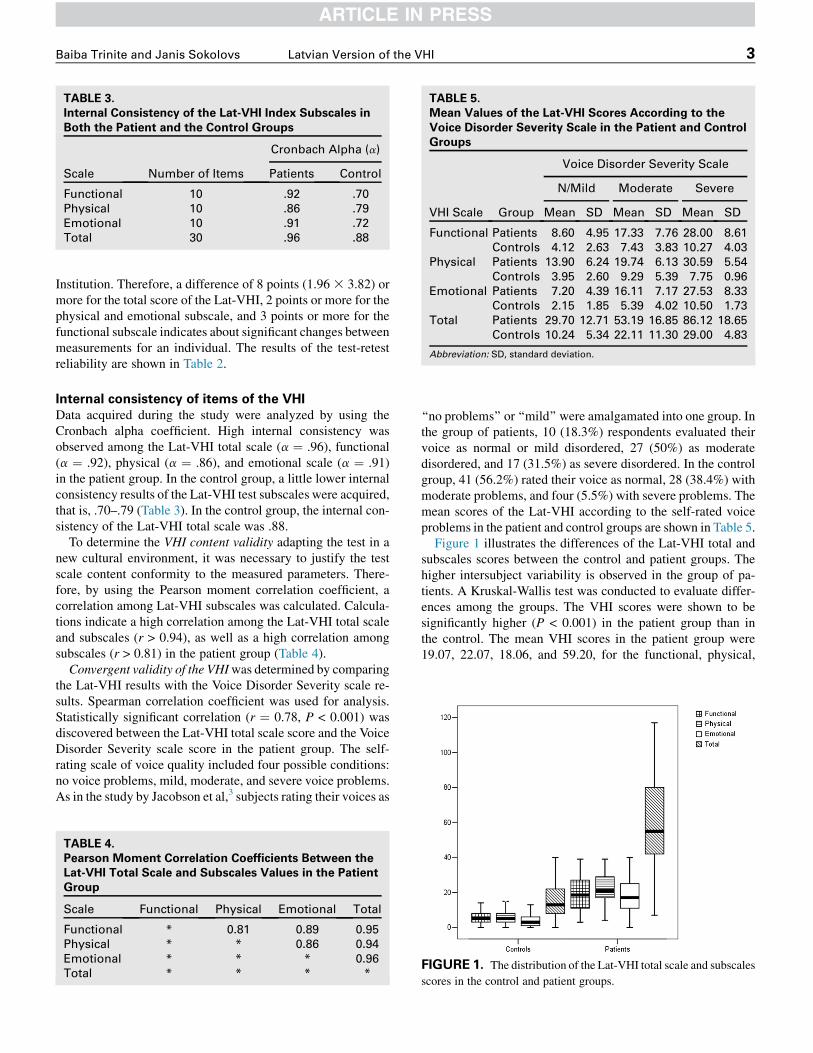
TABLE 3.
Internal Consistency of the Lat-VHI Index Subscales in
Both the Patient and the Control Groups
Scale Number of Items
Cronbach Alpha (a)
Patients Control
Functional 10 .92 .70
Physical 10 .86 .79
Emotional 10 .91 .72
Total 30 .96 .88
TABLE 5.
Mean Values of the Lat-VHI Scores According to the
Voice Disorder Severity Scale in the Patient and Control
Groups
VHI Scale Group
Voice Disorder Severity Scale
N/Mild Moderate Severe
Mean SD Mean SD Mean SD
Functional Patients 8.60 4.95 17.33 7.76 28.00 8.61
Controls 4.12 2.63 7.43 3.83 10.27 4.03
Physical Patients 13.90 6.24 19.74 6.13 30.59 5.54
Controls 3.95 2.60 9.29 5.39 7.75 0.96
Emotional Patients 7.20 4.39 16.11 7.17 27.53 8.33
Controls 2.15 1.85 5.39 4.02 10.50 1.73
Total Patients 29.70 12.71 53.19 16.85 86.12 18.65
Controls 10.24 5.34 22.11 11.30 29.00 4.83
Abbreviation: SD, standard deviation.
Baiba Trinite and Janis Sokolovs Latvian Version of the VHI 3
Institution. Therefore, a difference of 8 points (1.96 3 3.82) ormore for the total score of the Lat-VHI, 2 points or more for thephysical and emotional subscale, and 3 points or more for thefunctional subscale indicates about significant changes betweenmeasurements for an individual. The results of the test-retestreliability are shown in Table 2.
Internal consistency of items of the VHI
Data acquired during the study were analyzed by using theCronbach alpha coefficient. High internal consistency wasobserved among the Lat-VHI total scale (a ¼ .96), functional(a ¼ .92), physical (a ¼ .86), and emotional scale (a ¼ .91)in the patient group. In the control group, a little lower internalconsistency results of the Lat-VHI test subscales were acquired,that is, .70–.79 (Table 3). In the control group, the internal con-sistency of the Lat-VHI total scale was .88.
To determine the VHI content validity adapting the test in anew cultural environment, it was necessary to justify the testscale content conformity to the measured parameters. There-fore, by using the Pearson moment correlation coefficient, acorrelation among Lat-VHI subscales was calculated. Calcula-tions indicate a high correlation among the Lat-VHI total scaleand subscales (r > 0.94), as well as a high correlation amongsubscales (r > 0.81) in the patient group (Table 4).
Convergent validity of the VHIwas determined by comparingthe Lat-VHI results with the Voice Disorder Severity scale re-sults. Spearman correlation coefficient was used for analysis.Statistically significant correlation (r ¼ 0.78, P < 0.001) wasdiscovered between the Lat-VHI total scale score and the VoiceDisorder Severity scale score in the patient group. The self-rating scale of voice quality included four possible conditions:no voice problems, mild, moderate, and severe voice problems.As in the study by Jacobson et al,3 subjects rating their voices as
TABLE 4.
Pearson Moment Correlation Coefficients Between the
Lat-VHI Total Scale and Subscales Values in the Patient
Group
Scale Functional Physical Emotional Total
Functional * 0.81 0.89 0.95
Physical * * 0.86 0.94
Emotional * * * 0.96
Total * * * *
‘‘no problems’’ or ‘‘mild’’ were amalgamated into one group. Inthe group of patients, 10 (18.3%) respondents evaluated theirvoice as normal or mild disordered, 27 (50%) as moderatedisordered, and 17 (31.5%) as severe disordered. In the controlgroup, 41 (56.2%) rated their voice as normal, 28 (38.4%) withmoderate problems, and four (5.5%) with severe problems. Themean scores of the Lat-VHI according to the self-rated voiceproblems in the patient and control groups are shown in Table 5.
Figure 1 illustrates the differences of the Lat-VHI total andsubscales scores between the control and patient groups. Thehigher intersubject variability is observed in the group of pa-tients. A Kruskal-Wallis test was conducted to evaluate differ-ences among the groups. The VHI scores were shown to besignificantly higher (P < 0.001) in the patient group than inthe control. The mean VHI scores in the patient group were19.07, 22.07, 18.06, and 59.20, for the functional, physical,
FIGURE 1. The distribution of the Lat-VHI total scale and subscales
scores in the control and patient groups.
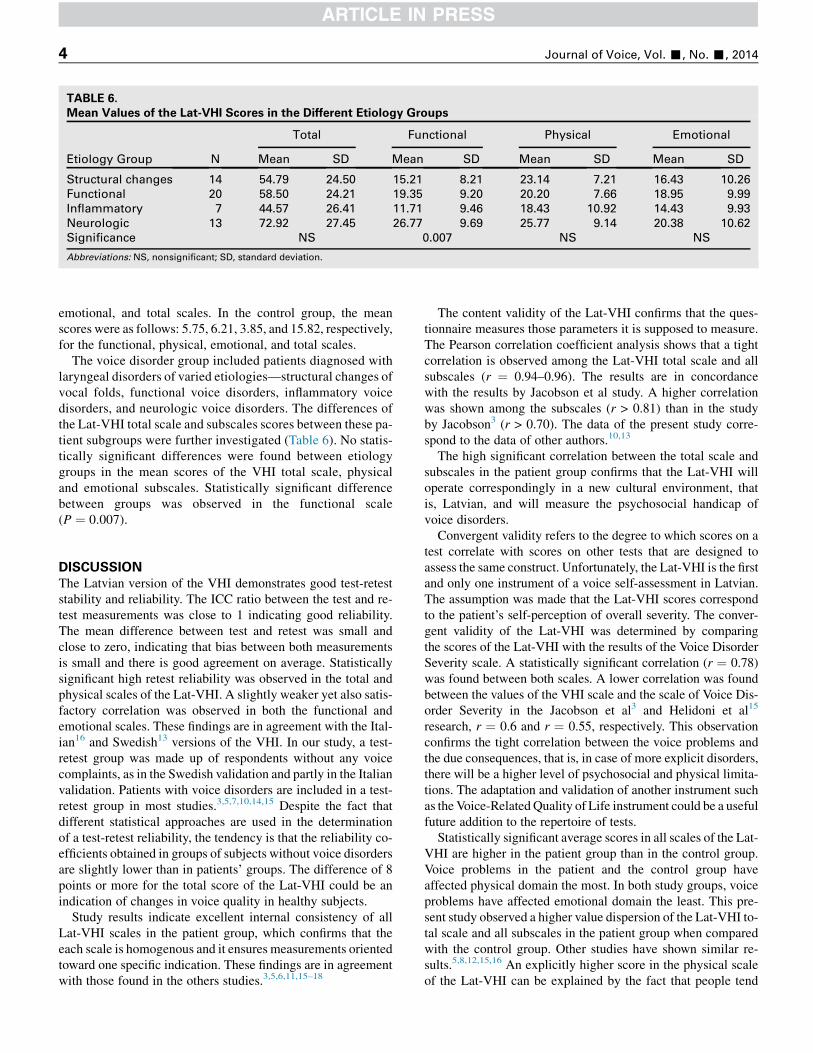
TABLE 6.
Mean Values of the Lat-VHI Scores in the Different Etiology Groups
Etiology Group N
Total Functional Physical Emotional
Mean SD Mean SD Mean SD Mean SD
Structural changes 14 54.79 24.50 15.21 8.21 23.14 7.21 16.43 10.26
Functional 20 58.50 24.21 19.35 9.20 20.20 7.66 18.95 9.99
Inflammatory 7 44.57 26.41 11.71 9.46 18.43 10.92 14.43 9.93
Neurologic 13 72.92 27.45 26.77 9.69 25.77 9.14 20.38 10.62
Significance NS 0.007 NS NS
Abbreviations: NS, nonsignificant; SD, standard deviation.
Journal of Voice, Vol. -, No. -, 20144
emotional, and total scales. In the control group, the meanscores were as follows: 5.75, 6.21, 3.85, and 15.82, respectively,for the functional, physical, emotional, and total scales.
The voice disorder group included patients diagnosed withlaryngeal disorders of varied etiologies—structural changes ofvocal folds, functional voice disorders, inflammatory voicedisorders, and neurologic voice disorders. The differences ofthe Lat-VHI total scale and subscales scores between these pa-tient subgroups were further investigated (Table 6). No statis-tically significant differences were found between etiologygroups in the mean scores of the VHI total scale, physicaland emotional subscales. Statistically significant differencebetween groups was observed in the functional scale(P ¼ 0.007).
DISCUSSION
The Latvian version of the VHI demonstrates good test-reteststability and reliability. The ICC ratio between the test and re-test measurements was close to 1 indicating good reliability.The mean difference between test and retest was small andclose to zero, indicating that bias between both measurementsis small and there is good agreement on average. Statisticallysignificant high retest reliability was observed in the total andphysical scales of the Lat-VHI. A slightly weaker yet also satis-factory correlation was observed in both the functional andemotional scales. These findings are in agreement with the Ital-ian16 and Swedish13 versions of the VHI. In our study, a test-retest group was made up of respondents without any voicecomplaints, as in the Swedish validation and partly in the Italianvalidation. Patients with voice disorders are included in a test-retest group in most studies.3,5,7,10,14,15 Despite the fact thatdifferent statistical approaches are used in the determinationof a test-retest reliability, the tendency is that the reliability co-efficients obtained in groups of subjects without voice disordersare slightly lower than in patients’ groups. The difference of 8points or more for the total score of the Lat-VHI could be anindication of changes in voice quality in healthy subjects.
Study results indicate excellent internal consistency of allLat-VHI scales in the patient group, which confirms that theeach scale is homogenous and it ensures measurements orientedtoward one specific indication. These findings are in agreementwith those found in the others studies.3,5,6,11,15–18
The content validity of the Lat-VHI confirms that the ques-tionnaire measures those parameters it is supposed to measure.The Pearson correlation coefficient analysis shows that a tightcorrelation is observed among the Lat-VHI total scale and allsubscales (r ¼ 0.94–0.96). The results are in concordancewith the results by Jacobson et al study. A higher correlationwas shown among the subscales (r > 0.81) than in the studyby Jacobson3 (r > 0.70). The data of the present study corre-spond to the data of other authors.10,13
The high significant correlation between the total scale andsubscales in the patient group confirms that the Lat-VHI willoperate correspondingly in a new cultural environment, thatis, Latvian, and will measure the psychosocial handicap ofvoice disorders.Convergent validity refers to the degree to which scores on a
test correlate with scores on other tests that are designed toassess the same construct. Unfortunately, the Lat-VHI is the firstand only one instrument of a voice self-assessment in Latvian.The assumption was made that the Lat-VHI scores correspondto the patient’s self-perception of overall severity. The conver-gent validity of the Lat-VHI was determined by comparingthe scores of the Lat-VHI with the results of the Voice DisorderSeverity scale. A statistically significant correlation (r ¼ 0.78)was found between both scales. A lower correlation was foundbetween the values of the VHI scale and the scale of Voice Dis-order Severity in the Jacobson et al3 and Helidoni et al15
research, r ¼ 0.6 and r ¼ 0.55, respectively. This observationconfirms the tight correlation between the voice problems andthe due consequences, that is, in case of more explicit disorders,there will be a higher level of psychosocial and physical limita-tions. The adaptation and validation of another instrument suchas theVoice-RelatedQuality of Life instrument could be a usefulfuture addition to the repertoire of tests.Statistically significant average scores in all scales of the Lat-
VHI are higher in the patient group than in the control group.Voice problems in the patient and the control group haveaffected physical domain the most. In both study groups, voiceproblems have affected emotional domain the least. This pre-sent study observed a higher value dispersion of the Lat-VHI to-tal scale and all subscales in the patient group when comparedwith the control group. Other studies have shown similar re-sults.5,8,12,15,16 An explicitly higher score in the physical scaleof the Lat-VHI can be explained by the fact that people tend

Baiba Trinite and Janis Sokolovs Latvian Version of the VHI 5
to associate physical manifestations of voice disorders withhow they perceive the current voice sounds, whereas functionallimitations and changes in emotional condition are related to alesser extent to perceptions of the current voice.
The Latvian version of the VHI is a statistically valid andreliable instrument to evaluate voice function and psychosocialimpact caused by the voice disorders in individual. The psy-chometric indications of the Latvian version of the VHI corre-spond to the psychometric indications of the original study byJacobson et al, as well as to the results acquired by other au-thors during test adaptation and validations. Individual VHI re-sults allow specialists to better understand motives behindlooking for help and illustrate limitation variations of activityand participation caused by the voice disorders in individual’slife.
CONCLUSIONS
The VHI is the first instrument of evaluation of bio-psychosocial consequences of voice disorders in Latvian.Latvian version of the VHI is a psychometrically validated in-strument whose indicators correspond to the psychometric in-dicators of the original sample. The VHI can be used in speechtherapists’ and physicians’ tools to evaluate the handicap ofvoice disorders.
REFERENCES1. Dejonckere PH, Bradley P, Clemente P, et al. A basic protocol for functional
assessment of voice pathology, especially for investigating the efficacy of
(phonosurgical) treatments and evaluating new assessment techniques.
Eur Arch Otorhinolaryngol. 2001;258:77–82.
2. Dejonckere P. Assessment of voice and respiratory function. In:
Remacle M, Eckel HE, eds. Surgery of larynx and trachea. Berlin, Heidel-
berg, Germany: Springer – Verlag; 2010:11–27.
3. Jacobson BH, Johnson A, Grywalski C, Silbergleit A, Jacobson G,
Benninger MS, Newman CW. The Voice Handicap Index (VHI): develop-
ment and validation. Am J Speech Lang Pathol. 1997;6:66–70.
4. Nawka T, Wiesmann U, Gonnermann U. Validierung des Voice Handicap
Index (VHI) in der deutschen Fassung. HNO. 2003;51:921–930 [in
German].
5. Lam PK, Chan KM, Ho WK, Kwong E, Yiu EM, Wei WI. Cross-cultural
adaptation and validation of the Chinese Voice Handicap Index–10. Laryn-
goscope. 2006;116:1192–1198.
6. Xu W, Han D, Li H, Hu R, Zhang L. Application of the Mandarin Chinese
version of the Voice Handicap Index. J Voice. 2010;24:702–707.
7. Woisard V, Bodin S, Puech M. The Voice Handicap Index: impact of the
translation in French on the validation. Rev Laryngol Otol Rhinol (Bord).
2004;125:307–312.
8. Guimar~aes I, Abberton E. An investigation of the Voice Handicap Index
with the speakers of Portuguese: preliminary data. J Voice. 2004;18:
71–82.
9. Pruszewicz A, Obrebowski A, Wiskirska-Woznica B, Wojnowski W. Com-
plex voice assessment—Polish version of the Voice Handicap Index (VHI).
Otolaryngol Pol. 2004;58:547–549.
10. HakkesteegtMM,WieringaMH, Gerritsma EJ, Feenstra L. Reproducibility
of the Dutch version of the Voice Handicap Index. Folia Phoniatr Logop.
2006;58:132–138.
11. Amir O, Ashkenazi O, Leibovitzh T, Michael O, Tavor Y, Wolf M.
Applying the Voice Handicap Index (VHI) to dysphonic and nondysphonic
Hebrew speakers. J Voice. 2006;20:318–324.
12. N�u~nez-Batalla F, Corte-Santos P, Senaris-Gonzalez B, Llorente-Pendas JL,
Gorriz-Gil C, Suarez-Nieto C. Adaptation and validation to the Spanish of
the Voice Handicap Index (VHI-30) and its shortened version (VHI-10).
Acta Otorrinolaringol Esp. 2007;58:386–392.
13. Ohlsson AC, Dotevall H. Voice Handicap Index in Swedish. Logoped Pho-
niatr Vocol. 2009;34:60–66.
14. Behlau M, Santos LMA, Oliveira G. Cross-cultural adaptation and valida-
tion of the Voice Handicap Index into Brazilian Portuguese. J Voice. 2011;
25:354–359.
15. Helidoni ME, Murry T, Moschandreas J, Lionis C, Printza A,
Velegrakis GA. Cross-cultural adaptation and validation of the Voice Hand-
icap Index into Greek. J Voice. 2010;24:221–227.
16. Schindler A, Ottaviani F, Mozzanica F, Bachmann C, Favero E, Schettino I,
Ruoppolo G. Cross-cultural adaptation and validation of the Voice Hand-
icap Index into Italian. J Voice. 2010;24:708–714.
17. Malki KH, Mesallam TA, Farahat M, Bukhari M, Murry T. Validation and
cultural modification of Arabic Voice Handicap Index. Eur Arch Otorhino-
laryngol. 2010;267:1743–1751.
18. Datta R, Sethi A, Singh S, Nilakantan A. Translation and validation of the
Voice Handicap Index in Hindi. J Laryngol Voice. 2011;1:12–17.
19. RankinG, StokesM. Reliability of assessment tools in rehabilitation: an illus-
tration of appropriate statistical analyses. Clin Rehabil. 1998;12:187–199.
20. Bland JM, Altman DG. Statistical methods for assessing agreement be-
tween two methods of clinical measurement. Lancet. 1986;1:307–310.
21. Rascevska M. Constructions and Adaptations of Psychological Tests and
Questionnaires. Riga, Latvia: RaKa; 2005:279.
22. Pring T. Research Methods in Communication Disorders. London; Phila-
delphia: Whurr Publishers; 2005.
23. Streiner DL, Norman GR. Health Measurement Scales: A Practical Guide
to Their Development and Use. 2nd ed. Oxford, UK: Oxford University
Press; 1995:104–127.
Journal of Voice, Vol. -, No. -, 20146
APPENDIX
The Voice Handicap Index (Latvian translation)
Instruction (in Latvian). �Sos apgalvojumus daudzi cilv�eki irlietoju�si, lai aprakst�ıtu savu balsi un t�as ietekmi uz vinu dz�ıvi.
F1 Mana balss ir iemesls tam, ka cilv�ekiem ir gr�uti sadzirdP2 Run�ajot man tr�ukst elpas.F3 Cilv�ekiem ir gr�ut�ıbas saprast mani trok�snain�a telp�a.P4 Manas balss skan�ejums main�as dienas laik�a.F5 Maniem tuviniekiem ir gr�uti sadzird�et mani, kad es sa
F6 Es ret�ak run�aju pa telefonu nek�a es grib�etu.E7 Run�ajot ar citiem, es esmu saspringts (-ta) savas balss
F8 Es izvairos no cilv�eku grup�am savas balss d�el.E9 �Skiet, ka mana balss kaitina cilv�ekus.P10 Cilv�eki jaut�a: ,,Kas noticis ar tavu balsi?’’
F11 Es ret�ak run�aju ar draugiem, kaiminiem un radiniekiem
F12 Cilv�eki l�udz man atk�artot teikto, kad m�es run�ajam tie�siP13 Mana balss skan �cerksto�si.P14 Man ir saj�uta it k�a man b�utu j�asasprindzin�as, lai veidoE15 Es esmu iev�erojis (-usi), ka citi cilv�eki nesaprot manas
F16 Balss gr�ut�ıbas ierobe�zo manu person�ıgo un sabiedrisk
P17 Manas balss skaidr�ıba ir iepriek�s neparedzama.
P18 Es m�eģinu p�arveidot savu balsi, lai t�a skan�etu cit�adi.F19 Sarunu laik�a es j�utos nenemts (-a) v�er�a savas balss d�eP20 Man ir stipri j�apiep�ulas, lai run�atu.P21 Mana balss ir slikt�aka vakar�a.F22 Man ir maz�akas darba iesp�ejas balss probl�emu d�el.E23 Manas balss probl�emas satrauc mani.
E24 Es esmu maz�ak komunikabls (-la), jo man ir balss prob
E25 Mana balss liek man justies nepilnv�ert�ıgam.
P26 Mana balss ,,aizl�ust’’ runas vid�u.E27 Mani kaitina, kad cilv�eki l�udz man atk�artot iepriek�s teik
E28 Es j�utos ne�erti, kad cilv�eki l�udz man atk�artot iepriek�s t
E29 Mana balss liek man justies nekompetentam (-tai).
E30 Es kaunos par savas balss probl�em�am.
Apvelciet to atbildi, kas nor�ada, cik bie�zi jums ir bijusi t�adapati pieredze.0-nekad 1-gandr�ız nekad 2-da�zreiz 3-gandr�ız vienm�er 4-
vienm�er.
�et mani. 0 1 2 3 4
0 1 2 3 4
0 1 2 3 4
0 1 2 3 4
ucu vinus cauri istab�am. 0 1 2 3 4
0 1 2 3 4
d�el. 0 1 2 3 4
0 1 2 3 4
0 1 2 3 4
0 1 2 3 4
savas balss d�el. 0 1 2 3 4
viens ar otru. 0 1 2 3 4
0 1 2 3 4
tu balsi. 0 1 2 3 4
balss probl�emas. 0 1 2 3 4
o dz�ıvi 0 1 2 3 4
0 1 2 3 4
0 1 2 3 4
l. 0 1 2 3 4
0 1 2 3 4
0 1 2 3 4
0 1 2 3 4
0 1 2 3 4
l�emas. 0 1 2 3 4
0 1 2 3 4
0 1 2 3 4
to. 0 1 2 3 4
eikto. 0 1 2 3 4
0 1 2 3 4
0 1 2 3 4




















![Computer development [Latvian]](https://img.pdfslide.net/doc/110x75/5568449fd8b42a26518b5035/computer-development-latvian.jpg)







