Embed Size (px)
Citation preview

ADRENAL INSUFFICIENCY IN CRITICALLY ILL PATIENTS
Dalal Abdelgadir R2 pediatics

Objectives
To review normal physiology of adrenal gland and glucocorticoids
Normal adrenal response to stress Adrenal insufficiency in critical illness:
pathophysiology and incidence Evidence of treatment with glucocorticoids Case presentation Recommendation for diagnosis and
management in adult patients

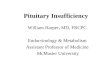
Physiology of the adrenal gland
CRH produced by hypothalamus
CRH stimulates pituitary gland to produce ACTH
ACTH stimulates adrenals to produce cortisol
Cortisol exerts a negative feedback on production of CRH and Cortisol

Zona fasiculata 75%
Zona Glomerulosa 15%
Zona reticularis 10%
mineralocorticoids
Stress cortisol, androgens
Basal cortisol, androgens

Production of steroid hormones

Physiology of glucocorticoids 90% bound to corticosteroid binding
globulin and albumin to a lesser extent 10% free cortisol is physiologically
active, half life is 70 -120 mins Cortisol is not stored in adrenal gland Glucocorticoids bind to intracelullar
receptors then moves into the nucleus affecting transcription of various genes

Physiology of glucocorticoidsMetabolic: Stimulates gluconeogenesis, decrease glucose
utilization Decreases protein synthesis and increases
catabolism Increases lypolysis and oxidation of fatty acidsCardiovascular: Increases blood pressure Increases sensitivity of vasculature to
catecholamines & angiotensin II

Physiology of glucocorticoids Anti-inflammatory effects: Reduces circulating T, B lymphocytes,
esinophils, monocytes and neutrophils at sites of inflammation
Decreases production of cytokines & chemokines
Increased production of microphage migration inhibitory factor
Increases red cell production

Adrenal insufficiency

Adrenal insufficiency
Primary adrenal insufficiency
Secondary adrenal insufficiency
Critical illness related corticosteroid
insufficiency

Primary adrenal insufficiency
Congenital:
CAH Adrenal hypoplasia
congenita Familial glucocorticoid
deficiency Adrenoleukodystroph
y Aldosterone
deficiency
Acquired:
Autoimmune Infectious
diseases Infiltrative
processes Drugs

Secondary adrenal insufficiencyCongenital ACTH,
CRH deficiency:
Isolated Panhypopituitaris
m Associated with
structural defects e.g. supra optic dyplasia
Acquired: Lymphocytic
hypophysitis Neoplasms Exogenous
steroids

Critical illness related GC insufficiency
Is inadequate cellular corticosteroid activity for the severity of the patients illness

Normal HPA response to stress Multiple changes occur to maintain
homeostasis during stress Activation of sympathoadrenal system
leading to secretion of epinephrine and norepinephrine
Activation of HPA axis lead to release of CRH, ACTH and eventually cortisol

Normal HPA response to stress Corticosteroid binding protein levels
fall as low as 50% leading to increase in free cortisol
Increased translocation of GR complexes into the nucleus
Results in alteration of systemic inflammatory response and cardiovascular function

Adrenal insufficiency - pathophysiology
Is inadequate cellular corticosteroid activity for the severity of patients illness
Dynamic process, patient may not have it on admission but develop it later
Poorly understood Structural damage to adrenal gland due
to hemorrhage or infarction may lead to long term AI

AI – pathophysiology
Most critically ill develop reversible HPA axis dysfunction
Decreased production of CRH, ACTH or cortisol Decrease and alterations of glucocorticoid
receptors Decrease nuclear translocation of glucocorticoid-
receptor complexes due to endotoxins and proinflammatory cytokines
Failure of activated GRs to down regulate production of inflammatory mediators (systemic inflammation-associated GC resistance)

Translocation inhibited by endotoxins and cytokines
Decreased or abnormal receptors
Failure of GR to down regulate proinflammatory factors
CRH
ACTH
cortisol

AI – pathophysiology
Some studies showed non survivors of severe sepsis have random cortisol level > 20 mcg/dl (552 nmol/l) but incremental increase < 9 (248) after ACTH stim test
Others found that non survivors had lower random cortisol level compared to survivors
Lower levels of cortisol and high ACTH associated with severe disease and poor outcome

When to suspect AI in critically ill pts
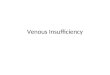
Shock poorly responding to fluids and vasopressors especially septic shock
Catecholamine-dependant shock Prolonged mechanical ventilation Sudden deterioration of seriously ill
patients with DIC, traumatic shock, severe burns or sepsis may be due to adrenal hemorrhage or infarction

Incidence of AI
Incidence variable within studies ranging 15 – 60%
Probably due to different definitions used, different study populations
Sarthi et al. assessed children with fluid refractory shock 30% of patients with septic shock identified
with AI ( increase < 9 (248) after low dose ACTH stim test)
Patients with AI had higher incidence of catecholamine refractory shock, but no difference in mortality

Incidence of AI
Hatherill et al. reported incidence of 52% in children with septic shock
Menon and Clarson reported 31% of critically ill
Menon conducted a study to determine beliefs and practices regarding AI revealed that 41% of endocrinologist thought it rarely or never happen in PICU setting, 81% of intensivists thought it sometimes or often happens

Diagnosis of AI
Different criteria in literature include: Delta cortisol after high dose ACTH stim
test < 9 (248) Baseline cortisol < 5 (138) Baseline cortisol < 7 (193) Basal cortisol< 20 (552), Delta cortisol < 9
(248) Delta cortisol < 9 (193) Peak < (baseline x 2)

Diagnosis of AI
Annane et al used metyrapone stim test to assess high dose ACTH stim test: Baseline < 10 (276) or delta cortisol < 9 (248) were
best predictors of adrenal insufficiency Best predictor of normal adrenal response is
baseline > 44 (1214) or increase > 17 (464) Metyrapone stimulation test: inhibits conversion
of 11 deoxycortisol to cortisol, leading to increase in 11 deoxycortisol and drop of cortisol
Low cortisol increases ACTH leading to further increase in 11 deoxycortisol

Diagnosis of AI
Currently based on random cortisol levels and delta cortisol after high dose ACTH stimulation test
Issues: Free cortisol is of more physiological importance but
normal levels in acute illness not established, test not widely available
Low dose ACTH stimulation test thought to be more physiologic and sensitive but limited data
Delta cortisol assess ability of adrenal cortex to produce cortisol but does not confirm integrity of HPA axis
Above tests do not evaluate resistance at end organ level

Should stress dose glucocorticoids be included in management of septic shock?

Rational behind treatment with GC Studies showing association between AI
and refractory shock Some studies showing favorable outcome
with administration of glucocorticoids In severe sepsis there is compromised
endothelial integrity, systemic vasoplegia and impaired cardiac contractility
Cortisol is thought to modulate biochemical pathways associated with those processes

Rational behind treatment with GC Adults with sepsis have different dose
response to norepinephrine compared to adults without sepsis
Marked improvement of dose response is seen after administration of GC
Down regulation of proinflammatory factors

Should we treat with glucocorticoids Menon survey based study revealed:
50% of Canadian intensivists would sometimes or often empirically treat hypotensive patients with glucocorticoids
81% of endocrinologist would never or occasionally recommend glucocorticoids

Should we treat with glucocorticoids Min et al. RCT of cortisol Vs placebo in
Dengue shock syndrome (1975) 48/98 received cortisol Fatality was 19% in cortisol group, 44% in
placebo group Sumarmo et al. studied treating with
cortisol (50 mg/kg single dose) in Dengue shock syndrome (1982) Mortality, length of shock, volume of fluid
resuscitation similar in both groups

Should we treat with GC
Tassinyom et al. RCT studied single dose methlprednisone Vs placebo in Dengue shock syndrome (1993) Similar rates of mortality and organ
dysfunction in both treatment and placebo groups
Slusher et al. studies administering dexamethasone 0.05 mg/kg/dose q 8hrs for 2 days (1996) No improved survival or time to
hemodynamic stability observed

Should we treat with GC
Markovitz et al. Retrospective cohort study using Pediatric Health information system database 2005 6693 children with severe sepsis Mortality 30% in those treated with steroids Mortality 18% in those not treated with
steroids Longer duration of inotropic support and
mechanical ventilation in steroid treated group
Limitation: no data on severity of illness

PALS algorithm for septic shock

Can we make conclusions?
Comparison of those studies difficult Small sample size Different definitions of adrenal
insufficiency Different indications for treatment Different steroid regimens

Downside of treating with GC Attenuating immunity and delaying
wound healing Hyperglycemia Adult data raised concerns of increase
risk of nosocomial infections, multiple organ dysfunctions
Possibly alteration of brain development e.g. neurodevelopmental outcome in neonates treated with dexamethasone for BPD

Downside of treating with GC Increased mortality and morbidity
associated with methylprednisone administration in traumatic brain injury
Increased mortality in ARDS patients started on steroids after 14 days of illness
Higher rates of neuromuscular weakness

Case presentation

Case presentation
14 yr old boy with Trisomy 21 Admitted to the PICU after cervical fusion
for atlantoaxial instability Presented with gradual decline of motor
function over 1.5 yrs No past hx of hypothyroidism, other
endocrinological disorders or exposure to exogenous steroids

Case presentation
Initial plan was to keep him intubated for 48 hrs post op
On POD 3 developed fever and increased ventilatory requirements
Later developed hypotension requiring fluid resuscitation and eventually vasopressors
Subsequently diagnosed with pneumonia and sepsis
Continued to be vasopressor dependant for 6 days
Adrenal insufficiency suspected

Case presentation
Random cortisol was 83 nmol/L (3) ACTH stimulation test:
Baseline cortisol: 95 nmol/L (3.4) At 30 min: 483 (17.5) Delta: 388 (14) At 60 min: 472 (17.1) Delta: 374 (13.5)

Case presentation
Received hydrocortisone: 80 mg/m2/day x 1 day then weaned gradually over 1week
Dramatic improvement, weaned off vasopressors within 24 hrs
Hydrocortisone gradually weaned

Case presentation
Course complicated by chylothorax and recurrent pneumonia leading to prolonged ventilation
Subsequently was difficult to wean off ventilator, failed extubation due to deconditioning of respiratory muscles
Tracheostomy preformed 4 months later still ventilator dependant
& G-tube fed Transferred to Bloorview hospital for
rehabilitation

More in the adult world
Recommendations for the diagnosis and
management of corticosteroid
insufficiency in critically ill adult
patients: Consensus statements from
and international task force by the
American College of Critical Care
Medicine

Recommendations for diagnosis and management in adults
Dysfunction if the HPA axis in critical illness is best described by the term critical illness related corticosteroid insufficiency
The terms absolute or relative adrenal insufficiency are best avoided in context of critical care
Diagnosed by delta cortisol < 9 mcg/dl after 250 mcg cosyntropin or random total cortisol of < 10 mcg/dl
Use of free cortisol can not be recommended at this time

Recommendations for diagnosis and management in adults
The ACTH stimulation test should not be used to identify those patients with septic shock or ARDS who should receive GC
Hydrocortisone should be considered in the management strategy of patients with septic shock, particularly those who have responded poorly to fluids and vasopressor agents (2B)

Recommendations for diagnosis and management in adults
Moderate dose GC should be considered in the management strategy of patients with early severe ARDS and before day 14 in patients with unresolved ARDS. The role of GC treatment in less severe ARDS and ALI is less clear (2B)
In patients with septic shock IV hydrocortisone should be given in a dose of 200 mg/day in 4 different doses or as bolus of 100 mg followed by a continuous infusion of 10 mg/hr (1B)

Recommendations for diagnosis and management in adults
The optimal duration of GC treatment in patients with septic shock and early ARDS is unclear. Patients with septic shock should be treated > 7days before tapering and those with ARDS > 14 days before tapering (2B)
GC treatment should be tapered slowly and not stopped abruptly (2B)
Treatment with fludrocortisone ( 50mcg PO OD) is considered optional
Dexamethasone is not recommended for treatment of septic shock or ARDS (1B)

Landmark studies in adults:
CORTICUS Double blinded, randomized, placebo
controlled multicentre study 500 patients with shock and evidence of
organ dysfunction attributable to shock were enrolled
Randomized to hydrocortisone or placebo 50 mg q6hrs IV x 5days 50 mg q12hrs x 3days 50mg q24hrsx 1day

CORTICUS - results
Results: More rapid resolution of shock in
treatment group No difference in 28 d mortality Higher incidence of new infections and
septic shock

Landmark studies in adults
Annane et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock
300 patients with refractory shock randomized to treatment with hydrocortisone 50mg IV q6hrs x 7days + oral fludracortisone 50 mg PO OD or placebo
30% decrease in mortality confined to the non-responder group

In summary
HPA activation necessary to help with adaptation to stress
There is evidence to support existence of adrenal insufficiency in critically ill patients
The clinical relevance of adrenal insufficiency in critically ill pediatric patients not clear
Safety and efficacy of steroid use in critically ill children is not proven
Wide practice variability exists Risks of adverse effects such as hyperglycemia,
nosocomial infections and myopathy/neuropathy are unknown

References
Recommendations for the diagnosis and management of corticosteroid insufficiency in critically ill adult patients: Consensus statements from an international task force by the American College of Critical Care Medicine, Crit Care Med 2008 Vol. 36, No. 6
Adrenal function in sepsis: The retrospective Corticus cohort study, Crit Care Med 2007 Vol. 35, No.
Endocrine Problems in Critically Ill Children, AACN Clinical Issues Volume 17, Number 1, pp. 66–78
A history of adjunctive glucocorticoid treatment for pediatric sepsis: Moving beyond steroid pulp fiction toward evidence-based medicine, Jerry J. Zimmerman, MD, PhD, FCCM, Pediatr Crit Care Med 2007 Vol. 8, No. 6
Adrenal status in children with septic shock using low-dose stimulation test, Manjunatha Sarthi, MD, Pediatr Crit Care Med 2007 Vol. 8, No. 1
Identification of adrenal insufficiency in pediatric critical illness, Kusum Menon, MD, MSc, FRCPC; Margaret Lawson, MD, MSc, FRCPC, Pediatr Crit Care Med 2007 Vol. 8, No. 3

THANK YOU