Embed Size (px)
Citation preview
Adrenal InsufficiencyAdrenal Insufficiency
UNC Internal Medicine Morning ReportUNC Internal Medicine Morning Report
June 28, 2010June 28, 2010
Edward L. Barnes, MDEdward L. Barnes, MD
Adrenal InsufficiencyAdrenal Insufficiency
Primary Adrenal Insufficiency is also known Primary Adrenal Insufficiency is also known as Addison’s Disease in honor of Dr. Thomas as Addison’s Disease in honor of Dr. Thomas AddisonAddison
Born in April 1793, at Long Benton, Born in April 1793, at Long Benton, Newcastle-upon-Tyne and died on June 29 Newcastle-upon-Tyne and died on June 29 1860, at 15 Wellington Villas, Brighton 1860, at 15 Wellington Villas, Brighton
Dr. Addison is also credited with the discovery Dr. Addison is also credited with the discovery of Pernicious Anemia of Pernicious Anemia
IntroductionIntroduction
Adrenocorticotropic Hormone (ACTH) is the Adrenocorticotropic Hormone (ACTH) is the major factor in the secretion of cortisol and major factor in the secretion of cortisol and androgenic steroids by the adrenal cortexandrogenic steroids by the adrenal cortex
ACTH secretion is regulated as a balance ACTH secretion is regulated as a balance between the stimulatory effects of CRH between the stimulatory effects of CRH (mediated by the CNS) and the negative (mediated by the CNS) and the negative feedback mediated by circulating levels of feedback mediated by circulating levels of glucocorticoidsglucocorticoids
Adrenal InsufficiencyAdrenal Insufficiency
Arises when cortisol levels are not sufficient to Arises when cortisol levels are not sufficient to meet the needs of the bodymeet the needs of the body
Cortisol aids in maintaining vascular tone, Cortisol aids in maintaining vascular tone, hepatic gluconeogenesis, and in maintaining hepatic gluconeogenesis, and in maintaining glycogenglycogen
Inadequate cortisol in times of stress can lead Inadequate cortisol in times of stress can lead to hypotension, shock, and hypoglycemiato hypotension, shock, and hypoglycemia
Adrenal InsufficiencyAdrenal Insufficiency
Mineralocorticoid deficiency typically leads to Mineralocorticoid deficiency typically leads to renal wasting of sodium, retention of renal wasting of sodium, retention of potassium, and reduced intravascular volumepotassium, and reduced intravascular volume
Primary Adrenal InsufficiencyPrimary Adrenal Insufficiency
Most commonly is of an autoimmune etiology, Most commonly is of an autoimmune etiology, resulting from chronic destruction of the adrenal resulting from chronic destruction of the adrenal cortexcortex
Typical histologic feature is lymphocytic infiltrationTypical histologic feature is lymphocytic infiltration Antibodies to adrenal cortical antigens are present Antibodies to adrenal cortical antigens are present
early in the disease processearly in the disease process Patients with autoimmune adrenal disease are more Patients with autoimmune adrenal disease are more
likely to have polyglandular autoimmune systems likely to have polyglandular autoimmune systems causing deficiency of other endocrine glandscausing deficiency of other endocrine glands
Primary Adrenal InsufficiencyPrimary Adrenal Insufficiency
Several Other Mechanisms Exist:Several Other Mechanisms Exist: Bilateral adrenal hemorrhageBilateral adrenal hemorrhage Infection: Tuberculosis, CMV, HistoplasmosisInfection: Tuberculosis, CMV, Histoplasmosis Metastatic DiseaseMetastatic Disease Deposition Diseases: Hemochromatosis, Amyloidosis, Deposition Diseases: Hemochromatosis, Amyloidosis,
SarcoidosisSarcoidosis Drug Induced: Ketoconazole, Etomidate, Rifampin, Drug Induced: Ketoconazole, Etomidate, Rifampin,
AnticonvulsantsAnticonvulsants Congenital Adrenal HyperplasiasCongenital Adrenal Hyperplasias
Secondary Adrenal InsufficiencySecondary Adrenal Insufficiency
Caused by pituitary failure of ACTH secretionCaused by pituitary failure of ACTH secretion Etiologies include:Etiologies include:
any cause of primary or secondary any cause of primary or secondary hypopituitarismhypopituitarism
Exogenous Glucocorticoid TherapyExogenous Glucocorticoid Therapy Megestrol, which has some glucocorticoid therapyMegestrol, which has some glucocorticoid therapy
Clinical PresentationClinical Presentation
Acute adrenal insufficiency (Adrenal Crisis) Acute adrenal insufficiency (Adrenal Crisis) should be expected in any patient acute, should be expected in any patient acute, unexplained volume depletion and shockunexplained volume depletion and shock
Hyperkalemia, acidosis, and hypoglycemia Hyperkalemia, acidosis, and hypoglycemia may also be accompanyingmay also be accompanying
Clinical PresentationClinical Presentation
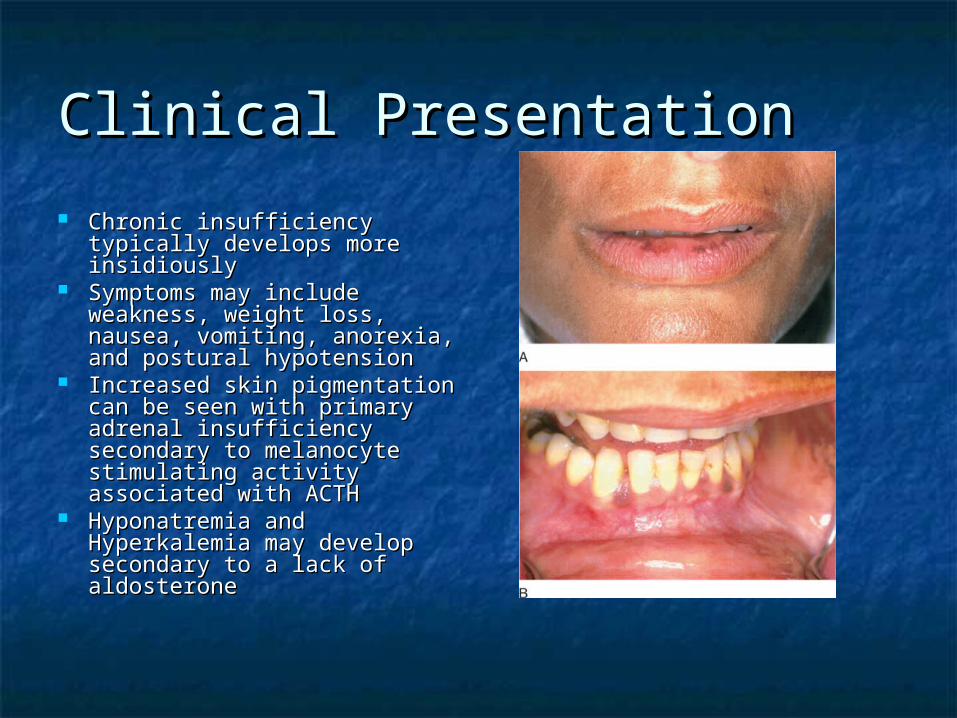
Chronic insufficiency typically Chronic insufficiency typically develops more insidiouslydevelops more insidiously
Symptoms may include Symptoms may include weakness, weight loss, nausea, weakness, weight loss, nausea, vomiting, anorexia, and postural vomiting, anorexia, and postural hypotensionhypotension
Increased skin pigmentation can Increased skin pigmentation can be seen with primary adrenal be seen with primary adrenal insufficiency secondary to insufficiency secondary to melanocyte stimulating activity melanocyte stimulating activity associated with ACTHassociated with ACTH
Hyponatremia and Hyperkalemia Hyponatremia and Hyperkalemia may develop secondary to a lack may develop secondary to a lack of aldosteroneof aldosterone
Clinical PresentationClinical Presentation
Secondary Adrenal Insufficiency may present Secondary Adrenal Insufficiency may present with evidence of adrenal insufficiency as well with evidence of adrenal insufficiency as well as other evidence of hypopituitarismas other evidence of hypopituitarism
Differential DiagnosisDifferential Diagnosis
Acute Adrenal insufficiencyAcute Adrenal insufficiency Various conditions can cause hypotension and or shockVarious conditions can cause hypotension and or shock
Chronic Adrenal InsufficiencyChronic Adrenal Insufficiency Chronic Starvation (anorexia nervosa)Chronic Starvation (anorexia nervosa) Gastrointestinal Disease secondary to inflammation or Gastrointestinal Disease secondary to inflammation or
malignancymalignancy Other causes of hyperpigmentation including drug Other causes of hyperpigmentation including drug
exposuresexposures Other causes of fatigue and malaiseOther causes of fatigue and malaise
Diagnostic WorkupDiagnostic Workup
Baseline Cortisol and ACTH levels should be Baseline Cortisol and ACTH levels should be obtained in the early morningobtained in the early morning A morning cortisol level of <3 A morning cortisol level of <3 g/dL is virtually g/dL is virtually
diagnosticdiagnostic A level of <10 A level of <10 g/dL is highly suspiciousg/dL is highly suspicious A level of >18 A level of >18 g/dL should rule out Adrenal g/dL should rule out Adrenal
Insufficiency except in the setting of a critically ill Insufficiency except in the setting of a critically ill patientpatient
Diagnostic WorkupDiagnostic Workup
Cosyntropin Stimulation TestCosyntropin Stimulation Test Measure morning cortisol level (pre-test level)Measure morning cortisol level (pre-test level) Administer 1 Administer 1 g dose Cosyntroping dose Cosyntropin Measure a second cortisol level 1 hour after Cosyntropin Measure a second cortisol level 1 hour after Cosyntropin
administrationadministration Normal response demonstrates a level of greater than 20 Normal response demonstrates a level of greater than 20 g/dL g/dL
after cosyntropinafter cosyntropin Patients with both primary and secondary adrenal insufficiency Patients with both primary and secondary adrenal insufficiency
will not demonstrate appropriate responsewill not demonstrate appropriate response Patients with primary insufficiency will fail to respond to Patients with primary insufficiency will fail to respond to
repeated administrations, however patients with secondary repeated administrations, however patients with secondary insufficiency may show an increased response to repeated insufficiency may show an increased response to repeated testing/stimulationtesting/stimulation
Diagnostic WorkupDiagnostic Workup
Further determination of primary vs. secondary Further determination of primary vs. secondary adrenal insufficiency will be based upon ACTH adrenal insufficiency will be based upon ACTH levellevel
High ACTH level expected in primary High ACTH level expected in primary insufficiencyinsufficiency
Treatment: Acute Adrenal Treatment: Acute Adrenal Insufficiency Insufficiency
Treat Acute Adrenal Insufficiency with Treat Acute Adrenal Insufficiency with Hydrocortisone 50-100 mg IV q8 hrsHydrocortisone 50-100 mg IV q8 hrs
In addition, volume resuscitate with Normal SalineIn addition, volume resuscitate with Normal Saline
Treatment: Chronic Adrenal InsufficiencyTreatment: Chronic Adrenal Insufficiency
Hydrocortisone 20-30 mg po dailyHydrocortisone 20-30 mg po daily Typically divide dose 2/3 in am, 1/3 in pmTypically divide dose 2/3 in am, 1/3 in pm
May use Prednisone 5 mg po daily instead May use Prednisone 5 mg po daily instead Fludrocortisone 0.05-0.1 mg po qam Fludrocortisone 0.05-0.1 mg po qam
Not necessary in patients with secondary adrenal Not necessary in patients with secondary adrenal insufficiencyinsufficiency
Provide instruction for periods of acute illness or Provide instruction for periods of acute illness or increased stressincreased stress

The EndThe End
References:References:
1. Pearce, JMS. Thomas Addison. J R Soc Med. 2004 June; 97(6): 297–300. 1. Pearce, JMS. Thomas Addison. J R Soc Med. 2004 June; 97(6): 297–300.
2. Ontjes, DA. Disorders of the Adrenal Cortex. Netter’s Internal Medicine, 22. Ontjes, DA. Disorders of the Adrenal Cortex. Netter’s Internal Medicine, 2ndnd ed. 2009; 321-4. ed. 2009; 321-4.
3. Adrenal Insufficiency. Little: Dental Management of the Medically Compromised Patient, 7th 3. Adrenal Insufficiency. Little: Dental Management of the Medically Compromised Patient, 7th eded. . 2007.2007.
4. Oelkers, W. Adrenal Insufficiency. N Engl J Med. 1996 Oct 17;335(16):1206-12.4. Oelkers, W. Adrenal Insufficiency. N Engl J Med. 1996 Oct 17;335(16):1206-12.