Embed Size (px)
Citation preview
POSTGRAD. MED. J. (1965), 41, 73
AGENESIS OF THE CORPUS CALLOSUM
J. N. HARCOURT-WEBSTER, M.A., M.B., B.Chir.*Junior Assistant Pathologist
J. H. RACK,'M.A., M.IB., B.Chir.Assistant Pathologist
Department of Pathology, University of Cambridge
COMPLETE or partial agenesis of the corpuscallosum is uncommon especially in adults;the incidence amongst patients in institutionswhere numerous air encephalograms are per-formed is 3% (Carpenter and Drukemiller,1953). Reil (1812) published the first reportof a case, describing the necropsy findings ina 30 year old woman of low mentality; furthercases discovered at necropsy were subsequentlyreported (Urquardth, 1880; Richter, 1886;Bruce, 1889; Dunn, 1889; Cameron, 1917;de Large, 1925). Baker and Graves (1933) re-viewed 83 cases, in a wide variety of age groups,first diagnosed at necropsy. The diagnosisduring life was first made by Davidoff andDyke (1934) using pneumo-encephalography;the pneumo-encephalographic features hadbeen observed by Guttman (1929) but theirsignificance was not appreciated until necropsyrevealed complete agenesis. Fukai, Oguma andSujiyama (1960) reviewed 187 cases of com-plete and partial agenesis; 130 cases were provenat necropsy, 57 diagnosed by pneumo-ence pha-lography only. Since their review a further22 cases have been reported, 7 diagnosed orconfirmed at necropsy, 15 diagnosed bypneumo-encephalography only.The function of the corpus callosum,
originally regarded as the seat of the soul(Mingazzini, 1922), has been much, discussedboth on the evidence from cases of completeand partial agenesis and from that followingsurgical division in man and experimentalanimals. No characteristic clinical syndromeaccompanies complete or partial agenesis of thecorpus callosum nor are there any specificneurological or psychiatric accompaniments.In some cases of congenital agenesis there areno readily detected deficiencies; the 25th suchcase, which is also the 17th asymptomatic adultwith complete agenesis, is here reported with ashort review of the literature.
*Present Address: Department of Pathology, Uni-versity of Edinburgh.
Case ReportA 65-year-old builder's labourer was admitted to
hospital with a three months history of flatulence andepigastric discomfort. He claimed to have been fitand well all his life, a statement corroborated by hisrelatives and medical records. Shortly before theonset of his symptoms, he had attended the Opth-almic Department with some loss of vision; this wasfound to be due to cataracts and he was awaitingtheir surgical removal at the time of admission.There was no relevant family history and no note-worthy abnormality of his central nervous system ormental state.A radiological diagnosis of carcinoma of the
stomach was made and substantiated at laparotomy.Sub-total gastrectomy was performed and the dia-gnosis confirmed histologically, but bronchopneu-monia supervened and he died on the fourth post-operative day.
NecropsyThere was no unusual feature at the site of the
Polya gastrectomy; there was no residual- tumour ormetastasis. The lungs showed the changes of bron-chopneumonia, confirmed histologically.
Brain (1173 g.): On removing the dura mater alarge volume of cerebro-spinal fluid escaped from acommon ventricle. There was no falx cerebri ortentorium cerebelli. The hemispheres were symmetri-cal and united along their supero-medial borders bya tough membrane (Fig. 1). The corpus callosum andseptum lucidum were absent, there being a widelypatent common ventricle (Fig. 2). On the inferioraspect, because of the absence of the anterior columnsof the fomix and the anterior commissure, there wasa free communication with the common ventricle(Fig. 3). There was no abnormality of the Circle ofWillis or cerebral arteries. The lateral surface of thehemispheres showed a normal sulcal and gyral pat-tern, whilst an anterior view similarly presented anormal contour.
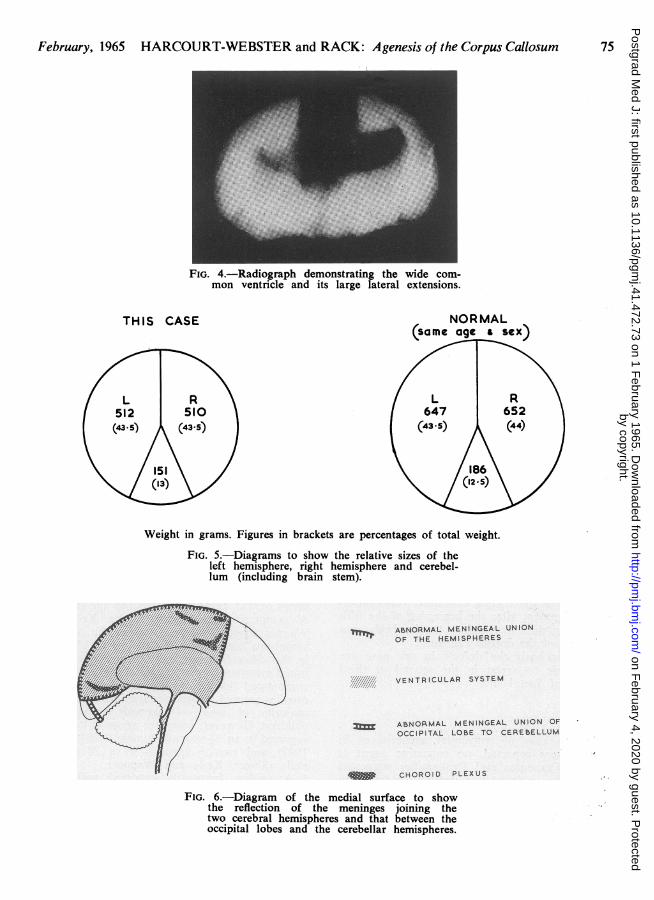
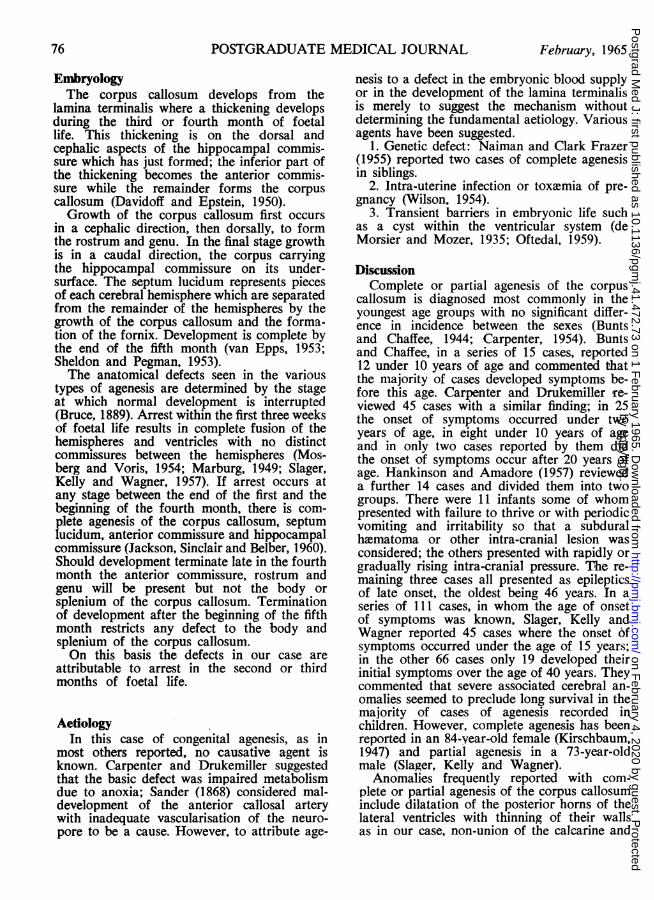
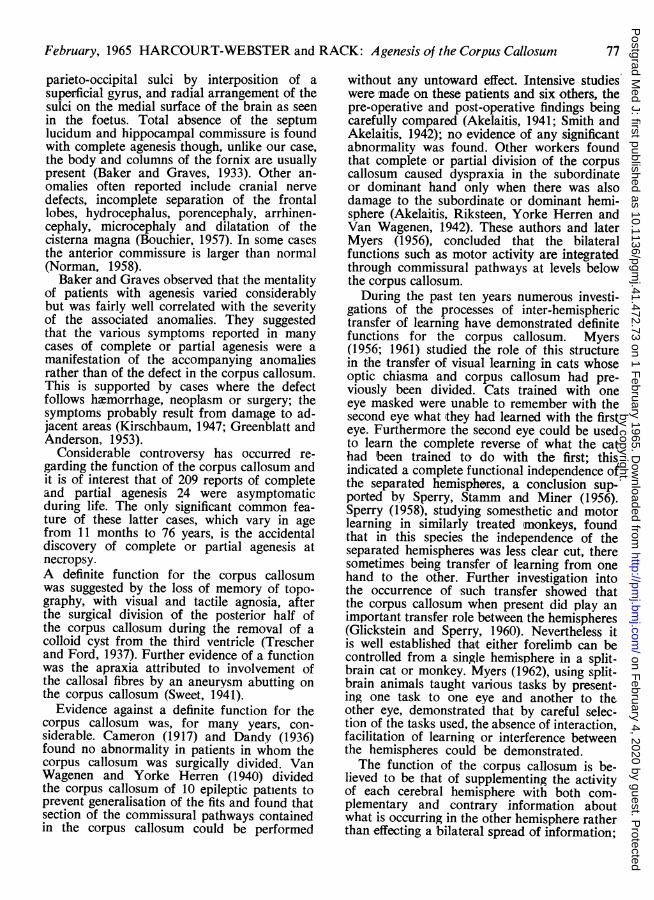
After fixation in 15% formol saline and radio-graphic examination (Fig. 4), the mid-brain wasdivided transversely and the cerebrum mid-sagitally.The pieces were weighed and compared with anothersimilarly divided brain from a man of similar ageand stature (Fig. 5). The lateral ventricles were largewith symmetrical dilatation of the anterior and post-erior horns; the inferior horns were absent. Whilstfragments of the choroid plexus were attached tothe medial surfaces of the hemispheres, no frag-ments were attached to the walls of the lateralventricles or their horns. An unusual reflection of themeninges joined the two cerebral hemispheres to-gether, whilst another shorter reflection connectedthe occipital lobes with the cerebellum (Fig. 6).
by copyright. on F
ebruary 4, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.41.472.73 on 1 F
ebruary 1965. Dow
nloaded from
POSTGRADUATE MEDICAL JOURNAL
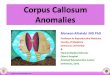
Cross section of this case. Cross section of normal brain.
FIG. 1.-Diagrammatic comparison of this case with the normal. The corpus callosum andseptum lucidum are absent, the two hemispheres being joined along their superomedialborders by a membrane.
FIG. 2.-View from above through the widelypatent common ventricle.
The cerebral hemispheres were cut into coronalslices 1 cm. thick; this revealed a considerable de-ficiency in the grey and white matter. The anteriorcommissure, forceps minor, septum lucidum, pinealbody, stria habenularis and the genu, body andsplenium of the corpus callosum were not found.With the exception of slightly raised areas at the site
L.M
FIG. 3.-View from below. This shows the freecommunication with the common ventricle dueto the absence of the anterior columns of thefomix and the anterior commissure.
of their attachments both the anterior and posteriorcolumns and the body of the fomix were also absent.The basal ganglia and the attachments of the cranialnerves, including the optic commisure and tracts,were normal.There was no abnormality on sectioning the mid-
brain, pons, medulla oblongata and cerebellum.
February, 196574by copyright.
on February 4, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.41.472.73 on 1 February 1965. D
ownloaded from
February, 1965 HARCOURT-WEBSTER and RACK: Agenesis of the Corpus Callosum 75
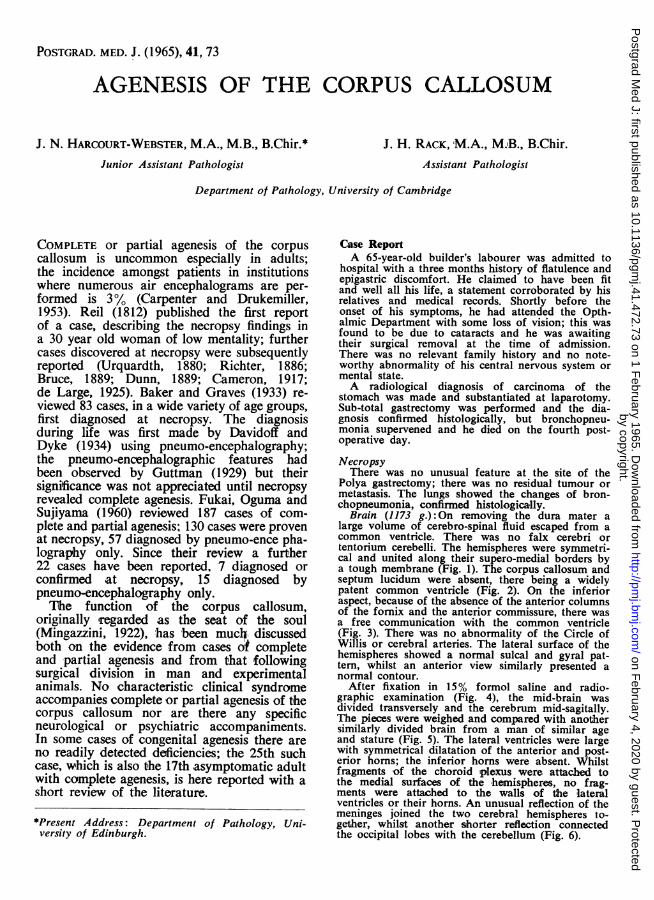
FIG. 4.-Radiograph demonstrating the wide com-mon ventricle and its large lateral extensions.
THIS CASE
L R512 510(43-5) (43.5)
151(13)
NORMAL(same age a sex)
L R647 652
(43-5) (44)
186 \\ /(12.5)\
Weight in grams. Figures in brackets are percentages of total weight.
FIG. 5.-Diagrams to show the relative sizes of theleft hemisphere, right hemisphere and cerebel-lum (including brain stem).
ASMiOMAL MINWOEA UNIONOF THE. HEMISPHERES -- .
VENTRICULAR SYSTEM
ASNOAMAL MENINGEAL UNION OFOCCIPITAL LOSE TO CEREbELLUM
CHOROID -PLEXUS
FIG. 6.-Diagram of the medial surface to showthe reflection of the meninges joining thetwo cerebral hemispheres and that between theoccipital lobes and the cerebellar hemispheres.
by copyright. on F
ebruary 4, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.41.472.73 on 1 F
ebruary 1965. Dow
nloaded from
POSTGRADUATE MEDICAL JOURNAL
EmbryologyThe corpus callosum develops from the
lamina terminalis where a thickening developsduring the third or fourth month of foetallife. This thickening is on the dorsal andcephalic aspects of the hippocampal commis-sure which has just formed; the inferior part ofthe thickening becomes the anterior commis-sure while the remainder forms the corpuscallosum (Davidoff and Epstein, 1950).Growth of the corpus callosum first occurs
in a cephalic direction, then dorsally, to formthe rostrum and genu. In the final stage growthis in a caudal direction, the corpus carryingthe hippocampal commissure on its under-surface. The septum lucidum represents piecesof each cerebral hemisphere which are separatedfrom the remainder of the hemispheres by thegrowth of the corpus callosum and the forma-tion of the fornix. Development is complete bythe end of the fifth month (van Epps, 1953;Sheldon and Pegman, 1953).The anatomical defects seen in the various
types of agenesis are determined by the stageat which normal development is interrupted(Bruce, 1889). Arrest within the first three weeksof foetal life results in complete fusion of thehemispheres and ventricles with no distinctcommissures between the hemispheres (Mos-berg and Voris, 1954; Marburg, 1949; Slager,Kelly and Wagner, 1957). If arrest occurs atany stage between the end of the first and thebeginning of the fourth month, there is com-plete agenesis of the corpus callosum, septumlucidum, anterior commissure and hippocampalcommissure (Jackson, Sinclair and Belber, 1960).Should development terminate late in the fourthmonth the anterior commissure, rostrum andgenu will be present but not the body orsplenium of the corpus callosum. Terminationof development after the beginning of the fifthmonth restricts any defect to the body andsplenium of the corpus callosum.On this basis the defects in our case are
attributable to arrest in the second or thirdmonths of foetal life.
AetiologyIn this case of congenital agenesis, as in
most others reported, no causative agent isknown. Carpenter and Drukemiller suggestedthat the basic defect was impaired metabolismdue to anoxia; Sander (1868) considered mal-development of the anterior callosal arterywith inadequate vascularisation of the neuro-pore to be a cause. However, to attribute age-
nesis to a defect in the embryonic blood supplyor in the development of the lamina terminalisis merely to suggest the mechanism withoutdetermining the fundamental aetiology. Variousagents have been suggested.
1. Genetic defect: Naiman and Clark Frazer(1955) reported two cases of complete agenesisin siblings.
2. Intra-uterine infection or toxemia of pre-gnancy (Wilson, 1954).
3. Transient barriers in embryonic life suchas a cyst within the ventricular system (deMorsier and Mozer, 1935; Oftedal, 1959).
DiscussionComplete or partial agenesis of the corpus
callosum is diagnosed most commonly in theyoungest age groups with no significant differ-ence in incidence between the sexes (Buntsand Chaffee, 1944; Carpenter, 1954). Buntsand Chaffee, in a series of 15 cases, reported12 under 10 years of age and commented thatthe majority of cases developed symptoms be-fore this age. Carpenter and Drukemiller re-viewed 45 cases with a similar finding; in 25the onset of symptoms occurred under twoyears of age, in eight under 10 years of ageand in only two cases reported by them didthe onset of symptoms occur after 20 years ofage. Hankinson and Amadore (1957) revieweda further 14 cases and divided them into twogroups. There were 11 infants some of whompresented with failure to thrive or with periodicvomiting and irritability so that a subduralhematoma or other intra-cranial lesion wasconsidered; the others presented with rapidly orgradually rising intra-cranial pressure. The re-maining three cases all presented as epilepticsof late onset, the oldest being 46 years. In aseries of 111 cases, in whom the age of onsetof symptoms was known, Slager, Kelly andWagner reported 45 cases where the onset ofsymptoms occurred under the age of 15 years;in the other 66 cases only 19 developed theirinitial symptoms over the age of 40 years. Theycommented that severe associated cerebral an-omalies seemed to preclude long survival in themajority of cases of agenesis recorded inchildren. However, complete agenesis has beenreported in an 84-year-old female (Kirschbaum,1947) and partial agenesis in a 73-year-oldmale (Slager, Kelly and Wagner).
Anomalies frequently reported with com-plete or partial agenesis of the corpus callosuminclude dilatation of the posterior horns of thelateral ventricles with thinning of their wallsas in our case, non-union of the calcarine and
76 February, 1965by copyright.
on February 4, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.41.472.73 on 1 February 1965. D
ownloaded from
February, 1965 HARCOURT-WEBSTER and RACK: Agenesis of the Corpus Callosum
parieto-occipital sulci by interposition of asuperficial gyrus, and radial arrangement of thesulci on the medial surface of the brain as seenin the foetus. Total absence of the septumlucidum and hippocampal commissure is foundwith complete agenesis though, unlike our case,the body and columns of the fornix are usuallypresent (Baker and Graves, 1933). Other an-omalies often reported include cranial nervedefects, incomplete separation of the frontallobes, hydrocephalus, porencephaly, arrhinen-cephaly, microcephaly and dilatation of thecisterna magna (Bouchier, 1957). In some casesthe anterior commissure is larger than normal(Norman, 1958).
Baker and Graves observed that the mentalityof patients with agenesis varied considerablybut was fairly well correlated with the severityof the associated anomalies. They suggestedthat the various symptoms reported in manycases of complete or partial agenesis were amanifestation of the accompanying anomaliesrather than of the defect in the corpus callosum.This is supported by cases where the defectfollows hemorrhage, neoplasm or surgery; thesymptoms probably result from damage to ad-jacent areas (Kirschbaum, 1947; Greenblatt andAnderson, 1953).
Considerable controversy has occurred re-garding the function of the corpus callosum andit is of interest that of 209 reports of completeand partial agenesis 24 were asymptomaticduring life. The only significant common fea-ture of these latter cases, which vary in agefrom 11 months to 76 years, is the accidentaldiscovery of complete or partial agenesis atnecropsy.A definite function for the corpus callosumwas suggested by the loss of memory of topo-graphy, with visual and tactile agnosia, afterthe surgical division of the posterior half ofthe corpus callosum during the removal of acolloid cyst from the third ventricle (Trescherand Ford, 1937). Further evidence of a functionwas the apraxia attributed to involvement ofthe callosal fibres by an aneurysm abutting onthe corpus callosum (Sweet, 1941).
Evidence against a definite function for thecorpus callosum was, for many years, con-siderable. Cameron (1917) and Dandy (1936)found no abnormality in patients in whom thecorpus callosum was surgically divided. VanWagenen and Yorke Herren (1940) dividedthe corpus callosum of 10 epileptic patients toprevent generalisation of the fits and found thatsection of the commissural pathways containedin the corpus callosum could be performed
without any untoward effect. Intensive studieswere made on these patients and six others, thepre-operative and post-operative findings beingcarefully compared (Akelaitis, 1941; Smith andAkelaitis, 1942); no evidence of any significantabnormality was found. Other workers foundthat complete or partial division of the corpuscallosum caused dyspraxia in the subordinateor dominant hand only when there was alsodamage to the subordinate or dominant hemi-sphere (Akelaitis, Riksteen, Yorke Herren andVan Wagenen, 1942). These authors and laterMyers (1956), concluded that the bilateralfunctions such as motor activity are integratedthrough commissural pathways at levels belowthe corpus callosum.During the past ten years numerouls investi-
gations of the processes of inter-hemispherictransfer of learning have demonstrated definitefunctions for the corpus callosum. Myers(1956; 1961) studied the role of this structurein the transfer of visual learning in cats whoseoptic chiasma and corpus callosum had pre-viously been divided. Cats trained with oneeye masked were unable to remember with thesecond eye what they had learned with the firsteye. Furthermore the second eye could be usedto learn the complete reverse of what the cathad been trained to do with the first; thisindicated a complete functional independence ofthe separated hemispheres, a conclusion sup-ported by Siperry, Stamm and Miner (1956).Sperry (1958), studying somesthetic and motorlearning in similarly treated (monkeys, foundthat in this species the independence of theseparated hemispheres was less clear cut, theresometimes being transfer of learning from onehand to the other. Further investigation intothe occurrence of such transfer showed thatthe corpus callosum when present did play animportant transfer role between the hemispheres(Glickstein and Sperry, 1960). Nevertheless itis well established that either forelimb can becontrolled from a single hemisphere in a split-brain cat or monkey. Myers (1962), using split-brain animals taught various tasks by present-ing one task to one eye and another to theother eye, demonstrated that by careful selec-tion of the tasks used, the absence of interaction,facilitation of learning or interference betweenthe hemispheres could be demonstrated.The function of the corpus callosum is be-
lieved to be that of supplementing the activityof each cerebral hemisphere with both com-plementary and contrary information aboutwhat is occurring in the other hemisphere ratherthan effecting a bilateral spread of information;
77
by copyright. on F
ebruary 4, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.41.472.73 on 1 F
ebruary 1965. Dow
nloaded from
78 POSTGRADUATE MEDICAL JOURNAL February, 1965
in persons with complete absence of the corpuscallosum the organisation of the brain is un-doubtedly very different from the normal butmuch work needs to be done in developingexperimental psychological tests on the linessuggested by animal experiments before defectsin inter-hemispheric transfer can be detected.
SummaryAgenesis of the corpus callosum is an un-
common abnormality; excluding the casereported, there are some 209 examples ofcomplete or partial agenesis in the literature.All age groups are represented but many casesare diagnosed in infancy or childhood becauseof severe symptoms or early death, both attri-buted to associated anomalies of the brain andnot to the defect in the corpus callosum. Thereis, however, a group of 25 asymptomatic casesof complete or partial agenesis; of these 17,including the present case, are adults withcomplete agenesis. The aetiology of most casesis unknown. The function of the corpus cal-losum is believed to be that of supplementingthe activity of each hemisphere with informa-tion from the other hemisphere rather thanbringing about a bilateral spread of informa-tion; tests for the detection of abnormalities ininter-hemispheric transfer have yet to beevolved.We wish to thank Mr. B. McN. Truscott for
permission to publish this case, the Department ofMedical Photography, The United Cambridge Hos-pitals for the illustrations, and Professors R. r. N.Greaves and G. L. Montgomery for their criticismand advice.
REFERENCESAKELAITIS, A. J. (1941): Studies on Corpus Cal-
losum. Higher Visual Functions in each Hom-onymous Field following Complete Section ofCorpus Callosum, Arch. Neurol. Psychiat.,(Chicago), 45, 788.
, RIKSTEEN, W. A., YORKE HERREN, R. andVAN WAGENEN, W. P. (1942): Studies on CorpusCallosum. Contribution to the Study of Dys-praxia and Apraxia following Partial andComplete Section of Corpus Callosum, ibid.,47, 971.
BAKER, R. C. and GRAVES, G. 0. (1933): PartialAgenesis of the Corpus Callosum, ibid., 29, 1054.
BOUCHIER, I. A. D. (1957): Agenesis of the CorpusCallosum, S. Afr. med. J., 31, 1220.
BRUCE, A. (1889): On the Absence of the CorpusCallosum in the Human Brain, Rep. Lab. R.Coll. Physicians Edinb., 1, 70.
BUNTS, A. T. and CHAFFEE, J. S. (1944): Agenesisof the Corpus Callosum with Possible Porence-phaly; Review of the Literature and Reportof a Case, Arch. Neurol. Psychiat., (Chicago),51, 35.
CAMERON, J. L. (1917): The Corpus Callosum:A Morphological and Clinical Study, Canad.med. Ass. J., 7, 609.
CARPENTER, M. B. (1954): Agenesis of CorpusCallosum: Study of 18 Cases Diagnosed duringLife, Neurology, 4, 200.
--, and DRUKEMILLER, W. H. (1953): Agenesisof the Corpus Callosum Diagnosed during Life,Arch. Neurol. Psychiat., (Chicago)., 69, 305.
DANDY, W. E. (1936): Operative Experience inCases of Pineal Tumours, Arch. Surg., 33, 19.
DAVIDOFF, L. M. and DYKE, G. A. (1934): Agene-sis of the Corpus Callosum: Diagnosis byEncephalography; Report of three cases, Amer.J. Roentgenol., 32, 1.
, and EPSTEIN, B. (1950): In 'The AbnormalPneumoencephalogram', 1st. ed. p. 429. Philadel-phia: Lea and Febiger.
DUNN, L. A. (1889): Case of Complete PrimaryAbsence of Corpus Callosum, Guy's Hosp. Rep.,46, 117.
VAN EPPS, E. F. (1953): Agenesis of the CorpusCallosum with Congenital Malformation in-cluding Atresias of Foramens of Luschka andMagendie, Amer. J. Roentgenol., 70, 47.
FUKAI, H., OGUMA, Y. and SUJIYAMA, Y. (1960):Agenesis of the Corpus Callosum: Report ofThree Cases and Review of the Literature, BrainNerve, 12, 772.
GLICKSTEIN, M. and SPERRY, R. W. (1960): In-termanual Transfer in Split-Brain Monkeys afterSomatic Cortical Ablation, Amer. Psychologist,15, 485.
GREENBLATT, J. and ANDERSON, C. (1953): PartialAgenesis of Corpus Callosum with Porence-phaly, Conn. State med. J., 17, 824.
GUTrMAN, L. (1929): Uber einen Falle von Ent-wicklungastorung des Gross-und Kleinhims mitBalkenmangel, Psychiat. neurol. Wschr., 31, 453.
HANKINSON, J. and AMADORE, L. V. (1957): Age-nesis of the Corpus Callosum Diagnosed byPneumo-encephalography, Brit. J. Radiol., 30,200.
JACKSON, F. E., SINCLAIR, J. and BELBER, C. J.(1960): Agenesis of the Corpus Callosum: ItsPneumo-encephalographic and AngiographicAppearance, Brit. nmed. J., ii, 42.
KIRSCHBAUM, W. R. (1947): Agenesis of the Corp-us Callosum and Associated Malformations, J.Neuropath., 6, 78.
DE LARGE, G. (1925): On Brains with Total andPartial Lack of Corpus Callosum and on Natureof Longitudinal Callosal Bundle, J. nerv. ment.Dis., 62, 449.
MARBURG, 0. (1949): $o-called Agenesia of theCorpus Callosum (Callosal Defect) AnteriorCerebral Dysraphism, Arch. Neurol. Psychiat.,(Chicago), 61, 297.
MINGAZZINI, G. (1922): Der Balken: Eine anato-mische, Physiopathogische and kilinische Studie,p. 212. Berlin: Springer.
DE MORSIER, G. and MOZER, J. J. (1935): Agen6sieComplete de la Commissure Calleuse et Troublesdu Development de 1'Hemisphere Gauche avecHemipar6sie Droite et Integrit6 Mentale, SchweizArch. Neurol. Psychiat., 35, 317.
MOSBERG, W. H. JR. and VORIS, H. C. (1954):Unusual Congenital Anomaly of Brain: Agenesisof Corpus Callosum, Absence of Septum Pellu-cidum and Fusion of Cerebral Hemisphere, J.Neuropath., 13, 369.
MYERS, R. E. (1956): Function of Corpus Callo-sum in Interocular Transfer, Brain, 79, 358.
by copyright. on F
ebruary 4, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.41.472.73 on 1 F
ebruary 1965. Dow
nloaded from
February, 1965 HARCOURT-WEBSTER and RACK: Agenesis of the Corpus Callosum 79
, (1961): Corpus Callosum and Visual Gnosis.In Brain, Mechanisms and Learning, ed. A.Fessard. Oxford: Blackwell.
, (1962): Transmission of Visual InformationWithin and Between the Hemispheres: A Be-havioural Study. In Interhemispheric Relationsand Cerebral Dominance, ed. V. B. Mountcastle,p. 51. Baltimore: Johns Hopkins.
NAIMAN, J. and CLARK FRAZER, F. (1955): Agenesisof Corpus Callosum: Report of Two Cases inSiblings, Arch. Neurol. Psychiat., (Chicago), 74,182.
NORMAN, R. M. (1958): In Neuropathology, ed.Greenfield, p. 320. London: Arnold.
OFTEDAL, S. I. (1959): Anomalies of the Mid-LineStructures of the Brain. Agenesis Corporis Cal-losi with a Mid-Line Cyst in One Case and aLipoma (?) in Another, Acta psychiat. scand.,34, 451.
REIL, J. C. (1812): Mangel des mittleren und freienTheils des Balkans in Menschengehion, Arch.Physiol., 11, 341.
RICHTER, A. (1886): Ueber die Windungen desMenschlichen Gehirns, Virchows Arch., 106, 380.
SANDER, J. (1886): Ueber Balkenmangel in Men-schlichen Gehim, Arch. Psychiat., 1, 229.
SHELDON, P. and PEGMAN, A. (1953): RadiologicalAppearances of Agenesis of Corpus Callosum,J. Neurol., 16, 117.
SLAGER, V. T., KELLY, A. B. and WAGNER, J. A.(1957): Congenital Absence of the Corpus Callo-sum: Report of a Case and Review of theLiterature, New Engl. J. Med., 256, 1171.
SMITH, K. U. and AKELAITIS, A. J. (1942): Studieson Corpus Callosum. Laterality in Behaviourand Bilateral Motor Organisation in Man Be-fore and After Section of the Corpus Callosum,Arch. Neurol. Psychiat., (Chicago), 47, 519.
SPERRY, R. W., STAMM, J. S. and MINER, NANCY(1956): Relearning Tests for Interocular Trans-fer Following Division of Optic Chiasma andCorpus Callosum in Cats, J. Comp. Physiol.Psychol., 49, 529.
, (1958): Corpus Callosum and Interhemi-spheric Transfer in the Monkey, Anat. Rec., 131,297.
SWEET, W. H. (1941): Sleeping Intracranial Ane-urysm Simulating Neoplasm: Syndrome ofCorpus Callosum, Arch. Neurol. Psychiat.,(Chicago), 45, 86.
TRESCHER, J. H. and FORD, F. R. (1937): ColloidCyst of the Third Ventricle: Report of a Case;Operative Removal with Section of the Post-erior Half of Corpus Callosum, ibid, 37, 959.
URQUHARDTH, A. R. (1880): Case of CongenitalAbsence of the Corpus Callosum, Brain, 3, 408.
VAN WAGENEN, W. P. and YORKE HERREN, R.(1940): Surgical Division of Commissural Path-ways in the Corpus Callosum: Relation toSpread of an Epileptic Attack, Arch. Neurol.Psychiat., (Chicago), 44, 740.
WILSON, S. A. K. (1954): In Textbook of Neurology,2nd. ed. vol. 11, p. 1255. London: Butterworth.
by copyright. on F
ebruary 4, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.41.472.73 on 1 F
ebruary 1965. Dow
nloaded from