Embed Size (px)
Citation preview
Clinical overview
An algorithm for the pharmacologicaltreatment of depression
Introduction
Antidepressants (ADs) are effective in the treat-ment of depression (1–7) but unfortunately non-response to treatment is a big clinical problem.Around 30% of the patients does not respond at alland another 30% responds only partially withoutreaching remission (8). This means that cliniciansare frequently confronted with the question �Whatto do next?� Several reviews have been published to
address this problem (9–16) with an abundantvariety of options. These include pharmacologicaloptions, other biological treatments such as elec-troconvulsive therapy (ECT), as well as psycho-therapeutic alternatives. A big variety can also befound in guidelines, which have been developed toassist clinicians in their treatment decisions byproviding the best available evidence for eachoption. Some of these guidelines contain treatmentalgorithms as an aid to help the clinician to choose
Spijker J, Nolen WA. An algorithm for the pharmacological treatmentof depression.
Objective: Non-response to treatment with antidepressants (AD) is aclinical problem.Method: The algorithm for pharmacological treatment of the Dutchmultidisciplinary guideline for depression is compared with four otheralgorithms.Results: The Dutch algorithm consists of five subsequent steps.Treatment is started with one out of many optional ADs (step 1); incase of non-response after 4–10 weeks, best evidence is for switching toanother AD (step 2); next step is augmentation with lithium as the bestoption (step 3); the next step is a monoamine oxidase inhibitor (MAOI)(step 4); and finally electroconvulsive therapy (step 5). There are majordifferences with other algorithms regarding timing of augmentationstep, best agents for augmentation and role of MAOI.Conclusion: Algorithms for AD treatment vary according to nationaland local preferences. Although the evidence for most of the treatmentstrategies is rather meagre, an AD algorithm appears to be an usefulinstrument in clinical practice.
J. Spijker1,2, W. A. Nolen3
1De Gelderse Roos, Mental Health Care, Ede, theNetherlands, 2Netherlands Institute of Mental Healthand Addiction, Utrecht, the Netherlands and3Department of Psychiatry, University Medical CenterGroningen, University of Groningen, Groningen, theNetherlands
Key words: major depressive disorder; treatmentalgorithm; antidepressants
Jan Spijker, Netherlands Institute of Mental Health andAddiction (Trimbosinstitute), PO Box 725, 3500 ASUtrecht, the Netherlands.E-mail: [email protected]
Accepted for publication September 23, 2009
Clinical recommendations
• Current antidepressant treatments strategies have only limited success in daily practice.• After failure of the first antidepressant, clinicians should adopt those treatment strategies that have
the best evidence: in addition to switching to another antidepressant, augmentation with lithium andswitching to a monoamine oxidase inhibitor.
• An algorithm is a strategy to deliver the best quality of care.
Additional comments
• This review, although comprehensive, does not cover the complete literature on antidepressanttreatment.
• More research into the usefulness of an antidepressant algorithm in the treatment of depression isneeded.
Acta Psychiatr Scand 2010: 121: 180–189All rights reservedDOI: 10.1111/j.1600-0447.2009.01492.x
� 2009 John Wiley & Sons A/S
ACTA PSYCHIATRICASCANDINAVICA
180

between the various options. Such algorithms canbe considered as a strategy to deliver step by stepthe most effective care (12).Medication algorithms are presented as decision
trees for medication management in subsequenttreatment steps. Some of the algorithms alsocontain decisions points that ensure proper evalu-ation at timely intervals (17). In possibly the firstalgorithm for the treatment of depression (18),recommended subsequent steps, each lasting4–6 weeks, were: step 1, an AD; step 2, switch toanother AD followed by lithium augmentation;step 3, a monoamine oxidase inhibitor (MAOI)and step 4, ECT. Since then, several other algo-rithms have been developed with similarities butalso differences.In this study, we will present the medication
algorithm for the treatment (in primary care as wellas specialised mental health care) of non-psychoticmajor depressive disorder (MDD) of the currentDutch multidisciplinary guideline for depressionand compare it with other medication algorithmsfor depression. Both authors were involved in thedevelopment of this guideline: the version of 2005(19, WAN) and the update of 2009 (20, JS).Before discussing the algorithms we will briefly
review the available evidence of the efficacy ofpharmacological treatments for the non-psychoticmajor depressive episode of unipolar MDD ofpatients who have not responded to the first AD.We will not discuss psychotherapy at length but wewill consider the indications for AD therapy vs.psychotherapy. Recent publications state that as aresult of publication bias, the efficacy of ADs isoverestimated (21) and that the difference betweenADs and placebo becomes only manifest andclinically relevant in severe depression (22). Onthe other hand, there is good evidence for psycho-therapy, especially cognitive behavioural therapy,also in severe depressive episodes (23–25). There-fore, we (and the Dutch guideline) recommendrestricting the indications for AD therapy in out-patient care to patients with at least moderatesevere depressive episodes. Psychotherapy is alsoan option for these patients and the choice foreither form of therapy or their combinationdepends on illness characteristics, past treatmenthistory and patient�s preferences.
Aims of the study
The primary aim of the study was to demonstratean algorithm for pharmacological treatment ofMDD and to compare this algorithm with othermedication algorithms. A secondary aim wasto illustrate the differences in these medication
algorithms so that clinicians realise that algorithmsdo not only reflect scientific evidence but also localand national preferences and routines.
Material and methods
For the review part of this study, we used theliterature searches that were performed for themost recent (2009) update of the Dutch multidis-ciplinary guideline for depression, with the searchterms (major) depression, ADs and the limits meta-analysis, systematic review and randomised con-trolled trial (RCT). Searches were performed inPsycINFO, Medline, Cochrane, Embase databasesuntil June 2008. Via the relevant articles we foundother articles from the reference lists. We referredto other guidelines and finally we used additionalpapers we were aware of. All the literature wasassessed. To weigh the evidence we used thefollowing method: Level A1: Systematic review;Level A2: Randomised double blind controlledtrial of good quality; Level B: Controlled studies oflower quality; Level C: Uncontrolled studies; andLevel D: Expert opinion;To find the guidelines and algorithms, we
searched in the same databases on these terms incombination with ADs.
Results
Antidepressants are effective drugs for the treat-ment of MDD, although their efficacy comparedwith placebo is only moderate (1–7). In the majormeta-analyses, mostly based on industry-spon-sored RCTs, response rates to ADs (most oftendefined as a reduction of at least 50% on adepression rating scale when compared with base-line) are nowadays around 50%. This is lower thanwhat was obtained between the 1960s and 1980s,possibly as a result of the inclusion of manypatients who had already received other treat-ments, including ADs, prior to their participationin RCTs.
The first step
In choosing an AD as a first step in treatment,there is ample choice. Several meta-analyses com-pared selective serotonin reuptake inhibitors(SSRIs) with tricyclic antidepressants (TCAs) (1,2), compared ADs in subgroups and treatmentsettings such as primary care (3), compared SSRIswith serotonine–norepinephrine reuptake inhibi-tors (SNRIs) (4) or mirtazapine (5) or comparedSSRIs with various others drugs including MAOIsand bupropion (a norepinephrine and dopamine
Algorithm for the pharmacological treatment of depression
181

reuptake inhibitor) (6). The conclusion from thesemeta-analyses is that the efficacy of the variousADs in out-patients is about equal. Only inhospitalised patients TCAs have been found moreeffective than SSRIs (2, 4). On the other hand,SSRIs have a statistically significant although verysmall and therefore probably clinically irrelevantadvantage over TCAs in overall discontinuationrates and tolerability (5–7).In conclusion, these results indicate that in
primary care as well as in secondary care (psychi-atric out-patients) SSRIs, the other novel ADssuch as SNRIs, mirtazapine, bupropion and stillalso the TCAs are good options in the first step(1–7). Thus, the choice could be based on otherissues such as patients characteristics (includingtreatment history), costs (the TCAs are the cheap-est drugs), and patient�s preference, for instancebased on the anticipation of specific adverse effects.Nevertheless, the SSRIs are the most frequentlyprescribed ADs in the first step in treatment.In case of non-response to the first AD, the first
action should be to re-evaluate the diagnosis (e.g. isthe diagnosis correct? and is there psychiatric orsomatic comorbidity?) and to check whether thepatient uses concomitant medication or othersubstances that may cause the depression andwhether there are adverse environmental situationsor negative life events (10–12). Compliance withthe medication should be also be discussed as manydepressed patients do not take their medication asprescribed, often because of (the fear of) adverseeffects (26). Finally, psycho-education aboutdepression and therapy is very helpful for thepatient to acknowledge and understand the illnessand to accept treatment (11).
What to do in the second step?
The most commonly used strategies after non-response to a first AD are: continuation of the ADat the same or at a higher dose, switching toanother AD, or augmentation of the AD with asecond drug, including adding a second AD. Allthese options are only weakly supported byevidence (9–16).
Continuation of treatment
Regarding continuation of treatment beyond4 weeks, we are not aware of any RCT thatsystematically addressed the question how long atrial with an AD should be before deciding to go tothe next step in treatment. There is some generalconsensus to wait for at least 4 weeks (with anadequate dosage) (27), with the option to extend
the trial to 6 weeks in case of some improvement(partial response) at week 4 (28) or to 10 weeks incase of combination treatment with psychotherapy(9). However, other authors recommended to waitfor 8 or even 12 weeks, such as in the USSequenced Treatment Alternatives to RelieveDepression (STAR*D) study, which evaluated theefficacy of a four-step treatment algorithm witheach step lasting 12 weeks (29).
Dose increase
In clinical practice, most clinicians continue treat-ment beyond 4–6 weeks in combination with doseincrease, sometimes even beyond the officiallyrecommended maximal dose. In a study byFredman et al. (30), 80% of the therapists choosedose escalation when response to a SSRI wasunsatisfactory. However, evidence is lacking forthis approach. A systematic review of seven RCTswith SSRIs involving 3086 patients addressed thisquestion (31). Four of these RCTs found no effectof dose escalation before week 4. In one trial doseescalation to 200 mg ⁄day of sertraline after6 weeks was even less effective than continuingtreatment at a dose of 100 mg ⁄day (32). In the twoother trials dose escalation of fluoxetine to60 mg ⁄day after 8 weeks was evaluated. In onetrial (33) dose increase was significantly moreeffective compared with augmentation with lithiumand desipramine in partial responders tot fluoxe-tine 20 mg; while in non-responders dose increaseand augmentation with lithium were both moreeffective than augmentation with despiramine.However, in a replication study (34), these effectswere not confirmed. In a recent RCT with 60 non-responding patients to paroxetine 20 mg, no effectof dose escalation tot 30–50 mg was found whencompared with placebo dose escalation (35).There are no trials in which dose escalation has
been compared with switching to another thera-peutic class of ADs. While there is thus no evidencefor dose escalation with regard to the SSRIs (31,35, 36), dose escalation with other ADs can beindicated, such as with TCAs (to optimise plasmalevels) and with venlafaxine which acts as a SSRI atlower doses, but as an SNRI at higher doses (37).
Switching
Switching to another AD is another widelypractised approach (38) and there are severaloptions. A recent systematic review found eightRCTs (39). Three RCTs with 641 patientsaddressed the efficacy of switching to a secondSSRI. Response rates varied between 17.6% and
Spijker and Nolen
182
70% and especially patients who were intolerantto the first SSRI could profit from a second SSRI.Regarding switching to a TCA, two RCTs with337 patients were found. Overall response ratesvaried between 16.5% and 48.5%, with lowerresponse rates for more treatment-resistantpatients. In four other RCTs, 1493 patients wereswitched to novel agents (mirtazapine, nefazodoneor venlafaxine). Response rates to the new drugvaried from 28% to 50% in patients withoutobvious treatment resistance while response ratesdropped in more resistant patients. Pooling resultsof three RCTs in which switch to venlafaxine wascompared with switch to another SSRI, showed amodest and clinically equivocally advantage forvenlafaxine (number needed to treat, NNT = 13;95% CI 9.1–25.0). In the STAR*D study, a switchfrom citalopram to bupropion with a responserates of 26.1%, was performed (40). Finally, onedouble blind and one open RCT (with 26 and 21patients) evaluated the switch to the MAOItranylcypromine with response rates of 42.9%and 45.5%, both being significantly more effectivethan control treatments (41). This positive resultwas different from the STAR*D study (109patients), in which only 12% responded, notbeing different from a control combination treat-ment (42) but the low response to tranylcypro-mine may be explained by the low mean dose of37 mg (43). Other MAOIs have also been studiedin resistant patients, such as phenelzine which wasnot found to differ from tranylcypromine regard-ing effect or tolerance (44).
Augmentation and combination
The third major option is to combine two treat-ments by adding a second drug (augmentation) toenhance the overall AD response or by combiningtwo ADs from the start of treatment (13–16). Inthis study, we only discuss the major augmentationand combination strategies: with lithium, thyroidhormone, buspirone, pindolol, other ADs and(atypical) antipsychotics (AAP).The best-documented augmentation strategy is
with lithium. In a recent meta-analysis of 10 RCTsinvolving 269 patients with mostly unipolar MDD,lithium was found superior to placebo with a meanresponse rate for lithium of 41.2% and for placeboof 14.4%, corresponding with a NNT of 3.7 (45).In most of the studies lithium was augmented to aTCA; the efficacy of lithium augmentation to aSSRI or other ADs is less well documented.A limitation of the studies was that half of themlasted shorter than 3 weeks while only one lasted6 weeks.
Augmentation with thyroid hormone (T3) isanother option. A meta-analysis involving eightstudies with 292 depressed unipolar but alsobipolar depressed patients (46) demonstrated itsefficacy with a relative response of 2.09 (95% CI1.31–3.32) and a NNT of 4.3. There was significantheterogeneity in the response rates among thetrials. When only RCTs were included in thepooled analysis, the relative response decreased to1.53 (95% CI 0.70–3.35) and this effect was notsignificant anymore (P = 0.29). Major limitationsof the studies are that T3 augmentation has beenstudied only in patients treated with a TCA andthat the studies did not last longer than 6 weeks(47).In the STAR*D study lithium augmentation was
compared with T3 augmentation in 127 patients.Both drugs were added to various medications(bupropion, sertraline, venlafaxine, citalopram,citalopram + bupropion or citalopram + buspi-rone). Remission was obtained with lithium in16% and with T3 in 25%, response in 16% and23% (not significant) (48). In only 57% of thepatients plasma levels of lithium were obtainedresulting in a mean plasma level of 0.6 mmol ⁄ l,indicating that many patients received probablytoo low dosages of lithium.Augmentation with buspirone was studied in
three RCTs, yielding a negative result in a placebocontrolled study with 119 patients (49) and a trendfavouring buspirone in a double blind study of 102SSRI non-responders (50) and a response of 27%for augmentation of buspirone to citalopram(compared with 32% for augmentation withbupropion) in 565 patients of the STAR*Dstudy (51).Selective serotonin reuptake inhibitors augmen-
tation with pindolol was studied in nine RCTs with594 patients. In five studies, pindolol augmentationwas used to speed up the response of the SSRI witha positive result at 2 weeks. In seven studiesresponse at 4–6 weeks was measured and thenthere was no advantage for augmentation withpindolol (52).Augmentation of a SSRI with an AD with
another pharmacological working mechanism (ortheir combination from the start of treatment) hasbeen studied in nine RCTs. Three studies with 430patients addressed mianserin. In one study aug-mentation with mianserin to fluoxetine was moreeffective than continuation of fluoxetine, and notdifferent from switching to mianserin (53) andanother study found that the combination offluoxetine and mianserin was more effective thanfluoxetine alone and not different from the combi-nation of fluoxetine plus pindolol (54). In a third
Algorithm for the pharmacological treatment of depression
183
study augmentation with mianserin to sertraline100 mg was not different form continuation ofsertraline, while both strategies were more effectivethan sertraline increased to 200 mg ⁄day (32).Augmentation with mirtazapine was studied in
non-responders to SSRIs (n = 22), venlafaxine(n = 3) or bupropion (n = 1) (55). In this smallstudy, mirtazapine augmentation was superior toaugmentation with placebo.The evidence for augmenting with a TCA is
doubtful. In one RCT, 41 patients non-responsiveto 8 weeks treatment with fluoxetine 20 mg ⁄daywere randomised to continuation of fluoxetine60 mg, to augmentation with lithium and toaugmentation with desipramine, with betterresponse rates for dose escalation of fluoxetine inpartial responders and for dose escalation offluoxetine and augmentation to lithium in non-responders (33). In a replication study with 101patients, no differences were found between similartreatment arms (34). However, another studyfound higher remission rates for the desipra-mine ⁄fluoxetine combination vs. monotherapywith either agent in 39 treatment-resistantin-patients (56).The combination of bupropion and citalopram
was more effective then bupropion alone in a RCTwith 61 patients (57).In the STAR*D study, 565 patients who had not
responded to citalopram were randomly assignedto augmentation with bupropion or buspirone.Remission rates were both 30% with bupropionand buspirone and response rates were 32% and27% respectively (not significant) (51).Augmentation with AAPs (olanzapine, quetia-
pine or risperidone) has been studied in 10 RCTswith in total 1500 patients (58). After pooling ofthe results, patientswith augmentationwith anAAPwere more likely to experience remission [Relativerisk (RR) = 1.75, P < 0.001] or clinical response(RR = 1.35, P = 0.001) than patients whoreceived adjunctive placebo. However, the rate ofdiscontinuation because of adverse events wasmore than three-fold higher among patients treatedwith AAPs than placebo. Two nearly identicalRCTs with together 743 non-responders to at leastone AD trial, proved efficacy of augmentation witharipiprazol with a treatment effect size of, respec-tively, 0.35 (59) and 0.39 (60) and low discontin-uations rates because of adverse effects (3.7%)respectively (2.2%).
Non-pharmacological alternatives
Electroconvulsive therapy has been reviewed by theUK ECT Review group (61) and proved to be
efficacious, and even more effective than pharma-cotherapy with a standardised effect size of )0.80(95% CI )1.29 to )0.29). Bilateral ECT is moreeffective than unilateral (standardised effect size)0.32; 95% CI )0.46 to )0.19) and high dose ECTled to a greater reduction in depressive symptomsthan low dose (mean change Hamilton depressionrating scale 4.1 points (95% CI 2.4–5.9).
The Dutch algorithm
Step 1: There is sufficient evidence that ADs areeffective in moderate to severe MDD and there isno preferred first choice AD (level A1). The choiceof the AD (a SSRI, a TCA, a SNRI, mirtazapine orbupropion) should depend on adverse reactionsprofile, patients� characteristics (including treat-ment history) and preferences. For hospitalisedpatients, treatment with a TCA is preferred but aSNRI is also an option (level A1).There is no evidence for dose escalation with a
SSRI in the first step (level A1). Prolongingtreatment at the same dose after 4 weeks is possiblebut there are not much data to support thisstrategy. On the contrary, recent data give evidencefor a rapid onset of action of SSRIs (62). Forclinical practice we would suggest that prolongingtreatment with the first SSRI to 6 (or even10 weeks) is an option only in case of some ⁄partialresponse. Especially patients with chronic depres-sion could improve with this longer treatmentperiod (63). In case of non-response with a TCA,dose adjustment with control of serum levels isadvised.Step 2: In case of non-response after 4 weeks and
in case of partial response after 6 (to 10) weeks, thebest step is to switch to another AD (level A2).Although there is evidence for switching, and ingeneral there is no preferential treatment (levelA2), there is a slight preference for switching to aTCA (with control of plasma levels) or to venla-faxine in view of their potential superiority.MAOIs should be reserved for later steps withthe exception for patients with MDD with atypicalfeatures. Another reason to switch to a TCA in thesecond step is reckoning with augmentation withlithium in the third step, as augmentation of a TCAwith lithium has a more solid base than with otherADs.Step 3: Lithium augmentation has by far the best
evidence (level A1) but for practical reasonslithium augmentation does not seem to be arealistic second step. Lithium utility in dailypractise is often limited by its side-effects (polyuria,polydipsia, tremor and thyroid dysfunction) andthe need for monitoring the serum lithium levels.
Spijker and Nolen
184
Therefore, we consider lithium augmentation as areasonable step after at least two unsuccessful trialswith AD monotherapy. The other augmentationoptions have only limited evidence: this applies tothe popular augmentation with mirtazapine as wellas with mianserin, bupropion and buspirone (alllevel B). There is some evidence for augmentationwith AAPs but their adverse effects are problem-atic, certainly in long-term treatment. The evidencefor T3 augmentation is weak (level A1) and thereare no data on treatment beyond 6 weeks so theutility of T3 augmentation on a large scale isquestionable.Step 4: Switch to a MAOI (tranylcypromine) is
the fourth step in case of non-response (level A2).Because of the dietary restrictions enforced bytranylcypromine treatment we do not considertranylcypromine as a reasonable second or thirdstep.Step 5: The evidence for ECT is strong (level
A1). However, ECT has its limitations in terms ofapplicability and therefore it is only the fifth step innon-response. However, severity of depression,adverse reactions of medication or concomitantsomatic illnesses could be reasons to advance thisstep.
Other algorithms
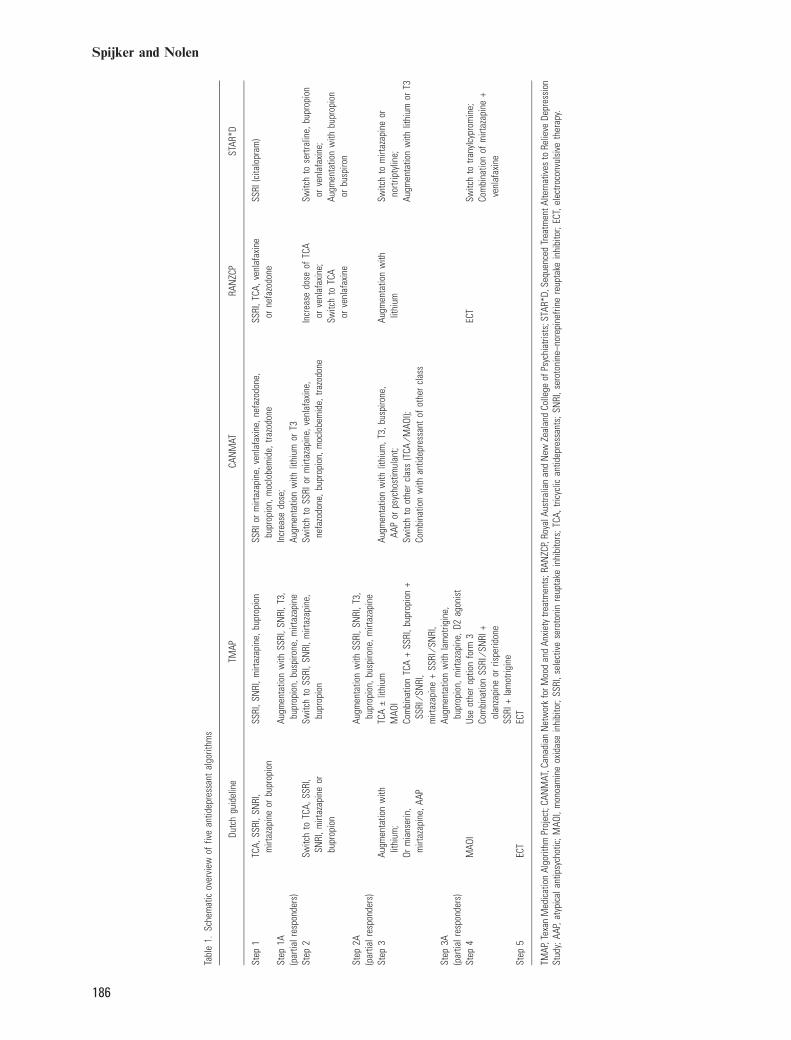
We identified three other algorithms for the (out-patient) treatment of non-psychotic depression:one from the Texan Medication Algorithm Project(TMAP) (64), and two from the CanadianNetwork for Mood and Anxiety Treatments(CANMAT) (65) and Royal Australian and NewZealand College of Psychiatrists (RANZCP) (66)guidelines for the treatment of depression. Otherguidelines, such as the US APA (67) and BritishNICE (68) guidelines only give general recommen-dations for the use of AD and do not contain analgorithm. Finally, we also included the algorithmof the STAR*D study (29) as being a large studycomparing many treatment options in a four-stepalgorithm design. An overview of the differentalgorithms is presented in the Table 1.The TMAP algorithm starts with several options
for monotherapy with an AD, in case of partialresponse there is an option to augment withvarious ADs or other agents (step 1A). In step 2(for non-responders to steps 1 or 1A) it is recom-mended to switch to another AD form the firststep. For partial responders to step 2 againaugmentation with the same medications as instep 1A is recommended (step 2A). Step 3 is aswitch to a TCA (with or without lithium) or toMAOI or to a combinations of AD. Before moving
forth to step 4, step 3A is an augmentationstrategy. Step 4 is one of the other options fromstep 3 or other combination strategies. Step 5 isECT. There is no time frame recommended whento determine non-response or partial response.Also in the CANMAT algorithm, SSRIs and
novel ADs are recommended as step 1, with apreference for paroxetine and venlafaxine indepression with melancholic features. In case ofnon-response the first step is to optimise the doseas tolerated. The next step in case of partialresponse is augmentation with lithium or T3 andin case of complete non-response a switch toanother AD. As a second step augmentation withvarious agents is recommended, or a switch toanother AD with a different mechanism or com-bination with another AD. TCAs (clomipramineand amitriptyline) are recommended for hospita-lised patients and the other TCAs and MAOIs arenot recommended as first line treatments becauseof safety and tolerability issues. The time frame todetermine when to go to a next step is not strictlyformulated but �some 3–4 weeks� is recommendedin case of non-response and �some weeks more� incase of partial response. Fluoxetine, moclobemideand sertraline are preferred ADs for atypicaldepression and mirtazapine, paroxetine, sertraline,venlafaxine and moclobemide for anxiousdepression.In the RANZCP algorithm a SSRI, a TCA,
venlafaxine or nefazodone are recommended foruncomplicated depression, with a preference for aTCA or venlafaxine in melancholic depression andfor phenelzine in atypical depression. In case ofpartial or non-response it is recommended toincrease the dose for TCAs, venlafaxine andnefazodone. In case of partial or non-response toa SSRI a switch to a TCA or venlafaxine isadvised. As a third step, augmentation with lithiumand in case of non-response ECT are suggested.There is no time frame recommended to determinenon-response or partial response.The STAR*D evaluated the efficacy of a four-
step treatment algorithm with each step lasting4 weeks. The first step is a SSRI (citalopram); inthe second step a switch to sertraline, bupropion,venlafaxine or an augmentation with bupropion orbuspirone is suggested. In the third step there aretwo switch options (to mirtazapine or nortripty-line) and two augmentation options (with lithiumor with T3). In the fourth step switching totranylcypromine and the combination of venlafax-ine and mirtazapine is recommended. STAR*D ispredominantly a medication algorithm with only inthe second step an option to switch to or toaugment with cognitive therapy.
Algorithm for the pharmacological treatment of depression
185
Tabl
e1.
Sche
mat
icov
ervi
ewof
five
antid
epre
ssan
tal
gorit
hms
Dutc
hgu
idel
ine
TMAP
CAN
MAT
RAN
ZCP
STAR
*D
Step
1TC
A,SS
RI,S
NRI
,m
irtaz
apin
eor
bupr
opio
nSS
RI,S
NRI
,mirt
azap
ine,
bupr
opio
nSS
RIor
mirt
azap
ine,
venl
afax
ine,
nefa
zodo
ne,
bupr
opio
n,m
oclo
bem
ide,
trazo
done
SSRI
,TCA
,ven
lafa
xine
orne
fazo
done
SSRI
(cita
lopr
am)
Step
1A(p
artia
lres
pond
ers)
Augm
enta
tion
with
SSRI
,SN
RI,T
3,bu
prop
ion,
busp
irone
,mirt
azap
ine
Incr
ease
dose
;Au
gmen
tatio
nw
ithlit
hium
orT3
Step
2Sw
itch
toTC
A,SS
RI,
SNRI
,mirt
azap
ine
orbu
prop
ion
Switc
hto
SSRI
,SN
RI,m
irtaz
apin
e,bu
prop
ion
Switc
hto
SSRI
orm
irtaz
apin
e,ve
nlaf
axin
e,ne
fazo
done
,bup
ropi
on,m
oclo
bem
ide,
trazo
done
Incr
ease
dose
ofTC
Aor
venl
afax
ine;
Switc
hto
TCA
orve
nlaf
axin
e
Switc
hto
sertr
alin
e,bu
prop
ion
orve
nlaf
axin
e;Au
gmen
tatio
nw
ithbu
prop
ion
orbu
spiro
nSt
ep2A
(par
tialr
espo
nder
s)Au
gmen
tatio
nw
ithSS
RI,S
NRI
,T3,
bupr
opio
n,bu
spiro
ne,m
irtaz
apin
eSt
ep3
Augm
enta
tion
with
lithi
um;
Orm
ians
erin
,m
irtaz
apin
e,AA
P
TCA
€lit
hium
MAO
ICo
mbi
natio
nTC
A+
SSRI
,bup
ropi
on+
SSRI
⁄SN
RI,
mirt
azap
ine
+SS
RI⁄S
NRI
,
Augm
enta
tion
with
lithi
um,T
3,bu
spiro
ne,
AAP
orps
ycho
stim
ulan
t;Sw
itch
toot
her
clas
s(T
CA⁄M
AOI);
Com
bina
tion
with
antid
epre
ssan
tof
othe
rcl
ass
Augm
enta
tion
with
lithi
umSw
itch
tom
irtaz
apin
eor
nortr
ipty
line;
Augm
enta
tion
with
lithi
umor
T3
Step
3A(p
artia
lres
pond
ers)
Augm
enta
tion
with
lam
otrig
ine,
bupr
opio
n,m
irtaz
apin
e,D2
agon
ist
Step
4M
AOI
Use
othe
rop
tion
form
3Co
mbi
natio
nSS
RI⁄S
NRI
+ol
anza
pine
orris
perid
one
SSRI
+la
mot
rigin
e
ECT
Switc
hto
trany
lcyp
rom
ine;
Com
bina
tion
ofm
irtaz
apin
e+
venl
afax
ine
Step
5EC
TEC
T
TMAP
,Tex
anM
edic
atio
nAl
gorit
hmPr
ojec
t;CA
NM
AT,C
anad
ian
Net
wor
kfo
rMoo
dan
dAn
xiet
ytre
atm
ents
;RAN
ZCP,
Roya
lAus
tralia
nan
dN
ewZe
alan
dCo
llege
ofPs
ychi
atris
ts;S
TAR*
D,Se
quen
ced
Trea
tmen
tAlte
rnat
ives
toRe
lieve
Depr
essi
onSt
udy;
AAP,
atyp
ical
antip
sych
otic
;MAO
I,m
onoa
min
eox
idas
ein
hibi
tor;
SSRI
,sel
ectiv
ese
roto
nin
reup
take
inhi
bito
rs;T
CA,t
ricyc
lican
tidep
ress
ants
;SN
RI,s
erot
onin
e–no
repi
nefri
nere
upta
kein
hibi
tor;
ECT,
elec
troco
nvul
sive
ther
apy.
Spijker and Nolen
186
Discussion
In this article, we presented the algorithm of theDutch guideline for the treatment of depressionand we compared this algorithm with the algo-rithms of the TMAP, CANMAT, RANZCPguidelines and of the STAR*D study.The four algorithms have much in common.
They all start with first AD monotherapy; switch-ing to another AD is recommended in the secondstep in case of non-response and combination ofADs is only advised as a later step.However, at closer look, there are also many
differences. First, regarding the choice of AD instep 1. The Dutch algorithm has the broadestrecommendation (a SSRI, a SNRI, mirtazapine,bupropion or a TCA) then the RANZCP (a SSRI,a TCA, nefazodone or venlafaxine) but inCANMAT and TMAP TCAs are not consideredfirst step ADs. The algorithm of STAR*D startedwith a SSRI.Another difference is when to augment? In
CANMAT, augmentation is already recommendedas a second step option in case of partial responseto the first step. In the RANZCP and the Dutchalgorithm augmentation is the third step. TMAPadvises after each step to augment with variousagents in case of partial response. STAR*Devaluated switching and augmentation options insteps 2 and 3. Lithium is the favourite augmenta-tion option in the Dutch, RANZCP andCANMAT algorithms, but there are differentalternatives for lithium: T3 in CANMAT, mians-erin, mirtazapine or an AAP in the Dutch algo-rithm and bupropion, buspirone and T3 inSTAR*D. In TMAP many alternatives are pre-sented for augmentation.The third major difference is the place of the
MAOI. While the RANZCP does not mention aMAOI at all, tranylcypromine is recommended asstep 4 (and in step 2 for patients with atypicaldepression) in the Dutch algorithm, and in TMAPand CANMAT as one of the options in step 3.There are also different recommendations for
specific subtypes of depression. In the Dutchalgorithm, there is no special mention of themelancholic subtype but a preference for TCAs inhospitalised patients just as in the CANMAT.In the RANZCP, venlafaxine and TCAs and inCANMAT, paroxetine and venlafaxine arefavoured for melancholic depression. For theatypical depressive subtype phenelzine is men-tioned as a first step in RANZCP; in theCANMAT and Dutch guideline as a second stepafter a SSRI. Only the CANMAT recommendsspecific ADs for the anxious depression.
It is obvious that the algorithms do not onlyreflect scientific evidence but also local andnational preferences and routines. Differencesbetween the algorithms in the sequencing ofsteps and whether to switch or to augment afternon-response to the first AD are not surprisingbecause there is no evidence for a preferredsequential approach, as also demonstrated inSTAR*D in which there were no statisticallysignificant differences in efficacy between any ofthe options in the subsequent steps (40, 51).STAR*D, however, has two major limitations,restricting the significance of the outcomes: therewas no placebo condition and it involved anequipoise randomisation (29).Nevertheless, some major conclusions can be
drawn. First, dose escalation of a SSRI is not asensible step and can be thus be omitted as an extra(or in between) step in patients not responding tothe standard dose. Second, of the augmentationoptions, the best evidence is for augmentation withlithium. Third, of the switch options, there islimited but rather strong evidence for MAOIs asone of the available options in case of treatmentresistance.Considering the differences in the algorithms
and the unresolved issues, the question is relevantwhether the use of algorithms in daily practiceshould be encouraged. The TMAP algorithm wastested in depressed out-patients and was foundmore efficacious than care as usual (69) withimprovements in depressive functioning andreduced side-effects burden. Probably, the highlystructured procedure of treatment is responsiblefor this outcome (70). Based on this limitedevidence, we are convinced that an algorithm-based treatment approach has a strong potentialto be more effective. Therefore, we stronglyrecommend to include algorithms in guidelines,especially when various different treatmentoptions are available and to promote their usein daily practice. But also to make them mutualcomparable and to do further research on theireffectiveness.
Declaration of interest
Doctor Nolen received grant support from Netherlands Orga-nisation for Health Research and Development, NetherlandsOrganisation for Scientific Research, Stanley Medical ResearchInstitute, Astra Zeneca, Eli Lilly, GlaxoSmithKline, Wyeth;received speaker�s fees from Astra Zeneca, Eli Lilly, Johnson &Johnson, Pfizer, Servier and Wyeth and is on the advisoryboard of Astra Zeneca, Cyberonics, Eli Lilly, GlaxoSmith-Kline, Johnson & Johnson, Pfizer and Servier. Doctor Spijkerhas received speaker�s fees from Astra Zeneca, Wyeth andGlaxoSmithKline.
Algorithm for the pharmacological treatment of depression
187
References
1. Geddes JR, Freemantle N, Mason J et al. SSRIs versus otherantidepressants for depressive disorder. The CochraneLibrary 2000; Issue 2:1–24.
2. Anderson IM. Selective serotonin reuptake inhibitors versustricyclic antidepressants: a meta-analysis of efficacy andtolerability. J Aff Dis 2000;58:19–36.
3. MacGillivray S, Arroll B, Hatcher S et al. Efficacy andtolerability of selective serotonin reuptake inhibitorscompared with tricyclic antidepressants in depressiontreated in primary care: systematic review and meta-anal-ysis. Br Med J 2003;326:1014–1017.
4. Machado M, Iskedjian M, Ruiz I, Einarson TR. Remission,dropouts, and adverse drug reaction rates in majordepressive disorder: a meta-analysis of head-to-head trials.Curr Med Res and Opinions 2006;22:10825–10837.
5. Anderson IM. Meta analysis of antidepressant drugs:selectivity versus multiplicity. In: den Boer JA, Westenberg
MGM, eds. Antidepressants: selectivity versus multiplicity.Amsterdam: Benecke NI, 2001:85–99.
6. Williams JW, Mulrow CD, Chiquette E et al. A systematicreview of newer pharmacotherapies for depression inadults: evidence report summary. Ann Intern Med2000;132:749–756.
7. Arrol B, MacGilivray S, Ogston S., et al. Efficacy andtolerability of tricyclic antidepressants and SSRIs com-pared with placebo for treatment of depression in primarycare: a meta-analysis. Ann Fam Med 2005;3:449–456.
8. Greden JF. The burden of disease for treatment-resistantdepression. J Clin Psychiatry 2001;62(Suppl 16):26–31.
9. Thase ME, Rush AJ. When at first you don�t succeed:sequential strategies for antidepressant nonresponders.J Clin Psychiatry 1997;58(Suppl 13):23–29.
10. Nelson JC. Managing treatment resistant major depression.J Clin Psychiatry 2003;64:5–12.
11. McIntyre RS, Muller A, Mancini DA, Silver ES. What todo if an initial antidepressant fails? Can Fam Physican2003;49:449–457.
12. Thase ME. Therapeutic alternatives for the difficult to treatdepression: a narrative review of the state of the evidence.CNS Spectrums, 2004;9:808–821.
13. Dodd S, Horgan D, Malhi GS, Berk M. To combine or notto combine? A literature review of antidepressant combi-nation therapy J Aff Dis 2005;89:1–11.
14. Rojo JE, Ros S, Aguera L, de la Gandara J, de Pedro JM.Combined antidepressant: clinical experience. Acta Psy-chiatr Scand 2005;112(Suppl 428):25–31.
15. Ros S, Aguera L, de la Gandara J, Rojo JE, de Pedro JM.Potentiating strategies for treatment-resistant depression.Acta Psychiatr Scand 2005;112(Suppl 428):14–24.
16. DeBattista C. Augmentation and combination strategiesfor depression. J Psychopharmacol 2006;20:11–18.
17. Trivedi MH. Using treatment algorithms to bring patientsto remission. J Clin Psychiatry 2003;64:8–13.
18. Nolen WA, Haffmans J. Treatment of resistant depres-sion. Review on the efficacy of various biological treat-ments, specifically in major depression resistant to cyclicantidepressants. Int Clin Psychopharmacol 1989;4:217–228.
19. Multidisciplinaire Richtlijn Depressie. Richtlijn voor dediagnostiek en behandeling van volwassen clienten met eendepressie. Utrecht: Trimbos-instituut Utrecht, 2005.
20. Update Multidisciplinaire Richtlijn Depressie. Richtlijnvoor de diagnostiek en behandeling van volwassen clientenmet een depressie. Utrecht: Trimbos-instituut Utrecht,2009.
21. Turner EH, Matthews AM, Linardatos E, Tell RA, Rosen-
thal R. Selective publication of antidepressant trials and itsinfluence on apparent efficacy. New Engl J Med2008;358:252–260.
22. Kirsch I, Deacon BJ, Huedo-Median TB et al. Initial severityand antidepressants benefit: a meta-analysis of data sub-mitted to the Food and Drug administration. PloS Med2008;5:260–268.
23. DeRubeis RJ, Crits-Christoph P. Empirically supportedindividual and group psychological treatments for adultmental disorders. J Consult Clin Psychol 1998;66:37–52.
24. DeRubeis RJ, Gelfand LA, Tang TZ et al. Medicationsversus cognitive behavior therapy for severely depressedoutpatients: mega-analysis of four randomized compari-sons. Am J Psychiatry 1999;156:1007–1013.
25. DeRubeis RJ, Hollon SD, Amsterdam JD, et al. Cognitivetherapy vs medications in the treatment of moderate tosevere depression. Arch Gen Psychiatry 2005; 62: 409–416.
26. Claxton AJ, Li Z, McKendrick J. Selective serotonininhibitor treatment in the UK, risk of relapse or recurrenceof depression. Br J Psychiatry 2000;177:163–168.
27. Szedegi A, Jansen WT, van Willigenburg APP, van der
Meulen E, Stassen HH, Thase ME. Early improvement inthe first 2 weeks as a predictor of treatment outcome inpatients with major depressive disorder: a meta-analysisincluding 6562 patients. J Clin Psychiatry 2009;70:344–353.
28. Quitkin FM, McGrath PJ, Stewart JW et al. Chronologicalmilestones to guide drug change When should cliniciansswitch antidepressants?. Arch Gen Psychiatry 1996;53:785–792.
29. Rush AJ, Fava M, Wisniewski SR et al. Sequenced treatmentalternatives to relieve depression (STAR*D): rationale anddesign. Control Clin Trials 2004;25:119–142.
30. Fredman SJ, Fava M, Kienke AS et al. Partial response,nonresponse and relapse with selective serotonin reuptakeinhibitors in major depression: a survey of current next-step practices. J Clin Psychiatry 2006;1:403–408.
31. Ruhe HG, Huyser J, Swinkels JA, Schene AH. Dose escala-tion for insufficient response to standard-dose selectivereuptake inhibitors in major depressive disorder. A sys-tematic review. Br J Psychiatry 2006;189:309–316.
32. Licht RW, Qvitzau S. Treatment strategies in patients withmajor depression not responding to first-line sertralinetreatment. A randomised study of extended duration oftreatment, dose increase or mianserin augmentation. Psy-chopharmacol 2002;161:143–151.
33. Fava M, Rosenbaum JF, McGrath PJ et al. Lithium andtricyclic augmentation of fluoxetine treatment for resistantmajor depression. Am J Psychiatry 1994;151:1372–1374.
34. Fava M, Alpert J, Nierenberg A et al. Doubleblind study ofhigh dose fluoxetine versus lithium or desipramine aug-mentation of fluoxetine in partial and non-repsponders tofluoxetine. J Clin Psychopharmacol 2002;22:379–387.
35. Ruhe HG, Booij J, van Weert HC et al. Evidence why par-oxetine dose escalation is not effective in major depressivedisorder: a randomized controlled trial with assessment ofserotonin transporter occupancy. Neuropsychopharmacol2009;34:999–1010.
36. Aldi M, Baethge Ch, Heinz A et al. Is dose escalation ofantidepressants a rational strategy after a medium-dosetreatment failed? A systematic review Eur Arch PsychiatryClin Neurosci 2005;255:387–400.
37. Corruble E, Guelfi JD. Does increase dose improve efficacywith poor antidepressant response: a review. Acta Psychi-atr Scand 2000;101:343–348.
38. Mischoulon D, Nierenberg ASA, Kizilbash L et al. Strategiesfor managing depression refractory to selective serotonin
Spijker and Nolen
188
reuptake inhibitor treatment: a survey of clinicians. Can JPsychiatry 2000;45:476–481.
39. Ruhe HG, Huyser J, Swinkels JA, Schene AH. Switchingantidepressants after a first selective reuptake inhibitor inmajor depressive disorder A systematic review. J ClinPsychiatry 2006;67:10836–10855.
40. Rush AJ, Trivedi MH, Wisniewski SR et al. Bupropion-SR,sertraline or venlafaxine-XR after failure of SSRIs fordepression. N Eng J Med 2006;354:1231–1242.
41. Nolen WA, van de Putte JJ, Dijken WA et al. Treatmentstrategy in depression. II. MAO inhibitors in depressionresistant to cyclic antidepressants: two controlled crossoverstudies with tranylcypromine versus L-5-hydroxytrypto-phan and nomifensine. Acta Psychiatr Scand 1988;78:676–683.
42. McGrath PJ, Stewart JW, Fava M et al. Tranylcypromineversus venlafaxine plus mirtazapine following three failedantidepressant medication trials for depression:a STAR*D report. Am J Psychiatry 2006;63:1531–1541.
43. Nolen WA, van de Broek WW, Birkenhager T. Treatmentwith low dose of tranylcypromine resulted in disappointingremission rate. Am J Psychiatry 2007;164:524.
44. Birkenhager TK, van den Broek WW, Mulder PG, Bruijn JA,Moleman P. Efficacy and tolerability of tranylcypromineversus phenelzine: a double-blind study in antidepressant-refractory depressed inpatients. J Clin Psychiatry.2004;65:1505–1510.
45. Crossley NA, Bauer M. Acceleration and augmentation ofantidepressants with lithium for depressive disorders: twometa-analyses of randomized placebo-controlled trials.J Clin Psychiatry 2007;8:935–940.
46. Aronson R, Offman HJ, Joffe RT, Naylor D. Triiodothy-ronine augmentation in the treatment of refractorydepression. A meta-analysis. Arch Gen Psychiatry1996;53:842–848.
47. Joffe RT, Sokolov ST. Thyroid hormone treatment of pri-mary unipolar depression: a review. Int J Neuropsycho-pharmacol 2000;3:143–147.
48. Nierenberg AA, Fava M, Trivedi MH et al. A comparison oflithium and T(3) augmentation following two failed med-ication treatments for depression: a STAR*D report. Am JPsychiatry 2006;163:1519–1530.
49. Landen M, Gjorling G, Agren H, Fahlen T. A randomized,double blind placebo controlled trial of buspirone incombination with an SSRI in patients with treatmentrefractory depression. J Clin Psychiatry 1998;59:664–668.
50. Appelberg BB, Syvalahti EK, Koskine TE et al. Patientswith severe depression may benefity from busprioneaugmentation of selective serotonin reuptake inhibitors:results from a placebo-controlled, randomized, double-blind, placebo wash in study. J Clin Psychiatry 2001;62:448–452.
51. Trivedi MH, Fava M, Wisniewski SR et al. Medicationaugmentation after the failure of SSRIs for depression.N Engl J Med 2006;354:1243–1252.
52. Ballesteros J, Callado LF. Effectiveness of pindolol plusserotonin uptake inhibitors in depression: a meta-analysisof early and late outcome from randomised controlledtrials. J Aff Dis 2004;79:137–147.
53. Ferreri M, Lavergne F, Berlin I et al. Benefits frommianserin augmentation of fluoxetine in patients withmajor depression non-responders to fluoxetine alone. ActaPsychiatr Scand 2001;103:66–72.
54. Maes M, Libbrecht I, van Hunsel F et al. Pindolol andmianserin augment the antidepressant activity of fluxoetinein hospitalized depressed patients including those withtreatment resistance. J Clin Psychopharmacol 1999;19:177–457.
55. Carpenter LL, Yasmin S, Price LH. A double-blind, pla-cebo-controlled study of antidepressant augmentation withmirtazapine. Biol Psychiatry 2002;51:183–188.
56. Nelson JC, Mazure CM, Jatlow PI et al. Combining nor-epinephrine and serotonin inhibitors mechanisme fortreatment of depression: a double-blind randomized study.Biol Psychiatry 2004;55:296–300.
57. Lam RW, Hossie H, Solomons K, Yatham LN. Citalopramand bupropion-SR, combining versus switching in patientswith treatment resistant depression. J Clin Psychiatry2004;5:337–340.
58. Papakostas GI, Shelton RC, Smith J, Fava M. Augmen-tation of antidepressants with atypical antipsychoticmedication for treatment-resistant major depressive dis-order: a meta-analysis. J Clin Psychiatry 2007;68:826–831.
59. Marcus RN, McQuade RD, Carson WH et al. The efficacyand safety of aripiprazole as adjunctive therapy in majordepressive disorder. A second multicenter, randomized,double-blind placebo-controlled trial. J Clin Psychophar-macol 2008;28:156–165.
60. Berman RM, Marcus RN, Swanink R et al. The efficacy andsafety of aripiprazole as adjunctive therapy in majordepressive disorder. A multicenter, randomized, double-blind placebo-controlled trial. J Clin Psychiatry2007;68:843–853.
61. The UK ECT Review group. Efficacy and safety of elec-troconvulsive therapy in depressive disorders: a systematicreview and meta-analyse. Lancet 2003;361:799–808.
62. Taylor MJ, Freemantle N, Geddes JR, Bhagwagar Z.Early onset of selective serotonin reuptake inhibitorantidepressant action. Arch Gen Psychiatry 2006;63:1217–1223.
63. Rush AJ, Thase ME. Strategies and tactics in the treatmentof chronic depression. J Clin Psychiatry 1997;58(Suppl.13):14–22.
64. http://www.dshs.state.tx.us/mhprograms/tmapover.shtm.65. Canadian Network for Mood and Anxiety Treatments.
Clinical guidelines for the treatment of depressive disor-ders. IV Medications and other biological treatments. CanJ Psychiatry 2001;46(Suppl.):38–57.
66. Royal Australian and New Zealand College of Psychia-trists. Australian and New Zealand clinical practiceguidelines for the treatment of depression. Austral NewZeal J Psychiatry 2004;38:389–407.
67. US APA. Practice guideline treatment of patients withmajor depressive disorder, 2nd edn. Arlington: AmericanPsychiatric Association, 2000.
68. British NICE. Depression. Management of depression inprimary and secondary care. London UK: NationalInstitute for Clinical Excellence, 2004.
69. Trivedi MH, Rush AJ, Crimson ML et al. Clinical results forpatients with major depressive disorder in the TexasMedication algorithm Project. Arch Gen Psychiatry2004;61:669–680.
70. Adli MA, Bauer M, Rush AJ. Algorithms and collaborativecare systems for depression; are they effective and why?A systematic review. Biol Psychiatry 2006;59:1029–1038.
Algorithm for the pharmacological treatment of depression
189





























