Embed Size (px)
Citation preview
Surg Today (2006) 36:633–637DOI 10.1007/s00595-006-3214-9
An Icteric Type Hepatocellular Carcinoma with No Detectable Tumorin the Liver: Report of a Case
Tomoki Makino1, Shoji Nakamori1, Masaki Kashiwazaki1, Norikazu Masuda1, Masakazu Ikenaga1,Motohiro Hirao1, Kazumasa Fujitani1, Hideyuki Mishima1, Toshiro Sawamura1, Masashi Takeda2,Masayuki Mano2, and Toshimasa Tsujinaka1
Departments of 1 Surgery and 2 Pathology, National Hospital Organization, Osaka National Hospital, 2-1-14 Hoenzaka, Chuo-ku,Osaka 540-0006, Japan
within the biliary tract, or compression of the biliarytract by the tumor.1–6 These types have been classified asicteric type HCC by Lin et al.2 Since Mallory et al.1 firstdescribed a case of HCC accompanied with obstructivejaundice secondary to biliary hemorrhage from a tumorinvading the cystic duct, a number of similar reportshave been found in the literature.3,7–10 In most of thesecases, the main tumors were detected in the liver. Weherein report a case of a successful resection of an ict-eric type HCC without a detectable original tumor inthe liver.
Case Report
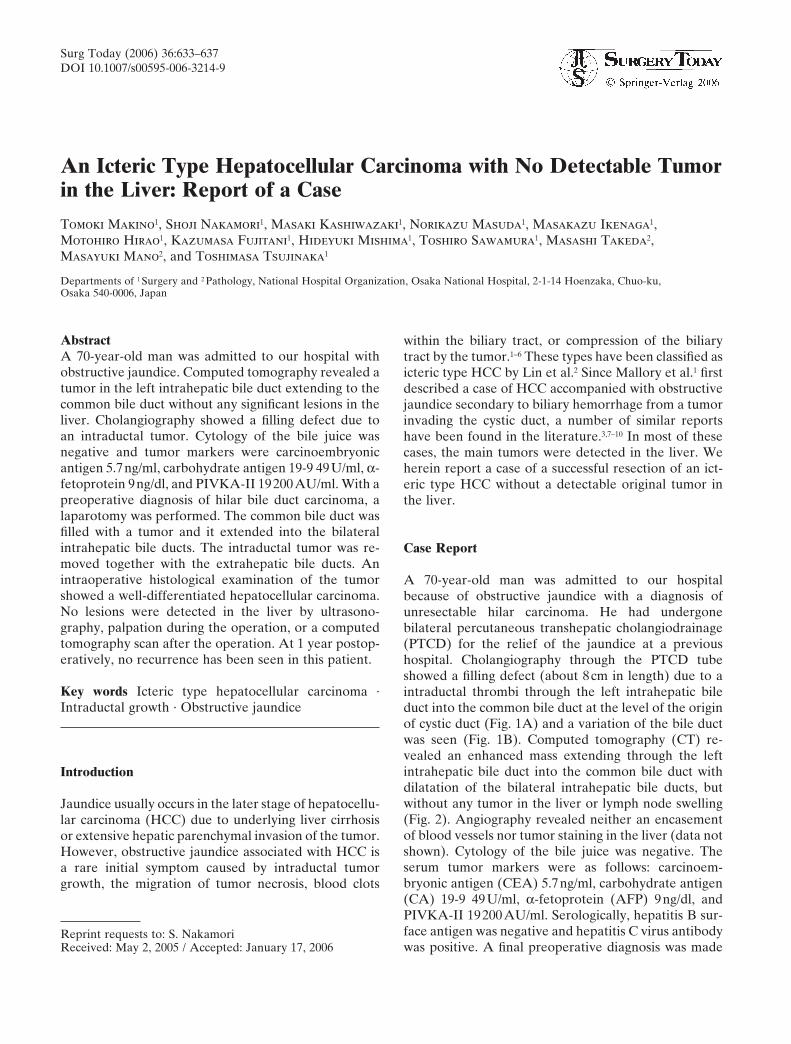
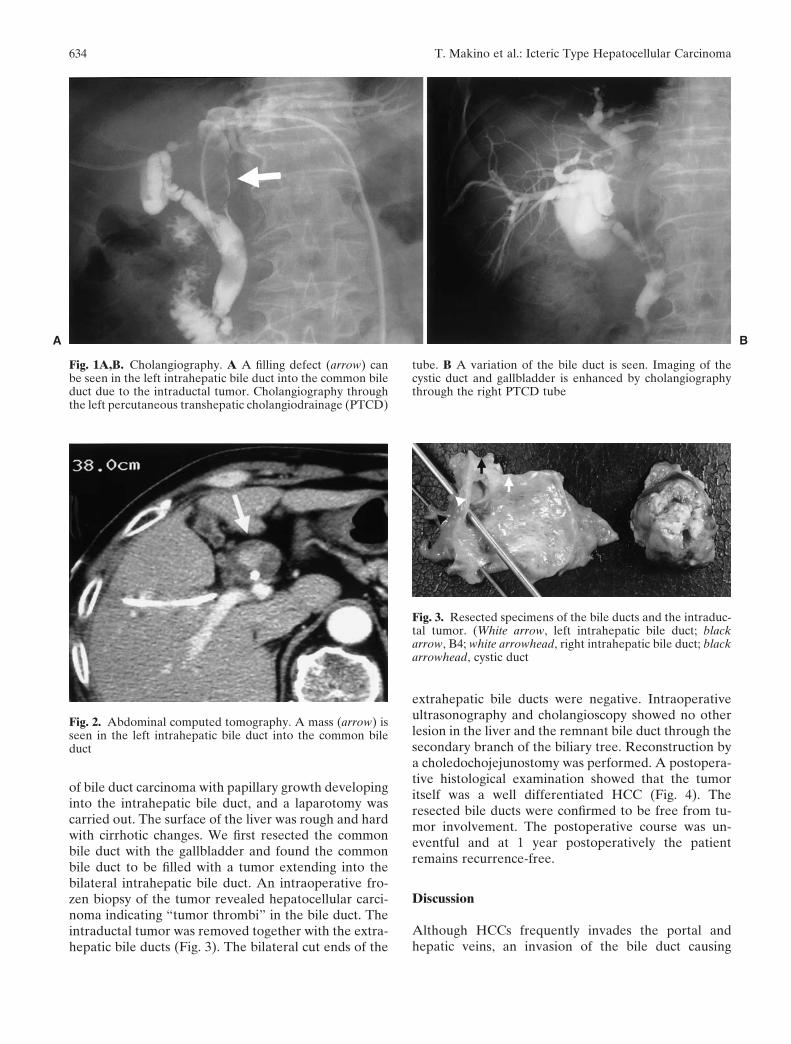
A 70-year-old man was admitted to our hospitalbecause of obstructive jaundice with a diagnosis ofunresectable hilar carcinoma. He had undergonebilateral percutaneous transhepatic cholangiodrainage(PTCD) for the relief of the jaundice at a previoushospital. Cholangiography through the PTCD tubeshowed a filling defect (about 8cm in length) due to aintraductal thrombi through the left intrahepatic bileduct into the common bile duct at the level of the originof cystic duct (Fig. 1A) and a variation of the bile ductwas seen (Fig. 1B). Computed tomography (CT) re-vealed an enhanced mass extending through the leftintrahepatic bile duct into the common bile duct withdilatation of the bilateral intrahepatic bile ducts, butwithout any tumor in the liver or lymph node swelling(Fig. 2). Angiography revealed neither an encasementof blood vessels nor tumor staining in the liver (data notshown). Cytology of the bile juice was negative. Theserum tumor markers were as follows: carcinoem-bryonic antigen (CEA) 5.7ng/ml, carbohydrate antigen(CA) 19-9 49U/ml, α-fetoprotein (AFP) 9ng/dl, andPIVKA-II 19200 AU/ml. Serologically, hepatitis B sur-face antigen was negative and hepatitis C virus antibodywas positive. A final preoperative diagnosis was made
AbstractA 70-year-old man was admitted to our hospital withobstructive jaundice. Computed tomography revealed atumor in the left intrahepatic bile duct extending to thecommon bile duct without any significant lesions in theliver. Cholangiography showed a filling defect due toan intraductal tumor. Cytology of the bile juice wasnegative and tumor markers were carcinoembryonicantigen 5.7ng/ml, carbohydrate antigen 19-9 49U/ml, α-fetoprotein 9ng/dl, and PIVKA-II 19200AU/ml. With apreoperative diagnosis of hilar bile duct carcinoma, alaparotomy was performed. The common bile duct wasfilled with a tumor and it extended into the bilateralintrahepatic bile ducts. The intraductal tumor was re-moved together with the extrahepatic bile ducts. Anintraoperative histological examination of the tumorshowed a well-differentiated hepatocellular carcinoma.No lesions were detected in the liver by ultrasono-graphy, palpation during the operation, or a computedtomography scan after the operation. At 1 year postop-eratively, no recurrence has been seen in this patient.
Key words Icteric type hepatocellular carcinoma ·Intraductal growth · Obstructive jaundice
Introduction
Jaundice usually occurs in the later stage of hepatocellu-lar carcinoma (HCC) due to underlying liver cirrhosisor extensive hepatic parenchymal invasion of the tumor.However, obstructive jaundice associated with HCC isa rare initial symptom caused by intraductal tumorgrowth, the migration of tumor necrosis, blood clots
Reprint requests to: S. NakamoriReceived: May 2, 2005 / Accepted: January 17, 2006
634 T. Makino et al.: Icteric Type Hepatocellular Carcinoma
of bile duct carcinoma with papillary growth developinginto the intrahepatic bile duct, and a laparotomy wascarried out. The surface of the liver was rough and hardwith cirrhotic changes. We first resected the commonbile duct with the gallbladder and found the commonbile duct to be filled with a tumor extending into thebilateral intrahepatic bile duct. An intraoperative fro-zen biopsy of the tumor revealed hepatocellular carci-noma indicating “tumor thrombi” in the bile duct. Theintraductal tumor was removed together with the extra-hepatic bile ducts (Fig. 3). The bilateral cut ends of the
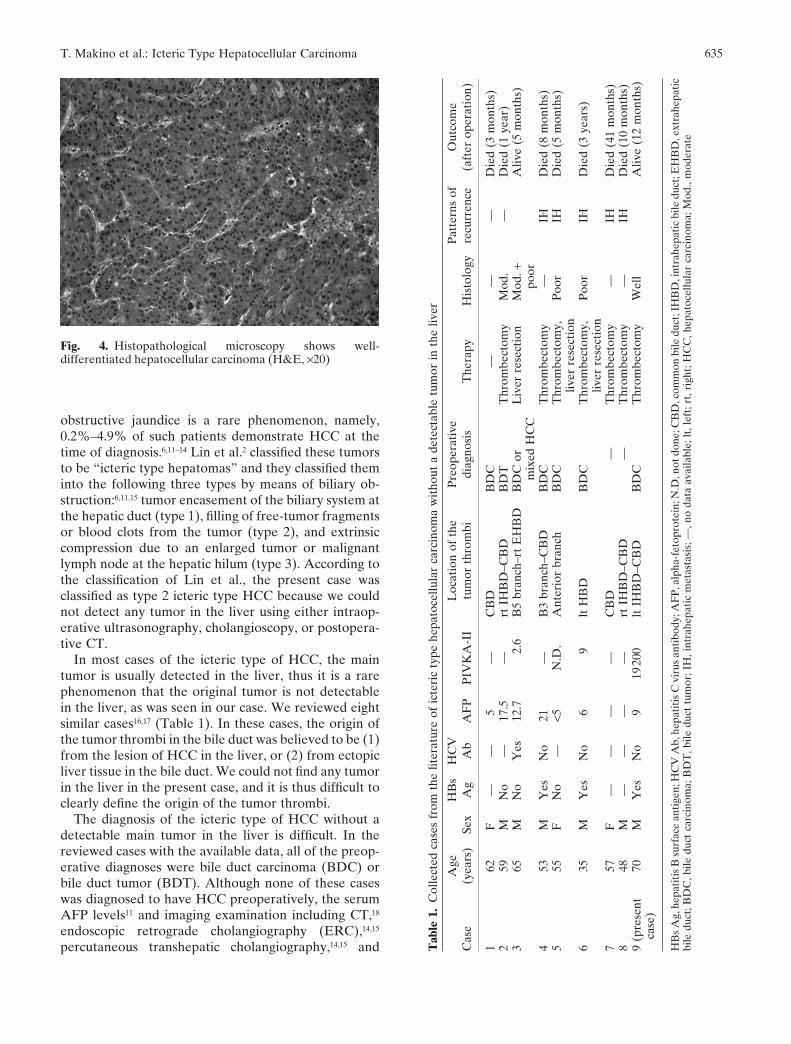
extrahepatic bile ducts were negative. Intraoperativeultrasonography and cholangioscopy showed no otherlesion in the liver and the remnant bile duct through thesecondary branch of the biliary tree. Reconstruction bya choledochojejunostomy was performed. A postopera-tive histological examination showed that the tumoritself was a well differentiated HCC (Fig. 4). Theresected bile ducts were confirmed to be free from tu-mor involvement. The postoperative course was un-eventful and at 1 year postoperatively the patientremains recurrence-free.
Discussion
Although HCCs frequently invades the portal andhepatic veins, an invasion of the bile duct causing
Fig. 1A,B. Cholangiography. A A filling defect (arrow) canbe seen in the left intrahepatic bile duct into the common bileduct due to the intraductal tumor. Cholangiography throughthe left percutaneous transhepatic cholangiodrainage (PTCD)
tube. B A variation of the bile duct is seen. Imaging of thecystic duct and gallbladder is enhanced by cholangiographythrough the right PTCD tube
Fig. 2. Abdominal computed tomography. A mass (arrow) isseen in the left intrahepatic bile duct into the common bileduct
Fig. 3. Resected specimens of the bile ducts and the intraduc-tal tumor. (White arrow, left intrahepatic bile duct; blackarrow, B4; white arrowhead, right intrahepatic bile duct; blackarrowhead, cystic duct
A B
635T. Makino et al.: Icteric Type Hepatocellular Carcinoma
obstructive jaundice is a rare phenomenon, namely,0.2%–4.9% of such patients demonstrate HCC at thetime of diagnosis.6,11–14 Lin et al.2 classified these tumorsto be “icteric type hepatomas” and they classified theminto the following three types by means of biliary ob-struction:6,11,15 tumor encasement of the biliary system atthe hepatic duct (type 1), filling of free-tumor fragmentsor blood clots from the tumor (type 2), and extrinsiccompression due to an enlarged tumor or malignantlymph node at the hepatic hilum (type 3). According tothe classification of Lin et al., the present case wasclassified as type 2 icteric type HCC because we couldnot detect any tumor in the liver using either intraop-erative ultrasonography, cholangioscopy, or postopera-tive CT.
In most cases of the icteric type of HCC, the maintumor is usually detected in the liver, thus it is a rarephenomenon that the original tumor is not detectablein the liver, as was seen in our case. We reviewed eightsimilar cases16,17 (Table 1). In these cases, the origin ofthe tumor thrombi in the bile duct was believed to be (1)from the lesion of HCC in the liver, or (2) from ectopicliver tissue in the bile duct. We could not find any tumorin the liver in the present case, and it is thus difficult toclearly define the origin of the tumor thrombi.
The diagnosis of the icteric type of HCC without adetectable main tumor in the liver is difficult. In thereviewed cases with the available data, all of the preop-erative diagnoses were bile duct carcinoma (BDC) orbile duct tumor (BDT). Although none of these caseswas diagnosed to have HCC preoperatively, the serumAFP levels11 and imaging examination including CT,18
endoscopic retrograde cholangiography (ERC),14,15
percutaneous transhepatic cholangiography,14,15 and
Fig. 4. Histopathological microscopy shows well-differentiated hepatocellular carcinoma (H&E, ×20)
Tab
le 1
.C
olle
cted
cas
es f
rom
the
lite
ratu
re o
f ic
teri
c ty
pe h
epat
ocel
lula
r ca
rcin
oma
wit
hout
a d
etec
tabl
e tu
mor
in t
he li
ver
Age
HB
sH
CV
Loc
atio
n of
the
Pre
oper
ativ
eP
atte
rns
ofO
utco
me
Cas
e(y
ears
)Se
xA
gA
bA
FP
PIV
KA
-II
tum
or t
hrom
bidi
agno
sis
The
rapy
His
tolo
gyre
curr
ence
(aft
er o
pera
tion
)
162
F—
—5
—C
BD
BD
C—
——
Die
d (3
mon
ths)
259
MN
o—
17.5
—rt
IH
BD
–CB
DB
DT
Thr
ombe
ctom
yM
od.
—D
ied
(1 y
ear)
365
MN
oY
es12
.72.
6B
5 br
anch
–rt
EH
BD
BD
C o
rL
iver
res
ecti
onM
od. +
Aliv
e (5
mon
ths)
mix
ed H
CC
poor
453
MY
esN
o21
—B
3 br
anch
–CB
DB
DC
Thr
ombe
ctom
y—
IHD
ied
(8 m
onth
s)5
55F
No
—<5
N.D
.A
nter
ior
bran
chB
DC
Thr
ombe
ctom
y,P
oor
IHD
ied
(5 m
onth
s)liv
er r
esec
tion
635
MY
esN
o6
9lt
HB
DB
DC
Thr
ombe
ctom
y,P
oor
IHD
ied
(3 y
ears
)liv
er r
esec
tion
757
F—
——
—C
BD
—T
hrom
bect
omy
—IH
Die
d (4
1 m
onth
s)8
48M
——
——
rt I
HB
D–C
BD
—T
hrom
bect
omy
—IH
Die
d (1
0 m
onth
s)9
(pre
sent
70M
Yes
No
919
200
lt I
HB
D–C
BD
BD
CT
hrom
bect
omy
Wel
lA
live
(12
mon
ths)
case
)
HB
s A
g, h
epat
itis
B s
urfa
ce a
ntig
en; H
CV
Ab,
hep
atit
is C
vir
us a
ntib
ody;
AF
P, a
lpha
-fet
opro
tein
; N.D
, not
don
e; C
BD
, com
mon
bile
duc
t; IH
BD
, int
rahe
pati
c bi
le d
uct;
EH
BD
, ext
rahe
pati
cbi
le d
uct;
BD
C, b
ile d
uct
carc
inom
a; B
DT
, bile
duc
t tu
mor
; IH
, int
rahe
pati
c m
etas
tasi
s; —
, no
data
ava
ilabl
e; lt
, lef
t; rt
, rig
ht; H
CC
, hep
atoc
ellu
lar
carc
inom
a; M
od.,
mod
erat
e

636 T. Makino et al.: Icteric Type Hepatocellular Carcinoma
magnetic resonance cholangiography19 could be helpfulfor the differential diagnosis between BDC (BDT) andHCC. Among them, the cholangiograms could be themost helpful in the case of negative tumor markers.Intraluminal filling defects and irregular cutting surface,which were found to be blood clots or necrotic tumordebris, are different from the conventional cholangio-graphic appearance of BDC.15 A retrospective analysisin the present case did not show a typical intraluminalfilling defect as is the case with BDC. The elevation ofPIVKA-II and the positive HCV markers, which weoverlooked in the present case, would thus be helpfulfor accurately diagnosing this type of HCC although thePIVKA-II level may not be reliable in the presence ofobstructive jaundice. Based on previous reports, theicteric type of HCC shows invasive growth and notumor capsule formation such as seen in hilarcholangiocarcinoma,13,18,19 while the tumor did notshow any invasive growth in the present case. An accu-rate diagnosis, however, cannot be reached until eithertumor biopsies or a resection is performed.20
Although the ideal treatment of the icteric type ofHCC would be a complete extirpation of the tumor, thesame as for other malignant tumors, the total resectionrate of these tumors is very low.6,11,13–15,19,21,22 One of thereasons for this may be due to the hepatic parenchymalinsufficiency exaggerated by persistent obstructive jaun-dice and the low hepatic reserve function associatedwith cirrhosis. Immediate biliary drainage is recom-mended for icteric type HCC and an operation shouldbe performed after the relief of jaundice and a subse-quent evaluation of the hepatic reserve function.12,21
According to the operative methods in our reviewedcases, 5 out of the 8 cases, including our case, received athrombectomy through a choledochotomy while 3 casesreceived a hepatic resection with a thrombectomy. Re-garding the surgical procedures in the three patientswho underwent a hepatic resection, a hepatic lobectomywas performed in two patients and a segmentectomy inone to resect the intrahepatic bile duct and the tumorthrombus in it. In two of these three cases, based on theavailable information, no main tumors were detected inthe resected specimens. In the present case, however,the liver function was estimated preoperatively to mar-ginally allow the performance of a left hepatic lobec-tomy, and the low functional level was confirmed asbeing due to obvious cirrhosis. To avoid liver dysfunc-tion after the operation we considered that a resectionof the extrahepatic bile ducts should be sufficient tocomplete the tumor removal because of the lack of anydetectable tumors in the secondary branch of the biliarytree as assessed by intraoperative cholangioscopy andintraoperative ultrasonography. Although a hepatic re-section for regional tumors of the intrahepatic bile ductis usually necessary when performing a curative resec-
tion for this type of HCC, a complete thrombectomywith a choledochotomy may therefore be adequate ifthe negative cut ends of the bile ducts and the absenceof regional intrahepatic tumors can be confirmed, as inthe present case.
The prognosis of icteric type HCC has been reportedto be poor11–13,15 although Lau et al.6 reported, in a studyof 49 icteric type HCC patients, that the overall survivalof these patients was similar to that of HCC patientswith no jaundice and he concluded that a good pallia-tion and occasional cure were possible with propertreatment. However, the icteric type of HCC with nodetectable hepatic tumor has a poor prognosis as in ourreviewed cases, although it is necessary to collect moresimilar cases with a longer-term follow-up for a betterevaluation of the prognosis. Regarding the patterns ofrecurrence in the icteric type of HCC with no detectablemain tumor, intrahepatic metastases, one of whichmight be the origin of the intraductal tumor, developedin all five patients based on the available information.Moreover, these recurrent cases included two patientswho had undergone a thrombectomy with a liver resec-tion. Considering this, the difficulty in accurately de-termining to optimal degree of a liver resection mightthus influence the poor prognosis of ictric type HCCwith no detectable hepatic tumors, if the tumor thrombiin the bile duct originate from a lesion in the liver. Apostoperative examination of the liver thus seems to beimportant for the early detection of recurrence, and atthe very least, a curative surgical resection and postop-erative intensive monitoring of potential hepatic lesionsare necessary to improve the prognosis.
References
1. Mallory TB, Castleman B, Parris EE. Case records of Massachu-setts General Hospital, case 33441. N Engl J Med 1947;237:673–6.
2. Lin TY, Chen KM, Chen YR, Lin WS, Wang TH, Sung JL. Icterictype hepatoma. Med Chir Dig 1975;88:267–70.
3. Kojiro M, Kawabata K, Kawano Y, Shirai F, Takemoto N,Nakashima T. Hepatocellular carcinoma presenting as intrabileduct tumor growth. A clinicopathological study of 24 cases.Cancer 1982;49:2144–7.
4. Lee KC, Sakai K, Kinoshita H, Hirohashi K, Tsuji Y, Kubo S,et al. Resection of hepatocellular carcinoma with obstructivejaundice caused by compression of the common hepatic duct. JSurg Oncol 1988;39:201–5.
5. Ueda M, Takeuchi T, Takahashi K, Okamoto S, Tanaka A,Morimoto T, et al. Classification and surgical treatment of hepa-tocellular carcinoma (HCC) with bile duct thrombi. Hepato-gastroenterology 1994;41:349–54.
6. Lau WL, Leung K, Leung TWT, Liew CT, Chan MSY, Yu SCH,et al. A logical approach to hepatocellular carcinoma presentingwith jaundice. Ann Surg 1997;225:281–5.
7. Johns W, Zimmerman A. Biliary obstruction due to hemobiliacaused by liver cell carcinoma. Ann Surg 1961;153:706–10.
8. Dickinson SJ, Santulli T. Obstruction of common bile duct byhepatoma. Surgery 1962;52:800–2.

637T. Makino et al.: Icteric Type Hepatocellular Carcinoma
9. Jurco S, Kim H. Extrahepatic biliary obstruction by hepatocellu-lar carcinoma. Am J Gastroenterol 1980;74:176–8.
10. Cleland P, Adjukiewicz A. Hepatoma and obstructive jaundice.Postgrad Med J 1980;56:371–2.
11. Chen MF, Jan YY, Jeng LB, Hwang TL, Wang CS, Chen SC.Obstructive jaundice secondary to ruptured hepatocellular carci-noma into the common bile duct. Cancer 1994;73:1335–40.
12. Shimada M, Takenaka K, Hasegawa H, Shirabe K, Gion T, KanoT, et al. Hepatic resection for icteric type hepatocellular carci-noma. Hepatogastroenterology 1997;44:1432–7.
13. Huang GT, Sheu JC, Lee HS, Lai MY, Wang TH, Chen DS.Icteric type hepatocellular carcinoma: revisited 20 years later.J Gastroenterol 1998;33:53–6.
14. Lau WY, Leow CK, Leung KL, Leung TW, Chan MSY, Yu SCH.Cholangiographic features in the diagnosis and management ofobstructive icteric type hepatocellular carcinoma. HPB Surg 2000;11:299–306.
15. Wu CS, Wu SS, Chen PC, Chiu CT, Lin SM, Jan YY, et al.Cholangiography of icteric type hepatoma. Am J Gastroenterol1994;89:774–7.
16. Peng SY, Wang JW, Liu YB, Cai XJ, Deng GL, Xu B, et al.Surgical intervention for obstructive jaundice due to biliary tumorthrombus in hepatocellular carcinoma. World J Surg 2004;28:43–6.
17. Kondo M, Dono K, Sakon M, Nagano H, Hayashi T, Umeshita K,et al. Two cases of hepatocellular carcinoma with bile duct inva-sion, but without a detectable tumor in the liver (in Japanese withEnglish abstract). Jpn J Gastroenterol Surg 2003;36:482–7.
18. Soyer P, Sibert A, Laissy JP. Intrahepatic bile duct dilatationsecondary to hepatocellular carcinoma: CT features in 10 pa-tients. Abdom Imaging 1995;20:114–7.
19. Tseng JH, Hung CF, Ng KK, Wan YL, Yeh TS, Chiu CT. Icterictype hepatoma: magnetic resonance imaging and magneticresonance cholangiographic features. Abdom Imaging 2001;26:171–7.
20. Murakami Y, Yokoyama T, Kanehiro T, Uemura K, Sasaki M,Morifuji M, et al. Successful diagnosis and resection of icterictype hepatocellular carcinoma. Hepatogastroenterology 2003;50:1634–6.
21. Tada K, Kubota K, Sano K, Noie T, Kosuge T, Takayama T, et al.Surgery of icteric-type hepatoma after biliary drainage andtranscatheter arterial embolization. Hepatogastroenterology1999;46:843–8.
22. Jan YY, Chen MF. Obstructive jaundice secondary to hepatocel-lular carcinoma into the common bile duct: choledochoscopicfindings. Hepatogastroenterology 1999;46:157–61.