Embed Size (px)
Citation preview
Br. J. Surg. 1984, Vol. 71, January. 43-45
0. Klimach, B.L.W. Chapman, C.J. Underwood and D. Charlesworth University Department of Surgery, University Hospital of South Manchester, West Didsbury, Manchester M20 8LR, UK
Correspondence to: Mr D. Charlesworth
An investigation into how the geometry of an end-to-side arterial anastomosis affects its function
The efects of altering the geometry of an end-to-side junction Mwe investigated in a hydraulic model. The dimensions of the tubes, pressures and ,flow rate and the jeqirency of pulsation were calculated by dimensional anal-vsis, to produce a model which simulated pulsatile .flow in small arteries. The ratio between the impedance of the 'bypass' and the impedance downstream from the junction was greater than unity when the two tubes ,firming the junction were of unequal diameter. No increase in downstream impedance was measured when the angle of junction was increased,fiom 45" to 135". Cine photographs of streamlines at the junction showed that flow passed smoothlv through the junction irrespective o f angle and that perturbations occurred only during that part of the cycle when flow was rewrsed, The results indicate that the angle at which a ,junction is made afects , f lo~ ' . The efect is small and is onlv seen when the ratio of diameters of the tubes is unity. The ratio oj'rhe diameters o f the two tubes which make up the junction has the greatest eflect on ,flow through the junction. Keywords: Femoro-distal bypass, hydraulic model
Selection of suitable patients has considerable influence on the early results of femoro-distal bypass and the quality ofthe 'run off seems to be the dominant influence'. In our experience, gluteraldehyde-stabilized human umbilical vein probably works well when the 'run off into the foot is good, and we assume that when mean flow through the graft is high the velocity of flow is above the 'thrombotic threshold velocity'. It is possible that factors within the prosthesis (compliance) or in the operation (ratio of diameter of prosthesis to recipient artery, and the angle of anastomosis) may also affect adversely the results ofthe operation.
As surgeons, we have usually accepted the teaching that the angle at which an arterial anastomosis is made is important in that turbulence occurs if the angle is not oblique*. Distur- bances of flow (turbulence in the extreme case) cause loss of pulsatile energy and may contribute to failure of a bypass.
The optimum configuration of an anastomosis, in terms of the ratio of the area of cross-section of the bypass to that of the recipient artery, is known to be 1: 1.1 (Reference 3), but how the angle at which an anastomosis is fashioned, and the relative effect of this in relation to variation in the area ratio, is not known. Both factors might be expected to affect the trans- mission of pulsatile energy, and, within limits, both are variable.
If the geometry of an anastomosis is critical, a knowledge of factors which affect its efficiency may eliminate some early failures. We have investigated how variations in the angle of anastomosis and the area of cross-section of a bypass relative to the recipient vessel affect the impedance of the anas- tomosis and whether these variables cause disturbances in the pattern of flow.
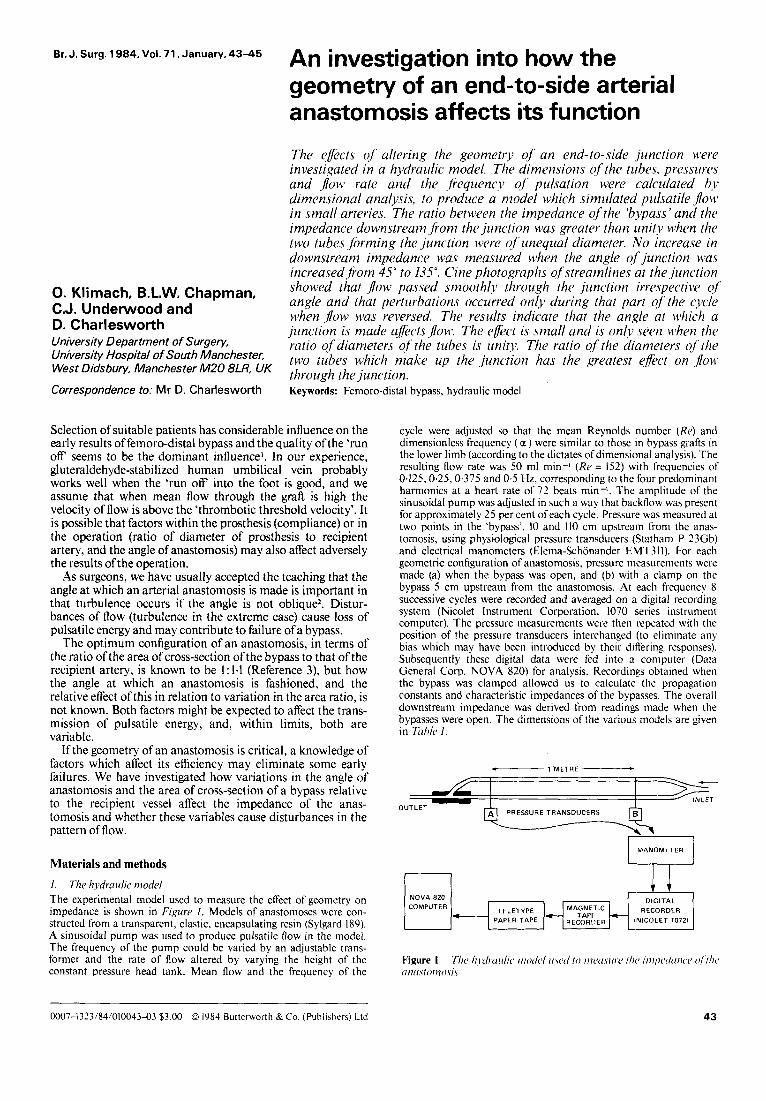
Materials and methods 1. The hydraulic model The experimental model used to measure the effect of geometry on impedance is shown in Figitre 1. Models of anastomoses were con- structed from a transparent. elastic, encapsulating resin (Sylgard 189). A sinusoidal pump was used to produce pulsatile flow in the model. The frequency of the pump could be varied by an adjustable trans- former and the rate of flow altered by varying the height of the constant pressure head tank. Mean flow and the frequency of the
cycle were adjusted so that the mean Reynolds number (Re) and dimensionless frequency ( a ) were similar to those in bypass grafts in the lower limb (according to the dictates of dimensional analysis). The resulting flow rate was 50 ml min-I (Re = 152) with frequencies of 0.125,0.25,0.375 and 0.5 Hz, corresponding to the four predominant harmonics at a heart rate of 72 beats min-I. The amplitude of the sinusoidal pump was adjusted in such a way that backflow was present for approximately 25 per cent of each cycle. Pressure was measured at two points in the 'bypass'. 10 and 110 cm upstream from the anas- tomosis, using physiological pressure transducers (Statham P 23Gb) and electrical manometers (Elema-Schonander EMT311). For each geometric configuration of anastomosis, pressure measurements were made (a) when the bypass was open, and (b) with a clamp on the bypass 5 cm upstream from the anastomosis. At each frequency 8 successive cycles were recorded and averaged on a digital recording system (Nicolet Instrument Corporation. 1070 series instrument computer). The pressure measurements were then repeated with the position of the pressure transducers interchanged (to eliminate any bias which may have been introduced by their differing responses). Subsequently these digital data were fed into a computer (Data General Corp. NOVA 820) for analysis. Recordings obtained when the bypass was clamped allowed us to calculate the propagation constants and characteristic impedances of the bypasses. The overall downstream impedance was derived from readings made when the bypasses were open. The dimensions of the various models are given in Tnhk 1.
. 1 METRE c
m
DIGITAL RECORDER
NOVA 820 COMPUTER
0007-13?3/84/01004343 $3.00 0 1Y84 Butterworth & Co. (Publishers) Ltd 43
Geometry of an end-to-side arterial anastomosis: 0. Klimach et al.
2. Theoretical model An electrical analogue of the hydraulic model is shown below (where ZU = upstream impedance, ZG = impedance of the bypass, Z v = impedance ofthe artery and ZD= downstream impedance).
ZG
ZU
zv
ZD
Pulse generator
The overall impedance Z = ZD + ZU + (-&+ ) -I zv
In the hydraulic model ZV and Zu were kept constant. ZG was measured for each of the tubes used in the experiments. ZD is the impedance downstream from the anastomosis and this impedance consists of two components, one of which is dependent on the effects of the angle of anastomosis and the ratio of cross-sectional areas of the two tubes, and the other ofwhich is constant.
3. Visualization ofthepatterns offrow The patterns of flow at the anastomosis were visualized by injecting a red dye (Biembrichs scarlet) into the bypass 10 cm upstream from the anastomosis, via a fine gauge needle connected to a constant infusion pump. The patterns of flow at the anastomosis were photographed using a high speed cine camera (Figure 2).
Results The effect of variations in the ratio of diameters of bypass and 'artery' and the angle of junction on impedance is shown in Table 2. The characteristic impedance of the bypass and impedance at the junction are given in columns 3 and 4.
No increase in downstream impedance was produced when the angle of the anastomosis was increased from 45 to 135". The ratio between the impedance of the bypass and down- stream impedance was found to be greater than unity when the bypass and 'artery' were of unequal internal diameter. The ratio was close to unity when bypass and 'artery' were of equal size.
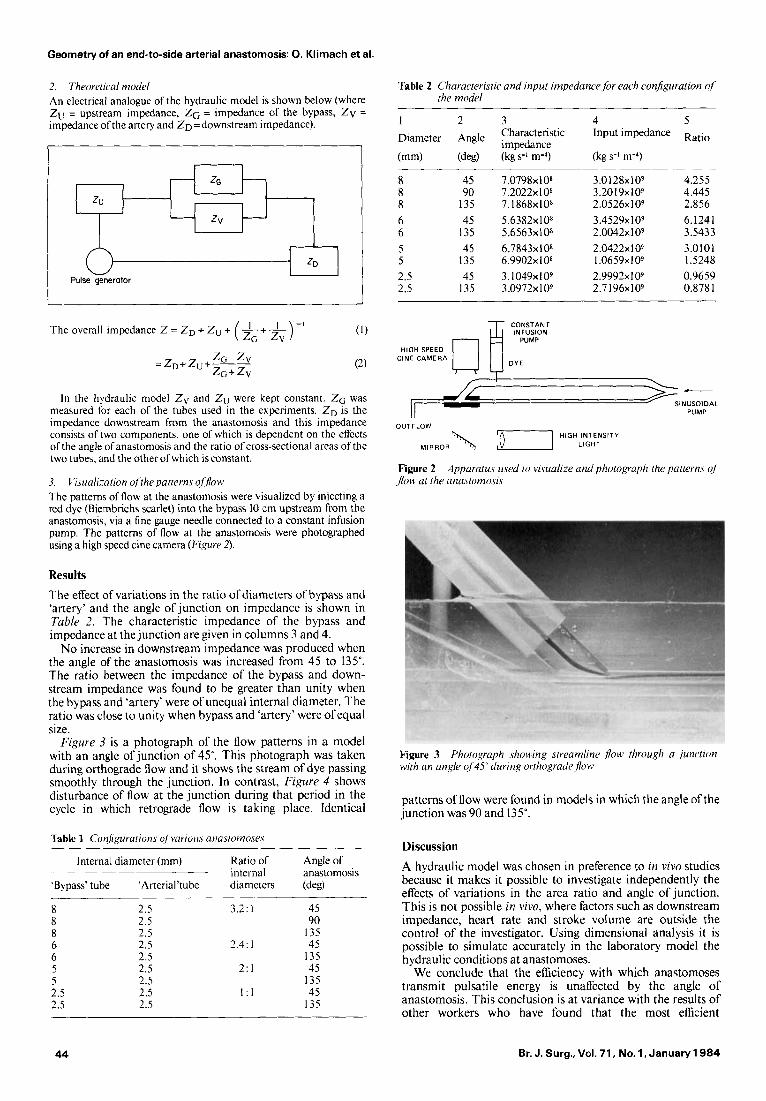
Figure 3 is a photograph of the flow patterns in a model with an angle of junction of 45". This photograph was taken during orthograde flow and it shows the stream of dye passing smoothly through the junction. In contrast, Figure 4 shows disturbance of flow at the junction during that period in the cycle in which retrograde flow is taking place. Identical
Table 1 Conhnuraiions o/ vuriou.\ anasiomoses
Internal diameter (mm) Ratio of Angle of internal anastomosis
'Bypass' tube 'Arterial'tube diameters (deg)
2.5 2.5
2.5 2.5 2.5 2.5 2.5 2.5 2.5 2.5 2.5
3.2: 1 45 90
I35 2.4: 1 45
135 2: I 45
135 I : I 45
I35
Table 2 Characteristic and input impedance,for each configuration of' the model
1 2 3 4 5 Diameter Angle Characteristic Input impedance Ratio
(mm) (deg) (kg s-l m-4) (kg s-' m-4) impedance
8 8 8 6 6 5 5 2.5 2.5
45 90
135 45
135 45
135 45
135
7.0798~1 O* 7 .2022~10~ 7.1868~10~ 5.6382~10~ 5.6563~10~ 6.7843~10~ 6.9902~10~ 3.1049~1 O9 3.0972~ 1 O9
3.0128~10~ 3.20 19x109 2.0526~10~ 3.4529~10~ 2.0042~1 O9 2.0422~ I O9 1.0659~10~ 2.9992~ I O9 2.7 1 96x109
4.255 4.445 2.856 6.1241 3.5433 3.0101 1.5248 0.9659 0.878 1
CONSTANl
HIGH SPEED CINE CAMERA
OUTFLOW "., HIGH INTENSITY LIGHT MIRROR
Figure 2 Apparatus used to visualize and photograph the patrerns of ,flow at the anastomosis
Figure 3 with an ungle of 45" during orzhogradefloM3
Photograph \houing streamline flow through a junction
patterns of flow were found in models in which the angle of the junction was 90 and 135".
Discussion A hydraulic model was chosen in preference to in vivo studies because it makes it possible to investigate independently the effects of variations in the area ratio and angle of junction. This is not possible in vivo, where factors such as downstream impedance, heart rate and stroke volume are outside the control of the investigator. Using dimensional analysis it is possible to simulate accurately in the laboratory model the hydraulic conditions at anastomoses.
We conclude that the efficiency with which anastomoses transmit pulsatile energy is unaffected by the angle of anastomosis. This conclusion is at variance with the results of other workers who have found that the most efficient
44 Br. J. Surg., Vol. 71, No. 1, January 1984

Geometry of an end-to-side arterial anastomosis 0. Klimach et al.
anastomosis is one with an acute angle ofjunction. In a study of bypass grafts across the iliofemoral arteries of dogs, Szilagyi ef aI.* estimated that an anastomosis constructed at an angle of 90" was 37 per cent less efficient, in terms of volume flow, than an anastomosis constructed at an acute angle. This work, however, applied only to the proximal anastomosis. Schultz and Strandness' measured the pressure and flow through bypasses across aorto-iliac segments removed at autopsy. They concluded that anastomoses constructed at 90" produce higher pressure gradients than anastomoses constructed at 45", particularly at high flow rates. However, no account was taken of the variations in the relative cross-sectional areas of the arteries: this could equally explain their observations.
Conversely, Blaisdell el d . 4 , in a study of bypasses across aorto-iliac arteries of dogs, were unable to demonstrate reduced flow through bypasses in which the angles of the proximal and distal anastomoses were reversed, i.e. greater than 90'. Our own results support the conclusions obtained by Blaisdell and also show that the closest agreement between the impedance of the junction and the downstream impedance occurred when the diameter ofthe bypass was identical to that of the 'artery'. If the impedance of junction differs from downstream impedance then reflections will occur at the junction. Reflected waves interact with the primary waves and cause loss of energy5. It is therefore desirable to avoid any impedance mismatch at a vascular anastomosis and our results, which are also in agreement with those of Newman el d . 6 , show that this can only be achieved when the diameter of the bypass and recipient artery are nearly equal.
It has been suggested that the angle at which a junction is made is related to the degree of disturbance in flow7. Our studies do not support this view. We found that streamline flow occurred across the junction during constant flow even when the angle was 135". Disturbance in the patterns of flow was found only in pulsatile flow and only during that portion of the cycle in which deceleration of flow occurred. No corre- lation was found between the angle at which the anastomosis was made and the amount of disturbance in flow. It has been suggested that disturbances of flow at vascular anastomoses may also be responsible for the formation of neointimal hyperplasiag?Y but, since our results show that the angle at which the anastomosis is made is not related to the extent of disturbances in flow, we feel that it seems unlikely to be a contributory factor.
Conclusion We conclude that the angle at which a vascular anastomosis is made has little effect on losses of pulsatile energy or on the degree of disturbances of flow which occurs at the junction, but a discrepancy in diameter between bypass and artery will lead to significant losses in pulsatile energy.
Figure 4 Photograph showing flow distzrrbatice in u model tt i th uri angle ofjitrzction ~1 '45" diiring retrograde f l o ~ ,
References I .
2.
3.
4.
5.
6.
7.
8.
9.
Klimach 0, Charlesworth D. Factors which affect the patency of Femoro-tibia1 bypasses for limb salvage. Br J Surg 1983; 70: 1-3 Szilagyi DE, Whitcomb JG, Schenker W, Waibel P. The laws of fluid flow and arterial grafting. Sicrgerv 1960; 47: 55-73 Schultz RD, Hokanson DE, Strandness DE. Pressure-flow relations of the end-to-side anastomosis. Surgery 1967; 52:
Blaisdell WE, Stuart FP, Hall AD. The effect of diameter and angulation on blood flow through plastic arterial substitute. h i Surg 1964; 30: 192-196 Logerfo FW, Songrant T, Tee1 T, Dewey CF. Boundary layer separation in modes of side-to-end arterial anastomoses. Arch
Newman DL, Gosling RG, Bowden NLR et al. Pressure amplitude increase on unmatching the aorto-iliac junction ofthe dog. Cardiovasc Res 1972; 6: 1-8 Crawshaw HM, Quist WC, Serrallach E, Valeri R, Logerfo FW. Flow disturbance at the distal end to side anastomosis. Arch S1tr;c:
Macan E, Noseda G, Longo T. Approach to fluid dynamic problems in reconstructive vascular surgery. Surgry 1969; 66: 994-1003 Szilagyi DE. Elliott JP. Hageman JH, Smith RF, Dall'olmo CA. Biologic forte of autogenous vein implants as arterial substitute. Ann Siirg1973; 178: 232-242
319-324
S W ~ 1979; 114: 1369-1373
1980; 115: 1280-1284
Paper accepted 5 May 1983
Br. J. Surg.. Vol. 71, No. 1, January 1 9 8 4 4 5