Embed Size (px)
Citation preview
An Open Clinical Trial of Buspirone in Children WithAttention-Deficit/Hyperactivity Disorder
SAV1TA MALHOTRA, M.D., PH.D., AND PARAMALA]ANARDHANAN SANTOSH, M.D., M.R.C.PsYCH.
ABSTRACT
Objective: The efficacy of buspirone in controlling the symptoms of children with attention-deficit/hyperactivity disorder
(ADHD) was examined in 12 children with ADHD. Buspirone was used solely in all the children. Method: Twelve children
(10 boys and 2 girls) aged between 6 and 12 years (mean age 8.2 years) with hyperkinetic disorder were studied.
Standard rating scales such as the Conners Parent Abbreviated 10-ltem Index (CPAI) and the Children Global
Assessment Scale (CGAS) were used to collect data on the symptoms of ADHD. Visual analog scores were also
obtained about the dimensions of hyperactivity, impulsivity, inattention, and disruptive behavior. All the subjects were
given buspirone in the dose of 0.5 mg/kg body weight per day. The dose range of buspirone used was 15 to 30 mg/day,
given in b.i.d, dosages. The subjects continued the regimen for a period of 6 weeks. The ratings were done at baseline,
1 week, 2 weeks, 4 weeks, and 6 weeks after starting buspirone. A detailed side effect checklist was administered at the
same intervals. The CPAI was also repeated after 2 weeks of discontinuation of buspirone. Results: When compared
with baseline scores, all 12 subjects had shown significant improvement in hyperactivity, impulsivity, inattention, and dis
ruptive behavior. The mean (SD) CPAI score improved from 24.75 (2.7) at baseline to 11.25 (2.73), and the CGAS scores
improved from 36.6 (5.58) to 67.1 (7.31) during the 6-week period of the study. The only side effect reported was mild
dizziness, during the first week, by two subjects. Stopping the drug at the end of the study period of 6 weeks resulted in
the reemergence of the symptoms. Conclusion: Buspirone showed a favorable side effect profile and significantly
reduced the symptoms of ADHD. It appears equally effective in improving the varied symptoms of the disorder. These
preliminary findings of apparent efficacy of buspirone for ADHD in children indicate that future controlled trials are
warranted. J. Am. Acad. Child Ado/esc. Psychiatry, 1998,37(4):364-371. Key Words: attention-deficit/hyperactivity dis
order, hyperkinetic disorder, buspirone, clinical trial.
Attention-deficit/hyperactivity disorder (ADHD) is characterized by inattentiveness, distractibility, hyperactivity,associated emotionality, and apparent intrusiveness ordestructiveness arising from impulsivity. Hyperkinetic
Accepted Nouember 5, 1991.Dr. Malhotra is all Additional Professor ill the Department of Psychiatry.
Postgraduate Institute of Medical Education and Research (PGIMERJ.
Chandigarb, India. Dr. Santosh was a Senior Resident ill the Department of
Psychiatry, PGIMER, when this study was conducted. Currently, he is a
Specialist Registrar ill Child and Adolescenr Psychiatry, Maudsley Hospital.
London.
The authors ackllowled,ge the assistance ofDr. Asba V Hareendran and Dr.
Praueen Fernandes ill the preparation Of this manuscript. The authors are l'ery
grateful to the two anon.ymou5 reviewers [or their ualuable comments lindsuggestiollS.
Reprint requests to Dr. Santosh, Specialist Registrar ill Child and Adolescent
Psychiatry. Maudslry Hospital, Denmark Hill, London SE58AZ, England.fax:
00441717080776.0890-8567/98/3704-0364/$0.1.001010 1998 by the American Academy
of Child and Adolescent Psychiatry.
364
disorder (HD) is a narrower diagnosis and is a subgroupof ADHD with implications different from those ofother disturbances such as conduct disorder (Hinshaw,1994; Taylor et al., 1986, 1991). Inattention is a requiredcriterion for HD but not for ADHD; children with HDshould correspond to the combined attention-deficit/hyperactivity subtype of ADHD (American PsychiatricAssociation, 1994), as well as meet stricter criteria for thepervasiveness of disorder across situations and theabsence of other psychiatric disorders such as anxietystates (World Health Organization, 1992). In the UnitedStates, one child in 20 meets the DSM-IV diagnosticcriteria for ADHD. The prevalence in Europe seems tobe much lower,about 1 in 200, mainly because Europeanpsychiatrists use the narrower ICD-JO diagnosis of HD.
Children with HD are at considerable developmentalrisk and have high rates of language and motor delays.They are prone to develop antisocial conduct disorders.
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, .\7:4, APRIL 1998

Severe hyperactivity may continue into adolescence andadult life and is a risk for social adjustment, evenwhen account is taken for coexistent conduct disorder(Farrington et aI., 1990; Gittelman et aI., 1985; Taylorand Hemsley, 1995).
The neurochemical basis of ADHD is still unclear.However, the features of ADHD and HD can berelieved with catecholamine-releasing drugs such asmethylphenidate, implying an underlying impairmentin dopaminergic function (Cook et al., 1995; Raskinet al., 1983; Shaywitz et aI., 1977, 1984) and noradrenergic function (Raskin et al., 1983; Shekim et al., 1979).
Pharmacotherapy with psychostimulants is one ofthe key elements in the treatment of ADHD. Acrossseveral studies, up to 70% of ADHD children treatedwith stimulants have been reported to exhibit a significant clinical response (Greenhill, 1992). In a recentstudy of 76 children with ADHD, methylphenidatetreatment normalized classroom behavior in 78% of thechildren whereas only 50% of the subjects reached thislevel when academic functioning was assessed (Rapportet al., 1994). However, because stimulants have sideeffects such as insomnia, tics, irritability, and anorexia,their use may be limited. Another significant problem isthat commonly prescribed stimulants such as methylphenidate and d-amphetamine have relatively shortperiods of action of 3 to 4 hours. In a routine schedule,dosages are administered in the morning and at noon.Behavioral improvements may be more conspicuousduring the daytime in school than in the evening athome. Finally, with stimulants there is a potential risk ofabuse and drug dependence, in particular with respectto adolescent ADHD patients and their social confederates. These shortcomings have forced a search foralternative medication for the treatment of ADHD.
Recent investigations into the effects of tricyclicantidepressants (TCAs) in ADHD have used morerobust dosages and examined the effects of commoncomorbid disorders such as depression, anxiety, and ticdisorders (Spencer et aI., 1994). TCAs may be moreeffective than stimulants for patients with comorbid disorders. Stimulant-nonresponsive ADHD may alsorespond to TCAs (Spencer et al. 1994). Youths withADHD (who may have had other comorbid disorders)have also been reported in an open case series to haveresponded to fluoxetine (Barickman et al., 1991).
Clonidine, an aradrenergic agonist, has also beenused with good results in ADHD and has been shown
]. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, .n,4, APRIL 1998
BUSPIRONE TRIAL FOR ADHD
in placebo-controlled trials to significantly attenuatehyperactivity and disruptive behaviors in children whohave ADHD (Gunning, 1992; Hunt et al., 1985).
The current practice of treating children with ADHDwith stimulants shows that up to 30% of them do notrespond. In India, the management of HD poses a special problem. The stimulants, which are considered asthe first line of pharmacotherapy, are not available. Currently, management primarily comprises psychoeducation, parental counseling, and using cognitive strategies,along with TCAs or clonidine. Therefore, we were onthe lookout for an alternative pharmacological agentthat was locally available and effective in HD.
Buspirone, an anxiolytic agent, was first synthesizedby Woo and Raeburn in 1972. Buspirone displays highaffinity and selectivity for the serotonin 5-HT1A receptor subtype (Temple et al., 1982). The 5-HT1A receptorsare localized in the presynaptic region of the serotonergic neurons in the raphe nucleus and are found in highconcentrations on target neurons in the hippocampusand septum. They are thus present both presynapticallyand postsynaptically. Presynaptically the 5-HT1A sornatodendritic receptor functions as an autoreceptor thatpotently inhibits the firing of serotonin neurons andreduces its synthesis, while it is a partial agonist at thepostsynaptic 5-HT IA receptors (Andrews and File,1993). The neurochemical and clinical effects of buspirone represent both its presynaptic and postsynapticactions. Conceivably, in some cases buspirone mayenhance, and in others, decrease serotonin neurotransmission (Sussman, 1994). Buspirone also has an affinityfor 5-HT2 receptors which might contribute to itstherapeutic efficacy (Taylor and Hyslop, 1991). Buspirone also has a modest effect on the dopamine systemand enhances dopamine synthesis and release (Tunicliffet al., 1992). It blocks the presynaptic dopaminergicreceptors rather than the postsynaptic dopaminergicones. This increases the firing of the midbrain neuronsand blocks the inhibiting effects of y-aminobutyric acidon dopaminergic neurons in the zona compacta of thesubstantia nigra (Eison and Temple, 1986).
Buspirone is also a partial agonist of a-adrenergicreceptors (Castillo et aI., 1993) and has been shown toincrease the spontaneous firing of noradrenergic neurons in the locus ceruleus (Sanghera et aI., 1983). Buspirene's major metabolite, 1,2-pyrimidinyl piperazine(I-PP), has a 15 to 30 times higher concentration of 1PP in the brain than the parent compound. I-PP binds
365

MALHOTRA AND SANTOSH
with uz-receptors and produces anticonflicr activity inrats (Gam mans et al., 1983). Thus, buspirone haseffects on monoaminergic systems which are akin tosome of the effects of methylphenidate, amphetamine,and TeAs individually. It was therefore hypothesizedthat buspirone would help in controlling inattention,hyperactivity, impulsivity, and also the behavioral problems associated with ADHD.
Buspirone has a number of potential advantages foruse with children. Side effects to buspirone are uncommon and are only mild or moderate when they dooccur. Since 1984, buspirone has been used in childrenand adolescents with anxiety disorders, and researchershave reported significant improvement with it (Balon,1994; Kranzler, 1989; Levine, 1988; Simeon et al.,1994; Zwier and Rao, 1994). The reported side effectswere very mild and included nausea, headaches, daytime tiredness, and increase in weight occasionally.However, Soni and Weintraub (1992) reported twocases of behavioral toxicity in children who were treatedfor anxiety with buspirone. They concluded thatalthough buspirone has been found to be useful in children, it appears that in certain individuals it may aggravate an underlying predisposition to psychosis and/oraggression. The other reported side effects are dizziness,light-headedness, diarrhea, paresthesia, excitation,sweating, and clamminess.
Ratey et al. (1989) used buspirone in the treatmentof nine developmentally disabled children who demonstrated anxiety as well as aggressive and self-injuriousbehavior. They demonstrated marked decrease inaggression, tantrum, anxiety, and self-injurious behavior. Realmuto et al. (1989) conducted an open-blind 4week trial in autistic children comparing buspirone withmethylphenidate and fenfluramine. Two of the threechildren with hyperactivity as the target symptomimproved with buspirone. Behavioral toxicity was seenin one of the two children treated with methylphenidateand a mild improvement in another with fenfluramine.No side effects were noted with buspirone. Quaisonet al. (1991) reported a case of an 8-year-old boy with adiagnosis of ADHD and conduct disorder who wasbeing treated with buspirone; the boy was initially given5 mg three times daily, and the dosage was graduallyincreased to 15 mg three times daily. Gradual cessationof aggressive behavior was reported.
More recently, Gross (1995), in a letter to the editor,reported on 50 children and adolescents of normal
366
intelligence with both ADHD and oppositional defiantdisorder, whose ADHD symptoms were significantlyhelped by the standard medications but whose oppositional symptoms remained a major problem. Buspironewas added as an adjunct to the medication or medications used for treating ADHD (average dose varyingbetween 15 and 60 mg of buspirone per day). Theratings made by parents showed an improvement inoppositional symptoms in approximately 90% of thesubjects . The greatest benefit appeared to be in improving self-control and reducing irritability, aggression, andtemper outbursts. Side effects were minimal and onlyrarely interfered with treatment.
In summary, all previous studies with buspirone havebeen conducted on poorly characterized, heterogeneousgroups, under open conditions. Despite case reportsabout improvement in hyperkinetic sympto ms andbehavioral symptoms in children, buspirone has notbeen tried as the sole treatment in children with ADHDor HD. Therefore, we felt that busp irone was an idealcandidate to be used in an open trial to investigate itseffect on the various symptoms of HD.
METHOD
Subjects
The sub jects were recruited from the Child Guidance Clinic,Department of Psychiatry, Postgraduate Institute of MedicalEducation and Research (PGIMER), Chandigarh, India . An ICD/0 diagnosis of HD was made after a det ailed psychiatri c interviewwith both the parents and the child and a playroom assessment bythe child psychologist. Of the 12 children (10 boys and 2 girls)meeting the ICD-/O criteria for the diagnosis of hyperkinetic disorder F90 (i.e., attention deficit disorder with hyperactivity andimpulsivity of the DSM-IV) , who entered the study, 4 had acomorbid conduct disorder (ICD-JO hype rkinetic conduct disorder). None of the subjects had anxiety disorder or any othercomorbid disorder. The children were aged between 6 and 12 years(mean age 8.2 years) and had an IQ of at least 70. Informed consentwas obtained from the parent s of the child ren who entered thestud y. None of the subjects had responded to an earlier package ofan adequate dosage of a TCA, psychoeducat ion of parents, andcognitive strategies used routinely in the C linic. None of them hadreceived any other medication for the man agement of the disorder.All 12 children were free of any medication for at least 6 weeks priorto entering the study. They were followed up for a period of 8 weeksafter entering the study, and none of them dropped out during th isperiod .
Experimental Procedure and Tests
The subjects initially und erwent an IQ assessment using Malin'sIntelligence Scale for Indi an Children . This is a standardizedinstrument used frequentl y in research. Their mean IQ was 86.4
]. AM . ACAD . C H I L D AD OL ESC . PSYCHIATRY, 37:4, APRIL 1998
(range 76 to 108). This was probably an underest imate of theiractual potential . arising from their poor ability to sustain attentionand impulsive responses during the tests . The Conners ParentAbbreviated IO-Item Index (CPAI) (Goyerte et al., 1978) was usedto rate the child's symptoms. and the Children's Global AssessmentScale (CGAS) (Shaffer et al., 1983) was used to rate their overallfunctioning. Symptoms used by the ICD-JO to make a diagnos is ofHD were classified into the "i narrenrion," "hyperact ivity," and"impulsivity" domains, and the sympto ms of disruptive beha viorwere used as the "behavior" domain. Parents were questioned aboutthese domains in detail and were asked to rate each of the fourdomains using a global visual analog score at each visit. The reliability coefficient (a) , using app ropr iate modification for nonsrandardized scales (based on average covariances), was .89 for this scale.A reliab ilit y coe fficien t of >.7 0 is generally acce pted as good(Cronbach, 195 I). The subjects were also administered a "buspironeside effect checklist" which had been compiled by the investigators,consisting of all the side effects reported in literature for buspirone.A provision for documenting any new side effect was incorporatedinto it.
Setting and Procedure
All subjects were treated as outpatients, and the parents wereallowed to contac t the investigators at any time if they suspected anyuntoward effects of the med icat ion . It was made clear that the subjects could Opt out of the stud y at any point if they wished to do so.Permission from the ethical committee of the PGIMER had beenobtained for the study. All subjects received buspirone, 0.5 mg/kgbody weight per day. The dosage of buspirone varied between 15and 30 rng/d ay, given in a b.i.d dose schedule. All subjects weregiven the full dose of buspiro ne from the start of the trial. The subjects were assessed on day 0, 7 . 14, 28. and 42. T he assessment ateach visit included the CPAI ; CGAS ; assessment of the dimen sionsof hyperactivity, inattention , impul sivity. and behavioral problems
BUSPIRON E TRIAL FOR ADHD
using a visual analog scale; and the buspirone side effect checkl ist.Drug compliance was ensured through regular inquiry, suggestion ,and pill count. A CPAI assessment was also repeated 2 weeks afterdiscontinuation of buspirone.
RESULTS
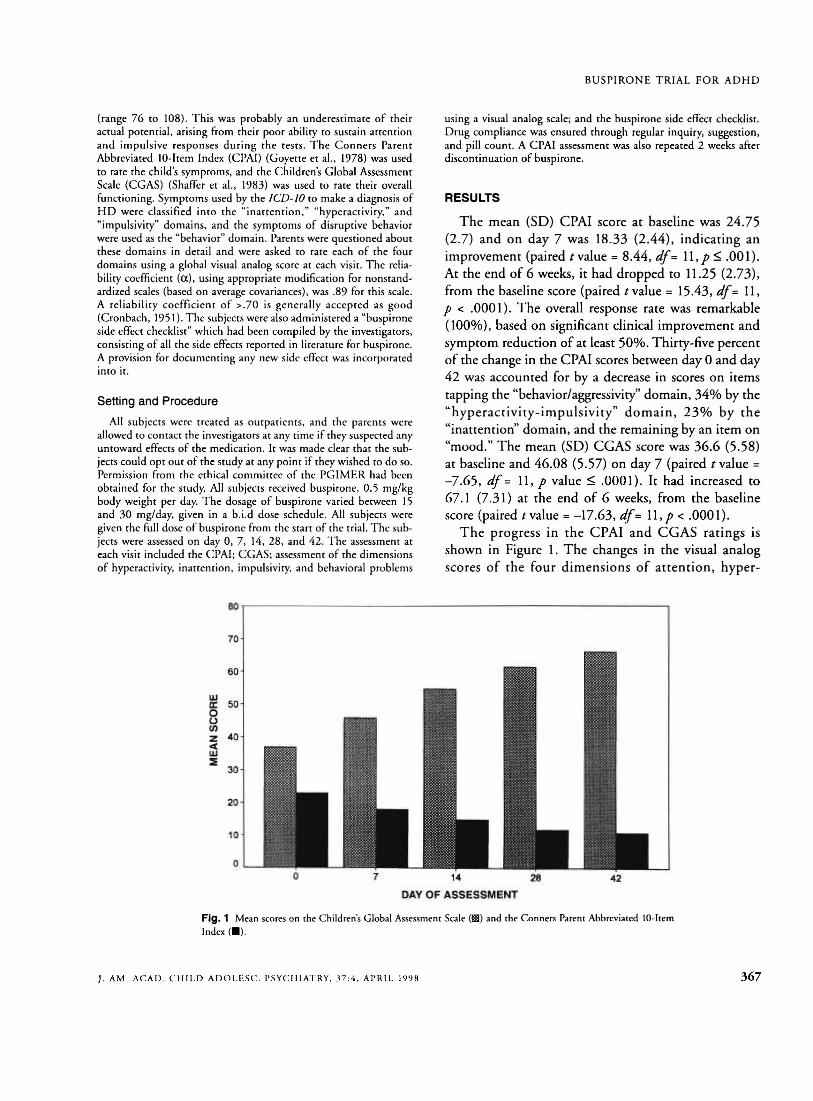
The mean (SO) CPAI score at baseline was 24.75(2.7) and on day 7 was 18.33 (2.44), indicating animprovement (paired tvalue = 8.44, df= 11,p ~ .001).At the end of 6 weeks , it had dropped to 11.25 (2.73),from the baseline score (paired t value = 15.43, df= 11,P < .0001). The overall response rate was remarkable(100%), based on significant clinical improvement andsymptom reduction of at least 50%. Thirry-five percentof the change in the CPA! scores between day 0 and day42 was accounted for by a decrease in scores on itemstapping the "behaviorlaggressiviry" domain, 34% by the"hyperactivity-impulsivity" domain, 23% by the"inattent ion" domain, and the remaining by an item on"mood." The mean (SO) CGA5 score was 36.6 (5.58)at baseline and 46.08 (5.57) on day 7 (paired t value =
-7.65 , df = 11, P value ~ .0001). It had increased to67.1 (7.31) at the end of 6 weeks , from the baselinescore (paired tvalue = -17.63, df= 11 ,p < .0001).
The progress in the CPAI and CGA5 ratings isshown in Figure 1. The changes in the visual analogscores of the four dimensions of attention, hyper-
eo
70
60 '
wa: 500u(f)
Z 40.q;w::E
30
20
10
07 14
DAY OF ASSESSMENT
28 42
Fig. 1 Mean scores on the Children's Global Assessment Scale (1IlII) and [he Conners Parent Abbreviated lO-ltemIndex (_).
J. AM. ACA D . C H I L D ADOL E SC. PSYCHIATRY, .P :4 . APRIL J<)')M 367
6
MALHOTRA AND SANTOSH
10 .,----- - - - - - - - - - - - - - - - - - - - - - - - - - - -----.
6
uJa:ouCIlZ<l:
~ 4
2
oo 7 14 28
DAY OF ASSESSMENT42
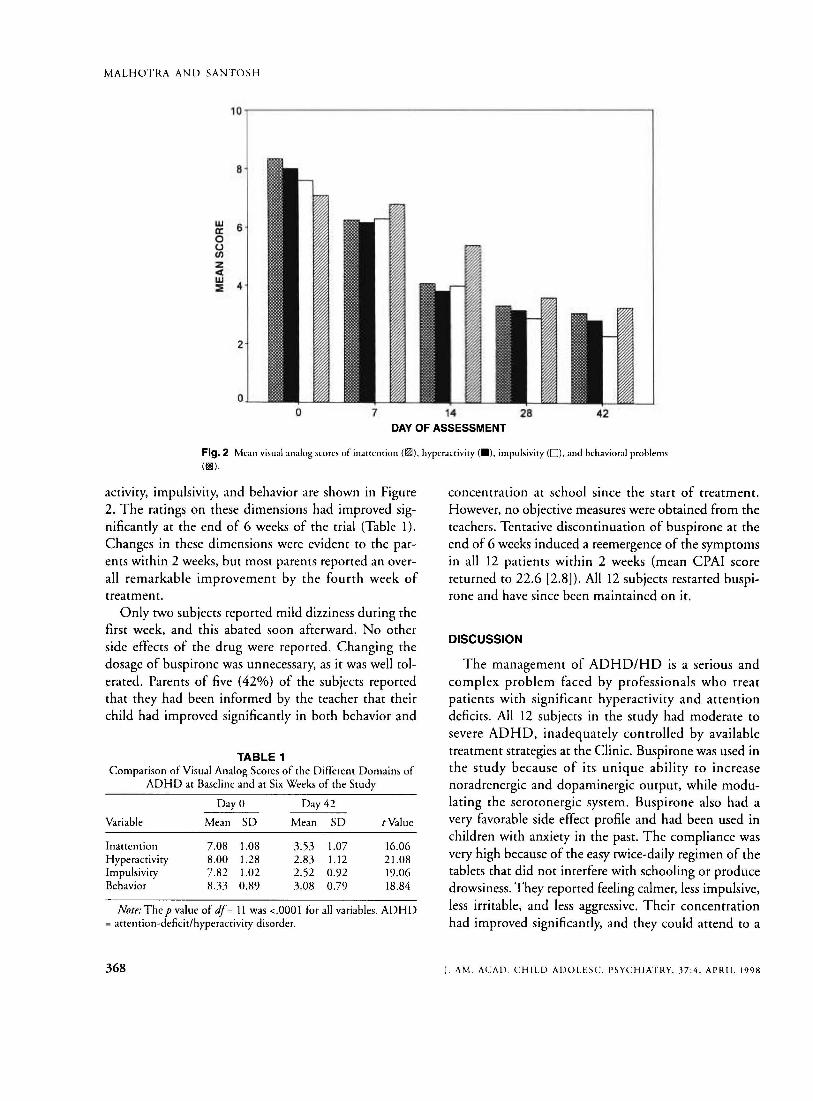
Flg.2 Mean visual analog scores of inattention (~), hyperacriviry (_), impulsiviry (0), and behavioral problems
(1IlIl).
activity, impulsivity, and behavior are shown in Figure2. The ratings on these dimensions had improved significantly at the end of 6 weeks of the trial (Table 1).Changes in these dimensions were evident to the parents within 2 weeks, but most parents reported an overall remarkable improvement by the fourth week oftreatment.
Only two subjects reported mild dizziness during thefirst week, and this abated soon afterward. No otherside effects of the drug were reported. Changing thedosage of buspirone was unnecessary, as it was well tolerated. Parents of five (42%) of the subjects reportedthat they had been informed by the teacher that theirchild had improved significantly in both behavior and
TABLE 1Comparison of Visual Analog Scores of the Different Domains of
ADHD at Baseline and at Six Weeks of the Study
Day 0 Day 42
Variable Mean SO Mean SO tValue
Inattention 7.08 1.08 3.53 1.07 16.06Hyperactivity 8.00 1.28 2.83 1.12 21.08Impulsivity 7.82 1.02 2.52 0.92 19.06Behavior 833 0.89 3.08 0.79 18.84
Note: The p value of df= 11 was <.0001 for all variables. ADHD= attention-deficit/hyperactivity disorder.
368
concentration at school since the start of treatment.However, no objective measures were obtained from theteachers. Tentative discontinuation of buspirone at theend of 6 weeks induced a reemergence of the symptomsin all 12 patients within 2 weeks (mean CPAI scorereturned to 22.6 [2.8]). All 12 subjects restarted buspirone and have since been maintained on it.
DISCUSSION
The management of ADHD/HD is a serious andcomplex problem faced by professionals who treatpatients with significant hyperactivity and attentiondeficits. All 12 subjects in the study had moderate tosevere ADHD, inadequately controlled by availabletreatment strategies at the Clinic. Buspirone was used inthe study because of its unique ability to increasenoradrenergic and dopaminergic output, while modulating the serotonergic system. Buspirone also had avery favorable side effect profile and had been used inchildren with anxiety in the past. The compliance wasvery high because of the easy twice-daily regimen of thetablets that did not interfere with schooling or producedrowsiness. They reported feeling calmer, less impulsive,less irritable, and less aggressive. Their concentrationhad improved significantly, and they could attend to a
J. AM. ACAD, CHILD ADOLESC. PSYCHIATRY, .H:4. APRIL 1998

task for much longer. Their social interactions were alsoreported to have improved significantly. There was norebound worsening of symptoms or tolerance developing during the convenient twice-daily schedule of thedrug treatment. It is significant to note that the ratingsof all four dimensions of attention, hyperactivity,impulsivity, and behavioral problems, as recorded usinga visual analog scale, had improved significantly withbuspirone. As far as we are aware, this is the first reportof buspirone being used as rnonorherapy for the management of children with ADHD with or without conduct problems. Another significant finding was thatapart from a decrease in the CPAI scores, the childrenactually showed a general improvement in CGASratings, indicating that there was a generalization of thebenefits accrued, into global functioning. This coordinated use of global and syndrome-specific scaleshelped us to be more confident about the impact ofbuspirone on these children with HD. Issues such asrebound worsening of symptoms and tolerance to themedication did not seem to be a problem in these children. Though very encouraging, the results of the studyneed to be reconfirmed using double-blind crossovertrials in different sett ings.
The significant improvement in impulsivity andhyperactivity is in keeping with the report by Mandoki(1994), on a 6-year-old boy whose symptoms ofADHD after head trauma improved with buspirone.The improvement in behavioral problems in our subjects is similar to that reported by Gross (1995) in a tr ialof buspirone as an adjunct to standard medication forchildren with ADHD whose oppositional defiant disorder symptoms remained a major problem. Unlike theearlier investigators, however, we found that the children improved in all spheres despite receiving rnonotherapy with buspirone.
Researchers interested in the biological basis ofADHD have focused on the interactions of the prefrontal cortex with the caudate (Hynd et aI., 1993; Louet al., 1989 ; Roeltgen and Schneider. 1994) and thebrainsrern's dopamine and noradrenergic systems(Shaywitz er al., 1978) . Many stud ies suggest thatdopaminergic dysfunction is associated with ADHD(Cook et al., 1995; Raskin et al., 1983; Shaywitz et al.,1977, 1984; Sokol et al. 1987) . Magnetic resonanceimaging studies in children with ADHD have revealedabnormalities in brain structu res that are normally richin dopamine receptors, such as reduced volume of
J. AM . AC A D . C H IL D ADO L ESc:. PSY CHIATRY. .n :4 . APRIL 19 98
BUSPIRONE TRIA L FOR ADHD
prefrontal cortex and caudate nucleus, especially on theright side (Castellanos et al. , 1996). Recently, thedopamine hypothesis has been further supported by thefinding of an unusually high frequency of the sevenrepeat form of the dopamine receptor gene DRD4 inchildren with ADHD and a correspondingly lowfrequency of the four repeat allele, which is by far thecommonest form in the general population (Lahosraet aI., 1996). Dopamine has been hypothesized toimprove prefrontal function through intensifying theappropriate signal by exciting delay-related firing in cellswith specific mnemonic fields (Sawaguchi et aI., 1990).Norepinephrine depletion in rodents results in increaseddistractibility (Carli et aI., 1983; Roberts et aI., 1976)and motor hyperactivity (Pearlson and Robinson, 1981;Raskin et al., 1983). Postjunctional stimulation of Cl.2A
noradrenergic receptors by Cl.ragonists results in cognitive enhancement (Arnsten and Cai , 1993; Arnstenet al., 19%) and probably aids the inhibition of irrelevant sensory stimulation, thus providing a protectiveframework during cueing and delay periods (Li andMei , 1995). Serotonergic dysfunction is rarely implicated in pure ADHD, while it is usually linked toADHD with comorbid aggression or mood problems.Children with ADHD and comorbid conduct disordershow 5-HT dysfunction (Stoff et al., 1987), andaggressive children with ADHD show greater 5-HTdy sfunction than do nonaggressive children withADHD (Halperin et al., 1994; Krue si et aI., 1990,1992). Data suggest that aggressive and non aggressivechildren with ADHD represent partially distinct subtypes, with nonaggressive children having greatercognitive deficits and aggressive children having greaterpsychosocial disturbances (Halperin er al., 1990;Realmuto er al., 1989). Thus, in summary, centralnoradrenergic and dopaminergic mechanisms probablyunderlie attention deficits, while serotonergic mechanisms, though not directly implicated in ADHD,appear to be related to ADHD comorbid with aggression or mood disturbance and may be important in thebehavioral disturbances associated with ADHD.However, it is vital to realize that the various monoaminergic circuits do not function in isolation and areinterconnected and modulate one another.
The limitations of this study include its small samplesize, lack of a control group, absence of objective ratingsby teachers, and lack of neuropsychological assessmentof atren rional processes and impulsivity. One has to
369

MALHOTRA AND SANTOSH
remain cautious in interpreting the results as largerstudies are necessary to rule out a general "calming"effect which results mainly in reduction of motoractivity. It could be argued that all 12 children did havesignificant behavioral disturbances because of theseverity of the disorder, and it remains to be seenwhether buspirone would produce similar improvementwhen used in milder cases of ADHD.
Future studies should include relevant neuropsychological testing and teacher assessment scales to get aglobal understanding of the improvement in these children. Other important issues to be looked into areregarding the minimal dosage necessary for response,the duration of treatment, and the effect of buspironeon the different DSM-IV subtypes of the disorder. Adouble-blind, placebo-controlled study looking into theeffect of buspirone on ADHD is already in progress inthe Clinic.
Clinical Implications
The differential neuromodulation of multiple neurotransmitters by buspirone possibly explains its relativelyquick response in ADHD, in comparison with itsresponse in other disorders. It could be hypothesizedthat the serotonergic modulation by buspirone couldhave resulted in improved behavior and impulsivity,while the dopaminergic and noradrenergic effects ofbuspirone could have resulted in improved attentionspan and hyperactivity. A very significant differencebetween buspirone and the stimulants is its excellentside effect profile and the ease of the therapeuticregimen. The taboo of using a stimulant drug can beovercome by using buspirone, which has no reportedabuse potential. Its efficacy in adults and adolescentswith ADHD and comorbid drug and alcohol abusewould be worthy of investigation. A double-blind crossover study comparing buspirone with well-establishedtreatments such as methylphenidate would be veryuseful. These open and preliminary findings of theapparent efficacy of buspirone for ADHD in childrenindicate that further controlled trials are warranted.
REFERENCESAmerican Psychiatric Association (1994), Diagnostic and Statistical Manual of
Mental Disorders, 4th edition (DSM-IV). Washington, DC: AmericanPsychiatric Association
Andrews N, File SE (1993), Increased 5-HT release mediates the anxiogenicresponse during benzodiazepine withdrawal: a review of supporting
370
neurochemical and behavioral evidence. Psychopharmacology (Berl)112:21-25
Arnsten AFT, Cai JX (1993), Post-synaptic alpha-2 receptor stimulationimproves memory in aged monkeys: indirect effects of yohimbine versusdirect effects of clonidine. Neurobiol Aging 14:597-603
Arnsten AFT, Steere JC, Hunt RD (1996), The contribution of alpha-2noradrenergic mechanisms to prefrontal cortical cognirive function:potential significance for ADHD. Arch GenPsychiatry 53:448-455
Balon R (1994), Buspirone in rhe treatment of separation anxiety in anadolescent boy. CanJ Psychiatry 39:581-582
Barickman L, Noyes R, Kuperman S et al. (1991), Treatment of ADHDwith Auoxetine: a preliminary rrial. JAm Acad Child AdolescPsychiatry30:765-767
Carli M, Robbins TW, Evenden JL, Everitt BJ (1983), Effect of lesions toascending noradrenergic neurons on performance of a 5-choice serialreaction task in rars: implications for theories of dorsal noradrenergicbundle function based on selective attention and arousal. BebauBrainRtf9:361-380
Castellanos FX, Giedd IN, Marsh WL et al. (1996), Quantitative brain magnetic resonance imaging in attention-deficit hyperactivity disorder. ArchGen Psychiatry 53:607-616
Castillo C. Ibarra M, MarquezjA et al. (1993), Pharmacological evidence forinteraction between 5-HTIA receptor agonists and subtypes of alpha- 1adrenoreceprors on rabbit aorta. Eur J Pharmacol24:141-148
Cook EH, Stein MA, Krasowski MD er al. (1995), Association of attentiondeficit disorder and the dopamine transporter gene. Am J Hum Gena56:993-998
Cronbach LJ (195 I), Coefficient alpha and the internal structure of tests.Psycbometrika 16:297-334
Eison AS, Temple DL Jr (1986), Buspirone: review of its pharmacology andcurrent perspectives on its mechanism of action. Am J Med 80(3Bsuppl}:I-9
Farringron Dr, Loeber R, van Kammen WB (1990), Long-term criminaloutcomes of hyperactivity-impulsivity-attention deficit and conductproblems in childhood. In: Straightand Devious Pathways From Childhood to Adulthood, Robins LN, Rutter M, eds. Cambridge, England:Cambridge University Press, pp 62-81
Gammans RE, Mayol RF, Eison MS (1983), Concentration of buspironeand I-pyrimidinyl piperazine, a metabolic, in rat brain. FedProc 42:377
Gittelman R, Mannuzza S, Shenker R, Bonagura N (1985), Hyperactiveboys almost grown up, I: psychiatric status. Arch Gen Psychiatry 42:937-947
Goyette CH, Conners CK, Ulrich RF (1978), Normative data on revisedConners parent and teacher rating scales. J Abnorm Child Psycho]6:221-236
Greenhill LL (1992), Pharmacotherapy: stimulants. Child Adolesc PsychiatrClin North Am 1:411-448
Gross MD (1995), Buspirone in ADHD with ODD (letter). JAm AcadGild AdolescPsychiatry 34: 1260
Gunning WB (1992), A controlled trial of clonidine in hyperkinetic children. Thesis, Erasmus University, Rotterdam, the Netherlands
Halperin JM, Newcom JH, Sharma Y er al. (1990), Inattentive and noninattentive ADHD children: do they constitute a unitary group?JAbnormChild P'JchoI18:437-449
Halperin JM, Sharma Y, Siever LJ er al. (1994), Seroronergic function inaggressive and non-aggressive boys with ADHD. Am J Psychiatry151:243-248
Hinshaw SP (1994), On the distinction between artentional deficit/hyperactivity and conduct problems/aggression in child psychopathology.Psychol Bull 101:443-463
Hunt RD, Minderaa RB, Cohen DJ (1985), Clonidine benefits childrenwith attention deficit disorder and hyperactivity: report of a doubleblind placebo-crossover therapeutic trial. JAm Acad Child AdolescPsychiatry 24:617-629
Hynd GW, Hem KL, Novey ES er al. (1993), Attention deficit-hyperactivitydisorder and asymmetry of the caudate nucleus. J Child Neurol 8:339-347
Kranzler HR (1989), Buspirone in an adolescent with overanxious disorder.JAm Acad ChildAdolesc Psychiatry 50:382-384
]. AM. ACAD. CHIl.D ADOl.ESC. PSYCHIATRY, .H:4, APRIL 1998

Kruesi KJP, Hibbs ED. Zajh T P et al. (1992 ). A 2 year prospective follow upstudy of child ren and adolescents with disruptive behavior disorders:predict ion by CSF 5-H[AA. homovanillic acid and autonomic measures?Arch Gen Psychiatry49:429-435
Kruesi KJP, Rappoport J. Hamburger SO et al. (1990). Cerebrospinal fluidmonoam ine metabolites. aggression and impulsivity in disruptive behavior disorders of child ren and adolescents. Arch Gen P.rychiatry47:4[9-426
Lahosta GJ, Swanson JM . Wigal SB et al. (19% ), Dopamine 0 4 receplOrgene polymorphism is associated with attention deficit hyperactivity disorder. Mol P.rychiatry 1:121-1 24
Levine S (1988). Buspirone: clinical studies in psychiatry. In: Buspirone: ANeu/ Introduction to the Treatment of Anxirty. Cader M, ed (Royal Societyof Med icine Services Intern ational Congress and Symposium Series).Lond on : Royal Society of Medicine Services Limited [33:43-47
Li B-M, Mei ZT (199 5), Alpha-2 adrenergic modulat ion of prefrontalneuron al activity related to working memory in monkeys. Presented at the3rd Congress of the Federal Asian and Oceanian Physiological Societies.Abstract 9-3(0)
Lou HC, Henriksen L. Bruhn P. Borner H. Bieber NJ (1989). Striataldysfunction in attent ion deficit and hyperkinet ic d isorder. Arch Neurol46:48- 52
Mando ki M ([994) . Buspirone treatment of traumatic brain injury in a childwho is highly sensitive to adverse effects of psychotrop ic medicat ions. JChild Adolesc P.rychopharmacoI4 :129-139
Pearlson G O. Robinson RG (198 1). Suction lesions of the frontal cerebralcortex in the rat indu ce asymmetrical behavioral and catecholam inergicresponses. Brain Rrs 218:233-242
Q uaison N, Ward 0 , Kitchen T (1991). Buspirone for aggression (Ieu er). ]Am Acad Child Adolesc Psychiatry30:1026
Rapport MD . Denney C. Du Paul GJ. Gardner MJ (1994). Attent ion deficitdisorder and rnethylphenidare: normalization rates. clinical effectiveness.and response prediction in 76 children. ] Am Acad Child AdolescPsychiatry 33:882-893
Raskin LA. Shaywirz BA. Anderson G M. Cohen OJ. Teicher MH . Liakis J(1983), Differential effects of selective dopam ine. no repinephrine orcatecholamine deplet ion on activity and learning in the developing rat.Pharmacol Biocbem Brhau 19:743-749
Ratey JJ. Sovner R. Mikkelsen E. Chmielinski HE (1989). Buspirone therapyfor maladaptive behavior and anxiety in developmentally disabled persons.] Clin Psychiatry 50:382-384
Realmuto G M . Augu st GJ. Ga rfinkel BD (1989) . Cli nica l effects ofbuspirone in autistic child ren.J Ciin P.rychopharmacoI 9:[22-[ 25
Roberts D CS. Price MTC. Fibiger H C (197 6), T he dor sal tegmen talnorad renergic projection: an analysis of its role in maze learning.J CompPhysiolPsychoI90 :363-372
Roeltgen DP, Schneider JS (1994). Task persistence and learning ability innormal and chronic low dose MPTP-treated monk eys. BehauBrain Res60:115-124
Sanghera MK . McMillen BA, Ge rma n DC (1983). Buspir one , a nonbenzod iazep ine anxio lyric, increases locu s ceru leus noradrenergicneuronal activity. Eur] Pharmacol 86:107-110
Sawaguchi T. Matsumura M. Kubota K (1990 ). Catecholaminergic effectsonneuron al activity related 10 a delayed response task in monkey prefront alcortex.] Nrurophysiol 63:1385-[ 400
j, AM. ACA D . CH I LD ADOL ESC. PSYCHIATRY, .37: 4 . APRIL 19 9 8
BUSPIRON E T R[AL FOR ADHD
Shaffer D. Go uld MS. Brasic J. Ambrosini 1', Bird HR . Aluwahlia S (1983).A chi ld ren's global assessment scale (CGAS). Arch Gen Psychiatry40:122 8-1231
Shaywitz BA. Cohen OJ. Bowers MB (1977), CSF monoamine metabo litesin children with minimal brain dysfunction: evidence for alteration ofbrain dopamine .JPediatr90:67-7 1
Shaywitz BA. Klopper JH . Go rdon JW (1978 ). Meth ylphenidate in 6hydroxydopamine-treated developing rat pups. Arch NruroI35 :463-469
Shaywirz BA, Teicher MH, Co hen DJ. Anderson GM, Young JG , Levitt I'(1984). Dopaminergic but not noradrenergic modulation of hyper activity and performance deficits in the develop ing rat pup. Psychopharmacology 82:73-77
Shekim WO , Dekirmenj ian J. Chapel JL (1979). Urinary MHPG excretionin min imal brain dysfunction and its mod ification by d-amphetamine.Am] P.rychiatry 136:667- 671
Simeon JG. Knot VJ. Dub ois D er aI . (1994) . Buspirone therap y of mixedanxiety disorders in childhood and adolescence: a pilot study. J ChildAdolesc Psychopharmacol4: 159-170
Sokol MS, Cam pbell M, Goldstein M et al. (1987). Attention deficit disorder with hyperactivity and the dopamine hypothe sis: case presentat ionsand theoret ical background. ] Am Acad Child Adolesc Psychiatry 26:428-433
Soni P,Weintraub AL (1992) . Buspirone-associated mental status changes. ]Am Acad Child Adolesc P.rychiatry 31:1098-1099
Spencer T, Wilens T, Biederman J (1994). Tricyclic ant idepressant treatmentof hyperactivity. Curr Opin Psychiatry 7:304- 307
Stoff DM . Pullock L, Vitello B. Behar D. Bridger WH (1987). Reduction of"H vimi prami ne bind ing sites on platelets of conduct disordered children.Nrurop.rychopharmacology 1:55-62
Sussman N (1994), The uses of buspirone in psychiatry. ] Clin Psychiatry12:3-1 9
Taylor E. Hem sley R (1995) . Treating hyperkinet ic d isorders in childh ood.BMj31O :1617-1618
Taylor E. Sandberg S. Thorley G , Giles S (l 99\) . Tb« Epidrmiology ofChildhood Hyperactivity (Ma udsley Mon ographs No . 33 ). O xford .England : O xford University Press
Taylor E. Schachar R. Thorley G. Wieselberg M (1986). Conduct disorderand hyperactivity. BrJ P.rychiatry 149:760- 777
Taylor Dr. Hyslop DK (l99\) , Chronic administration of buspirone downregulates 5-HT 2 receptor bind ing sites. Drug Deu Res 24:93-105
Temple DL Jr. Yevich Jp, New JS (1982), Buspirone: chemical profile of anew class of anxioselecrive agents. ] Clin Psychiatry 43:4- 10
Tun icliff G. Brokaw JJ. Hausz JA et aI . (1992). Influence of repeated treatment with buspirone on central 5-HT and dopamine synthesis. Neuropharmacology31:991-995
World Health Organization (1992). International Classification of Diseases,10th Revision: The Classification of Mental and Behavioral Disorders:Clinical Descriptions and Diagnostic Guidelines. Geneva: World HealthOrgan ization
Zwier KJ. Rao U (1994), Case study: busp irone use in an adolescent withsocial phobia and mixed personality disorder (cluster A type). JAm ACMChild Adolesc Psychiatry 33:1007-10 II
371

























