Embed Size (px)
Citation preview

AnaphylaxisAnaphylaxis
Peter MackOctober 31, 2007
Peter MackOctober 31, 2007

Hypersensitivity ResponsesHypersensitivity Responses
• 1975 - Gell & Coombs described a scheme for classifying immune responses which function as protective mechanisms
• However, these immune pathways can react inappropriately to produce a hypersensitivity or allergic response
• Hypersensitivity reaction I - IV
• 1975 - Gell & Coombs described a scheme for classifying immune responses which function as protective mechanisms
• However, these immune pathways can react inappropriately to produce a hypersensitivity or allergic response
• Hypersensitivity reaction I - IV

Type IType I
• Anaphylactic (immediate - type)• Physiologically active mediators
are released from mast cells & basophils
• Triggered by antigen binding to IgE antibodies on the membranes of these cells
• Eg. Anaphylaxis, allergic rhinitis
• Anaphylactic (immediate - type)• Physiologically active mediators
are released from mast cells & basophils
• Triggered by antigen binding to IgE antibodies on the membranes of these cells
• Eg. Anaphylaxis, allergic rhinitis

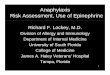
Type IType I
Cross-linkage of two IgE induce degranulation
Complement independent
Cross-linkage of two IgE induce degranulation
Complement independent
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

Type II (Cytotoxic Reactions)Type II (Cytotoxic Reactions)
• Antibody-dependent cell-mediated cytotoxic hypersensitivity
• IgG & IgM directed against antigens on foreign cells
• Antigens can be integral membrane components (ABO) or haptens that absorb to cell surfaces (AIHA)
• Antibody-dependent cell-mediated cytotoxic hypersensitivity
• IgG & IgM directed against antigens on foreign cells
• Antigens can be integral membrane components (ABO) or haptens that absorb to cell surfaces (AIHA)

Type IIType II
• Cell damage produced by:– Direct cell lysis after complete
compliment cascade activation– Increased phagocytosis by
macrophages– Killer T-cell lymphocyte producing Ab-
dependent cell-mediated cytotoxic effects
– Eg. ABO incompatibility, HIT
• Cell damage produced by:– Direct cell lysis after complete
compliment cascade activation– Increased phagocytosis by
macrophages– Killer T-cell lymphocyte producing Ab-
dependent cell-mediated cytotoxic effects
– Eg. ABO incompatibility, HIT

Type IIType II
• Complement activation
• Targeted cell destruction
• Complement activation
• Targeted cell destruction
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

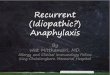
Type IIIType III
• Circulation, soluble antigens & antibodies that bind to form insoluble complexes that deposit in the microvasculature
• Complement is activated & neutrophils localize to the site & produce tissue damage
• Eg. Serum sickness after snake antisera
• Circulation, soluble antigens & antibodies that bind to form insoluble complexes that deposit in the microvasculature
• Complement is activated & neutrophils localize to the site & produce tissue damage
• Eg. Serum sickness after snake antisera

Type IIIType IIIBasement membrane
Endothelium
Antigen
Complement
IgG
PMN
Vasculitis, Increased capillary permeability

Type IVType IV
• Delayed hypersensitivity reactions• Interaction of sensitized
lymphocytes with specific antigens (antibody independent)
• Manifests 18-24h, peak 40-80h, disappears 72-96h
• Delayed hypersensitivity reactions• Interaction of sensitized
lymphocytes with specific antigens (antibody independent)
• Manifests 18-24h, peak 40-80h, disappears 72-96h

Type IVType IV
• Antigen-lymphocyte binding produces– Lymphokine synthesis– Lymphocyte proliferation– Generation of cytotoxic T-cells– Attraction of macrophages
• Cytotoxic T-cells specifically kill target cells that bear antigens identical to those that triggered the reaction
• Antigen-lymphocyte binding produces– Lymphokine synthesis– Lymphocyte proliferation– Generation of cytotoxic T-cells– Attraction of macrophages
• Cytotoxic T-cells specifically kill target cells that bear antigens identical to those that triggered the reaction

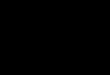
Type IVType IV
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Eg. Graft-versus-host, contact dermatitis

Intraoperative Allergic Reactions
Intraoperative Allergic Reactions
• 1:5,000 - 1:25,000 anesthetics• 3.4% mortality• >90% evoked by IV drugs occurs
within 5 minutes• Anaphylaxis is the most feared,
with circulatory collapse, reflecting vasodilation & decreased venous return
• 1:5,000 - 1:25,000 anesthetics• 3.4% mortality• >90% evoked by IV drugs occurs
within 5 minutes• Anaphylaxis is the most feared,
with circulatory collapse, reflecting vasodilation & decreased venous return

DefinitionsDefinitions
• Anaphylaxis (Portier & Richet)• “ana” - against• “prophylaxis” - protection• Profound shock & subsequent
death in dogs after 2nd challenge with a foreign antigen
• Mediated by antibodies
• Anaphylaxis (Portier & Richet)• “ana” - against• “prophylaxis” - protection• Profound shock & subsequent
death in dogs after 2nd challenge with a foreign antigen
• Mediated by antibodies

DefinitionsDefinitions
• Anaphylactoid– When antibodies are not responsible
for the reaction, or their involement cannot be proven
Cannot be distinguished from one another on the basis of clinical observation
• Anaphylactoid– When antibodies are not responsible
for the reaction, or their involement cannot be proven
Cannot be distinguished from one another on the basis of clinical observation

Systems Symptoms Signs Respiratory Dyspnea Coughing Chest discomfort Wheezing Sneezing Laryngeal edema Decreased pulmonary compliance Fulminant pulmonary edema Acute respiratory failure Cardiovascular Dizziness Disorientation Malaise Diaphoresis Retrosternal oppression Loss of consciousness Hypotension Tachycardia Dysrhythmias Decreased systemic vascular resistance Cardiac arrest Pulmonary hypertension Cutaneous Itching Urticaria Burning Flushing Tingling Periorbital edema Perioral edema
Recognition of Anaphylaxis During Regional and General Anesthesia

Anaphylactic ReactionsIgE-mediated pathophysiology
Anaphylactic ReactionsIgE-mediated pathophysiology
• Antigen binding to IgE initiates the reaction
• Prior exposure to the antigen (or substance of similar structure) is required for sensitization
• Allergic history may be unknown
• Antigen binding to IgE initiates the reaction
• Prior exposure to the antigen (or substance of similar structure) is required for sensitization
• Allergic history may be unknown

Anaphylactic Reactions IgE-mediated pathophysiology
Anaphylactic Reactions IgE-mediated pathophysiology• On re-exposure, antigen binds to &
bridges two immunospecific IgE Ab’s located on the surface of mast cells of basophils
• Liberates stored mediators– Histamine, tryptase, chemotactic
factors
• On re-exposure, antigen binds to & bridges two immunospecific IgE Ab’s located on the surface of mast cells of basophils
• Liberates stored mediators– Histamine, tryptase, chemotactic
factors

Anaphylactic ReactionsIgE-mediated pathophysiology
Anaphylactic ReactionsIgE-mediated pathophysiology
• Arachadonic acid metabolites (leukotrienes, prostaglandins)
• Kinins & cytokines
• Synthesized & released in response to cellular activation
• Arachadonic acid metabolites (leukotrienes, prostaglandins)
• Kinins & cytokines
• Synthesized & released in response to cellular activation

Anaphylactic ReactionsIgE-mediated pathophysiology
Anaphylactic ReactionsIgE-mediated pathophysiology
• Bronchospasm, upper airway edema• Vasodilation, increased capillary
permeability• Urticaria
• Challenge in sensitized individuals usually produces immediate clinical manifestations
• Bronchospasm, upper airway edema• Vasodilation, increased capillary
permeability• Urticaria
• Challenge in sensitized individuals usually produces immediate clinical manifestations

Clinical MediatorsClinical Mediators
• Histamine (H1, H2, H3 receptors)• H1 - releases NO from vascular
endothelium, increases capillary permeability, contracts airways & vascular smooth muscle
• H2 - gastric secretions, inhibits mast cell activation, & contributes to vasodilation
• Histamine (H1, H2, H3 receptors)• H1 - releases NO from vascular
endothelium, increases capillary permeability, contracts airways & vascular smooth muscle
• H2 - gastric secretions, inhibits mast cell activation, & contributes to vasodilation

HistamineHistamine
• Undergoes rapid metabolism by histamine N-methyltransferase & diamine oxidase located in endothelial cells
• Undergoes rapid metabolism by histamine N-methyltransferase & diamine oxidase located in endothelial cells

Peptide MediatorsPeptide Mediators
• Factors that cause granulocyte migration (chemotaxis) & collection at the site of inflammatory stimulus
• Eosinophilic chemotactic factor of anaphylaxis (ECF-A) – Draws eosinophils, but role is uncertain as
eosinophils release enzymes that can inactivate histamine & leukotrienes
• Factors that cause granulocyte migration (chemotaxis) & collection at the site of inflammatory stimulus
• Eosinophilic chemotactic factor of anaphylaxis (ECF-A) – Draws eosinophils, but role is uncertain as
eosinophils release enzymes that can inactivate histamine & leukotrienes

Arachadonic Acid MetabolitesArachadonic Acid Metabolites
• Leukotrienes & prostaglandins are both synthesized after activation of mast cells
• Metabolism of phospholipid membranes via lipoxygenase or cyclo-oxygenase
• Leukotrienes & prostaglandins are both synthesized after activation of mast cells
• Metabolism of phospholipid membranes via lipoxygenase or cyclo-oxygenase

LeukotrienesLeukotrienes
• C4, D4, E4
• Slow reacting
– Bronchoconstriction (> histamine)– Increased capillary permeability– Vasodilation– Coronary vasoconstriction– Myocardial depression
• C4, D4, E4
• Slow reacting
– Bronchoconstriction (> histamine)– Increased capillary permeability– Vasodilation– Coronary vasoconstriction– Myocardial depression

ProstaglandinsProstaglandins
PG D2
• Vasodilation• Bronchospasm• Pulmonary hypertension• Increased capillary permeability
PG D2
• Vasodilation• Bronchospasm• Pulmonary hypertension• Increased capillary permeability

KininsKinins
• Vasodilation• Increased capillary permeability• Bronchoconstriction
• Stimulates vascular endothelium to release vasoactive factors– Prostacyclin, NO
• Vasodilation• Increased capillary permeability• Bronchoconstriction
• Stimulates vascular endothelium to release vasoactive factors– Prostacyclin, NO

Platelet-Activating FactorPlatelet-Activating Factor
• Synthesized in activated mast cells• Extremely potent• Causes platelets to aggregate and
release inflammatory products• PAF causes profound wheal-and-
flare response, smooth muscle contraction & increase capillary permeability
• Synthesized in activated mast cells• Extremely potent• Causes platelets to aggregate and
release inflammatory products• PAF causes profound wheal-and-
flare response, smooth muscle contraction & increase capillary permeability

Non-IgE-Mediated ReactionsNon-IgE-Mediated Reactions
• Other immunologic & non-immunologic mechanisms liberate many of the same mediators producing clinically identical syndromes
• Other immunologic & non-immunologic mechanisms liberate many of the same mediators producing clinically identical syndromes

ComplementComplement
• “activation follows both immunologic (Ab-mediated, i.e., classic pathway) or nonimmunologic (alternative) pathways to include a series of multimolecular, self-assembling proteins that liberate biologically active complement fragments of C3 & C5”
• “activation follows both immunologic (Ab-mediated, i.e., classic pathway) or nonimmunologic (alternative) pathways to include a series of multimolecular, self-assembling proteins that liberate biologically active complement fragments of C3 & C5”

ComplementComplement
• C3a & C5a “anaphylatoxins”• Release histamine, contract
smooth muscle, increase capillary permeability and stimulate interleukin synthesis
• C3a & C5a “anaphylatoxins”• Release histamine, contract
smooth muscle, increase capillary permeability and stimulate interleukin synthesis

ComplementComplement
• C5a interacts with specific high-affinity receptors on PMNs & platelets initiating leukocyte chemotaxis, aggregation & activation
• C5a interacts with specific high-affinity receptors on PMNs & platelets initiating leukocyte chemotaxis, aggregation & activation

ComplementComplement
• Aggregated leukocytes embolized to various organs, producing microvascular occlusion & liberation of inflammatory mediators such as arachadonic acid metabolites, O2 free radicals & lysosomal enzymes
• Aggregated leukocytes embolized to various organs, producing microvascular occlusion & liberation of inflammatory mediators such as arachadonic acid metabolites, O2 free radicals & lysosomal enzymes

Nonimmunologic Release of HistamineNonimmunologic Release of Histamine• Many molecules administered in the
perioperative period release histamine in a dose-dependent, nonimmunologic fashion
• Mechanism not fully understood• Involves selective mast cell & basophil
activation• Cutaneous mast cells are the only cell
population that releases histamine in response to drugs & endogenous stimuli
• Many molecules administered in the perioperative period release histamine in a dose-dependent, nonimmunologic fashion
• Mechanism not fully understood• Involves selective mast cell & basophil
activation• Cutaneous mast cells are the only cell
population that releases histamine in response to drugs & endogenous stimuli

Drugs Capable of Nonimmunologic Histamine
Relsease
Drugs Capable of Nonimmunologic Histamine
Relsease• Antibiotics (Vancomycin)• Basic compounds• Hyperosmotic agents• Muscle relaxants (d-turbocurarine,
atracurium, mivacurium)• Opioids (morphine, meperidine,
codeine)• Thiobarbiturates
• Antibiotics (Vancomycin)• Basic compounds• Hyperosmotic agents• Muscle relaxants (d-turbocurarine,
atracurium, mivacurium)• Opioids (morphine, meperidine,
codeine)• Thiobarbiturates

Treatment PlanTreatment Plan
Airway Maintenance 100% O2 Intravascular volume expansion Epinephrine
Hypoxia Hypotension
2˚ to Vasodilation Increased capillary permeability Bronchospasm

Treatment PlanTreatment Plan
• Titrated to desired effect with careful monitoring
• Reactions can be protracted requiring aggressive therapy
• Manifestations may recur after successful treatment monitor in ICU x 24h
• Titrated to desired effect with careful monitoring
• Reactions can be protracted requiring aggressive therapy
• Manifestations may recur after successful treatment monitor in ICU x 24h

Watch for…Watch for…
• Persistent hypotension• Pulmonary hypertension• Lower respiratory obstruction• Laryngeal obstruction
• May continue for 5-32h despite vigorous therapy
• Persistent hypotension• Pulmonary hypertension• Lower respiratory obstruction• Laryngeal obstruction
• May continue for 5-32h despite vigorous therapy

Managment of Anaphylaxis During General Anesthesia Managment of Anaphylaxis During General Anesthesia
Initial Therapy
1. Stop administration of antigen 2. Maintain airway and administer 100% O2 3. Discontinue all anesthetic agents 4. Start intravascular volume expansion (2 – 4 l of crystalloid/ colloid with hypotension) 5. Give epinephrine (5 – 10 g iv bolus with hypotension, titrate as needed; 0.1 – 1.0 mg iv with cardiovascular collapse) Secondary Therapy
1. Antihistamines (0.5 – 1 mg ⋅ kg-1 diphenhydramin )e 2. Catecholamine infusions (startin gdo :ses epinephrin ,e 4 – 8 g ⋅ min-1; norepinephrine, 4 – 8 g ⋅ min-1; or isoproterenol, 0.5 – 1 g ⋅ min-1 as a dri ;p titrated to desired effect )s 3. Aminophyllin e(5 – 6 mg ⋅ kg-1 over 20 min with persisten tbronchospasm) 4. Corticosteroids (0.25 – 1 g hydrcortisone; alternatively, 1 – 2 g methylprednisolon )e 5. Sodium bicarbonat (0.e 5 – 1 mEq ⋅ kg-1 wit hpersisten thypotensio nor acidosi )s 6. Airway evaluatio n (before extubation)

Initial TherapyInitial Therapy
• Stop of limit further antigen administration
• Maintain airway & administer 100% O2
– Profound V/Q mismatch can accompany anaphylaxis
– ABG’s may be useful to follow
• Stop of limit further antigen administration
• Maintain airway & administer 100% O2
– Profound V/Q mismatch can accompany anaphylaxis
– ABG’s may be useful to follow

Initial TherapyInitial Therapy
• D/C all anesthetic drugs– Vapours are not the bronchodilator of
choice after anaphylaxis– Worsen hypotension– Interfere with body’s compensatory
response to CV collapse
• D/C all anesthetic drugs– Vapours are not the bronchodilator of
choice after anaphylaxis– Worsen hypotension– Interfere with body’s compensatory
response to CV collapse

Initial TherapyInitial Therapy
• Volume expansion – Hypovolemia (up to 40% loss of intravascular fluid into
interstitial space)– 2-4 L crystalloid/ colloid initially (an additional 25-50
ml/kg may be necessary)– Refractory hypotension additional monitoring
• TEE can assess intravascular volume, ventricular function & any other occult cause of CV dysfunction
• Useful to guide therapy
– Fulminant noncardiogenic pulmonary edema• Require intravascular volume repletion with careful
hemodynamic monitoring until capillary dysfunction improves
• Volume expansion – Hypovolemia (up to 40% loss of intravascular fluid into
interstitial space)– 2-4 L crystalloid/ colloid initially (an additional 25-50
ml/kg may be necessary)– Refractory hypotension additional monitoring
• TEE can assess intravascular volume, ventricular function & any other occult cause of CV dysfunction
• Useful to guide therapy
– Fulminant noncardiogenic pulmonary edema• Require intravascular volume repletion with careful
hemodynamic monitoring until capillary dysfunction improves

Initial TherapyInitial Therapy
• Epinephrine– Drug of choice
- adrenergic combats hypotension2 causes bronchodilation & inhibits mediator release by cAMP in mast cells & basophils
– Route & dose depend on patients condition– Rapid & timely as pts under GA may have altered
sympathoadrenergic responses, whereas pts under regional may be partially sympathectomized & require larger doses
• Epinephrine– Drug of choice
- adrenergic combats hypotension2 causes bronchodilation & inhibits mediator release by cAMP in mast cells & basophils
– Route & dose depend on patients condition– Rapid & timely as pts under GA may have altered
sympathoadrenergic responses, whereas pts under regional may be partially sympathectomized & require larger doses

Initial TherapyInitial Therapy
• Epinephrine– 50-100 g bolus– Titrated to restore BP along with
additional volume– Complete CV collapse (0.1-1 mg)– Laryngeal edema (w/o hypotension)
may give sc
• Epinephrine– 50-100 g bolus– Titrated to restore BP along with
additional volume– Complete CV collapse (0.1-1 mg)– Laryngeal edema (w/o hypotension)
may give sc

Secondary TreatmentSecondary Treatment
• Antihistamine– 0.5-1.0 mg/kg diphenhydramine (H1)
– Does not inhibit the reaction, or release of histamine
– Competes for receptor sites
– H2 antagonists remain unclear
• Antihistamine– 0.5-1.0 mg/kg diphenhydramine (H1)
– Does not inhibit the reaction, or release of histamine
– Competes for receptor sites
– H2 antagonists remain unclear

CatecholaminesCatecholamines
• Epinephrine infusions for persistent hypotension or bronchospasm– 0.05-0.1g/kg/min (5-10g/min) &
titrate to correct BP– Norepinephrine may also be useful in
refractory hypotension 2 SVR• 0.05-0.1g/kg/min (5-10g/min)
• Epinephrine infusions for persistent hypotension or bronchospasm– 0.05-0.1g/kg/min (5-10g/min) &
titrate to correct BP– Norepinephrine may also be useful in
refractory hypotension 2 SVR• 0.05-0.1g/kg/min (5-10g/min)

AminophyllineAminophylline
• Nonspecific phosphodiesterase inhibitor• Bronchodilates & histamine release
from MC & B’s by cAMP contractility & pulmonary vascular
resistance• Persistent bronchospasm &
hemodynamic stability– IV loading dose 5-6 mg/kg over 20 min– 0.5-0.9 mg/kg/hr
• Nonspecific phosphodiesterase inhibitor• Bronchodilates & histamine release
from MC & B’s by cAMP contractility & pulmonary vascular
resistance• Persistent bronchospasm &
hemodynamic stability– IV loading dose 5-6 mg/kg over 20 min– 0.5-0.9 mg/kg/hr

CorticosteroidsCorticosteroids
• Anti-inflammatory• 12-24h for effect• 0.25-1g IV hydrocortisone in IgE-
mediated reactions• 1-2g IV methylprednisolone in
complement-mediated– Eg. Pulmonary vasocontriction after
protamine
• May attenuate late-phase reactions
• Anti-inflammatory• 12-24h for effect• 0.25-1g IV hydrocortisone in IgE-
mediated reactions• 1-2g IV methylprednisolone in
complement-mediated– Eg. Pulmonary vasocontriction after
protamine
• May attenuate late-phase reactions

BicarbonateBicarbonate
• Acidosis develops quickly• Diminishes effect of epinephrine• Refractory hypotension & acidosis• 0.5-1 mEq/kg q5min• Follow ABG’s
• Acidosis develops quickly• Diminishes effect of epinephrine• Refractory hypotension & acidosis• 0.5-1 mEq/kg q5min• Follow ABG’s

Airway EvaluationAirway Evaluation
• Laryngeal edema may occur– Suggested by facial edema
• Leave intubated until edema subsides
• Air leak useful for patency• Consider direct laryngoscopy
• Laryngeal edema may occur– Suggested by facial edema
• Leave intubated until edema subsides
• Air leak useful for patency• Consider direct laryngoscopy

Perioperative ManagementPerioperative Management• Allergic drug reactions account for
6-10% of all adverse reactions• The risk of an allergic drug
reactions ~ 1-3% for most drugs• ~5% of adults (1 or more drugs)• ~15% of adults believe they are
allergic to specific drugs
• Allergic drug reactions account for 6-10% of all adverse reactions
• The risk of an allergic drug reactions ~ 1-3% for most drugs
• ~5% of adults (1 or more drugs)• ~15% of adults believe they are
allergic to specific drugs

Adverse Drug ReactionsAdverse Drug Reactions
• Predictable ADR account for ~80% of all reactions
• Dose dependent• Known pharmacologic action• Most serious, predictable ADR are
toxic & directly related to dose (OD)
• Predictable ADR account for ~80% of all reactions
• Dose dependent• Known pharmacologic action• Most serious, predictable ADR are
toxic & directly related to dose (OD)

Adverse Drug ReactionsAdverse Drug Reactions
• “Side effects are the most common adverse drug reaction and are undesirable pharmacologic actions of the drugs at usual prescribed dosages.”
• “Side effects are the most common adverse drug reaction and are undesirable pharmacologic actions of the drugs at usual prescribed dosages.”

Unpredictable ADR’sUnpredictable ADR’s
• Not dose dependent• Not related to pharmacologic actions• Immunologic response of the
individual• Proving the immunologic mechanism
may be a challenge
• Not dose dependent• Not related to pharmacologic actions• Immunologic response of the
individual• Proving the immunologic mechanism
may be a challenge

Unpredictable ADR’sUnpredictable ADR’s
– Occur only in a small percentage of pts receiving the drug
– Clinical manifestations do not resemble known pharmacologic actions
– Occur only in a small percentage of pts receiving the drug
– Clinical manifestations do not resemble known pharmacologic actions

Unpredictable ADR’sUnpredictable ADR’s
• In the absence of prior drug exposure, allergic symptoms rarely appear
• After sensitization the reaction can occur rapidly on re-exposure
• In the absence of prior drug exposure, allergic symptoms rarely appear
• After sensitization the reaction can occur rapidly on re-exposure

Immunologic MechanismsImmunologic Mechanisms
• All 4 mechanisms– Eg. Penicillin - different reaction in different
pts or spectrum in same pt
• In the same pt - anaphylaxis (I), hemolytic anemia (II), serum sickness (III), contact dermatitis (IV)
• Any one antigen can produce a diffuse spectrum of responses
• All 4 mechanisms– Eg. Penicillin - different reaction in different
pts or spectrum in same pt
• In the same pt - anaphylaxis (I), hemolytic anemia (II), serum sickness (III), contact dermatitis (IV)
• Any one antigen can produce a diffuse spectrum of responses

AGENTS IMPLICATED IN ALLERGIC REACTIONS DURING ANESTHESIA Anesthetic Agents
Induction agents (cremophor-solubilized drugs, barbiturates, etomidate, propofol) Local anesthetics (para-aminobenzoic ester agents) Muscle relaxants (succinylcholine, gallamine, pancuronium, d-tubocurarine, metocurine, atracurium, vecuronium, mivacurium, doxacurium, rocuronium) Opioids (meperidine, morphine, fentanyl) Other Agents
Antibiotics (cephalosporins, penicillin, sulfonamides, vancomycin) Aprotinin Blood products (whole blood, packed cells, fresh frozen plasma, platelets, cryoprecipitate, fibrin glue, gamma globulin) Bone cement Chymopapain Corticosteroids Cyclosporin Drug additives (preservatives) Furosemide Insulin Mannitol Methylmethacrylate Nonsteroidal anti-inflammatory drugs Protamine Radiocontrast dye Latex (natural rubber) Streptokinase Vascular graft material Vitamin K Colloid volume expanders (dextrans, protein fractions, albumin, hydroxyethyl startch)

Anesthetic DrugsAnesthetic Drugs
• Nearly all have been implicated• Muscle relaxants top the list
– Cross-sensitivity between succinylcholine & NDNMB
– Quaternary ammonium – Alternates should not be chosen
without testing
• Nearly all have been implicated• Muscle relaxants top the list
– Cross-sensitivity between succinylcholine & NDNMB
– Quaternary ammonium – Alternates should not be chosen
without testing

Anesthetic DrugsAnesthetic Drugs
• Life threatening reactions are more likely to occur in patients with a history of allergy, atopy or asthma
• Does not mandate further testing, pretreatment or avoidance of specific drugs
• Life threatening reactions are more likely to occur in patients with a history of allergy, atopy or asthma
• Does not mandate further testing, pretreatment or avoidance of specific drugs

EvaluationEvaluation
• Identification can be difficult• Circumstantial evidence of
temporal connection• in vitro & in vivo methods are
uncommon• Direct challenge (obvious hazards)• Drug-specific IgE
• Identification can be difficult• Circumstantial evidence of
temporal connection• in vitro & in vivo methods are
uncommon• Direct challenge (obvious hazards)• Drug-specific IgE

TestingTesting
• No testing & avoidance– One drug & clear temporal correlation
• Necessary– Many drugs are given– Preservatives
• No testing & avoidance– One drug & clear temporal correlation
• Necessary– Many drugs are given– Preservatives

Leukocyte Histamine ReleaseLeukocyte Histamine Release
• Incubate pts leukocytes with offending drug & measure histamine release as a marker for basophil activation
• False positives• Difficult to perform
• Incubate pts leukocytes with offending drug & measure histamine release as a marker for basophil activation
• False positives• Difficult to perform

Radioallergosorbant Test (RAST)Radioallergosorbant Test (RAST)
• in vitro detection of specific IgE directed towards particular antigens
• Pt serum exposed to antigen, a complex forms if specific IgE present
• Concentration is calculated (more quantitative than skin testing)
• in vitro detection of specific IgE directed towards particular antigens
• Pt serum exposed to antigen, a complex forms if specific IgE present
• Concentration is calculated (more quantitative than skin testing)

RASTRAST
• Avoids re-exposure• Limited by commercial availability
of drug-specific antigens• False positives (pts with elevated
IgE levels)• Meperidine, succinylcholine,
thiopental
• Avoids re-exposure• Limited by commercial availability
of drug-specific antigens• False positives (pts with elevated
IgE levels)• Meperidine, succinylcholine,
thiopental

Enzyme-linked Immunosorbent Assay (ELISA)Enzyme-linked Immunosorbent Assay (ELISA)
• Similar to RAST• Useful for protamine
• Similar to RAST• Useful for protamine

Intradermal TestingIntradermal Testing
• Most common method• Demonstrate “wheal-and-flare”• Simple, safe, useful• Requires re-exposure
• Most common method• Demonstrate “wheal-and-flare”• Simple, safe, useful• Requires re-exposure

LatexLatex
• Important cause of peri-operative anaphylaxis
• Sap from the tree Hevea brasiliensis (Rubber tree)
• 1979 - 1st case, contact dermatitis• 1989 - intraoperative anaphylaxis• 1991 - FDA “Dear Colleague”
• Important cause of peri-operative anaphylaxis
• Sap from the tree Hevea brasiliensis (Rubber tree)
• 1979 - 1st case, contact dermatitis• 1989 - intraoperative anaphylaxis• 1991 - FDA “Dear Colleague”

Latex - Risk FactorsLatex - Risk Factors
• Health care workers• Children with spina bifida• Frequent catheterizations• Foods (bananas, avocados, kiwis)• Atopy
• Health care workers• Children with spina bifida• Frequent catheterizations• Foods (bananas, avocados, kiwis)• Atopy

LatexLatex
• 24% incidence of contact dermatitis– Early stage of sensitization avoidance
• 12.5% incidence of latex-specific IgE positivity in anesthesiologists
• If proven strict avoidance is essential• Avoidance of anitgen exposure is the
best preventative therapy• Pretreatment is of little use
• 24% incidence of contact dermatitis– Early stage of sensitization avoidance
• 12.5% incidence of latex-specific IgE positivity in anesthesiologists
• If proven strict avoidance is essential• Avoidance of anitgen exposure is the
best preventative therapy• Pretreatment is of little use

SummarySummary
• 4 types of hypersensitivities
• 3 involve antibodies
• Anaphylaxis mediated by IgE
• Anaphylactoid is Ab independent
• 4 types of hypersensitivities
• 3 involve antibodies
• Anaphylaxis mediated by IgE
• Anaphylactoid is Ab independent

SummarySummary
• Anaphylaxis– Bronchospasm– Vasodilation, increased capillary
permeability– Urticaria
• Associated with profound CV collapse
• Anaphylaxis– Bronchospasm– Vasodilation, increased capillary
permeability– Urticaria
• Associated with profound CV collapse

SummarySummary
• Chemical mediators– Histamine– Leukotrienes & Prostaglandins– Kinins– Platelet-activating Factor– Complement
• Chemical mediators– Histamine– Leukotrienes & Prostaglandins– Kinins– Platelet-activating Factor– Complement

SummarySummary
• Management– ABCs– Volume expansion– Epinephrine
– Antihistamines, steroids, infusions
• Management– ABCs– Volume expansion– Epinephrine
– Antihistamines, steroids, infusions

SummarySummary
• Muscle relaxants• Antibiotics• Blood products• Latex• Colloids
• Muscle relaxants• Antibiotics• Blood products• Latex• Colloids

SummarySummary
• Testing– Leukocyte Histamine Release– RAST– ELISA– Skin testing
• Testing– Leukocyte Histamine Release– RAST– ELISA– Skin testing

ReferencesReferences
• Barash P. Clinical Anesthesia, 4th ed. Ch 49. Lippincott. 2001.
• Miller R. Miller’s Anesthesia, 6th ed. Ch 27. Churchill. 2005.
• Roizen M. Essence of Anesthesia Practice, 2nd ed. 2002
• Dunn P. Clinical Anesthesia Procedures of the Massachusetts General Hospital, 7th ed. p324. Lippincott. 2007.
• Barash P. Clinical Anesthesia, 4th ed. Ch 49. Lippincott. 2001.
• Miller R. Miller’s Anesthesia, 6th ed. Ch 27. Churchill. 2005.
• Roizen M. Essence of Anesthesia Practice, 2nd ed. 2002
• Dunn P. Clinical Anesthesia Procedures of the Massachusetts General Hospital, 7th ed. p324. Lippincott. 2007.